
Abstract
Study Design
Retrospective study
Objective
Our purpose was to evaluate spinal rotation measurement by scoliometer or EOS Imagings with reference to that by CT images, and to clarify their applicability in clinical practice.
Methods
Patients with adolescent idiopathic scoliosis (AIS) who were indicated for surgery were enrolled and the informed consents were obtained. The angle of trunk rotation (ATR) was measured by the scoliometer. Apical vertebral rotation (AVR) was measured with EOS Imaging and CT images. Paired T tests were used to compare the measurements between ATR or AVR-EOS and AVR-CT. Pearson correlation analysis was performed to explore the relationship between ATR or AVR-EOS and AVR-CT. Then subgroup analysis was performed.
Results
Forty-seven consecutive AIS patients with 62 curves were identified. In the whole group, the ATR, as well as AVR-EOS, was significantly smaller than the AVR-CT. Both ATR and AVR-EOS correlated with AVR-CT, although AVR-EOS correlated better. In thoracic group, there was no significant difference between ATR and AVR-CT (P = .236). A significant correlation was found between ATR and AVR-CT(r = .574, P < .001). In TL/L group, no significant difference was noted between AVR-EOS and AVR-CT (P = .414), and a significant correlation was found between AVR-EOS and AVR-CT(r = .824, P < .001).
Conclusion
ATR by scoliometer is numerically similar to AVR by CT and may evaluate the spinal rotation more appropriately in thoracic spine. AVR by EOS is numerically similar to AVR by CT and may be more applicable in TL/L spine. Appropriate methods could be selected according to the location of the curve.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) is a three-dimensional (3D) deformity of the spine that predominantly affects individuals of ages 10 to 17. Traditionally, Cobb angle is the primary measurement used to quantify the severity of AIS. However, this metric is limited to assessments of the spine in the coronal and sagittal planes.
More recent studies of vertebral rotation in the axial plane have provided a better understanding of AIS as a 3D condition. The rotation of vertebrae is part of the unknown pathogenic mechanism that leads to scoliosis 1 . It is very important to investigate vertebral rotation in classification and predicting the outcome of scoliotic curves. 2 Vertebral rotation essentially causes an asymmetric back prominence. Although the primary goal of the operative treatment in AIS is to stop curve progression, patients expect more improvements, primarily improved cosmesis. 3
Numerous methods based on different types of imaging, including X-ray, ultrasound, and computed tomography (CT) images, magnetic resonance imaging (MRI) and EOS Imaging, have been developed to evaluate vertebral axial rotation. Meanwhile, the scoliometer is widely used in clinical practice for the measurement of angle of trunk rotation (ATR). The purposes of the present study were to evaluate spinal rotation measurement by scoliometer or EOS Imagings with reference to that by CT images, and to clarify their applicability in clinical practice.
Materials and Methods
The study protocol was approved by our institution’s ethics review board. A retrospective enrollment process was performed to identify patients with AIS that were admitted to a single institution between March 2018 and December 2019 and received surgical intervention. The written informed consents were obtained before surgery for retrospective researches. The inclusion criteria were as follows: (1) diagnosed with AIS, (2) underwent EOS Imaging of the spine, (3) had ATR measured by the scoliometer, and (4) had CT images taken during the same period. The exclusion criteria were as follows: (1) scoliosis of other etiologies, (2) patients who were not surgically indicated because the relatively flexible spine may exacerbate the influence of postures.
The ATR (in degrees) were measured using the scoliometer in conjunction with Adam’s forward-bending test when the patient stood and flexed forward at the hips. The region of measurement included the thoracic and thoracolumbar/lumbar(TL/L) spine. The proximal thoracic spine was excluded because of the inaccurate measurements. Curves were excluded if the corresponding ATR was less than 5°.
EOS images were obtained by the EOS System(EOS Imaging, Paris, France) in a slot-scanning radiologic device that scans the posteroanterior (PA) and lateral planes simultaneously. 4 SterEOS software (Version: 1.6.5.8188, EOS Imaging, Paris, France) was utilized by experienced operators to simulate 3D spine reconstructions. The pelvis was defined first, and then the end and apical vertebrae of the target curves were identified on the EOS 2D (two-dimensional) images. Three-dimensional measurements were taken with fast 3D-guided processes. The accuracy of this methodology has been previously established 5 . The Cobb angle and apical vertebral rotation (AVR-EOS, in degrees) of the selected curves were generated spontaneously after 3D reconstruction.
