
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Anterior cervical discectomy and fusion (ACDF) is commonly used to treat an array of cervical spine pathology and is associated with good outcomes and low complication rates. Diabetes mellitus (DM) is a common comorbidity for patients undergoing ACDF, but the literature is equivocal about the impact it has on outcomes. Because DM is a highly prevalent comorbidity, it is crucial to determine if it is an associated risk factor for outcomes after ACDF procedures.
Methods:
Patients at a single institution from 2008 to 2016 undergoing ACDF were compared on the basis of having a prior diagnosis of DM versus no DM. The 2 cohorts were compared utilizing univariate tests and multivariate logistic and linear regressions.
Results:
Data for 2470 patients was analyzed. Diabetic patients had significantly higher Elixhauser scores (P < .0001). Univariate testing showed diabetic patients were more likely to suffer from sepsis (0.82% vs 0.10%, P = .03) and bleeding complications (3.0% vs 1.5%, P = .04). In multivariate analyses, diabetic patients had higher rates of non–home discharge (odds ratio [OR] = 1.37, 95% confidence interval [CI] = 1.07-1.75, P = .013) and prolonged length of stay (OR = 1.95, 95% CI = 1.25-3.05, P = .003), but similar complication (OR = 1.46, 95% CI = 0.85-2.52, P = .17), reoperation (OR = 0.77, 95% CI = 0.33-1.81, P = .55), and 90-day readmission (OR = 1.53, 95% CI = 0.97-2.43) rates compared to nondiabetic patients. Direct cost was also shown to be similar between the cohorts after adjusting for patient, surgical, and hospital-related factors (estimate = −$30.25, 95% CI = −$515.69 to $455.18, P = .90).
Conclusions:
Diabetic patients undergoing ACDF had similar complication, reoperation, and readmission rates, as well as similar cost of care compared to nondiabetic patients.
Introduction
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed procedures for patients suffering from a wide spectrum of cervical spine pathologies, 1 including degenerative disc disease, myelopathy, radiculopathy, trauma, and infection.2,3 Advantages to the procedure include low postoperative complication rates, 4 consistent good results, and relative procedural ease, thereby making it a popular surgical strategy for patients with maladies of the cervical spine.
Diabetes mellitus (DM) is one of the most commonly reported comorbidities for patients undergoing ACDF procedures,5,6 and its prevalence is projected to increase. 7 Many studies have shown that DM is linked to prolonged length of stay (LOS), readmission, dysphagia, infection, and discharge to non–home locations for patients who undergo spine surgery.5,6,8-11 It has also been linked to poorer surgical outcomes and wound dehiscence in other surgical procedures, especially abdominal panniculectomy and carpal tunnel operations.12,13 However, several studies have refuted the negative effect that DM may have on surgical outcomes. Cinotti et al claimed that outcomes of lumbar decompression surgery were similarly successful for diabetic and nondiabetic patients. 14 Cho et al also reported that type 2 DM was not a significant risk factor for perioperative complications or repeat surgeries for patients undergoing spinal deformity surgery. 15 Presently, it is unclear whether DM plays a significant role on the outcomes for cervical spinal surgery.
It is also unknown the effect DM has on cost of care for patients undergoing ACDF. One study concerning total-joint arthroplasty found the marginal cost of diabetic patients was $676 higher than that of nondiabetic patients. 16 However, the role DM may play as an independent risk factor for cost of care in ACDF has not been reported.
The goal of the present study is to determine the effect DM has on patient outcomes as well as to examine whether DM is an associated risk factor for adverse episode-based outcomes following ACDF. Furthermore, this study aims to analyze the role DM plays on cost of care for these patients. Due to the low complication rates of the procedure, large cohorts such as the one analyzed in this study are required to identify meaningful findings. Given that the literature has equivocal findings regarding DM as a predictive factor for other surgeries, this information could help physicians develop more effective treatment plans for patients with DM suffering from cervical spine diseases.
