
Abstract
Study Design
Retrospective cohort study using PearlDiver database.
Objectives
To evaluate the effect of prior thyroidectomy on complications of Anterior Cervical Discectomy and Fusion (ACDF) surgery.
Methods
PearlDiver was used to identify patients without prior dysphagia or dysphonia undergoing ACDF between the years 2010-2020Q1. Patients with and without prior thyroidectomy were matched by levels of fusion, alcohol use, and gastroesophageal reflux disease in a 1:5 ratio. Postoperative outcomes were assessed for each cohort with multivariable logistic regression, controlling for age, sex, and Elixhauser Comorbidity Index.
Results
Between 2010 and 2019, matched cohorts of 792 ACDF patients with prior thyroidectomy and 3960 ACDF only patients were included in the study. Of patients with previous thyroidectomy undergoing ACDF, 16.3% experienced dysphagia at 1-year compared with 10.6% for patients undergoing ACDF only (aOR=1.39, P=.004). Patients with previous thyroidectomy also had higher odds of dysphonia at 1-year following ACDF, as compared to patients with ACDF alone (2.7% vs 1.2%, aOR=1.74, P= .048). Patients undergoing ACDF with prior thyroidectomy did not have increased risk of revision at 1 year (aOR=1.10, P=.698), 2 years (aOR=1.16, P=.457), or 5 years (aOR=1.20, P=.255) following surgery. There were no differences in postoperative opioid utilization rates at 1 month (aOR=2.07, P=.138), 3 months (aOR=2.45, P=.095), 6 months (aOR=1.34, P=.520), and 12 months (aOR=1.69, P=.202). Prior thyroidectomy was not associated with reintubation following ACDF (P=.995).
Conclusions
Patients with prior thyroidectomy undergoing ACDF surgery experience increased odds of dysphagia and dysphonia at 1-year follow-up compared to those without prior thyroidectomy.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) surgery has long been a common treatment option for cervical radiculopathy and myelopathy. Utilization of ACDF has increased as much as 400% in recent decades. 1 Dysphagia and dysphonia are well known complications of anterior cervical surgery. Reported rates of postoperative dysphagia following ACDF vary greatly and have ranged from 1% to 79%. 2 The variability of these rates is largely due to evaluation at different postoperative time periods and the lack of a standardized measure of dysphagia.2,3
Thyroidectomies are also commonly performed procedures that occur adjacent to the surgical field of a typical ACDF. From 2000 to 2014, the proportion of thyroidectomies vs. lobectomies increased from 78.16% in 2000 to 85.67% in 2014. 4 Undergoing a thyroidectomy prior to an ACDF may alter virgin tissues of the neck, promoting scar formation and creating a revision environment for a primary ACDF. A prior thyroidectomy can therefore theoretically make an otherwise routine ACDF more susceptible to complication. However, no studies have previously investigated this theoretical relationship.
The purpose of this study was to examine whether a prior thyroidectomy affects complication rates for ACDF, specifically regarding dysphagia and dysphonia. We hypothesize that the consequences of a prior thyroidectomy will increase the risk of dysphagia and dysphonia after ACDF surgery. Furthermore, a secondary analysis of revisions, opioid use, and common medical complications is useful to determine whether ACDF surgery with prior thyroidectomy is associated with complications in general.
Methods
Database
This retrospective cohort study was conducted using data from the Mariners dataset from the PearlDiver Patient Records Database (Colorado Springs, CO; www.pearldiverinc.com). The dataset contains deidentified insurance claims information from over 144 million patients in the United States from 2010 through the first quarter of 2020. Institutional review board approval was not necessary as the data was deidentified. This information was sourced from all payer types, including commercial insurance, Medicare, Medicaid, and self-pay. ICD-9, ICD-10, and Current Procedural Terminology (CPT) codes were used to retrieve patient records.
Study Groups
Patients undergoing ACDF without pre-existing dysphagia or dysphonia were identified via CPT codes (Appendix A). Two cohorts were identified, those with and those without prior thyroidectomy. Inclusion criteria for thyroidectomy included partial thyroid lobectomy, total thyroid lobectomy, partial or complete thyroidectomy, resection of left and right thyroid glands, partial and complete substernal thyroidectomy, and other criteria as determined by the CPT, ICD9, and ICD10 codes included in the dataset (Appendix B). The distribution of number of levels of fusion (based on CPT code, CPT-22845, CPT-22846, or CPT-22847), and comorbidities, specifically smoking, alcohol use, GERD, and systemic sclerosis, were compared through Chi-squared analysis between cohorts. Those with differences significant to P < .15 were included in a matching algorithm that used a 1:5 ratio between patients with and patients without prior thyroidectomy (Appendix C).
Postoperative Complications
Patients undergoing ACDF were evaluated for post-operative complications in both groups: ACDF with prior thyroidectomy and ACDF without prior thyroidectomy. Postoperative outcomes included dysphagia, dysphonia, revision ACDF, readmission, surgical site infection, deep vein thrombosis (DVT), implant-related complications, reintubation, spinal cord injury, plexus injury, sepsis, pneumonia, other respiratory complications, and prolonged opioid use (Appendix D).
Statistical Analysis
Multivariable logistic regression, controlling for age, sex, and Elixhauser Comorbidity Index (ECI), was used to calculate odds ratios (aOR) and 95% confidence intervals for the rates of postoperative complications, between the two cohorts. For comparison of opioid utilization, regression also controlled for pre-operative opioid use. A P-value of .05 was set as the level of significance. All statistical analysis was conducted using the R statistical software integrated within PearlDiver.