CT images of the whole spine were obtained by low-dose CT scans using an Aquillion 64 system (Toshiba Medical Systems, Tokyo, Japan). We measured apical vertebral rotation on CT images (AVR-CT, in degrees) according to the method reported by Aaro-Dahlborn.
6
The AVR-CT was adjusted by the sacral rotation angle to eliminate the influence of whole-body rotation during the CT scanning.
7
All measurements were performed twice by two senior authors and then the mean value was used. In addition, subgroup analyses were performed by separating thoracic curves from TL/L curves.
Statistical Analysis
We calculated overall summary statistics in terms of means and standard deviations (SDs) for continuous variables such as ATR and AVR. Comparison was made between ATR and AVR-CT, as well as between AVR-EOS and AVR-CT using paired T tests. Pearson correlation analysis was performed to evaluate the relationship between ATR and AVR-CT, as well as between AVR-EOS and AVR-CT. The strength of correlation was defined according to the corresponding r values: negligible correlation (r < .3), weak correlation (.3 < r < .5), moderate correlation (.5 < r < .7), strong correlation (.7 < r < .9) and very strong correlation (r > .9). Statistical analyses were conducted with IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA); P value <.05 was considered significant.
Results
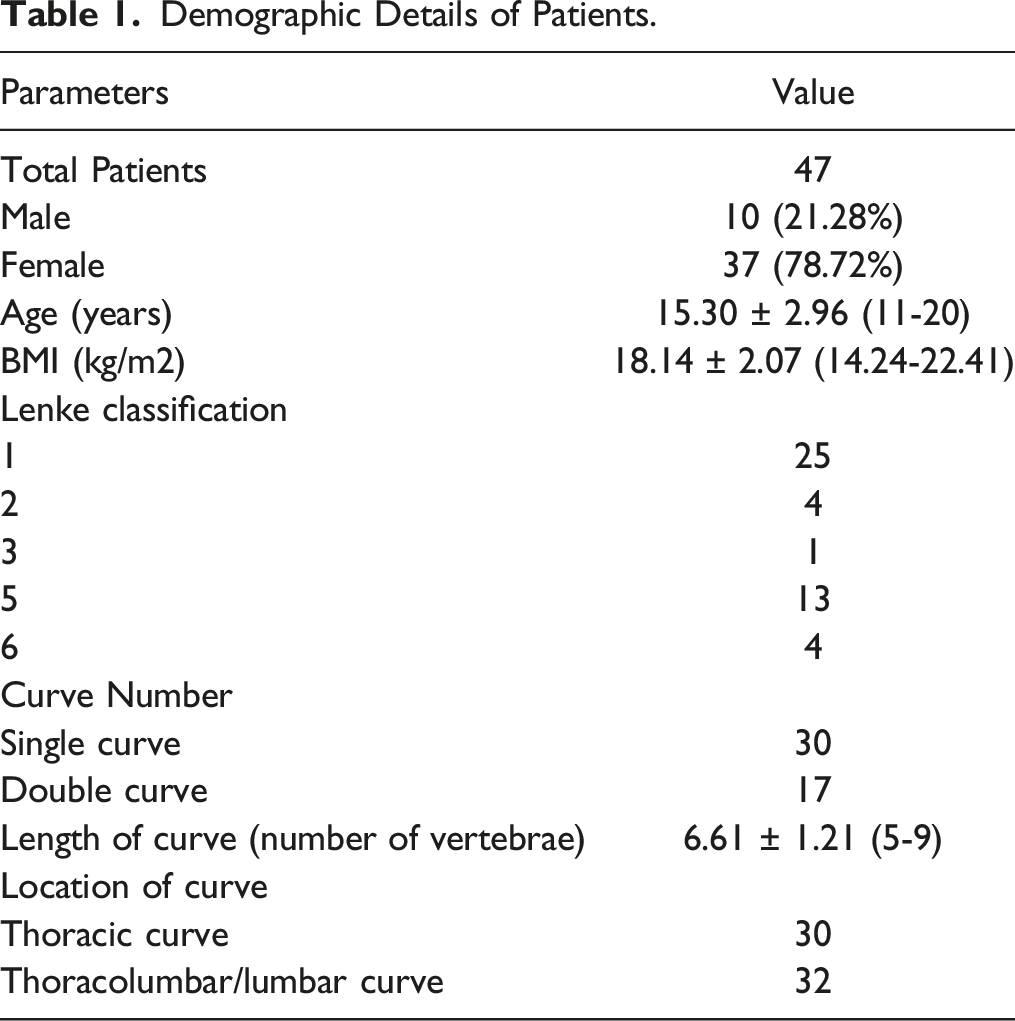
Demographic Details of Patients.
