
Abstract
Study Design
Systematic review
Objectives
We sought to synthesize the literature investigating the disparities that Medicaid patients sustain with regards to 2 types of elective spine surgery, lumbar fusion (LF) and anterior cervical discectomy and fusion (ACDF).
Methods
Our review was constructed in accordance with Preferred Reporting Items and Meta-analyses (PRISMA) guidelines and protocol. We systematically searched PubMed, Embase, Scopus, CINAHL, and Web of Science databases. We included studies comparing Medicaid beneficiaries to other payer categories with regards to rates of LF and ACDF, costs/reimbursement, and health outcomes.
Results
A total of 573 articles were assessed. Twenty-five articles were included in the analysis. We found that the literature is consistent with regards to Medicaid disparities. Medicaid was strongly associated with decreased access to LF and ACDF, lower reimbursement rates, and worse health outcomes (such as higher rates of readmission and emergency department utilization) compared to other insurance categories.
Conclusions
In adult patients undergoing elective spine surgery, Medicaid insurance is associated with wide disparities with regards to access to care and health outcomes. Efforts should focus on identifying causes and interventions for such disparities in this vulnerable population.
Introduction
The rates of spine surgery have been steadily increasing during the past few decades.1-3 Martin et al. demonstrated a 62.3% increase in volume of elective lumbar fusion (LF) from 2004 to 2015. 1 Similarly, a volume increase of 24.2% was reported by Lopez et al. for anterior cervical discectomy and fusion (ACDF) in the Medicare population from 2012-2017. 2 With the proportion of the elderly population projected to dramatically increase in the coming years, 4 the utilization of spinal procedures is expected to follow as degenerative spine conditions become more prevalent.5-7 Thus, identifying populations at risk for disparities in outcomes, costs, and access to these procedures is becoming increasingly important.
With the Medicaid expansion being 1 of the major provisions of the Affordable Care Act (ACA), the number of patients under Medicaid is higher than ever. 8 Aliu et al 9 demonstrated an increase in utilization of orthopedic procedures, including spine surgery, post-Medicaid expansion in the state of New York. While the results of this study would suggest a potential increase in access to spine surgery for Medicaid recipients, Medicaid recipients were still found to have less access to spine surgery with worse outcomes compared to other insurance beneficiaries.10-18 Understanding and mitigating these inequities is critical for the ability of spine surgeons and providers to provide better care for their patients. Although disparities in spine surgery regarding patients under Medicaid have been heavily studied,10-18 there is no systematic review in the literature that effectively compiles and discusses these findings.
The objective of this systematic review was to assess the effect of Medicaid insurance on patients undergoing spine surgery with regards to access, quality, and costs compared to patients under other insurance providers. We hypothesized that Medicaid beneficiaries will be negatively affected in all 3 categories. We focused on 2 commonly performed spine procedures, namely LF and ACDF, to limit the heterogeneity of studies analyzed with regards to type of surgery, while maintaining an overarching analysis of the disparities that Medicaid beneficiaries sustain in spine surgery.
Methods
Protocol
Our systematic review of the literature was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. 19
Search Strategy and Eligibility Criteria
On September 18, 2021, we searched PubMed, Embase, Scopus, CINAHL, and Web of Science. The search strategies utilized were developed by the authors and refined by a qualified librarian. The detailed search strategies are available as a supplementary appendix (Appendix A). We only included English-language peer-reviewed articles in which Medicaid patients were exposed to either lumbar fusion or anterior cervical discectomy and some aspect of their care was examined in comparison to other payer categories. We excluded articles that studied pediatric patients, non-elective cases such as trauma or malignancy, only Medicaid patients (no comparison), or only dual-eligible beneficiaries. We also excluded conference presentations, letters, reviews, commentaries, and expert opinions.
Study Selection
Two independent reviewers [DB, CO] performed title and abstract screening based on the predetermined eligibility criteria. The same 2 authors then performed full-text screening of the retrieved articles. In both cases, a third reviewer [FM] served as an arbitrator when there was a disagreement between the 2 primary reviewers. Additionally, references cited by included articles were also screened for inclusion. Included articles were then categorized by topic for analysis.
Data Extraction and Data Items
The following data was extracted: study design, publication year, dataset source (including years covered), sample size, type of spinal surgery, payer comparison groups, likelihood of undergoing surgery, costs/reimbursement, and outcome measurements. Reported measures of association for the outcomes of interests (including confidence interval and P-value) were recorded.