Results
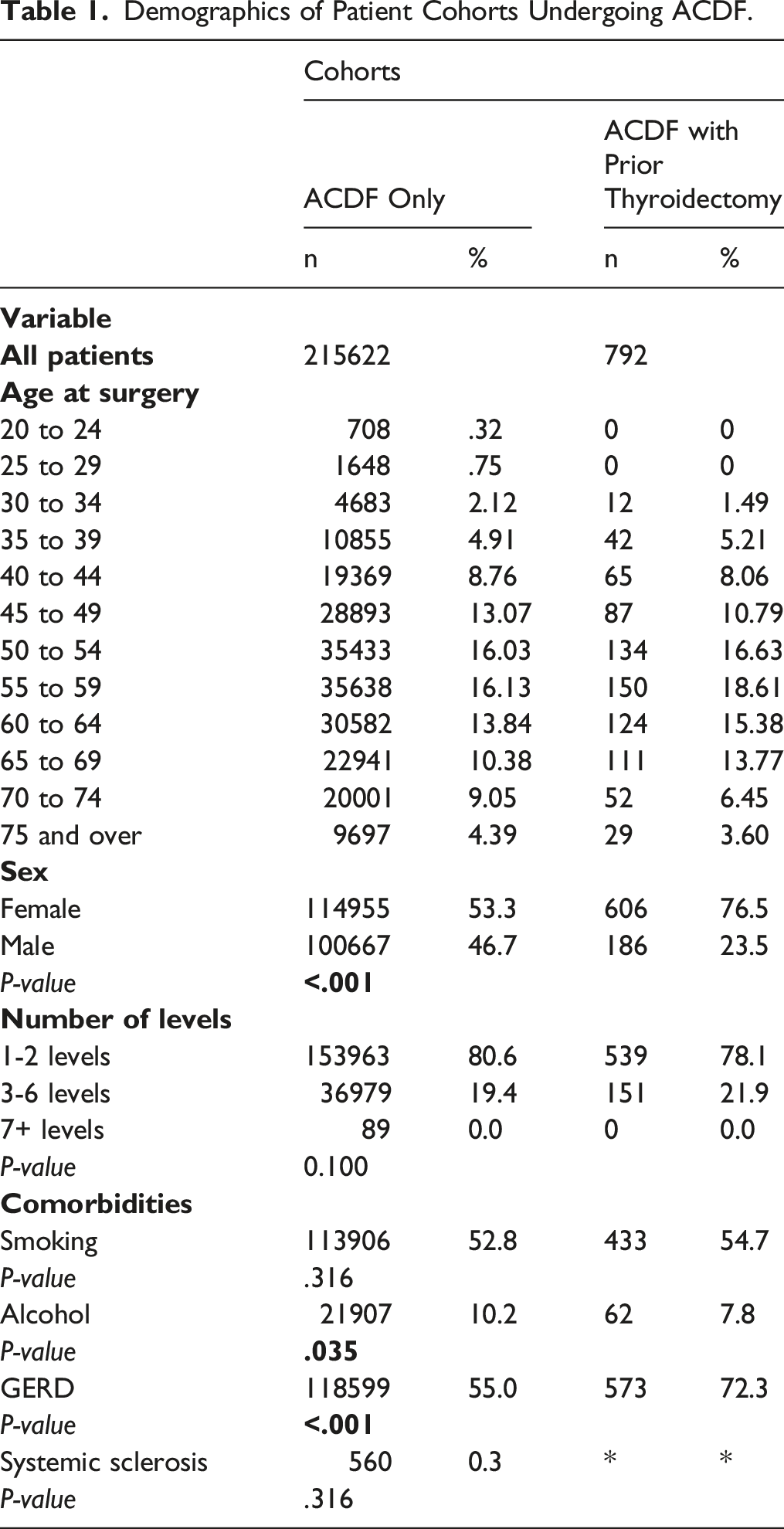
Demographics of Patient Cohorts
Demographics of Patient Cohorts Undergoing ACDF.
