
Abstract
Study Design
Retrospective Analysis.
Objective
The National Surgical Quality Improvement Program (NSQIP) database was used to determine whether race and ethnicity (R&E) are independent predictors of postoperative complications following spine surgery.
Methods
Demographic, comorbidity, and complication data were compared by R&E using chi-square and Kruskal-Wallis tests. Complications and postoperative categorical variables were combined and compared with logistic regression by R&E. Hospital times data was compared with both Kruskal-Wallis and linear regression. Regressions all controlled for age, weight, sex, and comorbidities. All R&E groups were compared to White patients.
Results
181,913 White, 21,501 Black, 10,710 Hispanic, 5611 Asian, 1249 Native American (NA), and 628 Native Hawaiian (NH) patients were in our analysis. Black patients experienced the highest rates of dyspnea (4.86%), diabetes (24.95%), and hypertension (63.49%), which was significantly different from the other groups (all P < 0.0001). Regression analyses revealed that Black patients experienced higher respiratory, urinary, cardiovascular, septic complications, and postoperative events compared to White patients (Odds ratio (OR) = 1.55, 1.35, 1.32, 1.29, 1.22; all P ≤ 0.0072). Hispanic patients had lower wound complications but higher urinary complications and postoperative events (OR = 0.82, 1.23, 1.11; all P ≤ 0.041). Asians had lower respiratory, cardiovascular complications, and postoperative events (OR = 0.66, 0.65, 0.79; all P ≤ 0.030). Native Americans had higher rates of wound, septic complications, and postoperative events (OR = 1.88, 1.96, 1.29; all P ≤ 0.033).
Conclusions
R&E predicts postoperative complication disparities following spine surgery. Black, Hispanic, and Native American patients have higher odds of complications. Targeted interventions focusing on perioperative care are needed to improve health equity.
Keywords
Introduction
Racial and ethnic disparities in healthcare have been well-documented across various medical fields, demonstrating that patients from minority groups often experience inferior outcomes compared to their White counterparts. Dickman et al 1 found that health disparities between White and Black patients have persisted for over 60 years, with growing inequities in healthcare visits, hospitalizations, and medical expenditures. In orthopedics, Amen et al 2 reported that Black patients were less likely to receive total knee and hip arthroplasties than White patients. This was supported by a meta-analysis showing disparities in surgery rates and outcomes for Black and Hispanic patients. 3 Another study found that differences in access to healthcare might be the source of the racial inequalities exhibited in the outcomes of rotator cuff surgeries. 4 In spine surgery, research has shown similar patterns of disparities but often focuses on a limited range of procedures or specific racial groups. Prior analyses have examined disparities in outcomes regarding anterior cervical discectomy and fusion, leaving a need to fill the gap on how these disparities manifest across a broader spectrum of spine surgeries. 5 Recent studies have also been limited to differences in postoperative outcomes among a limited number of racial and ethnic groups. In contrast, comprehensive analyses that include the full spectrum of spinal surgery across a more diverse group of racial and ethnic classifications such as Native Hawaiian & Pacific Islanders, Native American & Alaskan Native, and Asians have been notably absent.
This study aims to determine whether racial and ethnic identity independently predicts adverse postoperative outcomes following spinal surgeries by analyzing data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). Through a comprehensive analysis of patient data from 2015–2020, this paper sheds light on how racial and ethnic disparities persist in modern spine surgery and identifies specific areas where strategic, evidence-based interventions may be necessary to improve postoperative outcomes and advance health equity in spine surgery.
Methods
American College of Surgeons-National Surgical Quality Improvement Program Database
This study utilized patient data from the ACS-NSQIP Database from 2015 to 2020. This database contains over 200 data points per patient who underwent surgery at one of the over 600 sites nationwide participating in the program. All patients in the database have 30-day postoperative findings reported, which are collected from the patient’s charts and not insurance claims. This database has been validated in studies and is commonly used in surgical literature.6-9 All variables are defined in an extensive NSQIP user guide to standardize the reports input from trained clinical reviewers. Additionally, this study was approved by the Institutional Review Board (IRB) of Columbia University with IRB number AAAV2593. Informed consent was not required and waived by the local institutional board.
Inclusion and Exclusion Criteria
We initially included all patients with a primary Current Procedure Terminology (CPT) code relevant to spine surgery and had their surgeries performed from 2015 to 2020. A complete listing of the 131 different CPT codes used in this analysis can be found in the Appendix. Patients with missing information pertinent to our study, such as age, weight, race, and more, were removed according to complete case analysis. Additionally, patients with preoperative steroid use within 30 days of surgery, active wound infections, sepsis, those undergoing emergency procedures, those with congestive heart failure, renal failure, on dialysis, disseminated cancer, on a ventilator, and those with unexplained weight loss or a transfusion within 30 days before their surgery were excluded to better isolate the impact of race and ethnicity on outcomes.