Quality and Level of Evidence
The 2 primary reviewers utilized the methodological index for non-randomized studies (MINORS) criteria to evaluate the quality of included studies. 20 The third reviewer served as an arbitrator in cases of disagreement. The Oxford Centre for Evidence Based Medicine (OCEBM) levels of evidence were utilized to determine level of evidence for included studies. 21
Results
Our initial search resulted in 573 articles after duplicate removal. Twenty-two articles met eligibility criteria. Three additional articles were included from the references of articles initially selected. Ultimately, we included 25 articles in the systematic review. A flow diagram of our detailed search is depicted in Figure 1. PRISMA flow diagram detailing literature search. Search was Performed using PubMed, Embase, Scopus, CINAHL, and Web of Science databases on September 18, 2021.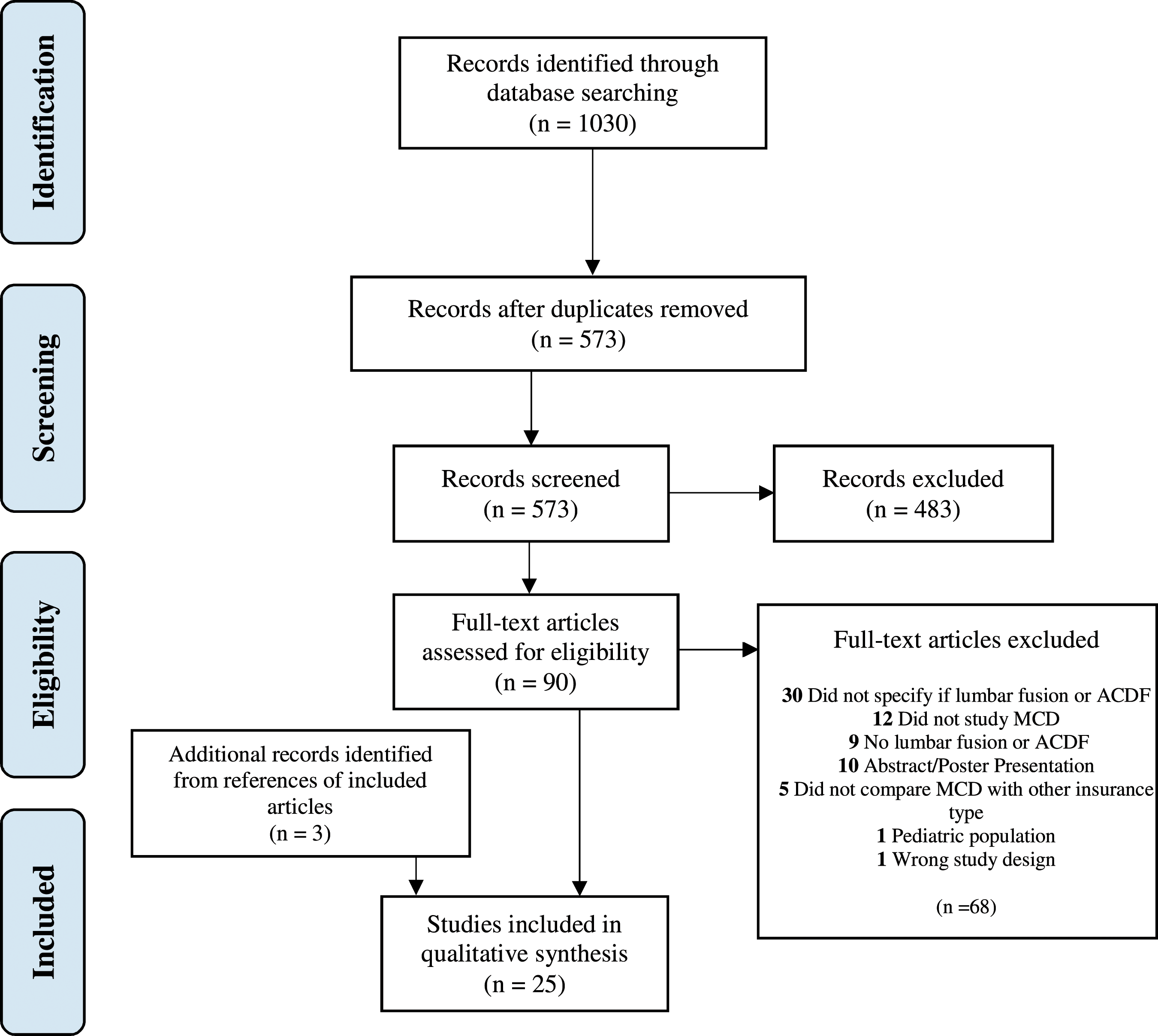
Included studies by Year, Data Source, Years Analyzed and Topic.
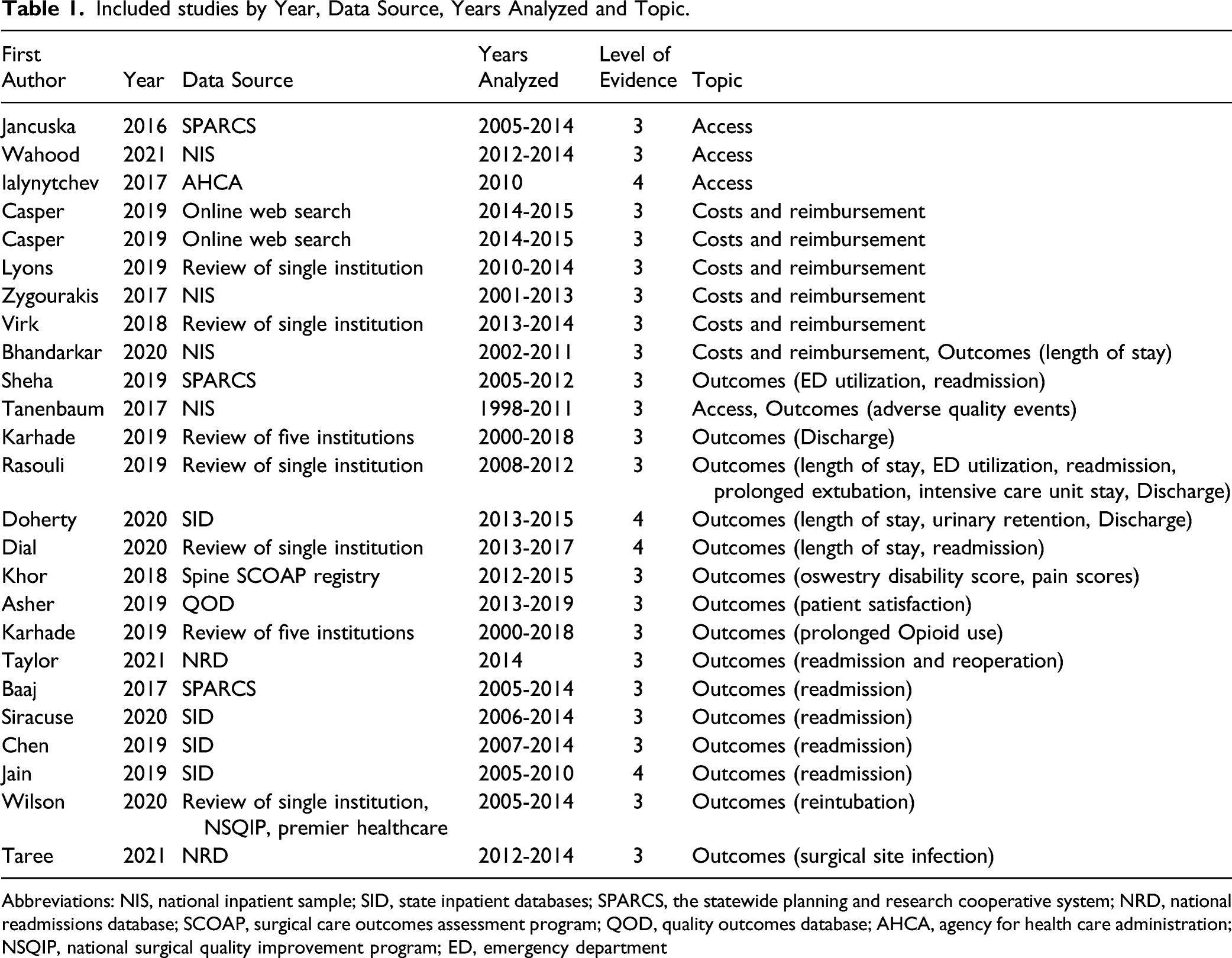
Abbreviations: NIS, national inpatient sample; SID, state inpatient databases; SPARCS, the statewide planning and research cooperative system; NRD, national readmissions database; SCOAP, surgical care outcomes assessment program; QOD, quality outcomes database; AHCA, agency for health care administration; NSQIP, national surgical quality improvement program; ED, emergency department
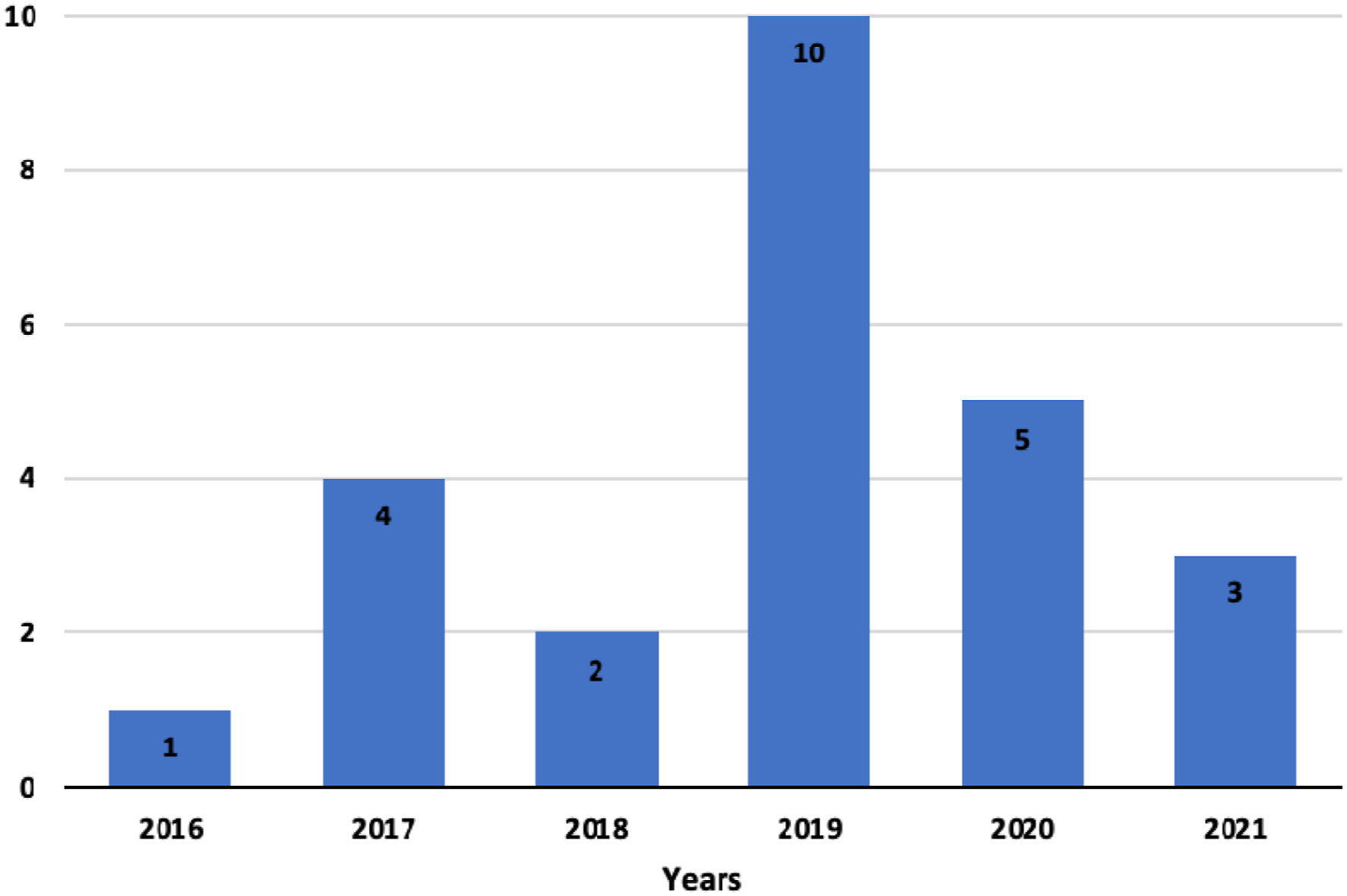
Articles included by year of Publication.
