
Abstract
Study design
Retrospective Aanalysis of a Large Cohort of Cases.
Objectives
To explore the rate and cause of revision surgery after spinal fusion in adolescent idiopathic scoliosis(AIS).
Methods
The patients diagnosed with AIS who underwent spinal fusion surgery in a single center from 2002 to 2018 were retrospectively analyzed. All the patients were followed up at least 2 years. The causes of revision surgery were analyzed and the incidence of revision surgery was counted.
Results
A total of 1816 AIS patients were included in the study. After an average of 8.5 years (range 3-18 years) follow-up, a total of 51 patients underwent 54 revision operations. The overall revision rate is 2.8%. The revision rate of combined approach (anterior and posterior) and anterior approach was 6.6% (8/122), and the revision rate of posterior approach was 2.5% (43/1694). The most common causes of revision were malposition of implants/implants failure (37%), followed by poor wound healing/ infection (23%). Spinal decompensation, adding on and proximal junctional kyphosis (PJK) accounted for 20%. The compensatory curve continued to worsen after selective fusion accounted for 14% and finally the discomfort with the implants accounted for 6%.
Conclusions
The overall revision rate of spinal fusion for AIS is 2.8%. The implants and incision problems were the most common causes of revision surgeries.
Background
Adolescent idiopathic scoliosis is a kind of spinal disease with unclear etiology. The main treatment goal is to prevent the progression of scoliosis. At present, spinal fusion is the gold standard for the treatment of cases with scoliosis more than 50 degrees or with progression of scoliosis after conservative treatment. Spinal internal fixation has evolved from the first-generation Harrington system, the second generation Luque system, the third generation CD system. Recently, the pedicle screw system was widely used all around the world. 1 The surgical approaches include anterior approach, combined anterior and posterior approach and simple posterior approach. The percent correction of the curve in scoliosis surgery has increased, however, there are still complications in spinal fusion surgery, such as scoliosis progression, internal fixation failure, wound infection, etc., and some cases need revision surgery.2,3 Revision surgery will increase the cost of treatment and increase the incidence of complications. Analyzing the causes and treatment modalities of revision surgery for idiopathic scoliosis is of great clinical significance for how to minimize surgical complications and improve patient satisfaction. The literature on revision surgery for idiopathic scoliosis is relatively few. The revision rate reported in the literature varied between 7.5% - 14.3%,4,5 There is no unified standard on the type and prognosis of revision surgery.
The patients diagnosed with AIS who underwent spinal fusion surgery in a single center from 2002 to 2018 were retrospectively analyzed. All the patients were followed up at least 2 years. The causes of revision surgery were analyzed and the incidence of revision surgery was counted.
Materials and Methods
Inclusion and Exclusion Criterion
This study was approved by the ethics committee of our hospital (IRB approval number:S-K1857). All patients had signed informed consent before the surgery about medical data or images application for scientific purpose without privacy disclosure. All the patients with the diagnosis of adolescent idiopathic scoliosis (AIS) who underwent spinal fusion surgery in our hospital (2002-2018) were retrospectively analyzed, and the demographic information, diagnosis, surgery charts and complications were recorded and analyzed. Only patients with a minimum of two-year follow-up were included. Other etiologies of scoliosis and patients who received non fusion surgeries were excluded. The end point was revision surgery.
Surgical Technique
All operations were performed by senior spinal surgeons. From 2002 to 2005, some cases underwent combined anterior and posterior surgery, including anterior discectomy and release, posterior lamina hook and pedicle screw internal fixation. From 2002 to 2010, some cases underwent thoracoscopic anterior correction and internal fixation, anterior retroperitoneal correction and vertebral screw internal fixation. After 2010, all patients underwent posterior correction and pedicle screw internal fixation.
Analyzing parameters
All patients were routinely taken whole spine X-ray before operation, and immediately after operation, 3 months, 6 months, 1 year, 3 years, 5 years and 10 years after operation. The Lenke classification, Cobb angle of main curve, type of internal fixation, surgical approach, fusion segment, reason and time of revision were recorded.
