
Abstract
Study Design
Cross-sectional ecological analysis.
Objectives
This study aims to assess the availability of robotic spine surgery across the United States and identify disparities in access.
Methods
We utilized provider-finding functions from major medical equipment manufacturers to identify robotic spine surgeons and categorized affiliated hospitals. Geospatial analyses combined with socioeconomic indicators, Rural-Urban Continuum Codes, and the Area Deprivation Index (ADI) provided insights into access disparities. Multivariate logistic regression and Student’s t-tests were used to identify county-level variables associated with hotspots and coldspots. Statistical significance was set at the P < .05 level.
Results
Ninety-one robotic spine surgeons were identified. Robotic spine surgeons were predominantly affiliated with nonteaching hospitals (50.55%), followed by minor teaching (38.46%) and major teaching (10.99%) hospitals. Access hotspots are in the Northeast and Southeast, with rural areas showing 22% lower odds of being hotspots (OR = 0.78, P < .001). Factors increasing the odds of being a hotspot include higher disability prevalence (OR = 1.19, P < .001), lack of insurance (OR = 1.18, P < .001), and older median age (OR = 1.17, P < .001). Educational attainment and ADI, despite being significant, had lower predictive values for access.
Conclusions
Disparities in access to robotic spine surgery are associated with socioeconomic, demographic, and geographic factors. The concentration of surgeons in nonteaching hospitals and higher-income areas may reflect market dynamics. Efforts to improve access should consider regional resources, hospital type, and community disadvantage.
Keywords
Introduction
Robotic-assisted surgery has experienced substantial growth across surgical subspecialties, driven by its ability to enhance precision, improve visualization, and reduce postoperative complications. 1 Building on its early clinical applications—such as laparoscopic cholecystectomy and stereotactic neurosurgical biopsy—robotic technology has been increasingly adopted in orthopaedic surgery and is projected to continue expanding. 2 While technology-assisted total knee arthroplasty—a category that includes both robotic and computer-navigated systems—accounted for just 7.2% of cases in 2019, this proportion is expected to rise to 50% by 2032, according to national estimates derived from the MarketScan Database. 3 While orthopaedic applications like joint arthroplasty have led much of this growth, robotic-assisted surgery has more recently been applied to spine surgery, where its advantages are particularly well-suited. Spine procedures—commonly performed by both orthopaedic and neurosurgical spine surgeons—often demand exceptional fixation and careful navigation around delicate structures with limited visualization, making them especially receptive to robotic assistance. Pedicle screw placement has, therefore, been particularly amenable to the advancements in robotic surgery, as leveraging preoperative computed tomography (CT) scans in computer-guided navigation has given spine surgeons a new tool to achieve more reliable placement of pedicle screws while avoiding critical structures, such as the vertebral artery in the cervical spine. 4 Although the initial cost and learning curve remain barriers, these are increasingly outweighed by the clinical precision and consistency robotic platforms provide in complex spinal procedures. Given that pedicle screw placement plays a crucial role in the treatment of spinal pathologies like nerve entrapment, instability, and deformities across the cervical, thoracic, and lumbar spine, the expanding application of robotics in spine surgery holds significant implications for the future of spinal health care.
With the increase in minimally-invasive spinal procedures being performed in the United States (U.S.) over the past decade, patients are being made aware of the increased variety of options that they have when implicated for spine surgery. 5 Although still early in its adoption curve, robotic-assisted spine surgery has seen a gradual rise in utilization. In a study of over 3.7 million elective spine procedures from 2007 to 2015 using the Nationwide Inpatient Sample — a nationally representative database of U.S. hospital admissions — robotic-assisted surgeries increased in complexity and were increasingly performed using posterior approaches, with fusion procedures accounting for an increasing share of robotic-assisted cases, rising from 40.9% in 2007 to 54.2% in 2015. 6 In a retrospective study conducted at a single U.S. institution, Kanaly et al. analyzed 151 consecutive patients who underwent instrumented spinal fusion — 100 with robotic assistance and 51 without. 7 Researchers found that the average size pedicle screw that the surgeon was able to place under computer-guided navigation was significantly larger without compromising patient safety, suggesting increased fixation within bone, decreasing the risk of revision spinal fusion. Another study by Matur et al. compared the pedicle screw accuracy of robotic-assisted vs fluoroscopic-guided surgery over 14 papers, 12 of which were randomized controlled trials. 8 Researchers found that robotic-assisted pedicle screw placement was associated with significantly higher odds of screw accuracy and lower risk of facet joint violations. A systematic review conducted by Fu et al. similarly compared robotic-assisted and fluoroscopic-guided techniques for 6,041 pedicle screw placements, with 2,748 being robotic-assisted and 3,293 being freehand. 9 Researchers noted a similar increase in screw placement accuracy and decreased incidence of proximal facet violations as described by Matur et al., combined with shorter postoperative stay, lower intraoperative blood loss, and less intraoperative radiation exposure. Preliminary economic models have supported this potential, with one study estimating over $600,000 in annual savings for a health system performing 557 robotic-assisted spine cases, largely due to reductions in revision surgeries, postoperative infections, and hospital length of stay. 10 Although research in the field is still warranted and the role of robotics as a standard approach for screw placement is largely up for debate, the current literature suggests that robotic-assisted spine surgery shows promise in increasing postoperative outcomes for patients. As a result, access to these technologies should be evaluated, providing insights into the communities where robotic-assisted spine surgery is most accessible and those communities in which increased access may be necessary.