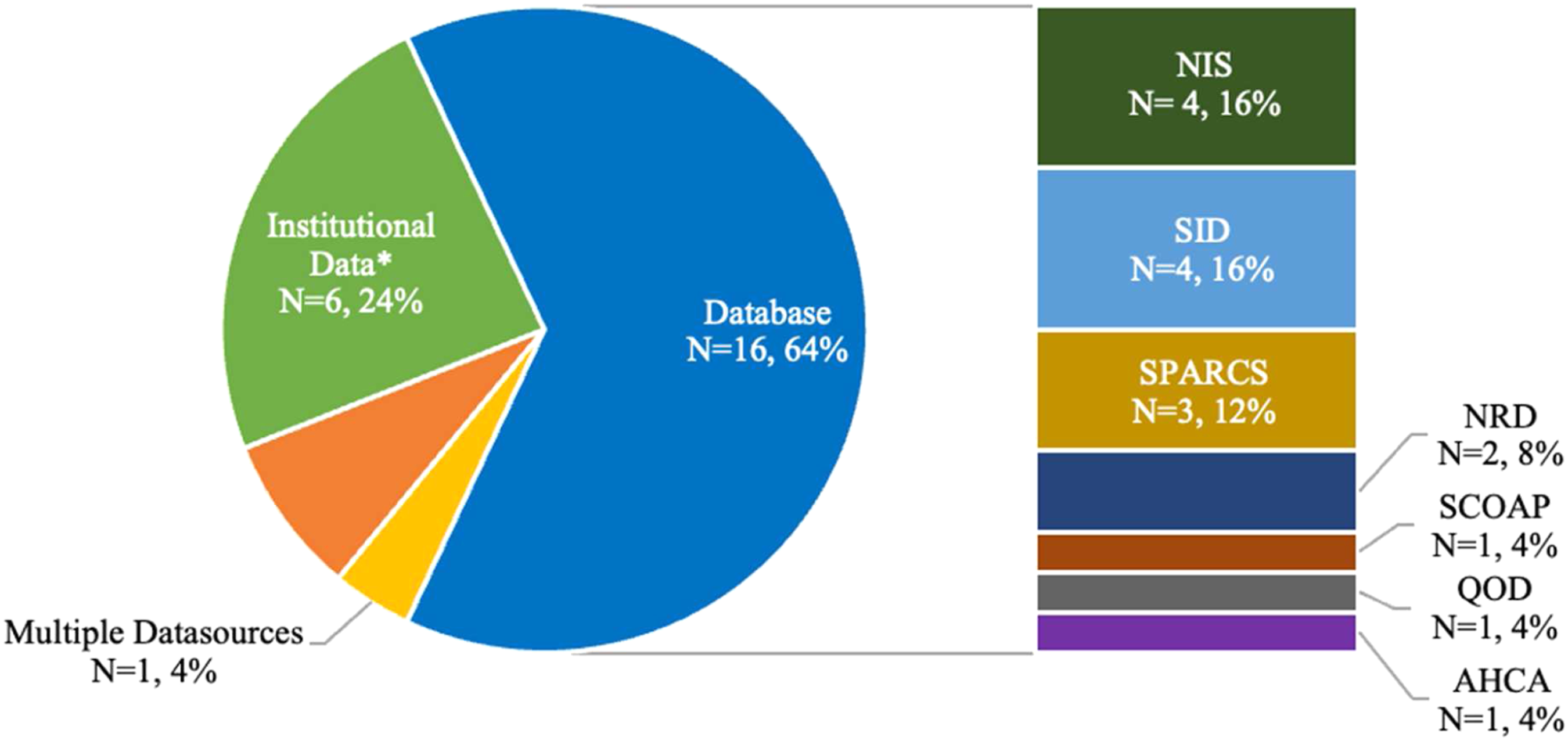
Articles included by data source.
Studies Reporting on Disparities in Access to Lumbar Fusion and Anterior Cervical Discectomy and Fusion in Medicaid Beneficiaries.
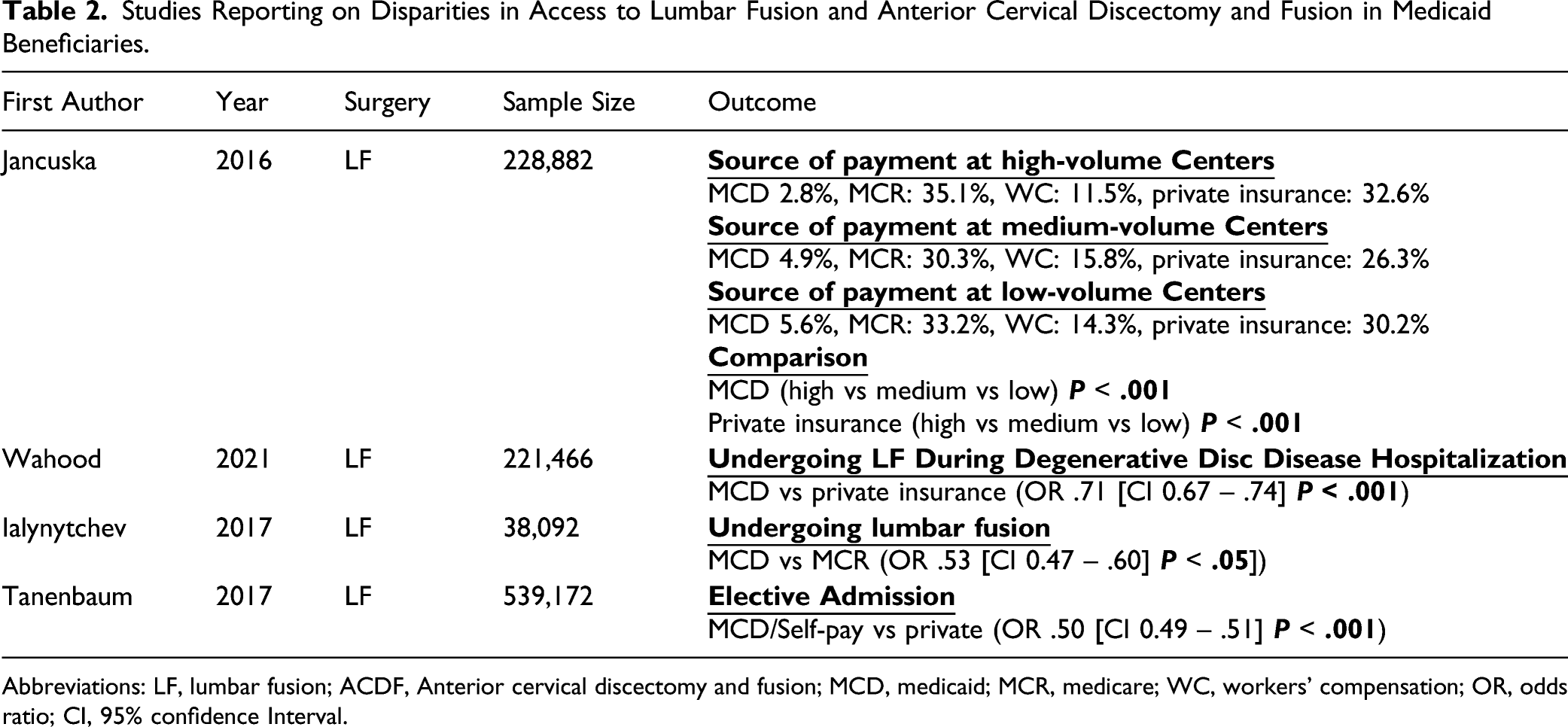
Abbreviations: LF, lumbar fusion; ACDF, Anterior cervical discectomy and fusion; MCD, medicaid; MCR, medicare; WC, workers’ compensation; OR, odds ratio; CI, 95% confidence Interval.