Revision Causes Categories
The causes for revision are divided into the following categories: 1. Malposition of implants/implants failure; 2. Poor wound healing or infection; 3. Worsening of compensatory curve; 4. Trunk decompensation/adding on/proximal junctional kyphosis; 5. Implant discomfort.
Statistics
The revision rates of different surgical approaches in different time periods were counted. The reasons for revision in different time periods from the initial operation time were counted. The characteristics of revision cases of combined/anterior approach and simple posterior approach were compared. The continuous variables were tested by independent sample t-test, and the classified variables were tested by chi square test or Fisher’s exact test. P < 0.05 was the difference, which was considered statistically significant.
Results
A total of 1816 AIS patients were included (2002-2018), including 272 male patients and 1544 female patients. The average operative age was 15 years (range 10-19). There were 30 cases of combined (anterior and posterior) surgery, 92 cases of anterior surgery and 1694 cases of posterior surgery.
After an average of 8.5 years (range 3-18 years) follow-up, a total of 51 patients underwent 54 revision operations. The overall revision rate is 2.8%. The average age of the revision cases were 14.3 years. There were 18 male patients and 33 female patients.
Revision rates in different surgical approaches and time periods.

Comparison of surgical parameters between revision cases of different surgical approaches.
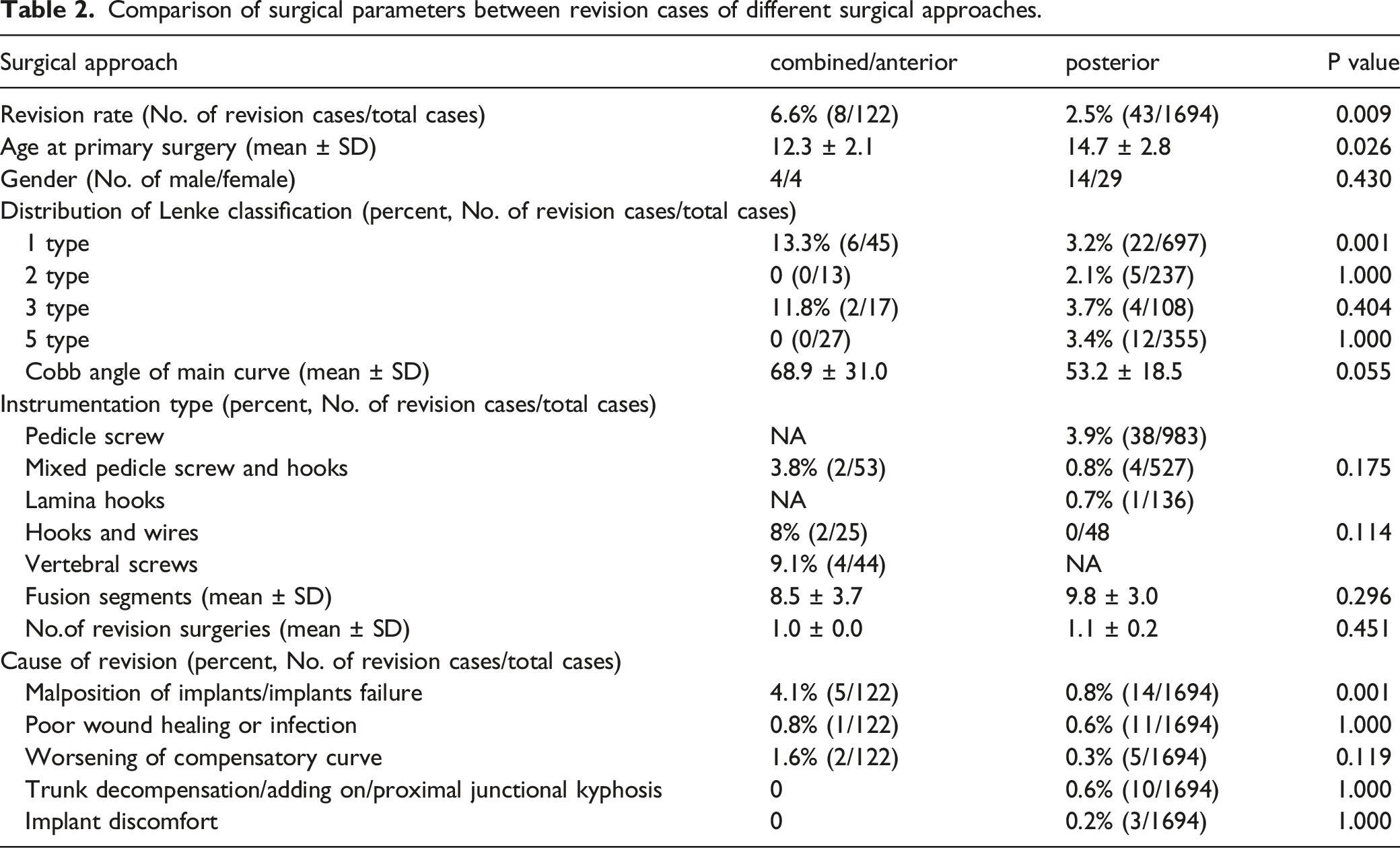
Through the analysis of the causes for the revision, it was found that the proportion of poor/failed internal fixation was the highest (19 cases, accounting for 37%, the incidence rate was 1.05%). The second cause was poor wound healing or infection (12 cases, accounting for 23%, the incidence rate was 0.66%), among which 7 cases of acute infection were treated with debridement and internal fixation retention. 