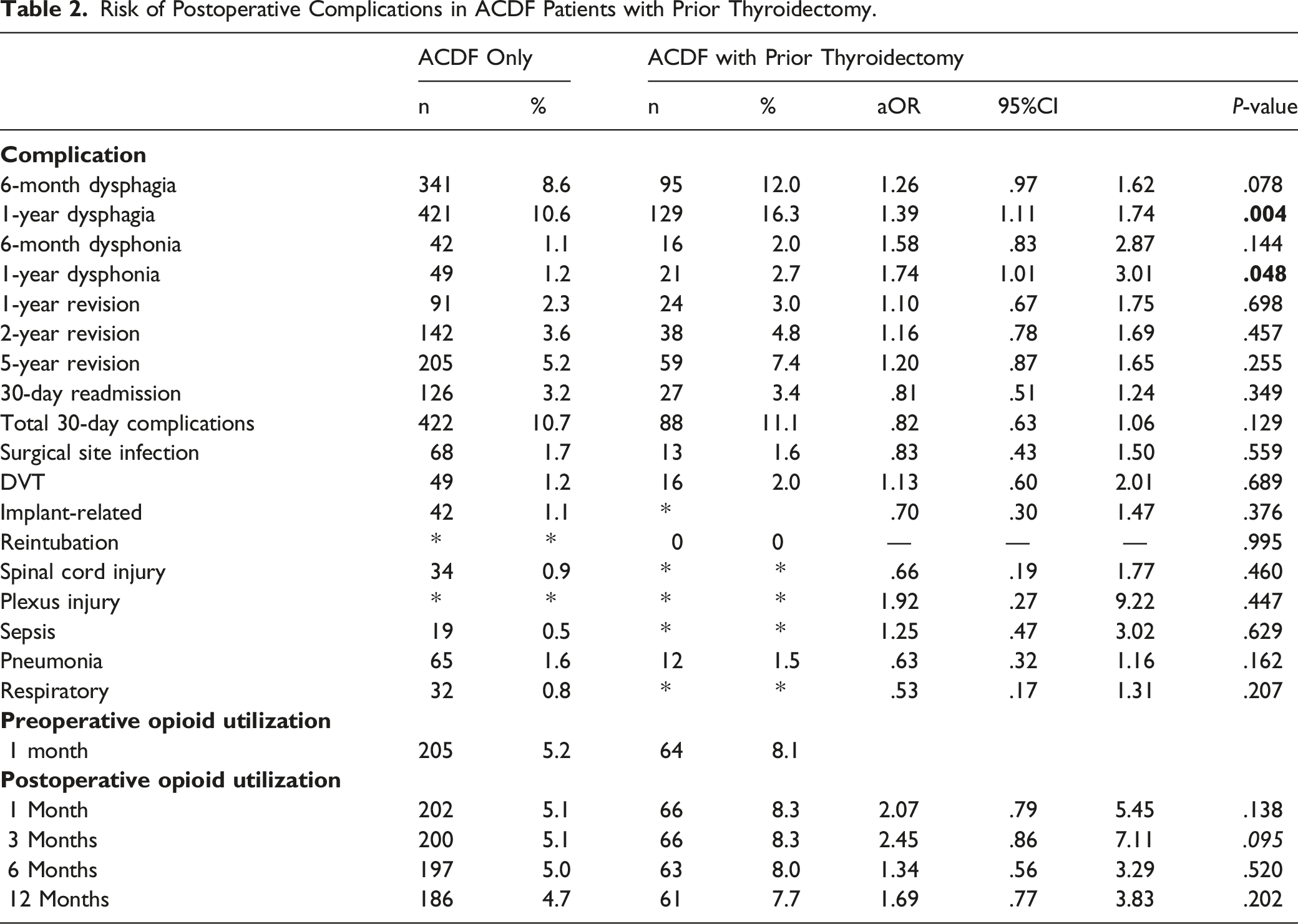
Dysphagia/Dysphonia in Patients With Prior Thyroidectomy
Risk of Postoperative Complications in ACDF Patients with Prior Thyroidectomy.
Revisions, Medical Complications, and Opioid Utilization in Patients With Prior Thyroidectomy
Patients who underwent ACDF without prior thyroidectomy had revision rates of 2.3%. 3.6%, 5.2% at 1-year, 2-years, and 5-years, respectively. Patients who underwent ACDF with prior thyroidectomy had revision rates revision of 3.0%, 4.8%, and 7.4% at 1-year, 2-years, and 5-years, respectively. These rates were not significantly different between cohorts (P>.05 for all, Table 2).
There were no significant differences in 30-day readmission (aOR=.81, P=.349), and total 30-day complications (aOR=.82, P=.129)
Discussion
This investigation examined the effect of an antecedent thyroidectomy on ACDF surgery and the risk of dysphagia and dysphonia. Conventional thyroidectomy typically consists of a midline transverse incision between the sternal notch and cricoid cartilage. Approach to the thyroid entails a central dissection through the platysma and then between the sternohyoid and sternothyroid muscles, with dissection laterally past the lateral border of the sternothyroid and ansa cervicalis. 5 In ACDF surgery, exposure for caudal levels such as C6, C7, and T1 may require retraction or division of these strap muscles in order to adequately visualize the surgical field. With overlap of anatomical structures and their intimate relationship with the recurrent laryngeal nerve (RLN), a primary ACDF can potentially become more complicated by a prior thyroidectomy.
Dysphagia and dysphonia are well described complications of ACDF. The etiology of dysphagia is multifactorial, with one possible cause including irritation, compression or injury to the RLN. 3 The rate of dysphagia is reported as high as up to 71% of ACDF surgeries, although this may occur at different time points. 6 In a study of 47 patients, 83.0% and 59.6% of ACDF patients experienced postoperative dysphagia at 1-week and 1-month, respectively. 7 In a separate literature review of 14 studies containing a total of 1336 patients, dysphagia rate was reported as 19.8%, 7.0%, and 7.6% for postoperative follow-up intervals of less than 12-months, 12- to 24-months, and greater than 24-months, respectively. 2 Our study of 216 414 patients reported a 6-month dysphagia rate of 9.2% and a 1-year rate of 11.6%. This reveals that reported/recorded dysphagia may be more prevalent over time as a patient recovers from ACDF surgery. Establishing risk factors for dysphagia is important for surgeons to consider when counselling patients. In a prior study revision surgery was found to be twice as likely to cause dysphagia as compared to primary surgery, likely caused by increased scar burden. 8 Wong et al 9 also determined that prior thyroidectomy and number of levels addressed during surgery as risk factors for dysphagia. This study corroborates these findings by reporting prior thyroidectomy was associated with 1.4-fold greater risk of dysphagia at 1 year, even after matching for levels of fusion, comorbidities and controlling for age, sex, and ECI.