Studies Reporting on Disparities in Costs and Reimbursement of Lumbar Fusion and Anterior Cervical Discectomy and Fusion in Medicaid Beneficiaries.
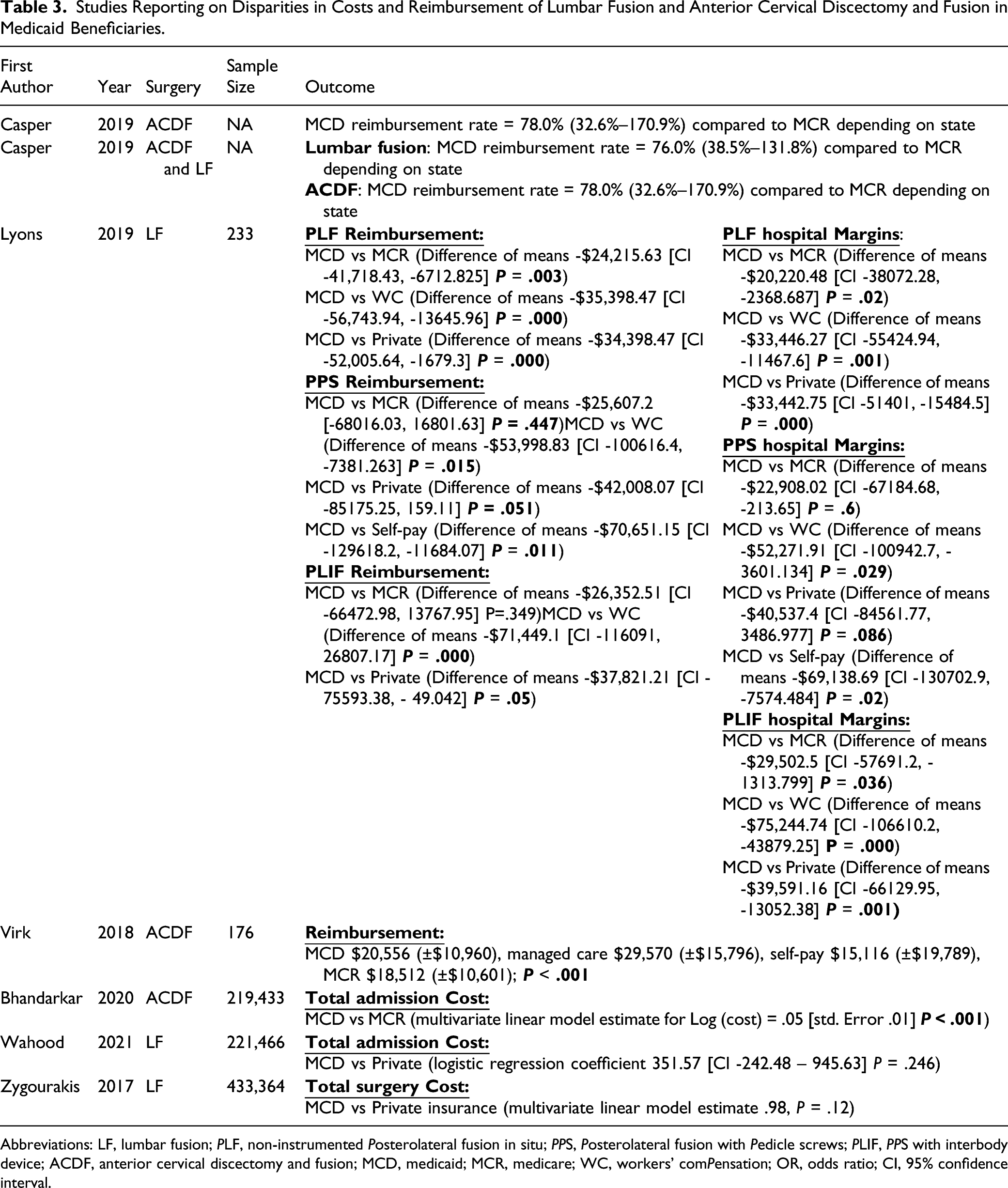
Abbreviations: LF, lumbar fusion; PLF, non-instrumented Posterolateral fusion in situ; PPS, Posterolateral fusion with Pedicle screws; PLIF, PPS with interbody device; ACDF, anterior cervical discectomy and fusion; MCD, medicaid; MCR, medicare; WC, workers’ comPensation; OR, odds ratio; CI, 95% confidence interval.
Studies RePorting on DisParities in Outcomes of Lumbar Fusion and Anterior Cervical Discectomy and Fusion in Medicaid Beneficiaries.