Measurements of Rotation Value and Comparisons between AVR-CT and ATR or AVR-EOS.
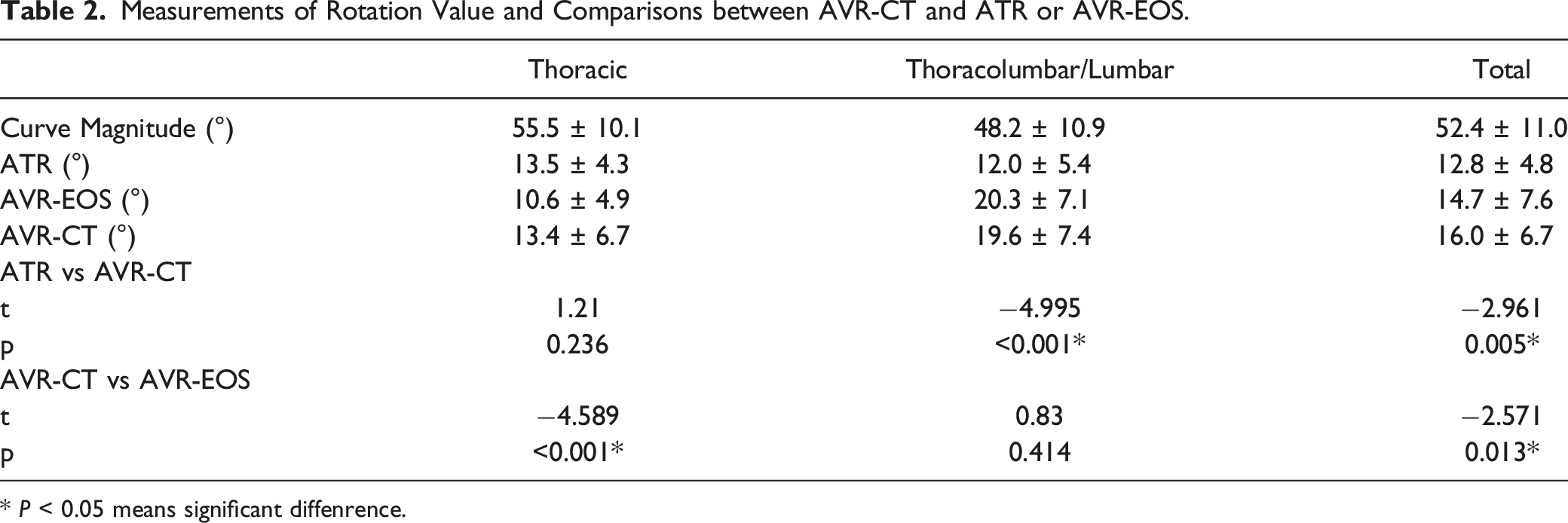
* P < 0.05 means significant diffenrence.