Dysphonia appears to be less common than dysphagia, occurring postoperatively in approximately 5% of ACDF cases, however reported rates vary widely from 1-70% of patients affected.6,10 This is supported by our study which also found lower rates of dysphonia compared to dysphagia at both 6-month and 1-year intervals across both groups. Dysphonia is also multifactorial and may be caused by pharyngeal swelling, laryngeal swelling, and injury to the RLN which may occur during retraction of soft tissue.11-15 Additionally, previous studies have shown that thyroid surgery may sometimes invoke permanent damage to the RLN, and therefore immobilization of the vocal cords.16,17 As with dysphagia, our study also demonstrated that previous thyroidectomy has increased odds of dysphonia at 1-year. To our knowledge, there are no prior studies that establish this association.
One prior study found that pre-operative opioid utilization was a novel risk factor for postoperative dysphagia and dysphonia after ACDF surgery. 18 Our study found that prior thyroidectomy was not associated with differences in postoperative opioid utilization. Regarding revision surgery, thyroidectomy may lead to anatomical changes, such as the presence of adherent strap muscles, and generalized scarring of the thyroid bed, which could make subsequent ACDF surgery more unpredictable and leave patients susceptible to longer term complications such as pseudarthrosis requiring revision. 4 However, the present study did not find differences in rates of revision ACDF between those with and without prior thyroidectomy. Furthermore, there were also no differences in medical complications of ACDF surgery after prior thyroidectomy, including short-term readmission. Reintubation is an infrequent yet disastrous complication which may occur following ACDF surgery due to airway compromise. 19 Our study did not find prior thyroidectomy to be a risk factor for this (P=.995).
Further research is needed to investigate other potential complications and long-term postoperative outcomes arising from ACDF surgery with prior thyroidectomy. Several studies have also demonstrated that peri-operative steroid use may reduce dysphagia after ACDF, especially in the early post-operative period.20,21 Therefore, this may be a useful management adjunct in ACDF patients with higher risk of dysphagia, such as prior thyroidectomy. It would also be prudent to investigate the severity and impact of dysphagia and dysphonia on the progression of patient recovery, which is not possible with billing database methodology. This could provide greater context when spine surgeons and patients weigh the risks and benefits of this procedure, as an increased risk of dysphagia and dysphonia may be acceptable if symptoms are minor in nature and do not significantly affect recovery. In addition, the mechanism by which a prior thyroidectomy increases the risk of developing dysphagia and dysphonia remains unclear and has not been investigated. Possible causes include increased scar tissue formation and injury or compression of the surrounding nerves due to repeated entry via the anterior approach. Understanding the exact causes of increased dysphagia and dysphonia due to prior thyroidectomy would be potentially beneficial, as spine surgeons could take appropriate precautions to minimize the risk that the patient develops these symptoms if ACDF surgery is indicated regardless of prior thyroidectomy. This is also particularly relevant when considering revision ACDF surgery. 22 In revision surgery, the other side of the neck tends to be used to avoid exploring a scarred surgical field and causing iatrogenic nerve injury. However, the effect of a prior thyroidectomy, and its sequalae on the surgical field and risk of complications, remains unclear in this circumstance.
As with all retrospective database studies, there are several limitations to consider for this study. Firstly, there may be inaccuracies in coding technique which could affect the representation of post-operative complications and limit the ability to capture all patients undergoing surgery. Additionally, the database does not include physical exam, imaging findings, surgical technique, levels specific to ACDF intervention, or perioperative steroid use which may be relevant for the ramifications of prior thyroid surgery. There may also be additional confounding factors which are unidentified in the regression analysis. The rates of reported dysphagia and dysphonia are surely underestimated by billing data, however, these data do likely represent patients with clinically significant dysfunction. Despite these limitations, this study is the largest known to establish an association between increased risk of dysphagia and dysphonia following ACDF surgery and prior thyroidectomy.
Conclusion
This study revealed an increased risk of dysphagia and dysphonia following ACDF surgery for patients with prior thyroidectomy. These findings appropriately contribute to the understanding of risk factors for dysphagia and dysphonia and can enable surgeons to effectively counsel patients with prior thyroidectomy undergoing ACDF surgery. Spine surgeons should be cautious when considering ACDF surgery for patients with prior thyroidectomy and in some may possibly consider posterior cervical fusion (PCF) as a viable alternative where indicated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
DA, JP, DY, AZ, CLM have no disclosures to report. EOK receives consulting fees from Seaspine, and Spineart. AHD receives consulting fees from Stryker, Orthofix, Spineart, and EOS, research support from Southern Spine, and Fellowship support from Orthofix.
Data Availability
Data for this project was obtained from the PearlDiver Mariner database (PearlDiver, Inc, Colorado Springs, CO) which includes deidentified patient records.
Appendix
Appendix B.