Race and Ethnicity Classification
Each patient in the database has a variable for race and another for whether they are ethnically Hispanic. Combining these variables, patients were put into 1 of 6 racial and ethnic groups: White, Black or African American (Black), Hispanic, Asian, Native American or Alaskan Native (Native American), and Native Hawaiian or other Pacific Islander (Native Hawaiian). All patients identified as Hispanic were put into the Hispanic group, irrespective of their inputted race.
Data of Interest
After dividing the study population into different racial and ethnic (R&E) groups, demographic data such as age, sex, height, and weight and derived data such as the patient’s mortality and morbidity probability were retrieved. BMI was calculated from height and weight. Additionally, data related to comorbidities (smoking, dyspnea, functional status impairments, diabetes, hypertension, chronic obstructive pulmonary disease (COPD), bleeding disorders), hospital times (operative time and total hospital length of stay), postoperative events (return to the operating room, unplanned readmission, and same year mortality) were retrieved. Lastly, various 30-day postoperative complications, including wound complications (superficial, deep incisional, organ space surgical site infections (SSI), and wound disruptions), respiratory complications (pneumonia, unplanned reintubation, pulmonary embolism, remaining on a ventilator over 48 hours post-operation), urinary tract complications (progressive renal insufficiency, acute renal failure requiring dialysis, and urinary tract infections), central nervous system occurrences (stroke), cardiovascular complications (cardiac arrest, myocardial infarction, and venous thrombosis requiring therapy), and septic complications (sepsis and septic shock) were collected. Patients were only considered to have developed a postoperative complication if the complication was absent before surgery.