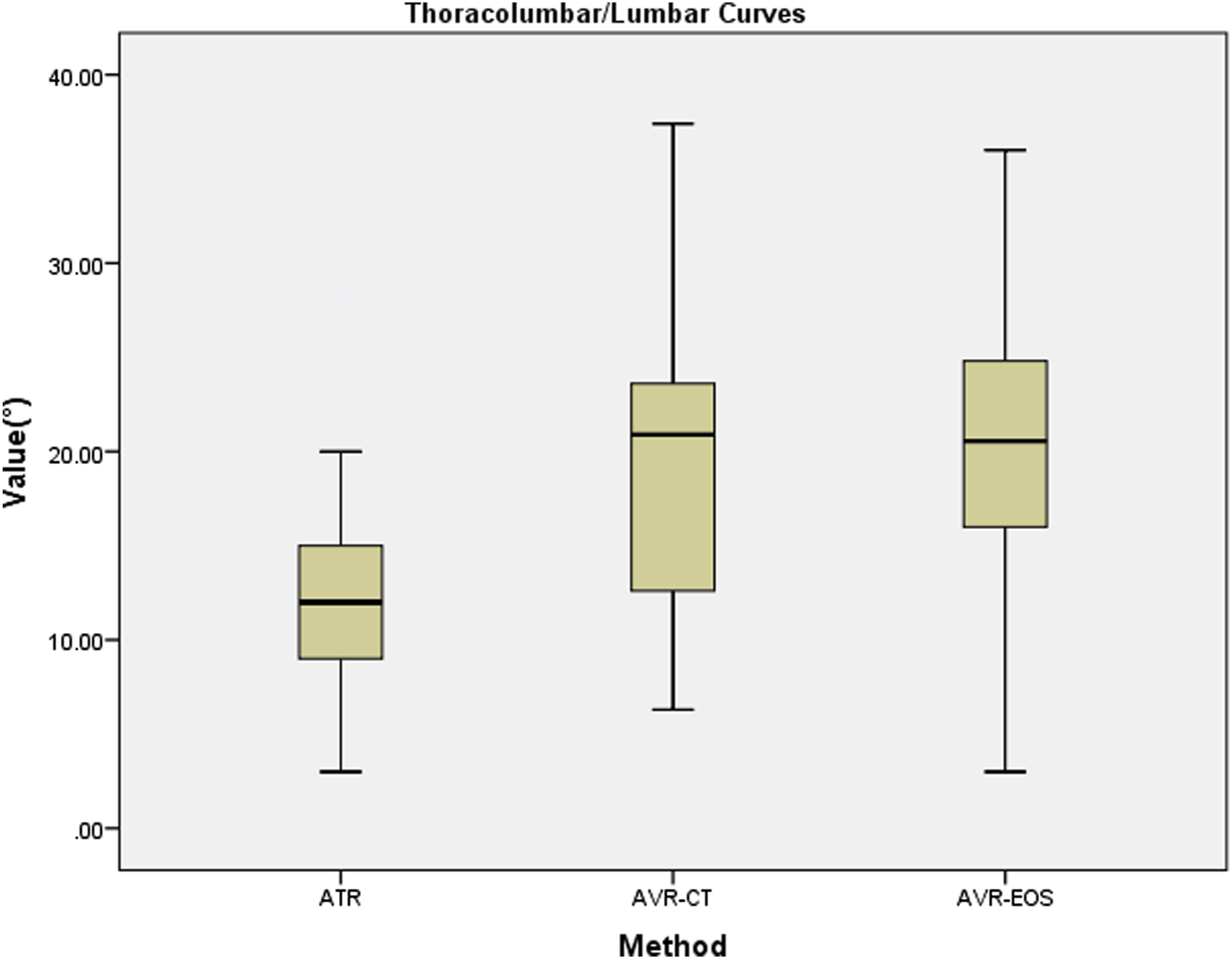
In subgroup analysis, thirty-six thoracic curves and twenty-six TL/L curves were identified and grouped. In thoracic group, AVR-EOS was significantly smaller than AVR-CT, and there was no significant difference between ATR and AVR-CT (Figure 1). Meanwhile, in TL/L group, ATR was significant smaller