The use of robotics has drastically changed the frontier of modern surgical approaches, with increased advances of these technologies in fields like orthopaedic joint replacement enabling them to become a mainstay for standard procedures. While previous studies have aimed to assess the potential benefits of robotic-assisted spine surgery, to the best of our knowledge, no studies have analyzed geospatial disparities in robotic spine surgery. This study aims to (1) analyze current access to robotic spine surgery across the continental U.S., (2) identify the types of medical centers that robotic spine surgeons are affiliated with, and (3) highlight the relative disparities between communities lacking and having access to robotic-assisted spine surgery. We hypothesize that robotic spine surgeons are more likely to be found in large, affluent urban areas with greater hospital infrastructure — particularly those affiliated with academic medical centers — and that regions with limited institutional resources or rural designation may face reduced access to these technologies. By identifying where access gaps exist, our findings may guide targeted efforts to expand availability and inform global efforts to address surgical equity as robotic technology continues to proliferate worldwide.
Methods
Study Design
This study was conducted as a cross-sectional ecological analysis of county-level access to robotic spine surgery in the continental U.S. This design was selected because it allows for evaluation of associations between geographic, socioeconomic, and institutional factors and access to care using publicly available, population-aggregated data. The ecological approach is well-suited for identifying large-scale spatial patterns and disparities in healthcare access.
Provider and Practice Identification
Provider-finding functions on Globus Medical (Audubon, PA) and Medtronic (Minneapolis, MN) websites were used to cover the entire range of the U.S. to obtain the full names and practice locations of each listed robotic spine surgeon and their utilized robotic system on January 26, 2024. Globus Medical and Medtronic were selected because they are the 2 leading manufacturers of robotic spine systems in the U.S., and at the time of data collection, they were the only companies offering publicly accessible, searchable provider directories. All hospitals that robotic spine surgeons had a listed affiliation with were placed into 1 of 3 categories based on the hospital response to the American Hospital Association survey: major teaching hospitals (those that are members of the Council of Teaching Hospitals [COTH]), minor teaching hospitals (non-COTH members that had a medical school affiliation reported to the American Medical Association), and nonteaching hospitals (all other institutions). 11
Geospatial Data Sets
The geographical distribution of robotic spine surgeons was mapped using the latitude and longitude of each practice location listed on the provider-function section of the robotic surgery website associated with each surgeon. The minimum travel distance from the centroid of each county Federal Information Processing Standards (FIPS) code to the nearest robotic spine surgeon was then calculated. This geographic information was then integrated with a comprehensive set of socioeconomic indicators at the county level, derived from the 2022 American Community Survey. 12 Additionally, counties were categorized according to the 2023 Rural-Urban Continuum Codes (RUCC) issued by the US Department of Agriculture, which ordinally ranks counties on a scale from 1 (most urbanized) to 9 (least urbanized). 13 Furthermore, the study incorporated the Area Deprivation Index (ADI) from 2021, which assesses counties on a scale from 1 to 100 based on economic disadvantage levels. 14 Metrics on population health at the county level were also included, utilizing the 2022 chronic disease prevalence data from the Center for Medicare and Medicaid Services. 15 Given the public availability of these datasets, which are aggregated at the population level, no institutional review board approval was required for this study.