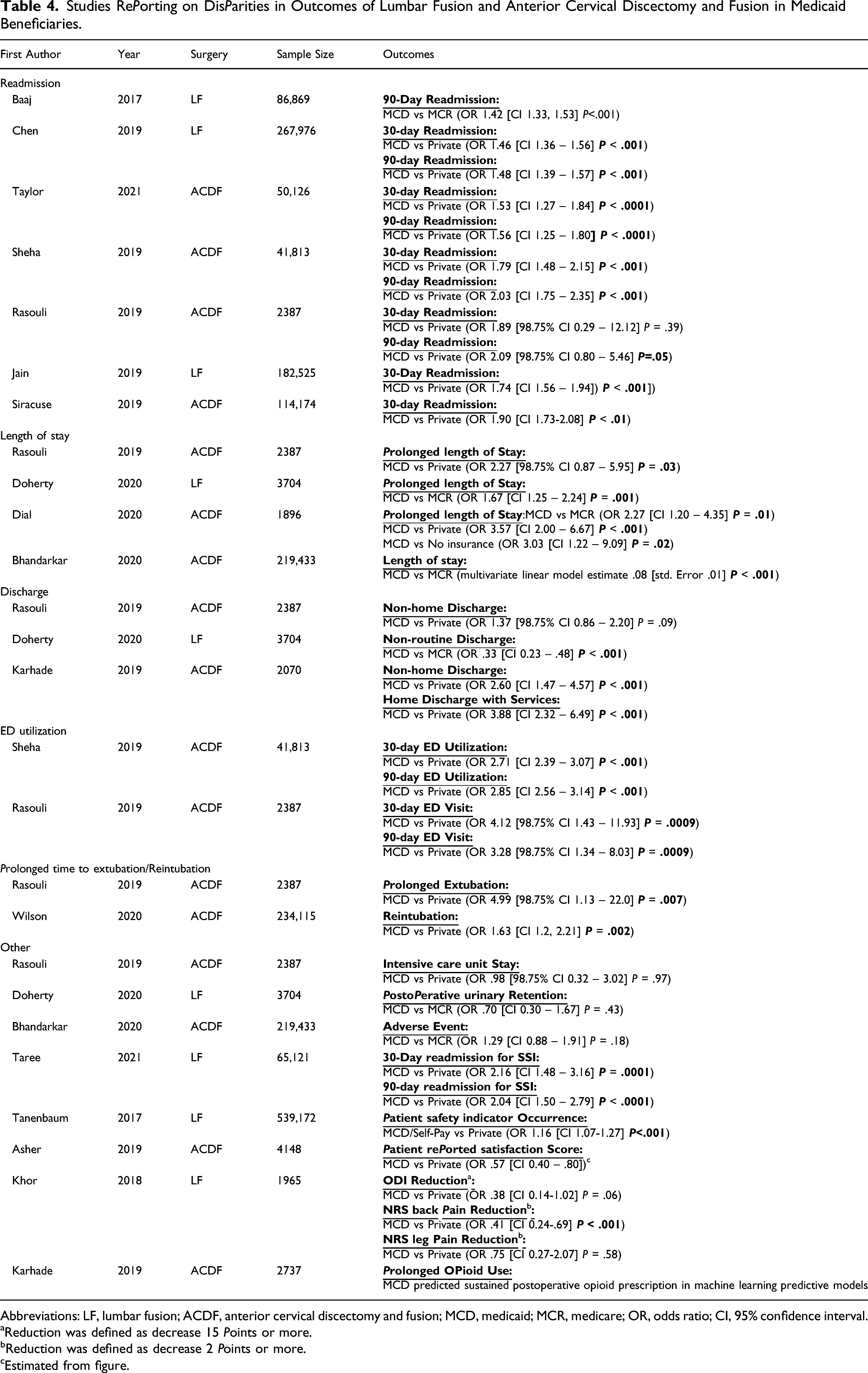
Abbreviations: LF, lumbar fusion; ACDF, anterior cervical discectomy and fusion; MCD, medicaid; MCR, medicare; OR, odds ratio; CI, 95% confidence interval.
aReduction was defined as decrease 15 Points or more.
bReduction was defined as decrease 2 Points or more.
cEstimated from figure.
Access
Four studies reported on the disparities in access to LF.10,12,15,22 three found that Medicaid was associated with a lower likelihood of undergoing LF surgery compared to other insurance types,10,12,22 and 1 found a lower odds of elective admission among Medicaid patients (Table 2). 15
Wahood et al 22 analyzed data from the National Inpatient Sample (NIS) and found that Medicaid admits were less likely to undergo LF during admission for disc disease compared to privately insured admits (OR .71, P < .001). Ialynytchev et al. performed a case-control study utilizing LF patients from the Florida Agency for Health Care Administration (AHCA) database. They found that Medicaid was associated with a lower likelihood of undergoing LF procedures compared to Medicare (OR .53, P < .05]). 12 Jancuska et al. examined LF procedures using the New York Statewide Planning and Research Cooperative System (SPARCS) data and compared insurance coverage of patients treated at low-volume centers and high-volume centers. They found that private insurance was over-represented at high volume-centers while Medicaid was over-represented at low-volume centers where LF procedures are less commonly performed and outcomes tend to be inferior (P < .001) (Table 2). 10 Tanenbaum et al 15 examined LF patients using NIS data and found that Medicaid/self-pay patients were less likely to be admitted electively relative to privately insured patients (OR .50, P < .001).
Reimbursement/Costs
Seven studies reported on the disparities in reimbursement and costs (Table 3).13,22-27
Four studies found that reimbursement rate was lower for Medicaid patients compared to other insurance types.23-25,27 Casper et al. 23 performed an online web search and found that average ACDF reimbursement rate for Medicaid patients is around 78% compared to Medicare patients. In another study, Casper et al 24 analyzed the same data for LF procedures and found a 76.0% ratio of Medicaid to Medicare reimbursement. Lyons et al 25 performed a retrospective chart review of a single institution and found that Medicaid reimbursed hospitals less than Medicare, workers’ compensation, and private insurers for all 3 LF procedures studied. Further analysis showed that hospital margins were lowest for Medicaid patients compared to other payer categories (Table 3). Virk et al 27 studied ACDF data from a single tertiary care center and found lower average reimbursement for Medicaid ($20,556) compared to managed care ($29,570) (P < .001).