Thyroidectomy Procedure Codes.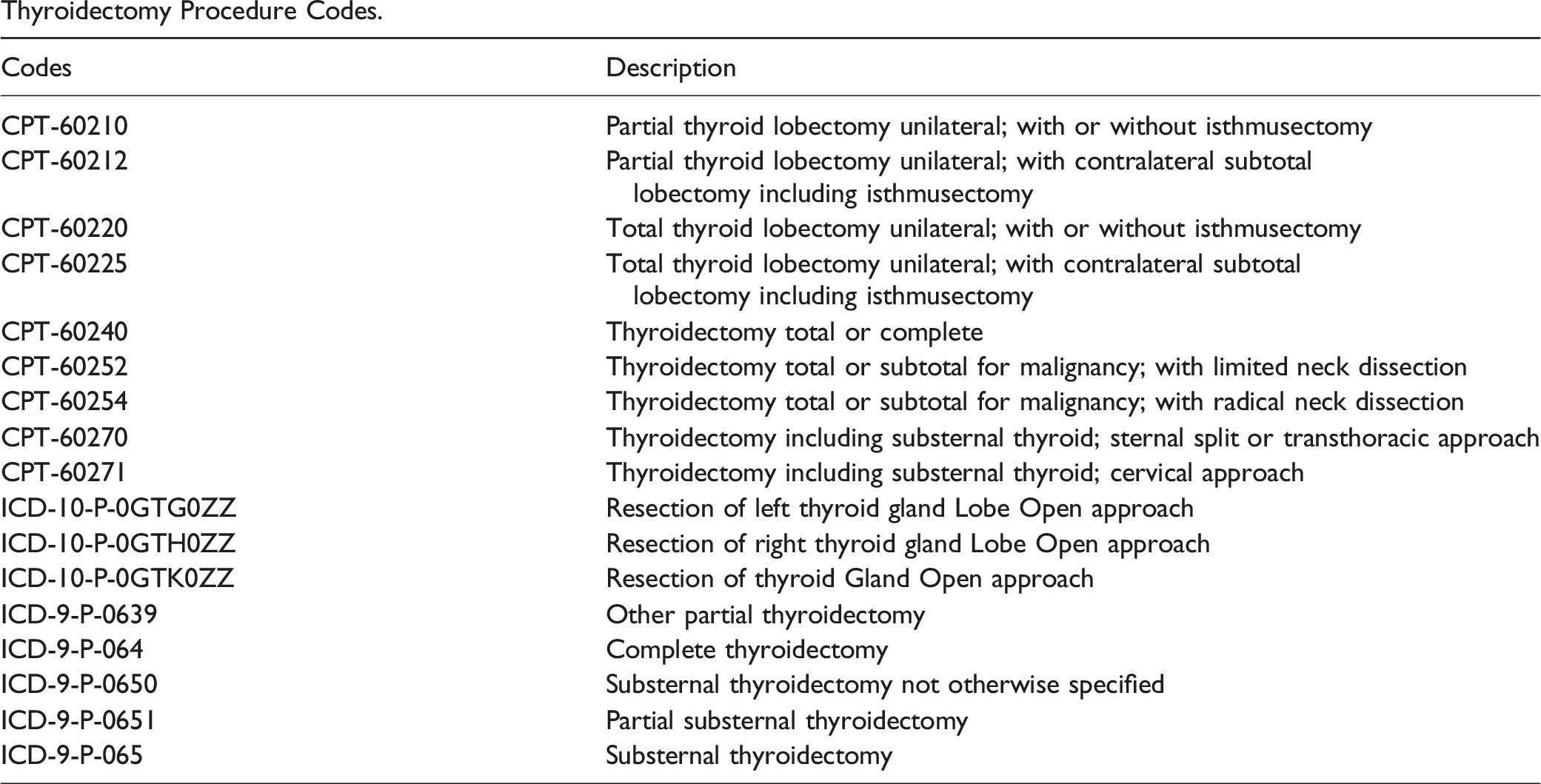
Codes
Description
CPT-60210
Partial thyroid lobectomy unilateral; with or without isthmusectomy
CPT-60212
Partial thyroid lobectomy unilateral; with contralateral subtotal lobectomy including isthmusectomy
CPT-60220
Total thyroid lobectomy unilateral; with or without isthmusectomy
CPT-60225
Total thyroid lobectomy unilateral; with contralateral subtotal lobectomy including isthmusectomy
CPT-60240
Thyroidectomy total or complete
CPT-60252
Thyroidectomy total or subtotal for malignancy; with limited neck dissection
CPT-60254
Thyroidectomy total or subtotal for malignancy; with radical neck dissection
CPT-60270
Thyroidectomy including substernal thyroid; sternal split or transthoracic approach
CPT-60271
Thyroidectomy including substernal thyroid; cervical approach
ICD-10-P-0GTG0ZZ
Resection of left thyroid gland Lobe Open approach
ICD-10-P-0GTH0ZZ
Resection of right thyroid gland Lobe Open approach
ICD-10-P-0GTK0ZZ
Resection of thyroid Gland Open approach
ICD-9-P-0639
Other partial thyroidectomy
ICD-9-P-064
Complete thyroidectomy
ICD-9-P-0650
Substernal thyroidectomy not otherwise specified
ICD-9-P-0651
Partial substernal thyroidectomy
ICD-9-P-065
Substernal thyroidectomy
Appendix C.