Geospatial Analyses
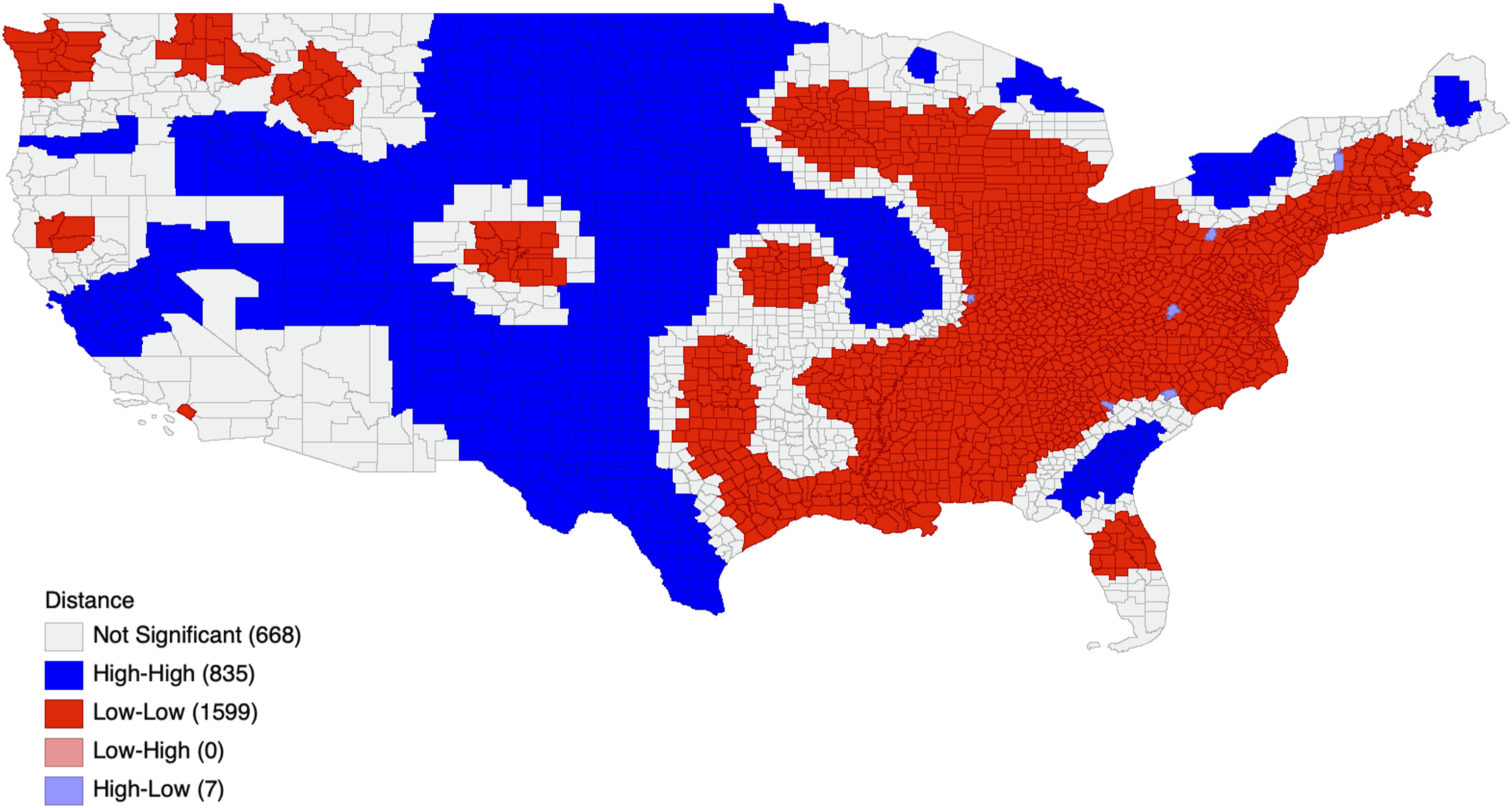
Cluster analysis and visualization of geographic data was conducted using the GeoDa software (Center for Spatial Data Science in Chicago, IL). Statistically significant hotspots, coldspots, and spatial anomalies in terms of travel distances to the nearest robotic spine surgeon were identified through a Moran’s I analysis. Statistical significance was set at the P < .05 threshold. Moran’s I categorizes counties into one of 5 groups: non-significant, or one of 4 significant categories — High-High, Low-Low, Low-High, and High-Low. High-High denotes areas where longer travel distances are prevalent, reflecting coldspots, whereas Low-Low indicates regions with shorter travel distances, or hotspots. Low-High areas are those with shorter travel distances but are surrounded by counties where longer travel distances are common. High-Low regions have longer travel distances but are adjacent to counties characterized by shorter travel distances. All statistical analyses were conducted using R statistical software (version 4.3.1; R Project for Statistical Computing, Vienna, Austria). Descriptive statistics, including means, proportions, and where appropriate, medians, were calculated for county-level variables. Comparisons between hotspot and coldspot counties were performed using Student’s t-tests for continuous variables, as these variables were approximately normally distributed and variances were comparable between groups. Multivariate logistic regression was then used to estimate odds ratios (ORs) for hotspot and coldspot status based on socioeconomic and geographic covariates. In determining the predictive variables for our model, a lasso regression analysis was implemented, a method previously validated for its efficacy in variable selection within large models.16-20 This process led to the identification and subsequent substitution of the top 7 predictive variables, continuing until achieving an Area Under the Curve (AUC) score of at least 0.800.