Three studies examined costs.13,22,26 Bhandarkar et al 13 analyzed NIS data and found that Medicaid was associated with increased admission cost for ACDF compared to Medicare (P < .001). In contrast, Zygourakis et al. and Wahood et al. examined LF patients and found no difference in mean total costs between Medicaid and private insurance patients.22,26
Health Outcomes
Seventeen studies reported on the associations of Medicaid with various perioperative LF or ACDF outcomes. All studies concluded that Medicaid was associated with worse health outcomes (Table 4).11,13-18,28-37
Readmission and emergency department utilization
Five studies examined rates of unplanned readmission and emergency department (ED) utilization. They all found higher rates of readmission or ED utilization among Medicaid beneficiaries compared to other insurance types.14,17,30-32 Baaj et al. and Chen et al. utilized national databases and found that Medicaid patients were more likely to have unplanned 30-day and 90-day readmissions post-LF when compared to Medicare and privately insured patients (Table 4).30,31 Taylor et al. and Sheha et al. utilized national databases while Rasouli et al. used data from a single institution.14,17,32 The 3 studies found a higher odds for unplanned readmission and ED visits for Medicaid post-ACDF compared to private insurance (Table 4).14,17,32
Two studies created prediction tools for readmission after ACDF and LF procedures using State Inpatient Databases (SID).28,29 Both tools predicted that Medicaid incurred higher risk of readmission.28,29 Jain et al. created and validated a prediction tool for 30-day readmission after LF. Medicaid insurance incurred the highest risk for readmission among other insurance types (OR 1.74 vs private insurance, P < .001). 28 Siracuse et al. developed a predictive risk scale for 30 day-readmission after ACDF surgery and found an odds ratio of 1.90 (P < .01) for Medicaid compared to private insurance. Their scale explained 97.1% of the variability in readmission rate, and the presence of Medicaid insurance imparted the highest increase in risk among more than 20 other variables. 29
Reintubation/extubation
Two studies reported on the risk of reintubation or prolonged extubation post-ACDF.17,33 Wilson et al 33 examined a cohort of patients in the Premier Healthcare Database and found that, compared to private insurance, Medicaid was associated with reintubation following ACDF on multivariate analysis (OR 1.63; P = .002). Rasouli et al 17 found higher rates of prolonged extubation in Medicaid patients compared to privately insured patients (OR 4.99; P = .007).
Prolonged length of stay
Four studies reported on prolonged length of stay in Medicaid beneficiaries.11,13,17,34 Doherty et al. utilized SID data and found an increased risk of prolonged length of stay post-LF in Medicaid vs Medicare beneficiaries (OR 1.67, P = .001). Rasouli et al 17 found that Medicaid patients had higher odds prolonged length of stay (OR 2.27, P = .03) than the private patients in a single institution post-ACDF. Dial et al 34 examined ACDF patients at a single institution and found that Medicaid was associated with higher risk of prolonged length of stay compared to Medicare (OR 2.27, P = .01), private insurance (OR 3.57, P < .001) and no insurance (OR 3.03,P = .02). Bhandarkar et al 13 assessed NIS patients undergoing ACDF and found that Medicaid was associated with a longer length of stay compared to Medicare and private insurance on multivariate linear analysis (P < .001).
Discharge
Three studies reported on discharge of Medicaid beneficiaries.11,16,17 A study by Karhade et al 16 utilized data from 5 centers and found that Medicaid insurance had higher odds of non-home discharge (OR 2.60, P < .001) and discharge with services (OR 3.88, P < .001) compared to private insurance after ACDF. In contrast, Rasouli et al 17 found no difference between Medicaid and private insurance with regards to non-home discharge post-ACDF. On the other hand, Doherty et al 11 found a decreased rate of non-routine discharge in Medicaid vs Medicare post-LF (OR .33, P < .001).
Other
Seven studies reported on other outcomes.11,15,17,18,35-37
Taree et al 35 utilized the National Readmission Database and found that Medicaid was associated with higher rate of surgical site infection requiring readmission within 30-days (OR 2.16, P = .0001) and 90-days (OR 2.04, P < .0001) post-LF compared to private insurance.
Tanenbaum et al 15 examined LF patients using NIS data and found that the odds of experiencing 1 or more Patient Safety Indicators (PSI), or adverse events, was greater for the Medicaid/self-pay cohort relative to the privately insured cohort on multivariate analysis (OR 1.16, P < .001).
Asher et al 36 queried the Quality Outcome Database (QOD) for ACDF patients and found that Medicaid patients had lower satisfaction scores compared to privately insured patients. Khor et al 18 combined data from the Surgical Care Outcomes Assessment Program (SCOAP) and patient reported outcome data and found that Medicaid patients were less likely to report improved back pain (OR .41, P < .001) post-LF. Karhade et al 37 utilized data from 5 centers to develop machine learning algorithms that predict prolonged opioid use after ACDF surgery. On global model explanation, Medicaid was among the most important predictors for prolonged opioid use.
Other findings among the aforementioned studies were absence of association between Medicaid and Intensive Care Unit admission, 17 post-operative urinary retention, 11 Oswestry Disability Index scores and leg pain scores, 18 and adverse events 13 (Table 4).
Discussion
We conducted a systematic review to synthesize studies examining the disparities that impact Medicaid beneficiaries with regards to 2 common elective spine procedures. Specifically, we uncovered disparities in access to surgery, in reimbursement rates, and in health outcomes. Overall, we found that the overwhelming majority of research, if not all, found significant disadvantages associated with Medicaid insurance. These findings were replicated in large database studies, multicenter studies, and single institution studies. Medicaid was predictive of less access to ACDF and LF surgery, lower reimbursement rates, and worse health outcomes. All our studies were relatively recent, with the oldest being from 2016. This speaks of the recently increased interest in studying disparities in spine surgery. With the increasing importance of spine surgery for the ageing population, highlighting such disparities is vital to developing interventions that can minimize them and their impact on patients.