Demographics for Matched Cohorts.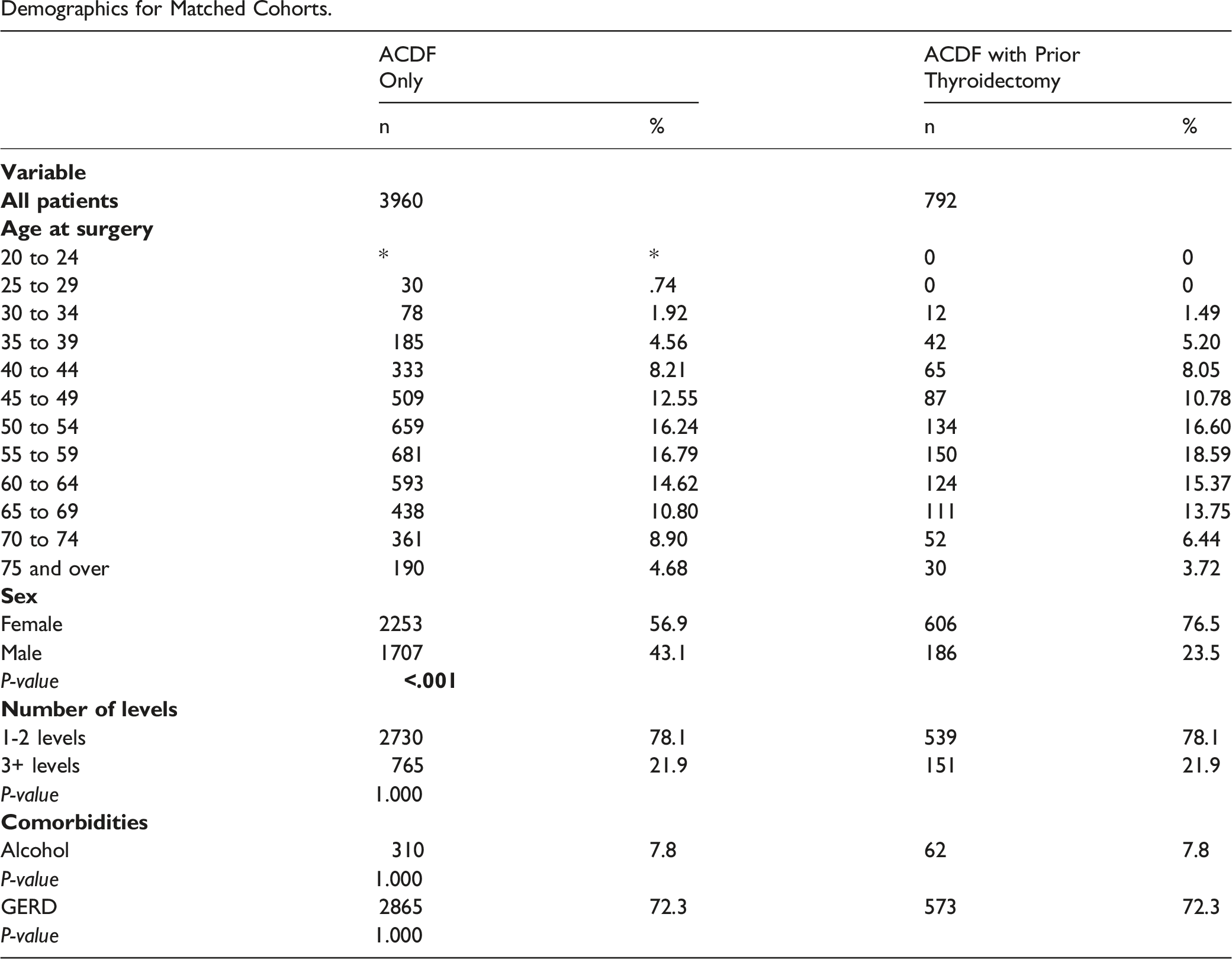
ACDF Only
ACDF with Prior Thyroidectomy
n
%
n
%
3960
792
20 to 24
*
*
0
0
25 to 29
30
.74
0
0
30 to 34
78
1.92
12
1.49
35 to 39
185
4.56
42
5.20
40 to 44
333
8.21
65
8.05
45 to 49
509
12.55
87
10.78
50 to 54
659
16.24
134
16.60
55 to 59
681
16.79
150
18.59
60 to 64
593
14.62
124
15.37
65 to 69
438
10.80
111
13.75
70 to 74
361
8.90
52
6.44
75 and over
190
4.68
30
3.72
Female
2253
56.9
606
76.5
Male
1707
43.1
186
23.5
P-value
1-2 levels
2730
78.1
539
78.1
3+ levels
765
21.9
151
21.9
P-value
1.000
Alcohol
310
7.8
62
7.8
P-value
1.000
GERD
2865
72.3
573
72.3
P-value
1.000
Appendix D.