Results
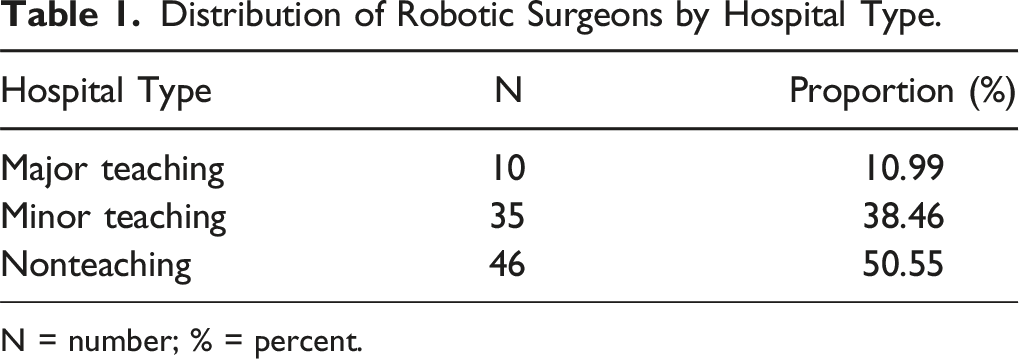
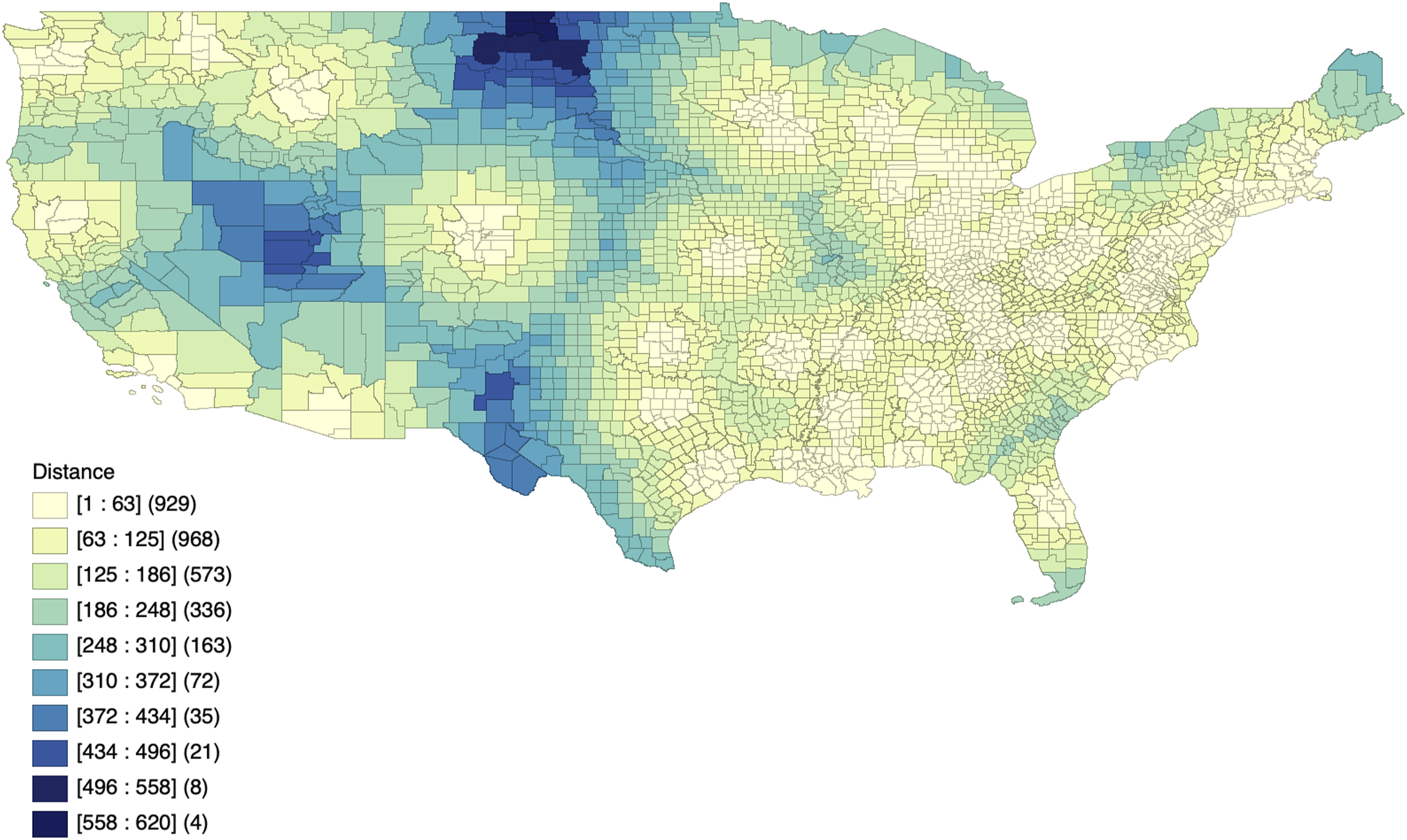
We identified 91 robotic spine surgeons through the provider-finding functions on Globus Medical (Audubon, PA) and Medtronic (Minneapolis, MN) websites (Figure 1). The majority of robotic spine surgeons practiced in nonteaching hospitals (n = 46, 50.55%), followed by minor teaching (n = 35, 38.46%) and major teaching hospitals (n = 10, 10.99%; Table 1). Hotspots of decreased travel distance were identified in the Northeast and Southeast U.S. with a median travel distance of 57 miles (Figures 2 and 3). Coldspots were distributed in nearly all other non-hotspot regions, with a median of 222 miles. Geographic Distribution of Robotic Spine Surgeons Across the Continental United States, with Each Black Dot Representing the Practice Location of