Material and Methods
Following institutional review board approval, the records of all patients undergoing spine surgery at one institution from January 1, 2008, to November 30, 2016, were reviewed for inclusion. Demographic, perioperative, and billing data was collected. Patients were identified as having undergone instrumented ACDF with the Current Procedural Terminology (CPT) codes 63 075, 22 554, and 22 551. Of note, all ACDF procedures at our institution involve instrumentation, allowing for consistency in analyzing procedure outcomes and cost. Those who underwent posterior approaches or had posterior cervical surgery in the same hospitalization were excluded using the CPT codes 63 045, 63 001, 63 015, 22 110, 22 210, and 22 600. Patients were likewise excluded if they underwent surgery for tumors, fractures, or infections using CPT codes 63 275, 63 276, 22 325, 22 326, 22 327, 63 270, 10 180, 63 266, and 63 267, so as to exclude urgent and emergent procedures. Consequently, all included procedures were elective. Diabetic patients were identified as those with records including the International Classification of Diseases, Ninth and Tenth Revision (ICD-9, ICD-10), codes 250.00 to 250.99, E10.00 to E10.9, and E11.00 to E11.9. Random sampling was performed to confirm diagnoses in patients classified as having DM. Patients were further classified by preoperative diagnosis (spinal stenosis, myelopathy, radiculopathy, or other) based on billing codes, utilizing ICD-9 and ICD-10 codes 723.0, 723.4, 722.71 722.1, M48.02, M48.03, M50.1, M54.12, M54.13, M47.22, M47.23, M50.0, M47.12, and M47.13.
After grouping by DM status, information regarding preoperative comorbidities was collected using the relevant ICD-9 and ICD-10 codes as described by Quan et al. 17 Patients’ overall comorbidity burden was estimated with the Elixhauser Comorbidity Index using a weighting system described by van Walraven et al 18 and validated in a population similar to this study’s by Menendez et al. 19 The Elixhauser Index includes 31 variables and was developed in 1998 to improve assessment of common patient comorbidities in predictions of cost of care and length of stay. 20 The large number of included variables requires large, administrative data sets such as this one for accurate analysis. It has also been validated for use with ACDF, 21 making it an ideal metric for use in the present study. Of note, while diabetes is classically included in the Elixhauser Index, the diagnosis of diabetes (both complicated and uncomplicated) was weighted to zero in the present analysis, consistent with the previously accepted van Walraven Algorithm, 18 so that our analysis is not affected by the presence of diabetes. The Elixhauser Comorbidity Index was then bucketed into groups of <0, 0, 1 to 4, and ≥5 for ease of interpretation.19,20
Demographic information collected included age, sex, calculated Elixhauser Index score, preoperative diagnosis, the number of segments involved in the operation, 22 and status of complicated versus uncomplicated disease for patients with DM. Patients were specifically classified as having either complicated or uncomplicated diabetes, based on the definition given by the Elixhauser Index by differing ICD-9 or ICD-10 codes. Postoperative complications were coded utilizing ICD-9 and ICD-10 codes, and the described complications included airway complications, bleeding, renal failure, myocardial infarction, cerebrovascular accident, pneumonia, pulmonary embolism, cardiac arrest, deep vein thrombosis, sepsis, septic shock, death, wound dehiscence, urinary tract infection, and superficial surgical site infection. Furthermore, postoperative complications including delayed extubation (defined as extubation after leaving the operating room), required intensive care unit (ICU) stay, prolonged length of stay (LOS), non–home discharge, and 30- and 90-day emergency department (ED) visits and readmissions were also quantified. Prolonged LOS was defined as LOS greater than or equal to the 75th percentile for the cohort. Finally, cost data was obtained from patient records representing direct cost of overall hospitalization per patient.
Statistical analysis was performed comparing patients with and without DM on the basis of demographics, comorbidity burden, postoperative outcomes, and cost. Categorical variables were analyzed using χ2 test or Fisher’s exact test, where necessary. Normality of continuous variables was assessed with the Kolmogorov-Smirnov tests; normally distributed variables were analyzed using Student’s t test, while nonparametric variables were assessed with the Mann-Whitney U test. Multivariate logistic regression modeling controlling for age, sex, Elixhauser Index score, preoperative diagnosis, number of segments fused, and complicated disease status for each patient was performed for a number of outcomes, in addition to univariate analysis. For each logistic regression, the independent variable was diabetes and the main dependent variable was the outcome listed. Four sequential linear regression models with an independent variable of DM and main dependent variable of direct cost were created such that each model added variables to elucidate if differences in cost between patients with and without DM could be isolated to certain sets of factors. All cost values were adjusted for inflation and reported in 2016 US dollars, utilizing conversions consistent with the Consumer Price Index for medical care provided by the US Bureau of Labor Statistics. The first model included only DM as a predicting factor, while the second model added patient-level factors such as age, sex, Elixhauser Index score, number of segments fused, preoperative diagnosis, and complicated diabetes status. The third model added surgical factors to the second model, including operative time and intraoperative amounts delivered for crystalloid solutions, colloid solutions, red blood cell (RBC) transfusions, platelet transfusions, fresh frozen plasma (FFP), and cryoprecipitate. The fourth model added LOS and number of days in the ICU. All regression covariates were selected due to known clinical relevance in the field and spine surgery literature. All covariates were included in regression analysis regardless of distributions in the present cohorts in order to account for residual confounding that may exist. No collinearity was identified between any of the variables.