6 cases were successful, and 1 case underwent debridement and implants removal. There were five cases of delayed infection (28-81 months from the initial operation, with an average of 49.6 months) and all of them underwent implants removal. The proportion of trunk decompensation/adding on/proximal junctional kyphosis (PJK) was the third cause of revision (10 cases, accounting for 20%, the incidence was 0.55%). Worsening of the compensatory curve accounted for 14% of all the revision cases (7 cases, incidence rate 0.39%). Discomfort with the implants who insisted implants removal accounted for 6% of the revision cases (3 cases, incidence rate 0.17%). (see Table 1, Figure 1) Illustration of proportion of different revision reasons.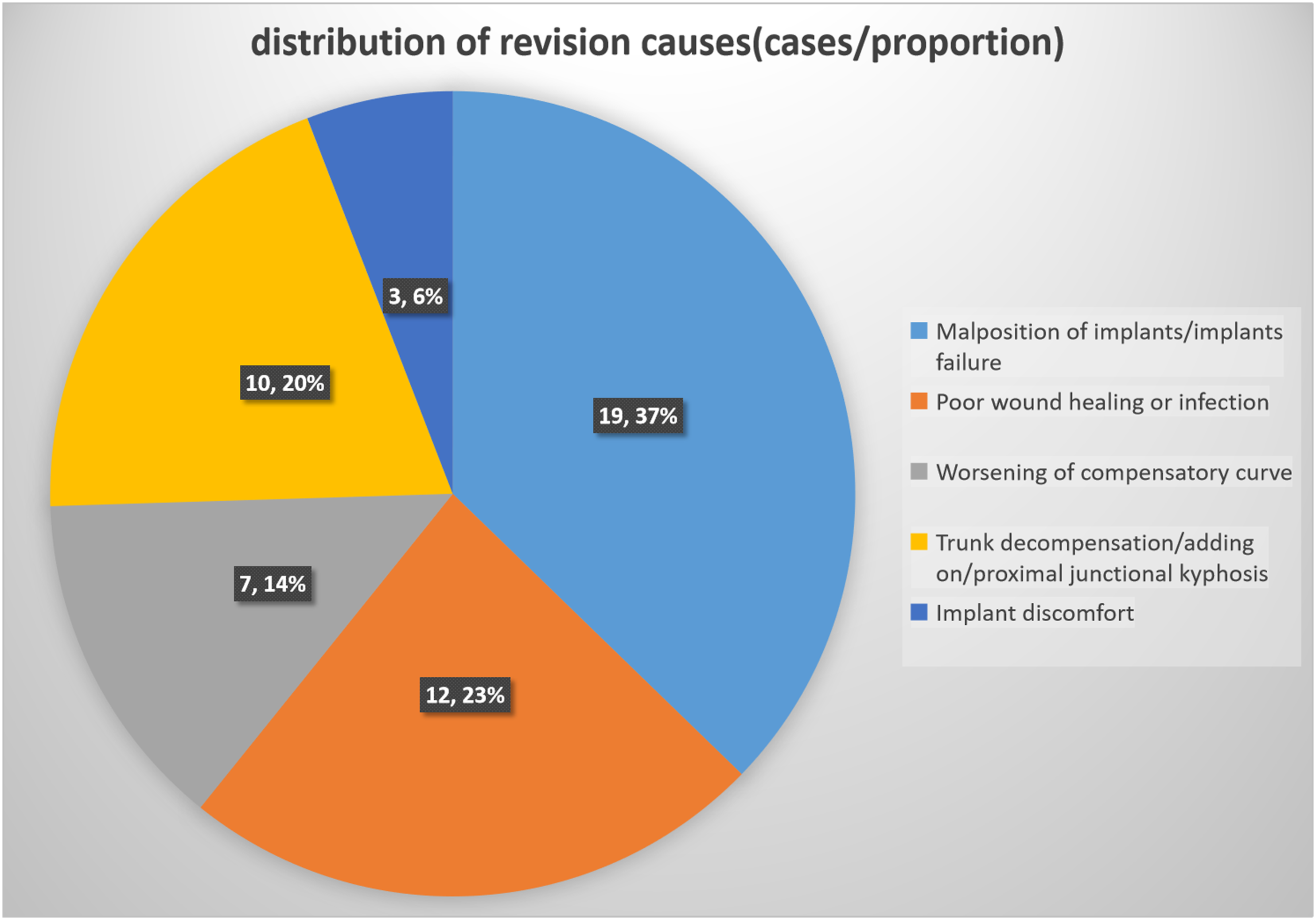
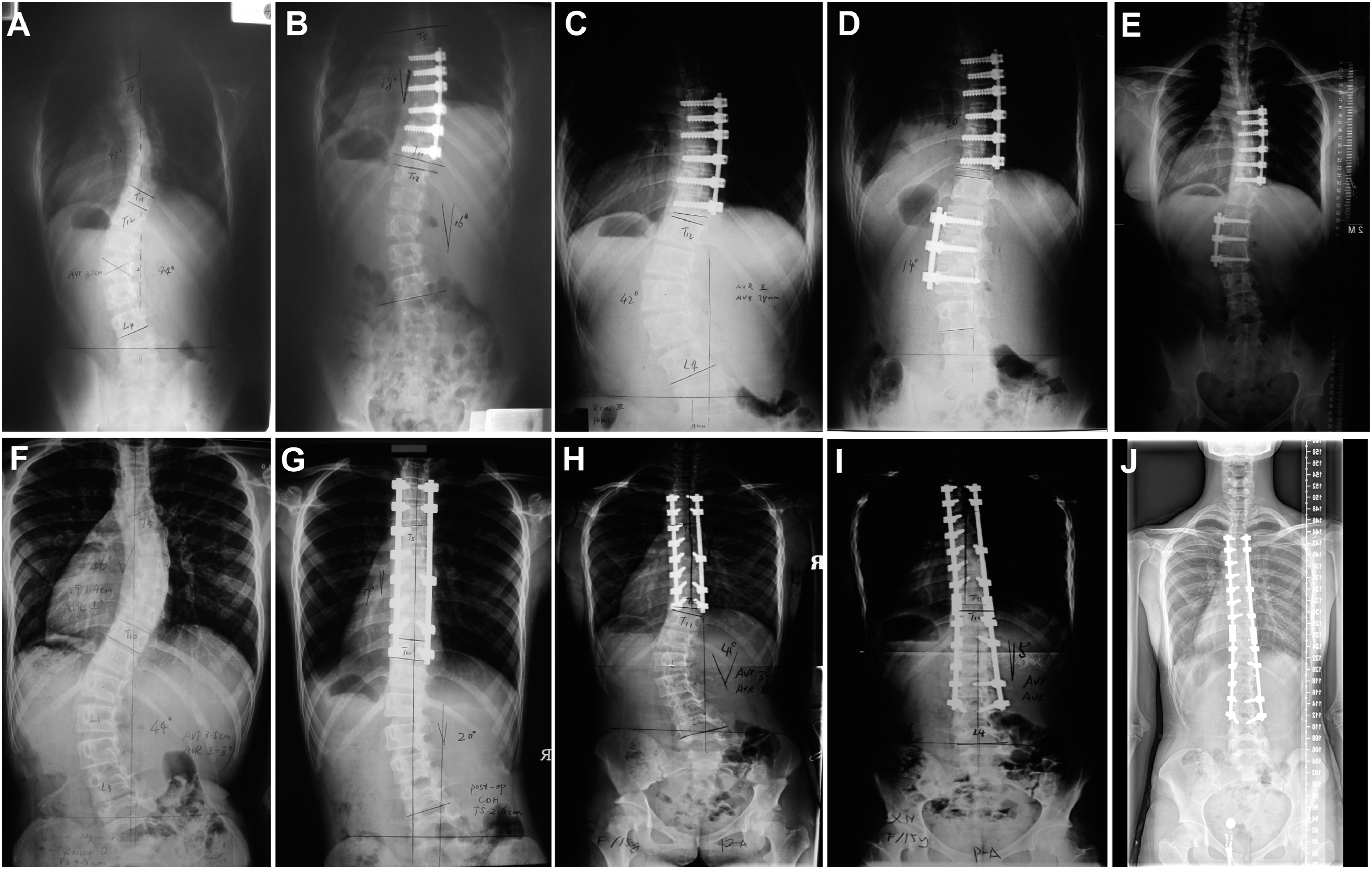
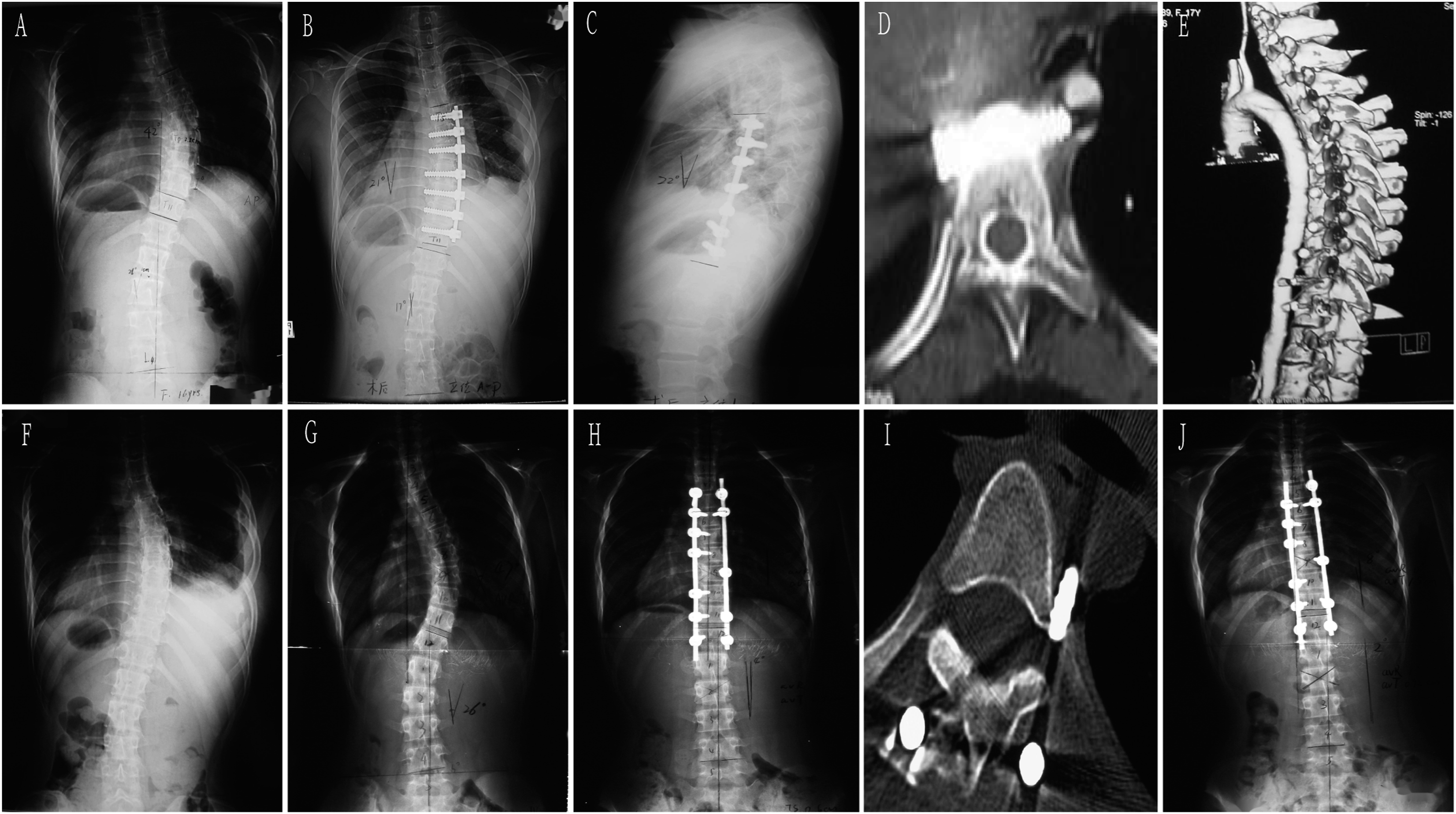