than AVR-CT, and no significant difference was noted between AVR-EOS and AVR-CT (Figure 2). A boxplot of the different methods used to measure the thoracic curves. A boxplot of the different methods used to measure the thoracolumbar/lumbar curves.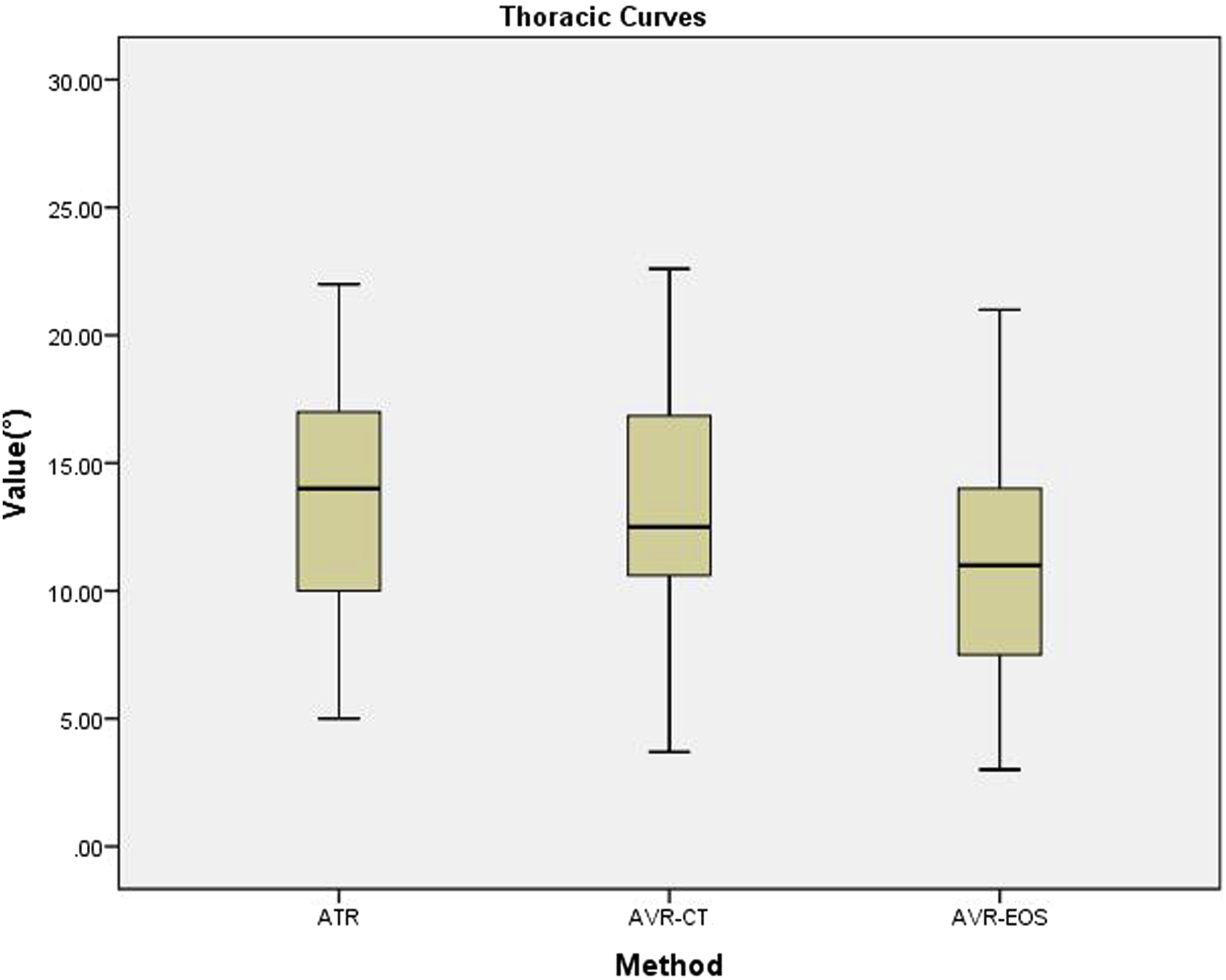
Correlation Analyses between AVR-CT and ATR or AVR-EOS.