All statistical analyses were performed in Statistical Analysis Software version 9.4 (SASv9.4). Significance was defined by a P value less than .05, and all confidence intervals (CIs) were set to 95%. For multivariate regression analyses, significant CIs do not include 1.00 in logistic regressions and do not include 0.00 in linear regressions.
Results
A total of 2470 patients underwent ACDF between 2008 and 2016; of these, 365 (15%) patients were diagnosed with DM. Of the diabetic patients, 27 (7.4%) were classified with complicated diabetes status based on the definition given by the Elixhauser Index. The DM cohort had significantly more comorbidities than the nondiabetic cohort, as evidenced by a higher proportion of patients with an Elixhauser score greater than 5 (21% vs 12%, P < .0001). Patients with DM also had higher rates of myelopathy diagnoses (38% vs 30%, P < .02; Table 1).
Demographicsa.
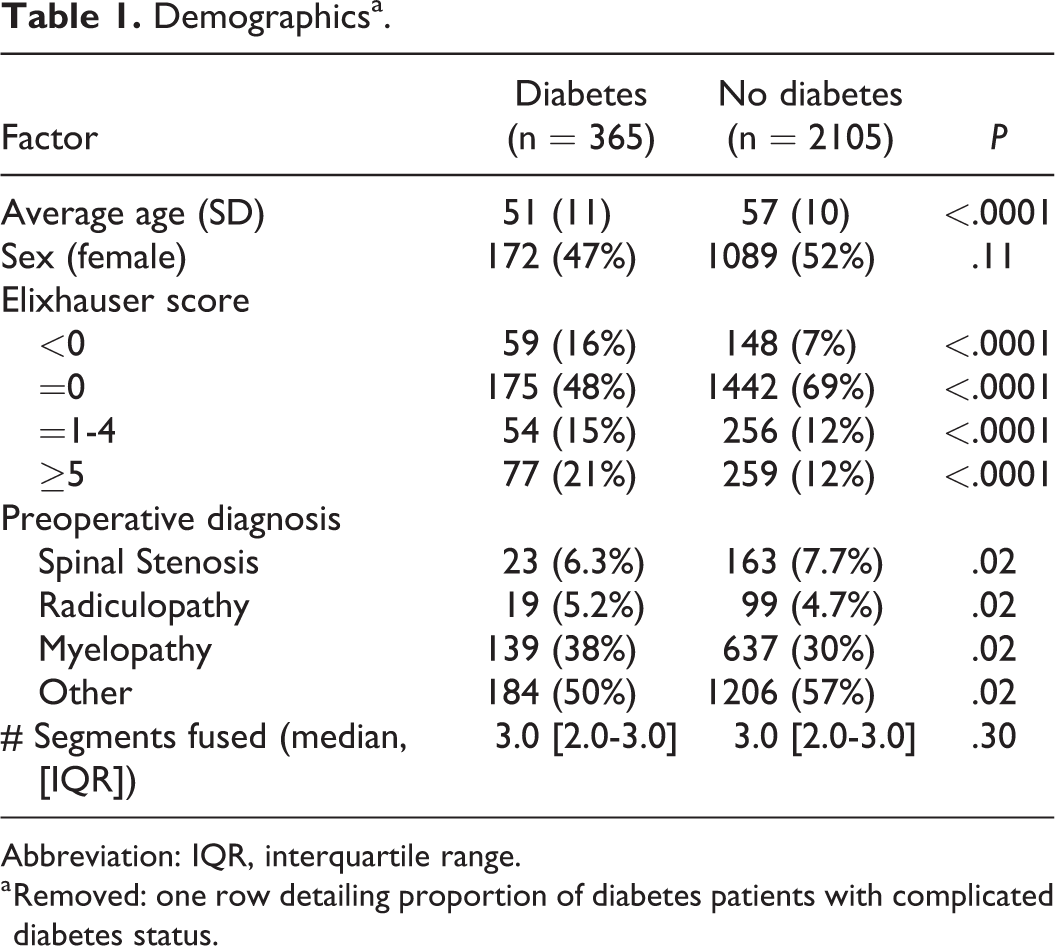
Abbreviation: IQR, interquartile range.