an Individual Robotic Spine Surgeon Distribution of Robotic Surgeons by Hospital Type. N = number; % = percent. Choropleth Map of Average Travel Distance (in Miles) From Each U.S. County to the Nearest Robotic Spine Surgeon Moran’s I Spatial Clustering Map of Average Travel Distance (in Miles) from Each U.S. County to the Nearest Robotic Spine Surgeon Across the Continental United States. “High-High” Clusters Represent Coldspots (Greater Travel Distance), While “Low-Low” Clusters Represent Hotspots (Shorter Travel Distance)
Multivariate Hotspot Versus Coldspot Logistic Regression
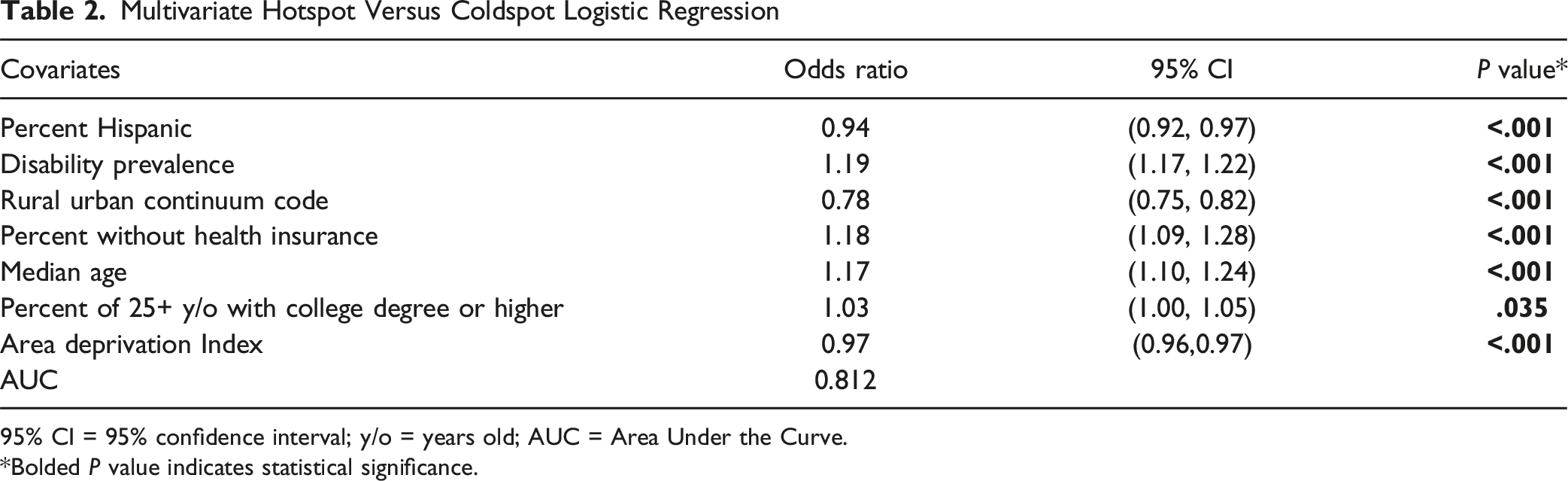
95% CI = 95% confidence interval; y/o = years old; AUC = Area Under the Curve.
*Bolded P value indicates statistical significance.
Univariate Coldspot and Hotspot Analysis Using Moran’s Clustering: Demographics.