Statistical Analysis
Patients were analyzed according to the 6 different racial and ethnic groups. Chi-square tests were used to compare categorical variables such as sex, smoking, and individual complications. Kruskal-Wallis tests were used to compare continuous variables such as age, BMI, and total hospital length of stay. Multivariate analyses were performed to study whether R&E are independent predictors of adverse outcomes. Logistic regression was used to analyze the postoperative events and combined categories of complications only, referred to as combined occurrences. These combined occurrences were postoperative events, wound, respiratory, urinary tract, cardiovascular, and septic complications grouped as described in the Data of Interest section. Linear regression was used to analyze operative time and total hospital length of stay. Regression models controlled for age, weight, sex, smoking, dyspnea, diabetes, hypertension, COPD, and bleeding disorders. The odds ratio (OR) and 95% confidence intervals (CI) for the combined occurrences were calculated for the logistic regressions. The beta coefficient (β) with 95% CI was also calculated for the operative time and total hospital length of stay for linear regression. Significance was set at a P-value of less than 0.05. All statistical analyses and figures were made using R, version 4.4.0. 10
Results
Patient Demographics and Comorbidities Analysis
Comparison of Demographics and Comorbidities Between Racial and Ethnic Groups (N = 221 612)
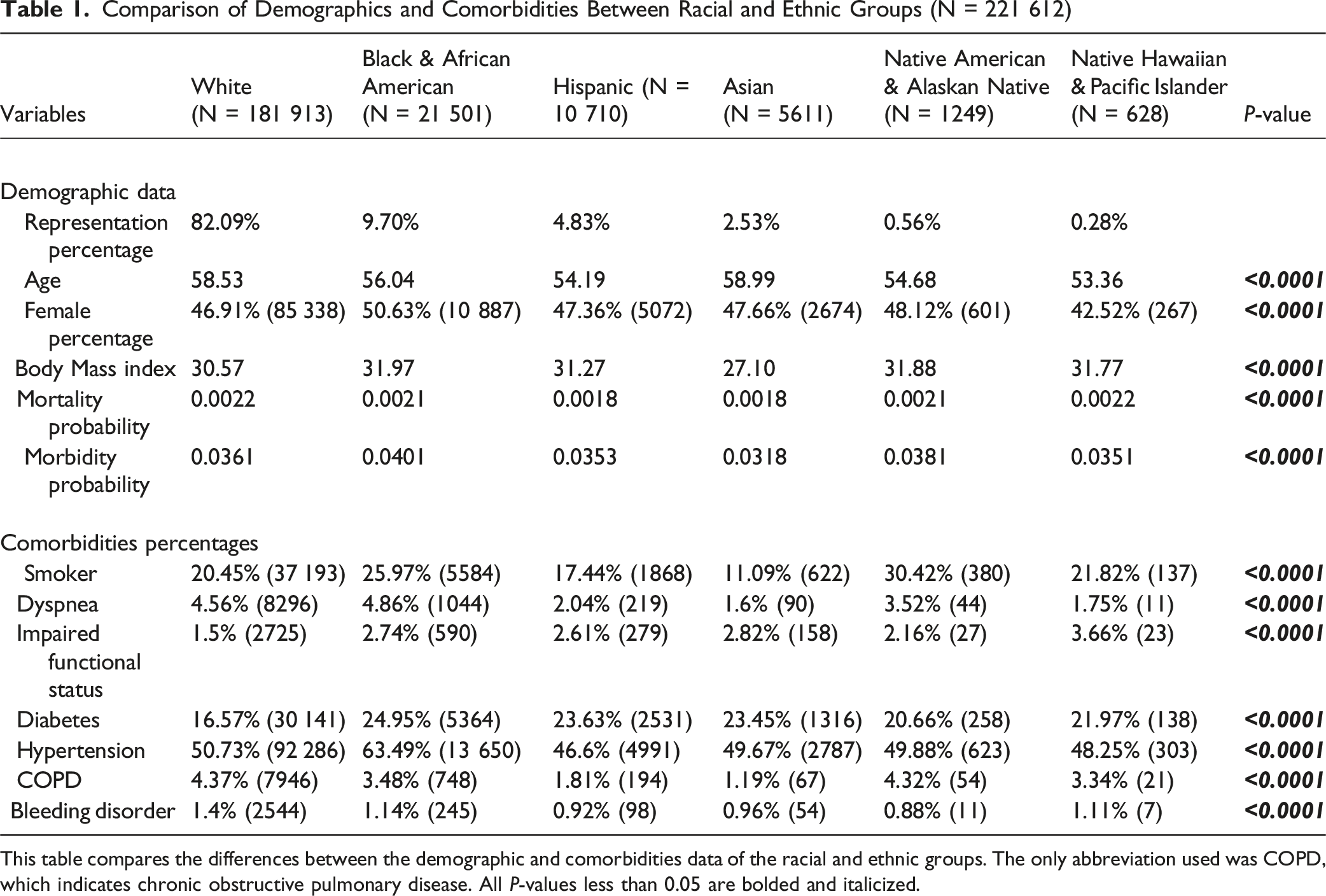
This table compares the differences between the demographic and comorbidities data of the racial and ethnic groups. The only abbreviation used was COPD, which indicates chronic obstructive pulmonary disease. All P-values less than 0.05 are bolded and italicized.