a Removed: one row detailing proportion of diabetes patients with complicated diabetes status.
Of the 15 in-hospital complications analyzed with univariate analysis, patients with DM were found to have significantly higher rates of sepsis (0.8% vs 0.1%, P = .03) and bleeding complications (3.0% vs 1.5%, P = .04). There were no other significant differences in complication rates between the 2 cohorts (Table 2).
In-Hospital Complication Rates.
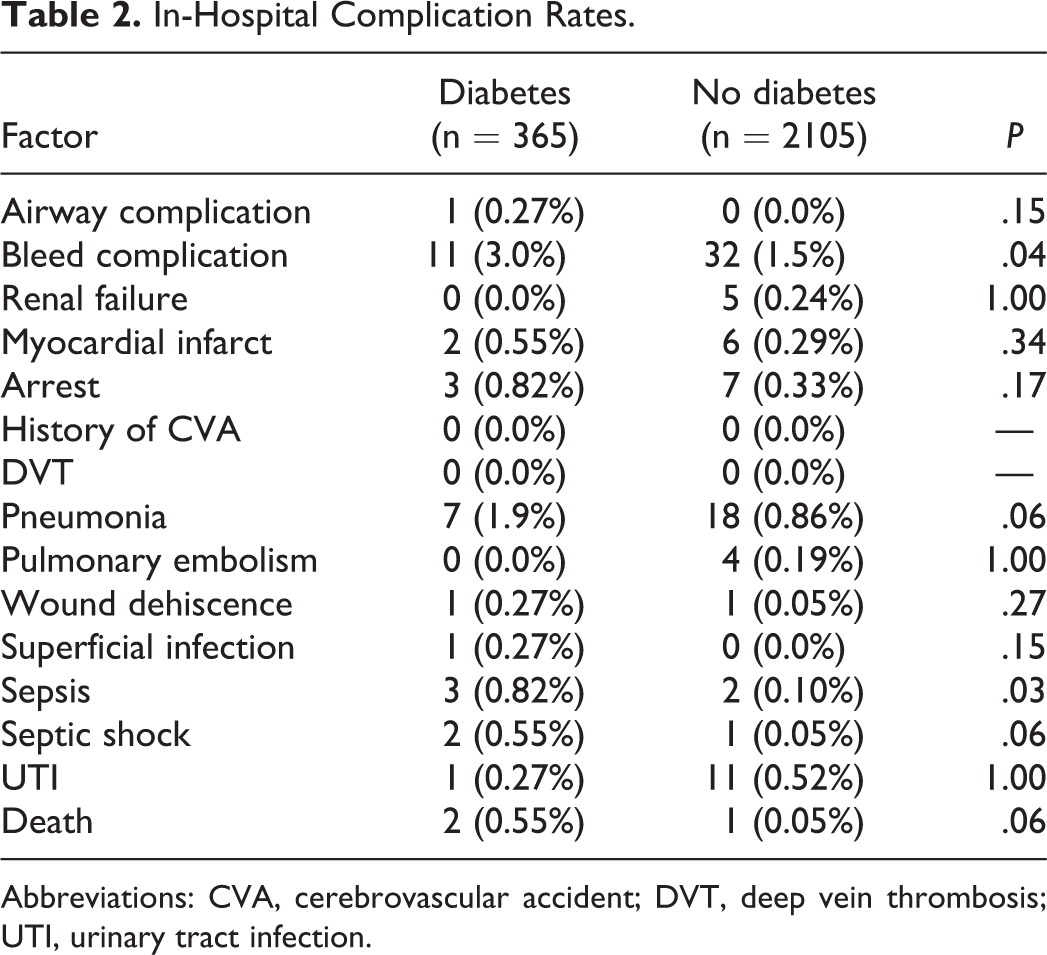
Abbreviations: CVA, cerebrovascular accident; DVT, deep vein thrombosis; UTI, urinary tract infection.