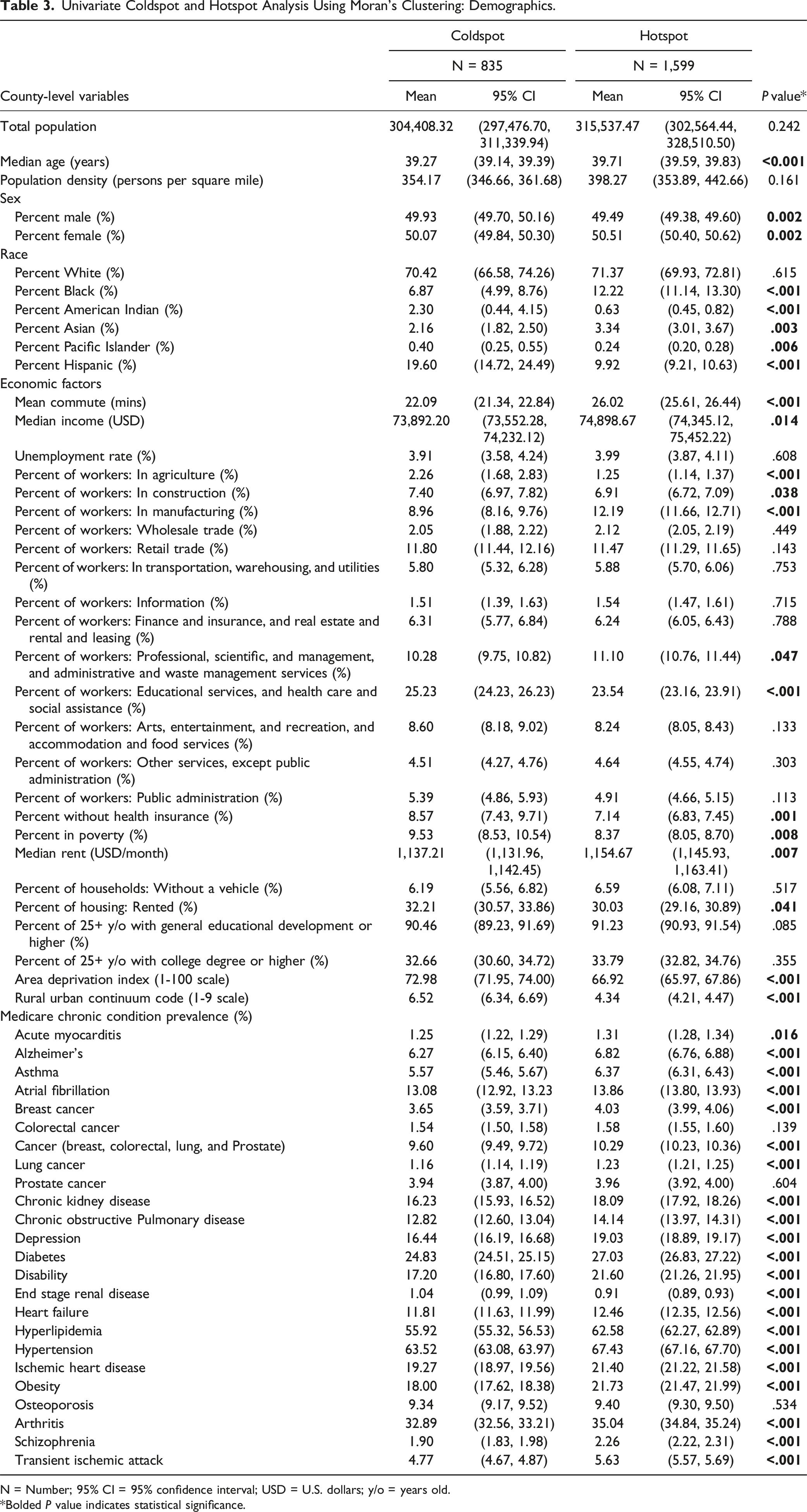
N = Number; 95% CI = 95% confidence interval; USD = U.S. dollars; y/o = years old.
*Bolded P value indicates statistical significance.
Discussion
As robotic spine surgery emerges as a tool to enhance surgical precision and potentially reduce recovery periods, it is important to characterize the current distribution of access to this technology. Upon multivariate logistic regression, factors such as the percentage of the Hispanic population, disability prevalence, RUCC codes, percentage without health insurance, poverty percentage, population density, median age, college education level, and the ADI were identified as the top county-level factors associated with relative access to this technology. Variables such as disability prevalence, metropolitan locations, non-health insurance coverage, median age, and higher education levels were significantly associated with access, illustrating the intricate interplay between socioeconomic determinants and the availability of robotic spine surgery. Conversely, the percentage of the Hispanic population and ADI underscore ethnic and socioeconomic disparities in access. Furthermore, our analysis highlighted substantial variation in travel distances for accessing care, with median distances of 222 miles for patients in the least accessible areas compared to 57 miles for those in areas with better access. These findings underscore the complexity of healthcare accessibility and reflect how socioeconomic, demographic, and geographic factors are associated with variation in the availability of healthcare innovations like robotic-assisted spine surgery. Given the cross-sectional and ecological nature of this study, these associations should not be interpreted as causal. Moreover, as the analysis is based solely on data from the continental U.S., findings may not be generalizable to other countries or healthcare systems.
Our analysis revealed that, among the 91 currently practicing robotic spine surgeons, the majority are in the Northeast and Southeast, with the fewest found in the West. Additionally, patients in areas with limited access, referred to as coldspots, had a median travel distance of 222 miles, in contrast to 57 miles in areas with better access, known as hotspots. This finding aligns with previous research indicating that rural populations may travel up to 250 miles for orthopaedic care, with a reported median travel distance of 45 miles for elective services.21-23 A study by Moore et al. exploring the distribution trends of the spinal surgery workforce, reveals significant regional disparities in the availability of neurologic and orthopaedic spine surgeons. 24 Specifically, the South and Northeast have seen considerable increases in spine surgeon numbers, with growth rates of 11.7% and 17.8%, respectively. 24 In contrast, the Midwest and West regions experienced lower growth rates, at 4.8% and 5.8%, respectively. 24 These variations in spine surgeon growth rates across different regions align with the patterns observed in the distribution and accessibility of robotic spine surgeons in our study. This correlation reflects broader trends observed in both traditional and robotic spinal surgery services, highlighting regional disparities in healthcare access and the evolving landscape of surgical care in the U.S. Efforts to address regional imbalances might include incentivizing robotic technology acquisition in underserved areas through regional grants, public-private partnerships, or bundled payment adjustments that offset the upfront cost of adoption in low-access states.