We first analyzed the patients’ demographic and comorbidity data according to their R&E. Significant differences were found when comparing the average age, female percentage, BMI, and mortality probability and morbidity probability (all P < 0.0001). White and Asian patients were older than other groups (58.53 and 58.99, respectively), Native Hawaiians had the lowest female representation (42.52%), Asian patients had the lowest BMIs (27.10), and Black patients had the highest morbidity probability (0.0401) (Table 1).
All comorbidities significantly differed among the groups (all P < 0.0001). White patients had the highest rates of COPD (4.37%) and bleeding disorders (1.4%) but the lowest impaired functional status (1.5%) and diabetes rates (16.57%). Black patients had the highest rates of dyspnea (4.86%), diabetes (24.95%), and hypertension (63.49%). Hispanics had the lowest rates of hypertension (46.6%). Asians had the lowest rates of smoking (11.09%), dyspnea (1.6%), and COPD (1.19%). Native Americans had the highest smoking rates (30.42%), second highest COPD rates (4.32%), and lowest bleeding disorders (0.88%). Lastly, Hawaiian patients had the highest rates of impaired functional status (3.66%) (Table 1).
Operative and Postoperative Variables Analysis
Comparison of Operative and Postoperative Events Between Racial and Ethnic Groups (N = 221 612)
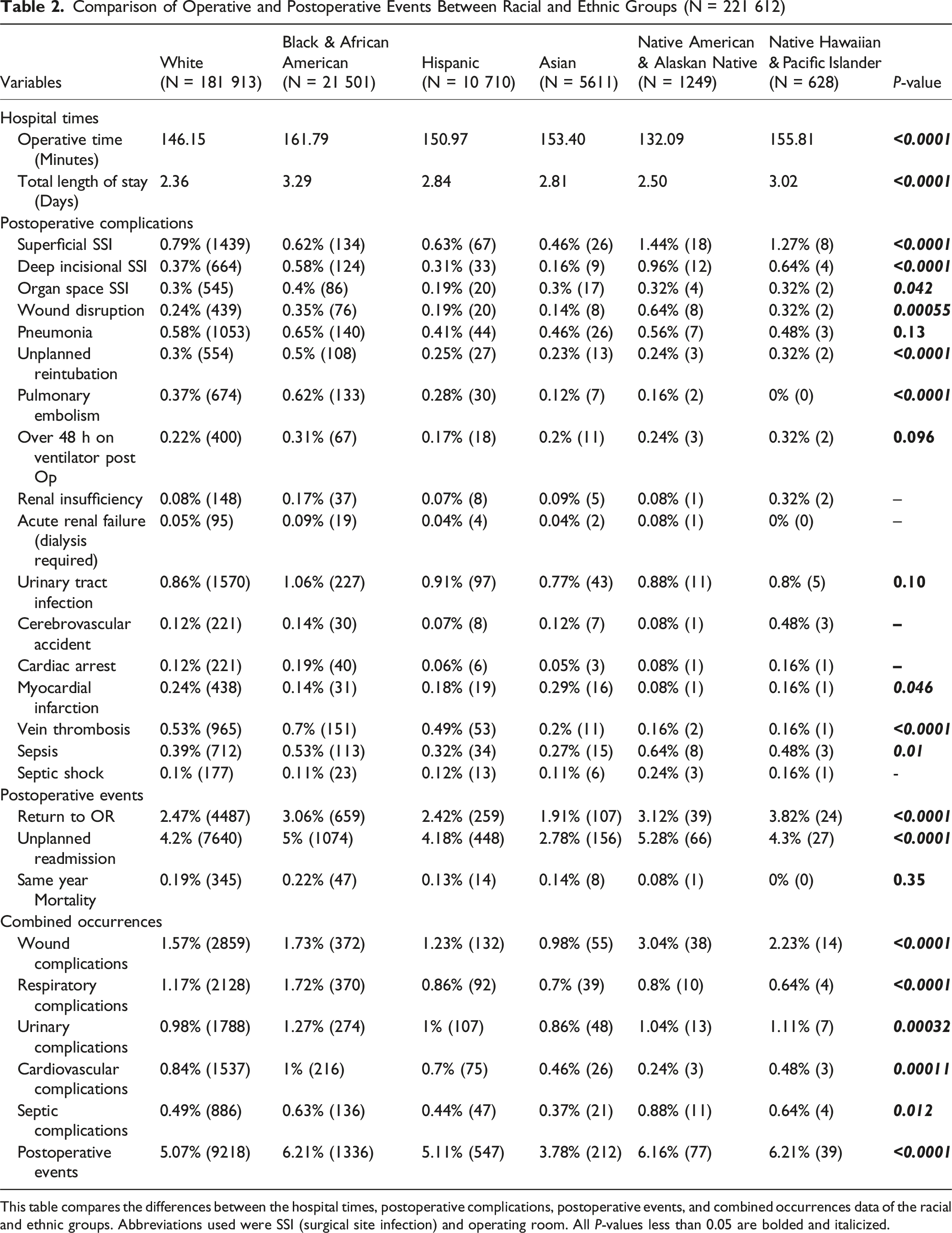
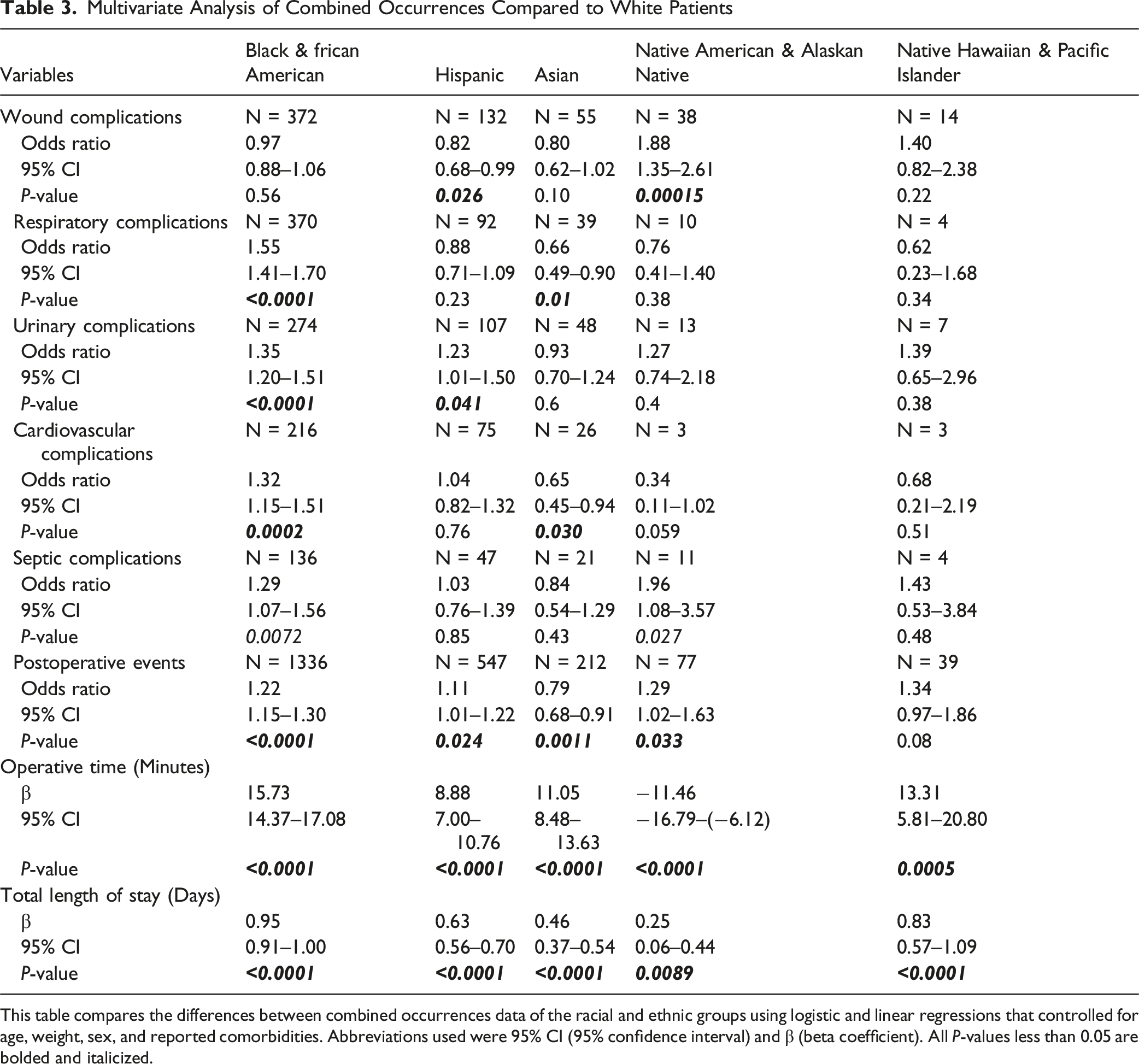
This table compares the differences between the hospital times, postoperative complications, postoperative events, and combined occurrences data of the racial and ethnic groups. Abbreviations used were SSI (surgical site infection) and operating room. All P-values less than 0.05 are bolded and italicized.