In univariate analysis, patients with DM had a higher proportion of delayed extubation (4.1% vs 1.4%, P = .0004), ICU stay (7.1% vs 3.5%, P = .001), overall complications (6.6% vs 3.3%, P = .003), prolonged LOS (49% vs 37%, P < .0001), non–home discharge (11% vs 4.3%, P < .0001), 30-day readmissions (4.4% vs 2.0%, P = .004), and 90-day readmissions (8.5% vs 4.5%, P = .001). After adjusting for age, sex, Elixhauser Comorbidity Index, preoperative diagnosis, and number of segments fused in multivariate analysis, only 2 variables retained a statistically significant difference in outcomes: non–home discharge (odds ratio [OR] = 1.37, 95% CI = 1.07-1.75, P = .013) and prolonged LOS (OR = 1.95, 95% CI = 1.25-3.05, P = .003). Of note, no significant differences were ever found between rates of reoperation (OR = 0.77, 95% CI = 0.33-1.81, P = .55; Table 3).
Episode-Based Outcomes: Univariate Analysis and Multivariable Logistic Regression.
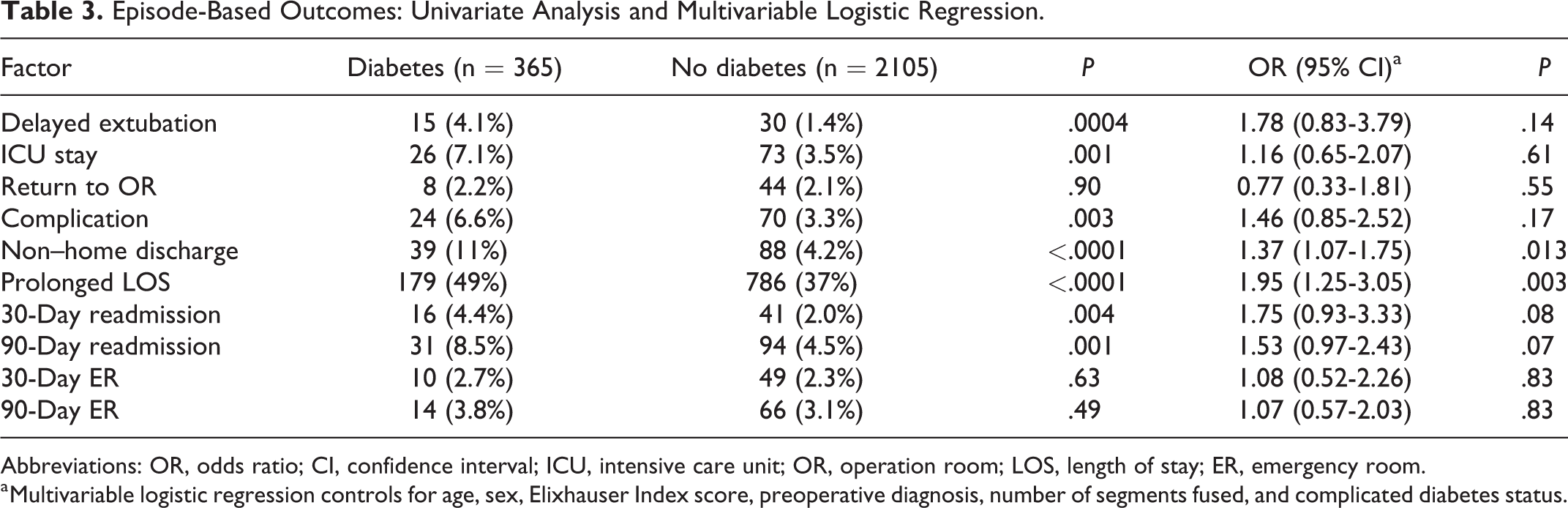
Abbreviations: OR, odds ratio; CI, confidence interval; ICU, intensive care unit; OR, operation room; LOS, length of stay; ER, emergency room.
a Multivariable logistic regression controls for age, sex, Elixhauser Index score, preoperative diagnosis, number of segments fused, and complicated diabetes status.