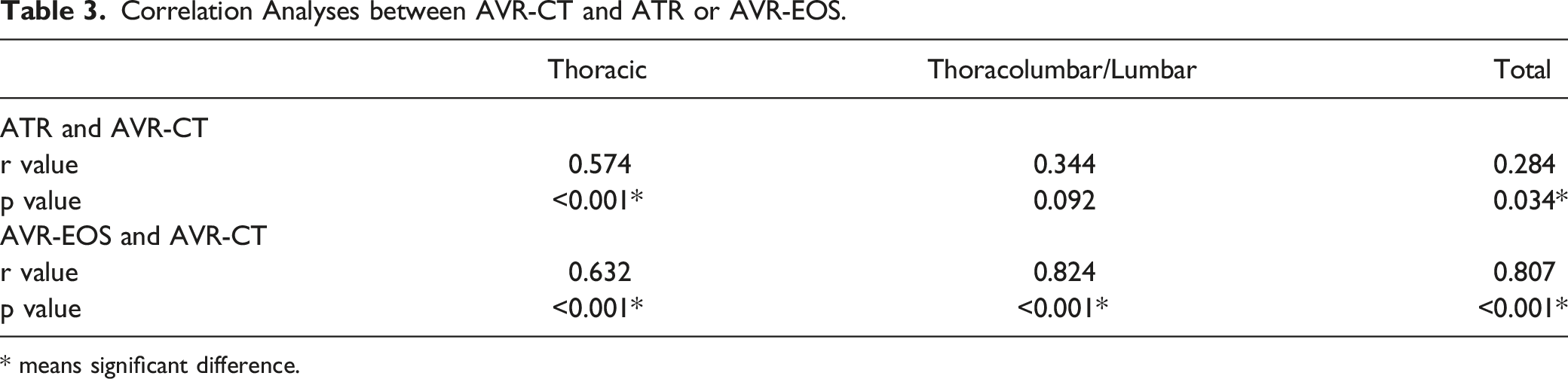
* means significant difference.
Discussion
AIS is a 3D spinal deformity that affects the orientation of the involved vertebrae, with the most severe rotation being in the apical vertebrae. A direct nonlinear relationship among the coronal, sagittal and axial parameters of the spinal deformity has been revealed. 8 . Despite the difficulty in measuring axial deformities, vertebral rotation is thought to be an important aspect of global spinal alignment. 9 It clinically manifests as a thoracic rib hump and lumbar prominence that becomes accentuated during the forward-bending test. 10
The scoliometer, which measures back asymmetry by ATR, is 1 of the most convenient tools in evaluating the axial deformity in AIS. 11 However, the error associated with scoliometer-based measurements can be as high as 4.9°, irrespective of the region of the spine examined. 12 On the other hand, measurements based on X-rays mainly include Nash-Moe method, Perdriolle method and Stokes method. They are indirect methods based on the position of posterior elements of the spine 13 . The measurement error is marked implied by the low repeatability and reliability on X-rays 7 . Another limitation of the methods above is that the vertebral rotation is assessed relatively to the radiographic sagittal plane, without pelvic rotation taken into consideration. Recently, advanced technology, such as machine learning and artificial intelligence, has been applied to analyze vertebral rotation in images, but it still needs further researches. 14 In addition to the methods above, real-time ultrasound, CT and MRI are used to measure vertebral rotation directly.
CT images are the golden standard in assessing vertebral rotation and other skeletal measurements because of its clearly defined reference points, high measurement accuracy and high inter-observer reliability. 5 But routine CT scans are not a viable option because of high-dose radiation exposure. Measurements based on MRI are similar to those by CT images, while MRI is uneconomical, and MRI scans are not performed routinely in the clinic. 15
More recently, vertebral rotation was generated by an EOS system after a 3D reconstruction of the whole spine was created 16 . EOS systems have the advantages of minimal radiation exposure, enabling scans to be performed in a weight-bearing upright position, and enabling modest 3D reconstruction models to be made, which increases their potential to be used in 3D studies in routine clinical care. 17
Al-Aubaidi et al. 18 enrolled 7 scoliosis patients with various etiologies and measured AVR with both EOS and CT images. There was no significant difference between AVR-EOS and AVR-CT. However, the sample size was too small and the etiological heterogeneity should not be neglected. The authors did not investigate correlations between different methods and no subgroup analysis was made. Pankowski et al. 19 determined that a significant discrepancy existed between ATR and intraoperative AVR-CT, and there was no significant correlation between the measurements taken with the 2 methods. In our study, the ATR was significantly different from the AVR-CT in the whole group, similar to Pankowski’s results. But the AVR-EOS was also significantly different from the AVR-CT, inconsistent with Al-Aubaidi’s research. Discrepancy among 3 measurements was reasonable because of the different positions in 3 different methods: supine in CT machines, standing upright in EOS devices and bending forward for the scoliometer. Thus, subgroup analysis was needed to specify the influence of positions.