Multivariate Analyses
We analyzed R&E’s effect on hospital times and combined occurrence variables with linear and logistic regression. All analyses used White patients as the reference variable. Black patients had significantly more respiratory (OR = 1.55, 95% CI = 1.41 to 1.70), urinary (OR = 1.35, 95% CI = 1.20 to 1.51), cardiovascular (OR = 1.32, 95% CI = 1.15 to 1.51), septic complications (OR = 1.29, 95% CI = 1.07 to 1.56), and postoperative events (OR = 1.22, 95% CI = 1.15 to 1.30) (P < 0.0001, P < 0.0001, P = 0.0002, P = 0.0072 and P < 0.0001, respectively). Hispanic patients had significantly fewer wound complications (OR = 0.82, 95% CI = 0.68 to 0.99) but more urinary complications (OR = 1.23, 95% CI = 1.01 to 1.50) and postoperative events (OR = 1.11, 95% CI = 1.01 to 1.22) (P = 0.026, P = 0.041, and P = 0.024, respectively). Asian patients had significantly fewer respiratory (OR = 0.66, 95% CI = 0.49 to 0.90) and cardiovascular complications (OR = 0.65, 95% CI = 0.45 to 0.94) and postoperative events (OR = 0.79, 95% CI = 0.68 to 0.91) (P = 0.01, P = 0.030, and P = 0.0011, respectively). Native American patients had significantly more wound (OR = 1.88, 95% CI = 1.35 to 2.61) and septic complications (OR = 1.96, 95% CI = 1.08 to 3.57) and postoperative events (OR = 1.29, 95% CI = 1.02 to 1.63) (P = 0.00015, P = 0.027, and P = 0.033, respectively). These data are displayed in Figure 1. Forest Plot of Multivariate Analysis of Combined Occurrences. This figure shows the Logistic Regression of the Combined Occurrences according to Race and Ethnicity. The Bars Represent the 95% CI of the Odds Ratio for Their Respective Group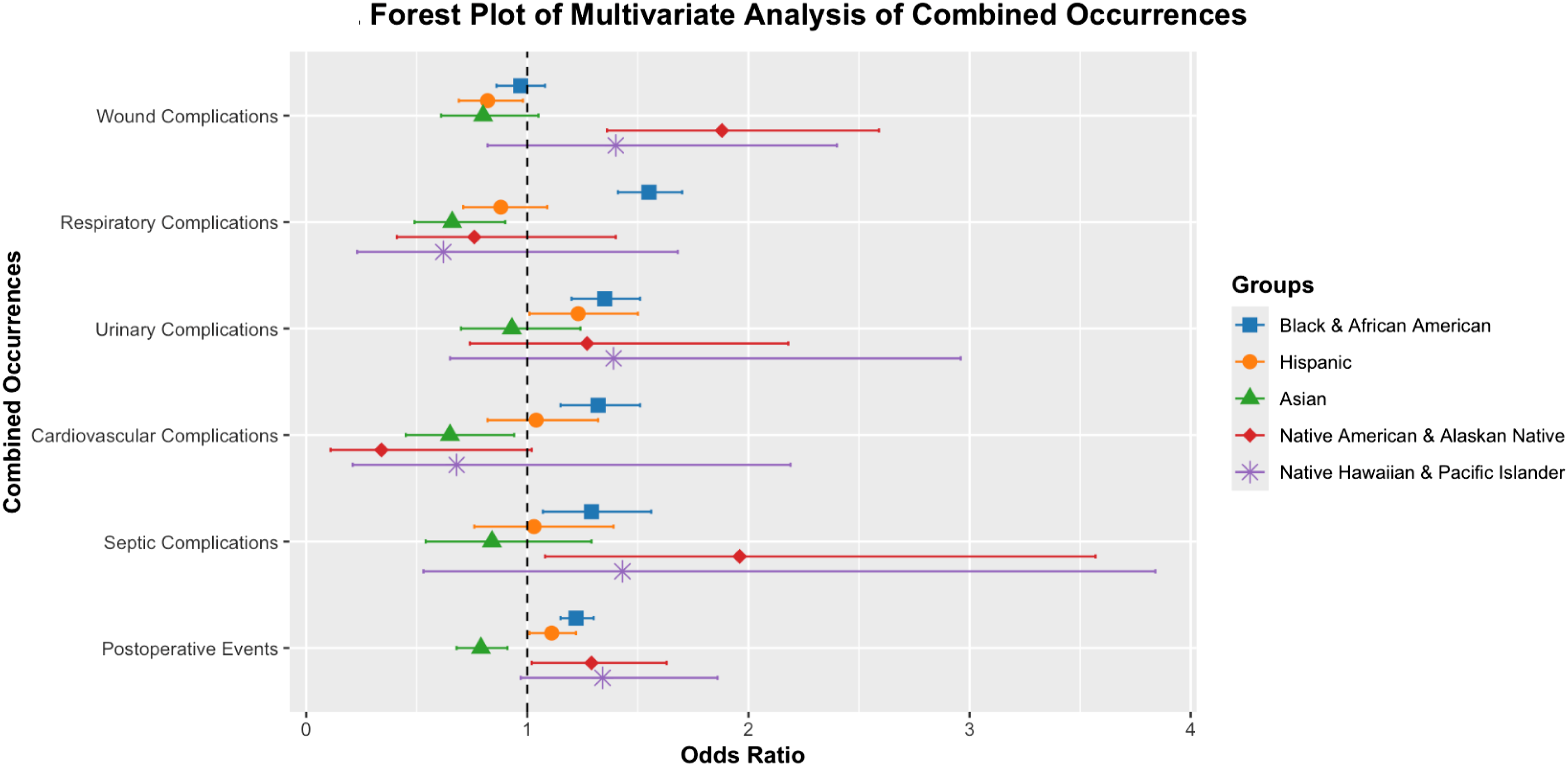
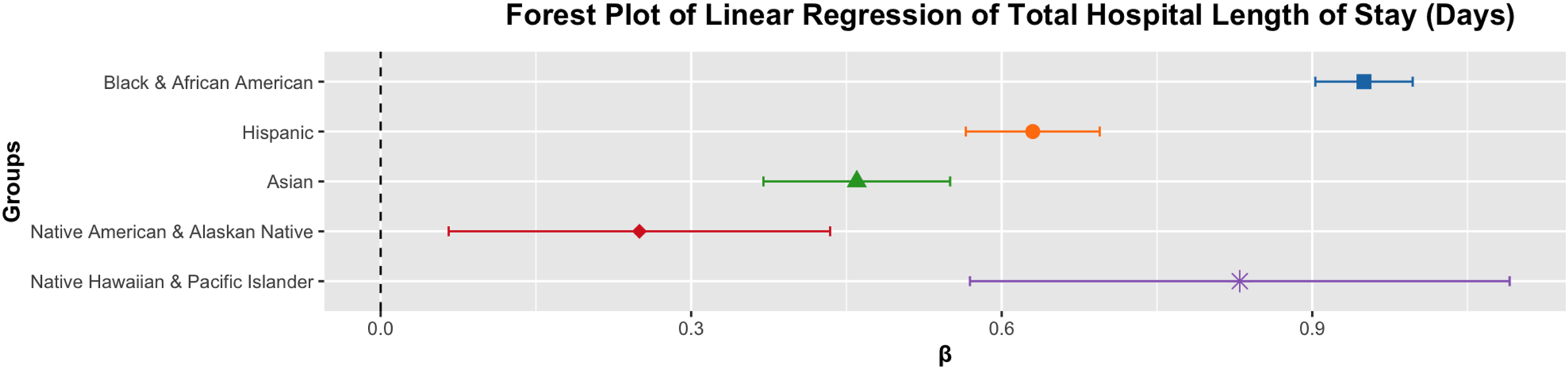
Operative times significantly differed for all R&E groups (all P ≤ 0.0005). Native American patients were the only group with shorter operative times (β = −11.46, 95% CI = −16.79 to −6.12). Figure 2 shows this operative time data in a forest plot. Lastly, all R&E groups had significantly different total hospital lengths of stay (all P ≤ 0.0089). All groups had longer total hospital lengths of stay, with the least prolonged stays of the R&E group being Native Americans (β = 0.25, 95% CI = 0.06 to 0.44) (Table 3). Figure 3 shows this length of stay data in a forest plot. Forest Plot of