Our study found that most robotic spine surgeons were affiliated with nonteaching hospitals, which was closely followed by minor teaching hospitals. These trends are consistent with findings in robotic general surgery, whereby Stewart et al. found that small and medium-sized hospitals and non-teaching hospitals performed more robotic general surgery. 25 Previous studies have demonstrated that market forces are the primary drivers in hospital acquisition of surgical robots, and that robot acquisition led to regional increases in genitourinary and gynecologic procedures.26,27 Given that nonteaching hospitals must work harder to attract patients, these market forces may contribute to the observed concentration of robotic spine surgeons at nonteaching hospitals.28,29 In addition to market dynamics, other factors may contribute to this pattern, including local income levels, payer mix, patient preferences for technologically advanced care, and the geographic distribution of surgeons trained in robotic techniques. These variables may influence both the demand for and feasibility of robotic technology adoption in different regions. Collaborative programs between academic centers and community hospitals could help disseminate robotic expertise, while training grants and surgeon certification initiatives may broaden the skilled workforce capable of using this technology.
Our analysis reveals significant disparities in access to robotic-assisted spine surgery, with socio-demographic factors — namely population demographics, economic status, and education levels — closely associated with access to hospitals offering this technology. This aligns with prior research indicating that education, urbanization, and median income are associated with enhanced access to robotic surgery.23,30,31 The implementation costs of robotic surgery systems, such as Medtronic’s Mazor X™, which has a list price of $850,000 and additional per-use disposable costs of $1,500, present a significant financial challenge. 32 This is particularly notable when considering the wide variation in hospital charges for lumbar spine fusion surgery, which can range from $40,000 to $80,000 based on geographic location. 33 The reluctance of orthopaedic and neurosurgical spine departments in economically disadvantaged areas to adopt robotic-assisted technologies can be attributed to several economic factors. The high upfront costs and ongoing expenses may not be justifiable in settings where reimbursement rates for procedures like spine fusions are lower. While preliminary economic models suggest potential savings with robotic-assisted spine surgery, real-world cost-effectiveness remains unclear. Many hospitals may not achieve sufficient case volume or reimbursement margins to offset the high capital and maintenance costs. This is particularly relevant for nonteaching hospitals, which made up the majority of robotic spine surgery sites in our study. In such settings, the decision to adopt robotic platforms may be influenced less by financial return and more by market pressures to remain competitive, attract referrals, or offer technologically advanced care. However, even these market-oriented incentives may not outweigh the underlying financial uncertainty, as the lack of conclusive evidence demonstrating cost-effectiveness further complicates adoption decisions. 34 Without clear data demonstrating that robotic-assisted surgeries lead to significantly better outcomes or cost savings compared to conventional methods, departments face difficulty in validating the investment.
Although robotic-assisted spine surgery has demonstrated equal or superior pedicle screw placement accuracy relative to freehand techniques, there is limited and conflicting evidence regarding its impact on radiation exposure, perioperative complications, and long-term clinical outcomes. 35 Additionally, despite the increasing use of robotic systems, few robust studies have assessed their cost-effectiveness in real-world settings.35,36 These knowledge gaps pose challenges to broader adoption, particularly in resource-constrained environments where the financial risk of investing in costly technology cannot be offset by proven outcome advantages or systemic savings. Until stronger evidence emerges, concerns about return on investment and clinical benefit are likely to temper enthusiasm for widespread implementation. Moreover, in regions with lower socioeconomic status, the potential for reduced reimbursement rates further complicates the financial viability of adopting such expensive technologies, especially if the outcomes and cost-effectiveness do not markedly differ from traditional surgical approaches. This economic uncertainty, coupled with insufficient evidence on improved patient outcomes or cost savings, contributes to the apprehension among spine surgery departments in more disadvantaged areas towards embracing robotic-assisted technologies. To improve access, policymakers and hospital administrators could consider shared-use models of robotic systems across hospital networks, targeted reimbursement incentives, or subsidized acquisition programs in economically disadvantaged regions. These observations are specific to the U.S. healthcare setting and may not apply to countries with different financing models or technology adoption patterns. Further studies are warranted to assess whether similar disparities exist in other countries and to better understand global trends in the adoption of robotic spine surgery and related technologies.