By analyzing the time distribution of the causes of revision, it was found that the main causes of early revision were poor wound healing or infection (7 cases, 13.7%). Malposition/failed internal fixation accounted for a high proportion in 3 months, 3 months-1 year and 1-2 years after operation. Revision for decompensation/adding on/proximal junction kyphosis mainly occurred 2-5 years after operation. The incidence of discomfort with implants was low, which mainly occurs during long-term follow-up (more than 10 years). (see Figure 2, Figure 3 and Figure 4) Time interval between primary surgery and revision surgery of different revision causes. Two typical revision cases of worsening of compensatory curve. Panel A: a 11-year girl with a thoracic curve 45 degree and lumbar curve 44 degree. Panel B:The patient underwent anterior selective fusion from T6-T11, the immediate postoperative Cobb angle of thoracic and lumbar curve were 18 degree and 16 degree respectively. Panel C-D: 2 years after the primary surgery, the lumbar curve increased to 42 degree and she underwent anterior revision surgery. Panel E showed 7 years after the revision surgery, a well balanced spine was maintained.Panel F: a 12-year girl with a thoracic curve 46 degree and lumbar curve 44 degree. Panel G:The patient underwent posterior selective fusion from T3-T10, the immediate postoperative Cobb angle of thoracic and lumbar curve were 7 degree and 20 degree respectively. Panel HI: 3 years after the primary surgery, the lumbar curve increased to 41 degree and she underwent posterior revision surgery. Panel J showed 6 years after the revision surgery, a well balanced spine was maintained. Panel A-C:A 16-year old girl underwent anterior correction with vertebral body screws. Panel DE: 1.5 year after the primary surgery, several screws were found too close to the aorta with no obvious symptoms. CTA