Linear Regression of Operative Time (Minutes) This figure shows the Linear Regression of the Operative Time (minutes) according to Race and Ethnicity. The Only Abbreviation Used is β (Beta Coefficient). The Bars Represent the 95% CI of the Odds Ratio for Their Respective Group Multivariate Analysis of Combined Occurrences Compared to White Patients This table compares the differences between combined occurrences data of the racial and ethnic groups using logistic and linear regressions that controlled for age, weight, sex, and reported comorbidities. Abbreviations used were 95% CI (95% confidence interval) and β (beta coefficient). All P-values less than 0.05 are bolded and italicized. Forest Plot of Linear Regression of Total Hospital Length of Stay (Days) This figure shows the Linear Regression of the Total Hospital Length of Stay (days) according to Race and Ethnicity. The Only Abbreviation Used is β (Beta Coefficient). The Bars Represent the 95% CI of the Odds Ratio for Their Respective Group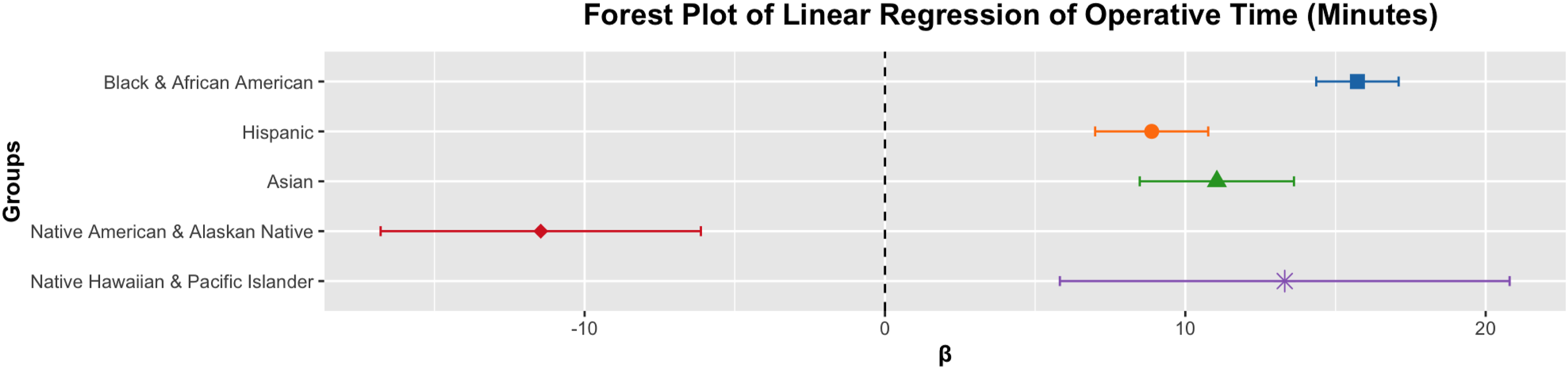
Discussion
Our analysis of the ACS-NSQIP data from 2015 to 2020 revealed significant racial and ethnic disparities in postoperative outcomes following spinal surgeries. Both Asian and White patients presented for spinal surgery at a later age compared to their peers (Table 1). This delayed presentation may indicate disparities in access to care, differences in cultural perceptions toward spine surgeries, or occupational factors. The Black patient cohort had a noticeably higher proportion of female patients (50.63%). Other research has shown that although women report higher rates of back pain compared to men, they often present for spine surgery less.11,12 Increased Black women representation in our study may indicate an increased disease burden for these patients. Furthermore, the disparity in Body Mass Index (BMI) across racial and ethnic groups was particularly notable, as Asian patients displayed the lowest average BMI. This observation aligns with previous studies, indicating a potential influence on uncontrolled surgical risk within this demographic. 13 Disparities were also noted in the comorbidity burden, such as the markedly higher prevalence of hypertension among Black patients (63.49%) and smoking among the Native American demographic (30.42%). This trend of increased prevalence of comorbidities being present within the Black community has risen over time from 1999 to 2018. 