Jankowski et al. 11 measured the AVR of 55 AIS patients with the scoliometer and EOS Imaging. The authors identified a significant correlation between ATR and ATR-EOS both in the lumbar curves and the thoracic curves. However, no CT measurements were taken as a reference. Krawczynski et al. 20 observed a positive correlation between ATR and radiographic (Perdriolle angle of rotation) measurements of rotation in the axial plane. They also found that the correlation was stronger for thoracic curves than lumbar curves. In our subgroup analysis, consistent to Krawczynski’s results, ATR was similar to AVR-CT (P = .236) and correlated with AVR-CT(P < .001) in thoracic group. On the other hand, AVR-EOS was similar to AVR-CT (P = .414) and correlated better with AVR-CT (r = .824, P < .001) in TL/L group. Based on above, ATR by scoliometer was more accurate in thoracic spine than that in TL/L spine, while AVR by EOS was more accurate in TL/L spine than that in thoracic spine.
The reason for the conclusion above was unclear but our potential explanations were as follows: first, the amplification of lateral rib extension. The bilateral ribs helped make measurement of scoliometer more feasible in thoracic region. While in lumbar region, back muscle hump was not as prominent as rib hump. Second, number of bony landmark and thinner posterior soft tissue in adam’s test. The back muscles, as well as the skin and subcutaneous tissue, were thinner when being stretched in forward bending position. In this condition at least 2 bony structures (bilateral ribs) were more prominent in thoracic region, and the scoliometer was more applicable with 2 bony landmarks. But in lumbar region, there was only 1 bony structure (median spinous process), which make scoliometer less applicable. Besides, the relatively inaccurate EOS 3D reconstruction in thoracic region. Obscured by ribs, costovertebral joints and costotranverse joints, measuring error was unavoidable and may be exaggerated in 3D reconstruction of thoracic spine. While in lumbar spine without ribs, costovertebral joints or costotranverse joints, this obscureness was less and the EOS 3D reconstruction was more accurate. Lastly, different rotation in different positions. In supine position within CT machine, the pressure on rib hump from CT machine bed may derotate thoracic vertebral column of the relatively flexible adolescent idiopathic curves, and this may amplify the difference of thoracic rotation between standing position in EOS machine and supine position in CT machine. However, without the derotation effect of rib hump on lumbar segments, as well as less contact between lordotic lumbar region and CT machine bed, change of lumbar rotation was less between standing position in EOS machine and supine position in CT machine. Nonetheless, these were just assumptive interpretation, and it still needs further explorations.
Limitations
One potential limitation of this study is the relatively small sample size, so a larger sample size may be further needed. Another limitation is that ATR by scoliometer and AVT-EOS by EOS 3D reconstruction are susceptible to operators’ subjectivity, but the measurements in present study were performed by experienced hands.
Strengths
First of all, no previous research elaborated the specific application of scoliometer and EOS imaging in evaluating spinal rotation. Secondly, although discrepancy of measurement results existed in the whole group, subgroup analysis detailed the relationship among them. Finally, the scoliometer is 1 of the most common and most convenient methods used in clinical practice. We specified its limited application in AIS lumbar curves.
Conclusion
In conclusion, the present study showed the comparison of 2 different methods in evaluating spinal rotation. ATR by scoliometer is numerically similar to AVR by CT and may evaluate the spinal rotation more appropriately in thoracic spine. On the other hand, AVR by EOS is numerically similar to AVR by CT and may be more applicable in TL/L spine. If EOS Imaging is not available when evaluating vertebral rotation is essential in TL/L spine, CT images may be indicated after serious consideration of its benefits and drawbacks. Drawbacks of different methods should not be underestimated. Appropriate methods could be selected according to the location of the curve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wu Jieping Medical Foundation (320.6750.2021-20-2, held by Bin Xiao), CAMS Innovation Fund for Medical Sciences (CIFMS) (2021-I2M-5-007, held by Wei Tian) and Beijing Health Technologies Promotion Program (BHTPP202001, held by Wei Tian).
IRB Approval/Research Ethics Committee
The study has got the IRB approval, IRB Approval No. 202201-25 from Ethics Committee of Beijing Jishuitan Hospital