Patients with DM had a direct cost of care that was $2237.59 (95% CI = $1200.83 to $3274.34, P < .0001) higher than patients without DM. After adjusting for demographic, surgical, and hospital-related factors utilizing sequential modeling, there was no significant difference in cost of care between the 2 groups, with cost of care of patients with DM approximately $30.25 less than patients without DM (95% CI - −$515.69 to $455.18, P = .90; Table 4). Detailed results for all controlled variables in the linear regression cost analysis can be found in the supplement materials.
Cost of Care: Linear Regressiona.
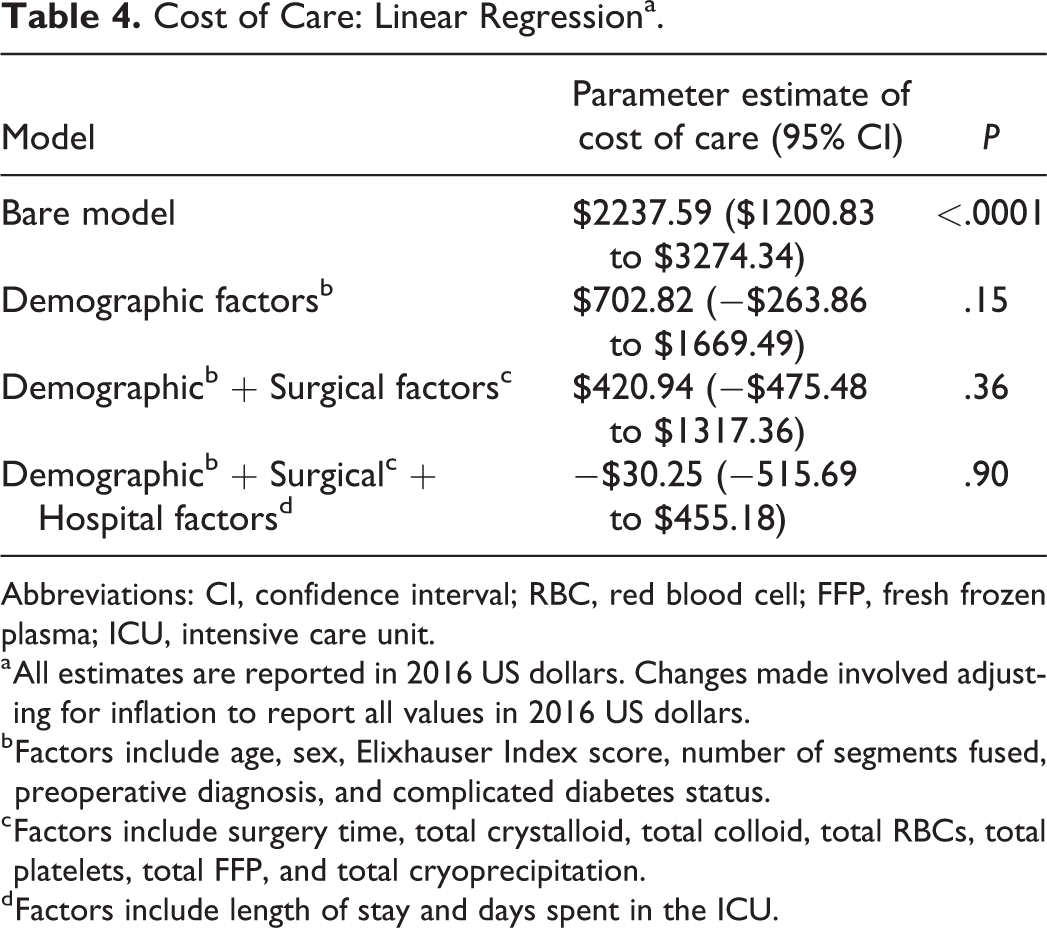
Abbreviations: CI, confidence interval; RBC, red blood cell; FFP, fresh frozen plasma; ICU, intensive care unit.
a All estimates are reported in 2016 US dollars. Changes made involved adjusting for inflation to report all values in 2016 US dollars.
b Factors include age, sex, Elixhauser Index score, number of segments fused, preoperative diagnosis, and complicated diabetes status.
c Factors include surgery time, total crystalloid, total colloid, total RBCs, total platelets, total FFP, and total cryoprecipitation.
d Factors include length of stay and days spent in the ICU.