Total 30-Day Complications.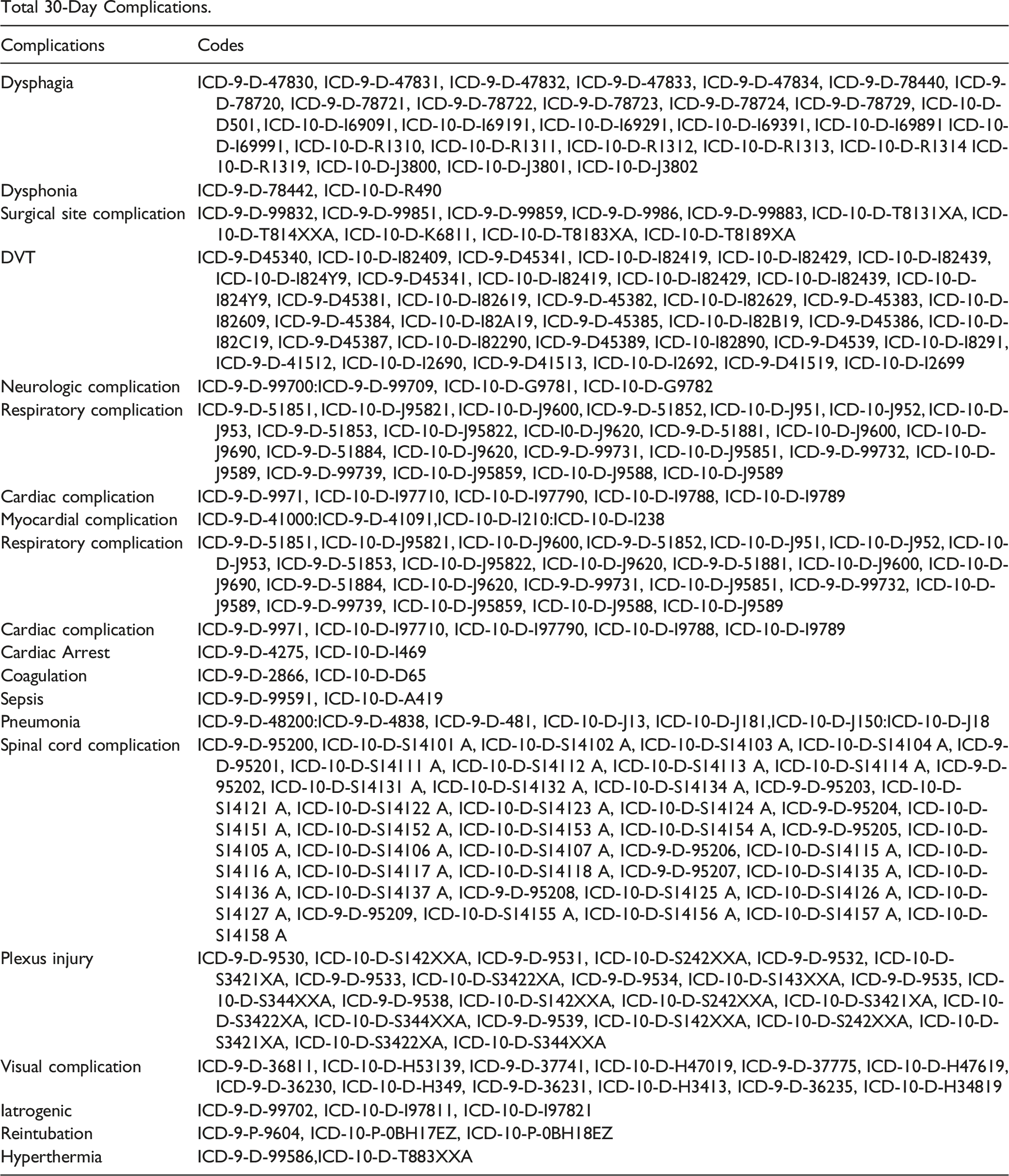
Complications
Codes
Dysphagia
ICD-9-D-47830, ICD-9-D-47831, ICD-9-D-47832, ICD-9-D-47833, ICD-9-D-47834, ICD-9-D-78440, ICD-9-D-78720, ICD-9-D-78721, ICD-9-D-78722, ICD-9-D-78723, ICD-9-D-78724, ICD-9-D-78729, ICD-10-D-D501, ICD-10-D-I69091, ICD-10-D-I69191, ICD-10-D-I69291, ICD-10-D-I69391, ICD-10-D-I69891 ICD-10-D-I69991, ICD-10-D-R1310, ICD-10-D-R1311, ICD-10-D-R1312, ICD-10-D-R1313, ICD-10-D-R1314 ICD-10-D-R1319, ICD-10-D-J3800, ICD-10-D-J3801, ICD-10-D-J3802
Dysphonia
ICD-9-D-78442, ICD-10-D-R490
Surgical site complication
ICD-9-D-99832, ICD-9-D-99851, ICD-9-D-99859, ICD-9-D-9986, ICD-9-D-99883, ICD-10-D-T8131XA, ICD-10-D-T814XXA, ICD-10-D-K6811, ICD-10-D-T8183XA, ICD-10-D-T8189XA
DVT
ICD-9-D45340, ICD-10-D-I82409, ICD-9-D45341, ICD-10-D-I82419, ICD-10-D-I82429, ICD-10-D-I82439, ICD-10-D-I824Y9, ICD-9-D45341, ICD-10-D-I82419, ICD-10-D-I82429, ICD-10-D-I82439, ICD-10-D-I824Y9, ICD-9-D45381, ICD-10-D-I82619, ICD-9-D-45382, ICD-10-D-I82629, ICD-9-D-45383, ICD-10-D-I82609, ICD-9-D-45384, ICD-10-D-I82A19, ICD-9-D-45385, ICD-10-D-I82B19, ICD-9-D45386, ICD-10-D-I82C19, ICD-9-D45387, ICD-10-D-I82290, ICD-9-D45389, ICD-10-I82890, ICD-9-D4539, ICD-10-D-I8291, ICD-9-D-41512, ICD-10-D-I2690, ICD-9-D41513, ICD-10-D-I2692, ICD-9-D41519, ICD-10-D-I2699
Neurologic complication
ICD-9-D-99700:ICD-9-D-99709, ICD-10-D-G9781, ICD-10-D-G9782
Respiratory complication
ICD-9-D-51851, ICD-10-D-J95821, ICD-10-D-J9600, ICD-9-D-51852, ICD-10-D-J951, ICD-10-J952, ICD-10-D-J953, ICD-9-D-51853, ICD-10-D-J95822, ICD-I0-D-J9620, ICD-9-D-51881, ICD-10-D-J9600, ICD-10-D-J9690, ICD-9-D-51884, ICD-10-D-J9620, ICD-9-D-99731, ICD-10-D-J95851, ICD-9-D-99732, ICD-10-D-J9589, ICD-9-D-99739, ICD-10-D-J95859, ICD-10-D-J9588, ICD-10-D-J9589
Cardiac complication
ICD-9-D-9971, ICD-10-D-I97710, ICD-10-D-I97790, ICD-10-D-I9788, ICD-10-D-I9789
Myocardial complication
ICD-9-D-41000:ICD-9-D-41091,ICD-10-D-I210:ICD-10-D-I238
Respiratory complication