14 Additionally, our findings that Native Americans smoke more frequently than other racial and ethnic groups confirm other reported trends.15-17 These findings highlight the need for tailored preoperative and perioperative management strategies to mitigate these identified risk factors effectively.
Table 3’s multivariate analysis, adjusting for demographic and clinical factors, confirmed persistent disparities in postoperative outcomes. Black patients had a 55% higher risk of respiratory complications, 29% higher risk of septic complications, and 32% higher risk of cardiovascular issues compared to White patients, suggesting these disparities go beyond pre-operative health differences. A study by Phillips et al showed differential rates of interventions for treating pulmonary embolism for Black patients after controlling for various socioeconomic and clinical variables, further implicating other factors that affect Black patients. 18 This finding calls for heightened postoperative vigilance and a greater emphasis on preventative measures in the Black population, such as increased telehealth services and community-level health interventions, which have been shown to improve health measures.15,18,19 Native American patients had nearly double the odds of wound (OR = 1.88) and septic complications (OR = 1.96) compared to White patients. This elevated risk emphasizes the importance of tailored intervention and prevention strategies regarding wound and septic-related concerns in this demographic, 20 as the higher rates of obesity, diabetes, and smoking observed in this population could potentially exacerbate the risk of these complications and lead to worse outcomes. Additionally, access to care could explain why Native Americans experience high rates of infections, as they have one of the highest rates of being uninsured compared to the other racial and ethnic groups at 27.1%.21,22 Conversely, Asian patients were found to have a lower likelihood of respiratory and cardiovascular complications in comparison to their White counterparts. This finding could be attributed to socioeconomic factors like income, education, and zip code differences warranting further exploration.