demonstrated filling defect of the aorta. Panel F:The implants were all removed in the revision surgery.Panel G-I:A 13-year old girl underwent posterior correction with pedicle screws. The immediate postoperative X-ray revealed malposition the left T5 screw and the CT scan showed the tip of the screw was next to the aorta. She underwent revision surgery and the screw was removed.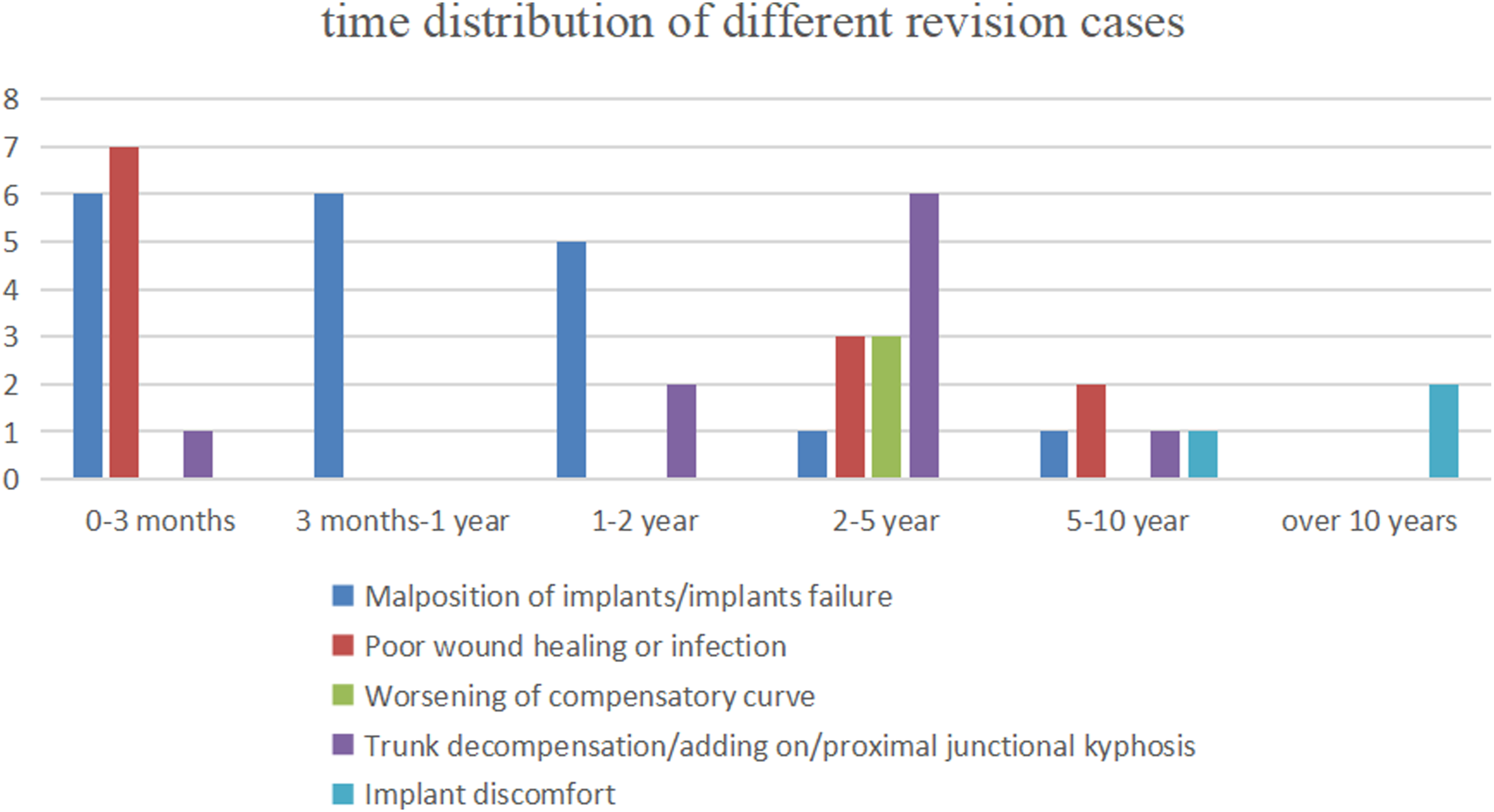
Discussion
Adolescent idiopathic scoliosis is the most common type of scoliosis. For the cases where the conservative treatment of scoliosis is ineffective, spinal fusion can stabilize the spine and reduce the cardiopulmonary dysfunction and social disorder caused by severe scoliosis. However, AIS surgery still has certain risks and complications, and some complications need revision surgery. Analyzing the incidence of revision surgery is of great significance to prevent complications and improve the safety of surgery.