Discussion
Surgical outcomes of patients with DM have been the subject of much research, as it is a widely prevalent comorbidity. There is controversy in the literature as several studies report adverse outcomes associated with DM, while others report equal outcomes between diabetic and nondiabetic patients. Furthermore, many studies reporting differences in surgical outcomes focus on spine operations other than ACDF and cannot necessarily be generalized to these procedures. The literature exploring DM as a predictive factor in spine surgeries is thus equivocal, and it is presently unclear whether DM plays a significant role in the outcomes of anterior cervical spinal surgery. The present results show few differences in complication rates and other outcomes between patients with and without DM, indicating that it is likely not a correlational risk factor in patients undergoing ACDF.
Multiple studies have previously identified correlations between DM and adverse outcomes for patients undergoing surgery. Mullins et al reported that patients with DM were more likely to have a prolonged LOS when undergoing ACDF. 5 Wang et al reported DM as a risk factor for developing dysphagia after anterior cervical surgery. 23 Phan et al reported an association between DM and a higher rate of UTIs. 8 However, all 3 of these associations were found using only either univariate or bivariate analysis and did not analyze the role of DM in the context of other risk factors. The significance of the role DM had on patient outcome was therefore uncertain. Additionally, while Parker et al found that DM was associated with higher chances of readmission after spine surgery, it was also found that their readmission cohort was more likely to have had lumbar surgeries and posterior approaches. 6 Thus, an association between DM and readmission cannot necessarily be assumed for patients undergoing ACDF. Cancienne et al found that rates of deep postoperative infections were linked to hemoglobin A1c (HbA1c) levels. 9 However, HbA1c = 7.5 mg/dL was used as the threshold to compare patients, and the World Health Organization (WHO) defines an HbA1c value of 6.5 mg/dL as a cutoff for diagnosing type 2 diabetes, with 7.0 mg/dL widely used as the goal for control of type 2 diabetes. This finding, therefore, cannot be generalized to all diabetic patients, especially those with well-controlled DM.
In the present results, few differences in complication rates were found between patients diagnosed with DM and patients without DM, except for higher rates of sepsis and bleeding complications found in patients with DM. Additionally, logistic regression results failed to identify diabetes as an independent risk factor for reoperation rate, required ICU stay, and 30- and 90-day readmission rates, and overall complication rate. Despite a logical link between diabetes and certain complications such as surgical site infection, myocardial infarction, and urinary tract infection, the present results suggest that DM is not, in fact, correlated with complications following ACDF. Additionally, while multivariate analysis found diabetic patients had higher rates of prolonged LOS and non–home discharge, it is likely that these findings are related and redundant, as multiple studies have revealed strong correlations between non–home discharges and prolonged LOS,24,25 in addition to a logical and logistical link. The present results do not identify any other differences in episode-based outcomes by multivariate analysis.
These minimal findings do not align with studies showing significant differences in the literature. One explanation is that DM may be an indicator of increased comorbidity burden. The present results show diabetic patients had a higher Elixhauser score on average, and several studies have shown an association between higher Elixhauser scores and poorer outcomes after undergoing surgery.26,27 Additionally, this study specifically controls for disease burden by accounting for Elixhauser Index score and complicated diabetes status (as defined by the Elixhauser Index as ICD-9 or ICD-10 codes for diabetes with renal, ophthalmologic, neurologic, or peripheral vascular manifestations) when comparing diabetic and nondiabetic cohorts in multivariate analysis. Hence, other factors that contribute to elevated Elixhauser scores—factors not controlled for in other studies—may drive higher rates of complications. This advances the theory that DM can be a driver of other conditions, which themselves may be more deleterious to patient health in the setting of spine surgery than DM itself. Therefore, patient DM status may be an indicator of poor health, but it is not itself a direct risk factor for episode-based outcomes. Perhaps greater surveillance of patients with DM, through effective glycemic control and optimal management of complicating conditions, is necessary rather than concern about their DM status.