Significant disparities in unplanned returns to the operating room and unplanned readmissions further highlight the intricate challenges minority populations face. 23 Specifically, Native American and Native Hawaiian patients were more likely to have an unplanned return to the operating room (3.12% and 3.82%), which might be indicative of potential complications arising from the initial surgery or the essential need for supplementary interventions due to suboptimal surgical outcomes. Furthermore, the elevated rates of unplanned readmission among Black and Native American patients (5% and 5.28%) suggest that these groups face barriers to effective post-discharge care, potentially arising from limited access to follow-up services, difficulties in managing postoperative complications or socioeconomic factors impeding recovery prospects. 24
In addition to surgical outcomes and complications, there were discrepancies in the utilization of surgery based on race and ethnicity. In this study, White patients received a disproportionately high number of surgeries (82.09%) in comparison with every other racial and ethnic group based on the United States Census parameters. The races and ethnicities that are most affected by this disparity are those who identify as Hispanic, who received 4.83% of the surgeries while making up 19.5% of the population; Asian patients, who received 2.53% of the surgeries while making up 6.4% of the population; and Black patients who received 9.7% of the surgeries while making up 13.7% of the population. 25 This underrepresentation of certain R&E groups complements other research that has found similar trends.26,27 Additionally, a meta-analysis by Chen et al found that R&E minority patients were less likely to be prescribed opioid analgesics and undergo spine surgery, with this trend of underutilization of surgery further supported by Milani et al..28,29 Given this noticeable discrepancy in healthcare utilization, further investigation and efforts are warranted to ensure that minority groups receive adequate access to healthcare and that there is no bias present in who physicians recommend for surgery.
This study offers valuable insights into racial and ethnic disparities in spine surgery but has limitations. Its retrospective design makes it difficult to establish causality, and the analysis was limited to NSQIP data, which excluded variables like insurance type, income, and residence. The NSQIP also did not account for patients identifying with more than one race, only considering the race each patient identified with most strongly. Lastly, it is important to report that ACS and the hospitals participating in ACS-NSQIP are the primary sources of the data used in this study, but they have not verified nor are responsible for the statistical validity of the data analysis or conclusions we made. Additionally, we were not able to ascertain the root causes due to the limitation of the NSQIP dataset. Moreover, we did not have robust socioeconomic data to thoroughly study the sociological and economic effects on the highlighted disparities. Future research is needed from other countries outside of the United States of America, to determine if these findings are observed globally. Despite its limitations, this study offers critical insights into the persistent disparities that continue to affect outcomes in spine surgery.
Spine Surgeons can take several takeaways from this study. It is important to recognize that certain populations are indeed subject to an increased likelihood to experience perioperative complications following spine surgery. Our study specifically highlights that considerable attention should be given to Native American and Hawaiian patients in addition to Black and Hispanic patients. Spine Surgeons should be mindful of the specific complications that each racial and ethnic group may experience. When possible, surgeons should discuss the aforementioned complications with patients and discuss strategies to improve modifiable risk factors. For instance, in groups that are at an increased likelihood of experiencing cardiovascular complications, aerobic exercise programs and nutritional habits can be discussed to optimize patients for surgery and to prevent postoperative complications. Moreover, surgeons should be aware that certain sociological and economic groups may not have access to resources that are available to middle class income individuals. This mindful approach will improve spine care and help offset the burden of racial and ethnic health disparities.
Conclusion
Collectively, our results reveal significant disparities in operative and postoperative outcomes following spinal surgery, indicating disproportionately higher rates of complications among Black, Hispanic, and Native American patients. These complications include longer operative times, extended hospital stays, and increased wound, respiratory, and cardiovascular complications. After adjusting for various factors in multivariate analysis, these disparities persisted, implying the presence of broader systemic issues at play. Future research should explore the underlying mechanisms driving these disparities and evaluate the effectiveness of targeted interventions. Addressing these challenges will ultimately lead to improved quality of care for all patients and ensure that advancements in spine surgery are distributed equitably among all racial and ethnic groups.
Footnotes
Ethics Approval
The Columbia University Institutional Review Board (IRB# AAAV2593) approved this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by The Columbia University Vagelos College of Physicians & Surgeons Office of Medical Education.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The data used in this study is available from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) upon request and with appropriate permissions.