The observed disparities in early access to robotic spine surgery are not merely descriptive findings; they have the potential to influence the future trajectory of technological equity in healthcare. Historically, widespread adoption of medical technologies has been accompanied by reductions in cost, iterative design improvements, and increased accessibility — benefits largely driven by early demand and investment. If access to robotic platforms remains concentrated in affluent or urban regions, these advancements may be unevenly distributed, reinforcing preexisting inequities. Promoting more equitable early access — through public-private partnerships, targeted reimbursement incentives, or shared-use infrastructure — could accelerate diffusion and help ensure that robotic spine surgery evolves into a widely accessible standard of care rather than a technology confined to select populations.
This study stands as the first investigation of the geographic distribution of robotic spine surgery services. However, there are several limitations. The county-level data employed, sourced from the ADI, Center for Medicare and Medicaid Services, and the U.S. Census, correspond to the latest available updates from 2021, 2022, and 2023, respectively. This temporal gap might not fully capture the current landscape. Focusing on the leading 2 manufacturers that dominate the current market, our analysis excludes a variety of other systems, some of which are in the pilot phase or already in use. As a result, surgeons using less common or regionally specific robotic platforms may not be captured, which could lead to underestimation of access in certain areas. Nevertheless, Globus Medical and Medtronic represent the majority market share in the U.S., making this a practical proxy for nationwide trends. Given the innovative nature of robotic spine surgery technology and its selective adoption, our sample size is naturally small. This reflects the technology’s early stage of development and limited user base. As the domain of robotic spine surgery is rapidly advancing with the advent of novel technologies, anticipated shifts in service distribution are impending. Data extraction involved manual retrieval from the publicly accessible domains of these manufacturers. The accuracy and recency of the data on each manufacturer’s website are uncertain, which could have led to the inclusion of surgeons who are trained in robotic spine surgery but do not regularly employ these techniques in their practice. This study, therefore, offers a preliminary exploration into the spatial dynamics of robotic spine surgery. Future studies should investigate how the distribution of robotic spine surgery workforce and infrastructure evolves over time to better understand adoption trends and regional growth patterns.
Conclusion
This geospatial analysis of robotic spine surgery in the continental U.S. identified substantial disparities in access to this technology, with hotspot regions concentrated in the Northeast and Southeast and coldspots prevalent across rural and socioeconomically disadvantaged areas. Multivariate modeling revealed that factors such as disability prevalence, lack of health insurance, and higher median age were significantly associated with access, while rurality and socioeconomic deprivation were linked to reduced availability. The predominance of robotic spine surgeons in nonteaching hospitals highlights potential market-driven dynamics influencing adoption. These findings suggest that geographic, institutional, and socioeconomic barriers play a critical role in shaping access to robotic spine surgery. Future research should explore longitudinal changes in service distribution, investigate patient-level outcomes associated with differential access, and assess policy mechanisms — such as shared infrastructure models or regional investment programs — that could promote equitable adoption of this technology across underserved areas.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mitchell K. Ng has the following disclosures: Johnson & Johnson Ethicon Inc. (paid consultant), CurvaFix Inc. (paid consultant), Pacira BioSciences Inc. (paid consultant), Sage Products Inc. (paid consultant), Alafair Biosciences Inc. (paid consultant), Next Science LLC (paid consultant), Bonutti Technologies Inc. (paid consultant), Hippocrates Opportunities Fund LLC (paid consultant), and Ferghana Partners Inc. (paid consultant). Christopher K. Kepler has the following disclosures: Clinical Spine Surgery (editorial or governing board), Curetiva (IP royalties), and Regeneration Technologies, Inc. (IP royalties). Alan S. Hilibrand has the following disclosures: CTL Amedica (IP royalties), North American Spine Society (board or committee member), Paradigm Spine (stock or stock options), and ZimVie (IP royalties). Alexander R. Vaccaro has the following disclosures: Accellus (other financial or material support; stock or stock options), Advanced Spinal Intellectual Properties (stock or stock options), AO Spine (other financial or material support), Atlas Spine (stock or stock options), Avaz Surgical (stock or stock options), AVKN Patient Driven Care (stock or stock options), Cytonics (stock or stock options), Deep Health (stock or stock options), Dimension Orthotics LLC (stock or stock options), Electrocore (stock or stock options), Elsevier (publishing royalties, financial or material support), Flagship Surgical (stock or stock options), FlowPharma (stock or stock options), Globus Medical (stock or stock options), Harvard Medtech (stock or stock options), Innovative Surgical Design (stock or stock options), Jaypee (publishing royalties, financial or material support), Jushi (Haywood) (stock or stock options), National Spine Health Foundation (board or committee member), Nuvasive (stock or stock options), Orthobullets (stock or stock options), Parvizi Surgical Innovation (stock or stock options), Progressive Spinal Technologies (stock or stock options), Rothman Institute and Related Properties (stock or stock options), Sentryx (other financial or material support; stock or stock options), Stout Medical (stock or stock options), Taylor Francis/Hodder and Stoughton (publishing royalties, financial or material support), Thieme (publishing royalties, financial or material support), and ViewFi Health (stock or stock options).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.