In our review, all studies examining access to care found that Medicaid beneficiaries sustain decreased access to LF and ACDF surgery. Previous work has shown that despite the implementation of the Affordable Care Act (ACA), Medicaid beneficiaries suffer from lower rates of access to general healthcare.38,39 1 reason could be the reluctance of healthcare systems to increase Medicaid coverage. A study by Sommers found that one third of primary healthcare providers did not accept new Medicaid patients in 2011-2012. 38 Later work by Neprash et al 40 found that despite increased coverage after the 2014 ACA expansion, most primary physicians did not increase their share of Medicaid patients. An article published in the New England Journal of Medicine noted that there are narrow networks of providers accepting Medicaid patients, 39 and those networks often have difficulty securing specialist providers. 41 Similar to our findings in elective spine surgery, this decreased access to healthcare has also been mirrored in various subspecialties within orthopedic surgery, with research showing greatly increased waiting times and lack of access to care in Medicaid patients.42-45 For instance, several “mystery caller” studies have shown that Orthopedic patients are less likely to be successful in scheduling appointments if they stated that they had Medicaid insurance.42,46 Wiznia et al 46 conducted a mystery caller study and found a surprising 27% success rate in securing appointments with an Orthopedic specialist for Medicaid compared to 91% for private insurance.
Our synthesis of reimbursement rates showed large differences, with Medicaid rates consistently lower than those of other payer groups (Table 3). This was coupled with sizably lower hospital margins for Medicaid patients reported by 1 of the studies in our review (Table 3). 25 Although these findings are not surprising, they could provide insight into the causes of decreased access to care by Medicaid patients. A study examining physician perceptions found that low reimbursement rates, inadequate financial resources, and poor coverage policies are sources of low provider satisfaction and reluctance to accept Medicaid patients. 47 Another study found that Medicaid physician fees remained substantially below Medicare fees in 2019. 48 The authors concluded that this could have important implications, not only on access to care for Medicaid enrollees, but also on proposals to expand coverage through Medicaid buy-in. 48
With regards to health outcomes, our review strongly shows that Medicaid insurance was predictive of worse perioperative outcomes. This included prolonged length of stay, lower satisfaction and outcome scores, higher pain scores, and higher odds of readmission, emergency department visits, surgical site infections, prolonged opioid use, and reintubation. The roots of these disparities are likely multifactorial, with numerous causes at play. One reason might be that Medicaid patients are more likely to be of lower socioeconomic status, which has been shown to be a major contributor to worse overall health and higher comorbidity burden.49-52 Another modifiable factor could be the tendency of Medicaid patients to be treated at less experienced low-volume centers, as shown by 1 study in our review. 10 A study by Spivack et al 53 concluded that practices with large patient base outside of Medicaid may be less inclined to accept Medicaid patients. This could be causing experienced high-volume centers which offer expensive treatment to other payer groups, particularly private insurances, to be less inclined to treat Medicaid patients. Interestingly, previous authors have noted that since Medicaid patients have worse outcomes, quality metrics for hospitals that treat more Medicaid patients could be adversely skewed, negatively impacting hospital ranking, reimbursement, and surgeon performance metrics, as compared to hospitals that treat more privately insured patients.17,49 This likely acts as a deterrent to establishing wide Medicaid coverage by highly-ranked hospitals and providers. Finally, access to technology, education level, and cultural, social, and language barriers are thought to play a role in the observed disparities.14,50,54
Our results are analogous to findings outside the United States. A study from Qatar, a country with both subsidized public and for-profit private insurance, found that better insurance coverage was associated with higher healthcare utilization. 55 The authors concluded that improving health coverage for disadvantaged populations may reduce healthcare disparities. 55 On the other hand, an analysis of the South Korean health system, which provides universal health insurance, found that lower income was associated with a higher incidence of preeclampsia and postpartum hemorrhage among pregnant women. 56 This suggests that lower socioeconomic status in centralized insurance systems may be analogous to Medicaid insurance status in the United States. In other words, although healthcare systems with centralized coverage may not have disparities related to insurance status, they do reflect those disparities with economic status instead. Umeh et al. performed a systematic review of community-based health insurance, a scheme designed to increase access to healthcare for rural communities, in over 8 low- and middle-income countries. 57 They found that higher economic status was strongly associated with higher willingness-to-pay and higher enrollment in these insurance systems, as well as higher healthcare utilization and lower drop-out rate. 57 Overall, our findings may reflect a global problem of socioeconomic disparities that manifests itself differently in different health systems.
Fiscella et al. proposed 5 principles for reducing disparities in healthcare. 49 Besides the need for research that highlights disparities, they pointed to the need for approaches that try to adjust for socioeconomic imbalances. For instance, deprived areas could receive higher reimbursement rates to compensate for the higher healthcare needs and higher rate of medical complexity and morbidity. 49 The authors also noted the importance of using quality measures that take socioeconomic status into account, so that measures for disadvantaged populations are not skewed based on the comorbidities when compared to the general population. 49 Other proposed measures to reduce disparities have included implementing tools to measure and monitor for disparities in care, promoting diverse healthcare workforce, and producing research that identifies disparities, such as this present work.58,59 To our knowledge, this is the first systematic review to synthesize literature on the disparities associated with Medicaid insurance in spine surgery.
This study has several limitations. Firstly, our strict inclusion criteria caused exclusion of numerous studies that examine other types of elective spinal surgery. Secondly, the quality and heterogeneity of reported measures made conducting a metanalysis difficult. Thirdly, most of the articles did not focus on associations with insurance as a primary aim; therefore, our data is drawn from secondary analyses. Lastly, all our studies were level 3 to 4 evidence and were observational in nature, which could limit conclusive determinations. Still, the strongly coherent literature and the repeated replication of the disparities in Medicaid populations grant confidence in our conclusions. Moreover, most studies included were based on large national databases with large sample sizes and strongly significant results.
Conclusion
Medicaid insurance is associated with significant disadvantages with regards to ACDF and LF spinal procedures. In our systematic review, Medicaid was predictive of less access to surgery, lower reimbursement rates, and worse health outcomes. These findings warrant close examination of the roots of inequities in spine surgery to produce interventions that can ameliorate these disparities.
Footnotes
Acknowledgments
We thank Carrie L. Price, MLS, at the Johns Hopkins Welch Medical Library for her assistance in developing the search strategy utilized in this systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by NIH National Institute on Aging under Award Number P01AG066603 and by the Gladden Society Research Grant.
Authors’Note
This work was performed at the Department of Orthopaedic Surgery, Johns Hopkins University, Baltimore, MD