In addition to comparable postsurgical outcomes, similar costs of care were also found. Initially, the present results suggested that unadjusted cost of care for patients with DM was significantly higher than that of patients without DM. This finding has been corroborated in other studies in total joint arthroplasty, which found a marginal cost increase of approximately $676 for patients with DM. 16 However, the present results suggest these findings do not endure when adjusting for other patient-level factors, such as age, sex, and comorbidity burden (Table 4). Therefore, it is possible that diabetic patients possess a variety of other comorbidities that contribute to higher costs in a bare model, yet show the insignificance of DM as a cost predictor in a model incorporating these other factors. DM is a good predictor of overall health as it has been correlated with higher rates of chronic kidney disease, congestive heart failure, peripheral vascular disease, and peripheral neuropathy,28-30 all of which were included in the Elixhauser Comorbidity Index and have been previously shown to be predictors of infection and higher cost in surgery.31-33 Therefore, similar to its lack of significance in predicting complications following ACDF, DM is perhaps more of a peripheral factor than a singular cost predictor in spine surgery.
Multiple limitations arise in this study due to the nature of ACDF procedures as well as having a limited sample size from a single institution. ACDF is known to have very low complication rates,1,3 and thus a lack of significant differences between in-hospital complication rates between diabetic and nondiabetic patients may be a product of sample size limitations as opposed to a lack of differences. Additionally, the present results only account for adverse events occurring during the index hospital stay, and therefore may underestimate delayed complications, such as pseudoarthrosis. Furthermore, these results do not account for multiple factors that are relevant to outcomes in ACDF patients, such as interbody fusion rates, loss of overall or segmental alignment, dislodgement or breakage of instrumentation, and pain or disability profiles. When adjusting complication rates for demographic factors, a general measure of comorbidity (Elixhauser score) was used instead of specific comorbidities due to sample size concerns. This prevents the authors from analyzing what specific factors contribute to poor health and elevated comorbidity scores. In addition, the methods do not include information on the type of diabetes, a metric to measure severity of disease such as HbA1C, or how long patients had diabetes, so this study is unable to compare etiologies or trend outcomes against severity. However, because complicated disease was controlled for in multivariate analysis, this study can still confidently say that the diagnosis of diabetes (especially uncomplicated diabetes) was not correlated with adverse outcomes or cost. Furthermore, like in any retrospective review, the present analysis is susceptible to other comorbidities or unknown confounding variables that are not included as controlling factors in regression models. Some specific examples are that smoking status, duration of symptoms, and previous spine surgeries were all not included in the demographic information, so their effects could also not be assessed. In terms of addressing consistency in patient care, this study was unable to account for multiple-surgeon involvement; however, at our institution, only the primary surgeon is responsible for postoperative management of the patient, limiting any management variation to the intraoperative arena. Last, data from this study was collected from a single academic medical center, and results may not be generalizable to smaller, nonacademic centers.
Despite these limitations, the present findings can be useful in future work investigating outcomes and costs of ACDF procedures. The present results show DM by itself does not increase cost of care and that other factors or comorbidities may be responsible for increases in cost. Future studies could attempt to identify which other factors are independent predictors of cost. While previous studies have identified predictive factors that correlate with prolonged LOS 34 and non–home discharge 10 after ACDF, there is a need for a prospective randomized controlled trial to differentiate between predictive factors that are causative, independent risk factors of adverse outcomes, and those that are merely correlated.
Conclusions
While patients with DM were more likely to have prolonged length of stay or non–home discharge, they have similar rates of complications, reoperations, and readmissions, as well as similar cost of care compared to patients without DM. Additionally they have higher Elixhauser scores, suggesting that DM is an indicator of overall patient disease burden rather than an independent risk factor for poor outcomes. Therefore, physicians should consider patients’ overall health when developing treatment plans for patients with DM. Although controlling patients’ DM in the hospital is undoubtedly important, physicians should consider that isolated DM, especially uncomplicated DM, may not predispose patients to complications following ACDF.
Supplemental Material
Supplemental Material, Supplement_Table_1_with_revisions - The Impact of Diabetes on Outcomes and Health Care Costs Following Anterior Cervical Discectomy and Fusion
Supplemental Material, Supplement_Table_1_with_revisions for The Impact of Diabetes on Outcomes and Health Care Costs Following Anterior Cervical Discectomy and Fusion by William H. Shuman, Sean N. Neifert, Jonathan S. Gal, Daniel J. Snyder, Brian C. Deutsch, Jeffrey H. Zimering, Robert J. Rothrock and John M. Caridi in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval was obtained from the institution’s institutional review board (HS# 16-00 565).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.