ICD-9-D-51851, ICD-10-D-J95821, ICD-10-D-J9600, ICD-9-D-51852, ICD-10-D-J951, ICD-10-D-J952, ICD-10-D-J953, ICD-9-D-51853, ICD-10-D-J95822, ICD-10-D-J9620, ICD-9-D-51881, ICD-10-D-J9600, ICD-10-D-J9690, ICD-9-D-51884, ICD-10-D-J9620, ICD-9-D-99731, ICD-10-D-J95851, ICD-9-D-99732, ICD-10-D-J9589, ICD-9-D-99739, ICD-10-D-J95859, ICD-10-D-J9588, ICD-10-D-J9589
Cardiac complication
ICD-9-D-9971, ICD-10-D-I97710, ICD-10-D-I97790, ICD-10-D-I9788, ICD-10-D-I9789
Cardiac Arrest
ICD-9-D-4275, ICD-10-D-I469
Coagulation
ICD-9-D-2866, ICD-10-D-D65
Sepsis
ICD-9-D-99591, ICD-10-D-A419
Pneumonia
ICD-9-D-48200:ICD-9-D-4838, ICD-9-D-481, ICD-10-D-J13, ICD-10-D-J181,ICD-10-D-J150:ICD-10-D-J18
Spinal cord complication
ICD-9-D-95200, ICD-10-D-S14101 A, ICD-10-D-S14102 A, ICD-10-D-S14103 A, ICD-10-D-S14104 A, ICD-9-D-95201, ICD-10-D-S14111 A, ICD-10-D-S14112 A, ICD-10-D-S14113 A, ICD-10-D-S14114 A, ICD-9-D-95202, ICD-10-D-S14131 A, ICD-10-D-S14132 A, ICD-10-D-S14134 A, ICD-9-D-95203, ICD-10-D-S14121 A, ICD-10-D-S14122 A, ICD-10-D-S14123 A, ICD-10-D-S14124 A, ICD-9-D-95204, ICD-10-D-S14151 A, ICD-10-D-S14152 A, ICD-10-D-S14153 A, ICD-10-D-S14154 A, ICD-9-D-95205, ICD-10-D-S14105 A, ICD-10-D-S14106 A, ICD-10-D-S14107 A, ICD-9-D-95206, ICD-10-D-S14115 A, ICD-10-D-S14116 A, ICD-10-D-S14117 A, ICD-10-D-S14118 A, ICD-9-D-95207, ICD-10-D-S14135 A, ICD-10-D-S14136 A, ICD-10-D-S14137 A, ICD-9-D-95208, ICD-10-D-S14125 A, ICD-10-D-S14126 A, ICD-10-D-S14127 A, ICD-9-D-95209, ICD-10-D-S14155 A, ICD-10-D-S14156 A, ICD-10-D-S14157 A, ICD-10-D-S14158 A
Plexus injury
ICD-9-D-9530, ICD-10-D-S142XXA, ICD-9-D-9531, ICD-10-D-S242XXA, ICD-9-D-9532, ICD-10-D-S3421XA, ICD-9-D-9533, ICD-10-D-S3422XA, ICD-9-D-9534, ICD-10-D-S143XXA, ICD-9-D-9535, ICD-10-D-S344XXA, ICD-9-D-9538, ICD-10-D-S142XXA, ICD-10-D-S242XXA, ICD-10-D-S3421XA, ICD-10-D-S3422XA, ICD-10-D-S344XXA, ICD-9-D-9539, ICD-10-D-S142XXA, ICD-10-D-S242XXA, ICD-10-D-S3421XA, ICD-10-D-S3422XA, ICD-10-D-S344XXA
Visual complication
ICD-9-D-36811, ICD-10-D-H53139, ICD-9-D-37741, ICD-10-D-H47019, ICD-9-D-37775, ICD-10-D-H47619, ICD-9-D-36230, ICD-10-D-H349, ICD-9-D-36231, ICD-10-D-H3413, ICD-9-D-36235, ICD-10-D-H34819
Iatrogenic
ICD-9-D-99702, ICD-10-D-I97811, ICD-10-D-I97821
Reintubation
ICD-9-P-9604, ICD-10-P-0BH17EZ, ICD-10-P-0BH18EZ
Hyperthermia
ICD-9-D-99586,ICD-10-D-T883XXA