Bartley et al 6 reported the perioperative and long-term complications of 3582 cases of AIS from 1995 to 2014, the incidence of perioperative complications was 2.6%. After a minimum of two years follow-up, the rate of main complications and revision surgery were 4.1%. The most commonly seen complications were wound related (1.9%) and implants related complications (0.8%). The cases we included were those after 2002 in order to exclude too old cases, and the results have more practical significance. Dannenbaum et al. 7 followed up 411 AIS patients for at least 2 years, and the revision rate was 12.2%. Symptomatic implants, pseudoarthrosis and infection were the most common causes. Among them, the revision rate of pedicle screw was the lowest (5.8%), and the revision rates of anterior and combined approaches were 10% and 20.8% respectively. Ramos et al. 8 analyzed 36335 AIS cases from 2002 to 2011, and the overall complication rate was 7.6%. The incidence of complications of posterior, anterior and combined approaches were 6.7%, 10.0% and 19.8% respectively. Ahmed et al. 9 followed up the “survival rate” of 1435 AIS cases from 1995 to 2009, that is, the proportion of patients who did not undergo revision surgery. The results showed that the revision rate was 5.2%. Campos et al. 10 reported 485 cases of AIS, and 4.9% of the patients needed unplanned reoperation. Luhmann et al. 11 reported 1057 cases of idiopathic scoliosis, with a revision rate of 3.9%. Our group of cases focused on cases with serious complications requiring revision surgery. The overall revision rate was slightly lower than that in the above literature. There were two reasons for our relative lower revision rate. Firstly, we only included patients after 2002, and we believe that the reduction may be attributed to the technique and instrumentation progress. Secondly, some recent cases still require a longer follow up. Although the revision rate of anterior surgery was higher than the posterior, there were no Lenke 5 cases in the anterior revision cases. This phenomenon implies that the main indication for anterior surgery may be Lenke 5C AIS curve. 12
Malposition/failed internal fixation was the most common cause of revision in our group. The literature reported that the incidence of fracture or displacement of internal fixation was 1.2% - 2.5%. 13 However, the revision rate may be underestimated as some internal fixation displacement didn’t show clinical symptoms. Although injuries of the aorta in spine surgery are rare, they may be life-threatening. 14 CT scan of 20 cases of anterior internal fixation found that 15% of the vertebral screws were less than 2 mm from the aorta. All screws were followed up for 4.1 years without any clinical symptoms. 15 In this group of cases, we reported two cases of screws adjacent to the aorta, both of which were removed. In recent 10 years, posterior pedicle screw fixation has become the mainstream. It can provide better correction rate and derotation force, and the revision rate is relative lower. The incidence of pedicle screw malposition is still high. Kwan reported 140 cases of AIS and found that lateral wall perforation was the most common type. 16 Although most cases didn’t show clinical symptoms, it was still recommended to remove the screw if the position of the screw was found too lateral and the distance from the aorta was less than 5 mm on CT images, because there was a risk of delayed erosion of the aorta. Some scholars suggest that 4 mm can be used as a safe range for the partial invasion of the spinal canal, but there is still a great risk in the concave side, because the spinal cord is close to the concave pedicle. 17
Poor wound healing or infection is the second leading cause of revision. The literature reported that the infection rate in AIS was 0.5% - 4.5%.18,19 Generally speaking, internal fixation should be retained in case of acute infection, because once the internal fixation is removed, it will be at the cost of losing correction. Whether to retain the bone graft material is still uncertain. Our experience is that loose allogeneic bone material should be removed during debridement and replaced with new bone graft material after complete debridement. In this series of cases, there were 7 cases of acute infection, all of which were treated with debridement and internal fixation were retained. 6 cases were successful, and 1 case underwent repeated debridement and implants removal. There were 5 cases of delayed infection, with an average time of 4 years after operation. Debridement combined with internal fixation removal was still the gold standard of treatment. According to the literature, the risk factors of delayed infection include long operation time, complicated with basic diseases, blood transfusion, no wound drainage and so on. 20 Decompensation of trunk, adding on phenomenon, proximal junctional kyphosis and aggravation of compensatory curve were another series of major causes of revision. The time of occurrence was generally 2-5 years after the initial operation. The main causes were the continuous growth of the spine and the improper selection of fusion segments. The main way of revision was to extend the fixed segment.
This study has the following shortcomings: firstly, the time span is long. With the progress of internal fixation technology, the treatment technology and concept have changed, and some instruments and surgical methods are no longer used. Secondly, some cases lack long-term follow-up results, which may underestimate the incidence of some complications, so further long-term follow-up data are still needed. Thirdly, due to the overall low incidence of complications, it is impossible to analyze the risk factors.
Conclusions
The overall revision rate of spinal fusion for AIS is 2.8%. The implants and incision problems were the most common causes of revision surgeries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the fundamental research funds for the central universities No.3332021013.