
Abstract
Study Design:
Retrospective study.
Objectives:
Our goal was to evaluate the rate of rod fracture and persistent pseudarthrosis in cohorts of patients treated with a dual rod or multiple-rod construct in revision surgery for pseudarthrosis.
Methods:
A dual rod construct was used in 23 patients, and a multiple rod construct in 24 patients, spanning the pseudarthrosis level. Two-year fusion grading, and rates of pseudarthrosis and implant failure, were assessed.
Results:
There were no differences in patient or surgical characteristics between the groups: (2- rod construct: Age 60 ± 14, Levels 10 ± 5, 3-column osteotomy:17%; multiple-rod construct: Age: 62 ± 11, Levels 9 ± 4, 3-column osteotomy:30%). Patients in the multiple rod construct were transfused a greater volume of packed red blood cells (pRBCs) intraoperatively (2.6 ± 2.9 vs. 1.1 ± 1.5 U, p < 0.0001). At 2 year follow up there was no difference in fusion grades at the previous level of pseudarthrosis, the rate of rod fracture or pseudarthrosis between the 2 groups, or rate of reoperation for pseudarthrosis, rod fracture, wound infection, hardware prominence, or PJK/PJF.
Conclusions:
Our data demonstrate no difference in fusion grade, or rates of rod fracture and revision at 2 years, after utilizing a dual rod versus multiple rod construct in revision surgery for pseudarthrosis. The low complication rates seen with either configuration warrant further investigation of the optimal instrumentation configuration.
Introduction
Despite advances and improvements in spinal instrumentation and techniques, fixation failure and pseudarthrosis continue to pose a challenge to experienced spinal deformity surgeons 1 and failed spinal surgeries remains a serious problem. Up to 23.6% of revision fusion surgeries are performed for pseudarthrosis. 2 Pseudarthrosis rates at the lumbosacral junction are reportedly 10% 3 for an L5-S1 fusion, up to 20% for 2-level fusions, 2 and up to 42% for a long construct for adult spinal deformity that extends to the sacrum. 4 At minimum patients present with persistent back pain, and more commonly radiographic evidence of fractured rods, and perhaps loss of alignment. 2 Studies demonstrate that self-reported clinical outcomes begin to decline at 1 year in adult spinal deformity (ASD) patients who develop a pseudarthrosis.5-7
A hallmark of the strategy in ASD surgery is to ensure a stable foundation for the long fusion construct, and promote a solid union at the lumbosacral junction to mitigate the long lever arm forces exerted by a construct extending to the thoracic spine. 8 In the revision setting for pseudarthrosis, various techniques are utilized to address the pseudarthrosis level including performing an interbody fusion, up-sizing pedicle screw instrumentation, and augmentation of posterolateral fusion mass.1,9,10 Instrumentation provides structural support until fusion is achieved, and is subject to fatigue under load cycling over time. Designing against the fatigue process may involve the strategy of using multiple rods spanning the level of pseudarthrosis, to theoretically provide a stiffer and more stable construct by which to achieve fusion at the nonunion level. Biomechanical studies have supported the concept that multiple rod constructs have a higher load to failure as well as decreased rod and surface strain, than do 2-rod constructs. 11 It has been shown that multiple rods crossing a 3 column osteotomy(3CO) site may help mitigate rod failure and improve fusion rates at the osteotomy site, compared with a 2-rod construct.12,13 However, the use of a multiple rod construct, particularly the use of multiple cobalt chrome rods, may increase the rate of proximal junctional kyphosis and iliac screw loosening at follow up.12,14
To date, there are no studies demonstrating significant improvement in long term fusion rates or clinical outcomes with a multiple rod construct versus a 2-rod construct in revision ASD surgery for pseudarthrosis. There is no clear consensus on the ideal revision construct for pseudarthrosis after index ASD surgery. 15 To that end, we sought to compare fusion grades at the previous level of pseudarthrosis, the rate of rod fracture or pseudarthrosis, as well as the rate of reoperation for pseudarthrosis, rod fracture, wound infection, hardware prominence, or PJK/PJF between patients who underwent revision surgery for pseudarthrosis with a 2-rod versus multiple rod construct. This study is the first to compare fusion rates and rate of rod fracture or reoperation between using a traditional 2-rod technique and a multiple-rod technique in revision ASD surgery for pseudarthrosis.
Materials and Methods
Study Design and Data Source
We retrospectively reviewed our institution’s prospectively collected database to identify patients who were aged 18 years or older when they underwent revision posterior spinal fusion (PSF) for ASD with a minimum of 5 levels fused, from January 2012 through December 2017. All of the data, including demographic, comorbidity, preoperative, intraoperative, and postoperative data from patients undergoing a variety of surgical procedures was recorded. This study was conducted under the supervision of our institutional review board.
All patients had at least 1 level of lower thoracic, thoracolumbar, or lumbar pseudarthrosis, diagnosed preoperatively by the operating surgeon by clinical exam consistent with recurrent axial or radicular pain in the postoperative period. All patients had subsequent imaging confirming pseudarthrosis including full-length standing radiographs, and thin-cut CT. The diagnosis of pseudarthrosis was confirmed by the presence of 1 of the following on advanced imaging: lack of consolidation or bridging trabecular bone through an interbody graft, radiolucent lines within the fusion mass, radiolucency or halo around the implant, progressive settling of an interbody graft, or absence of bridging bone in the posterior elements All operative reports for patients included in this study indicated gross motion at the pseudarthrosis level when tested intraoperatively. The last author on this study retrospectively confirmed the diagnosis of pseudarthrosis through retrospective review of imaging and operative reports. Treating the pseudarthrosis was the indication for surgery in all patients reviewed in this study, in addition to associated pathology including loss of alignment or instrumentation failure.
Patients who underwent a dual rod construct had a single rod placed on either side of the spinal column, with bilateral S1 and iliac screws. All rods were of 5.5 mm in diameter, and of cobalt chrome material. Local autograft, allograft, and rh-BMP2 were used. See Figure 1 for example of a patient who received a dual rod construct in revision surgery for pseudarthrosis.
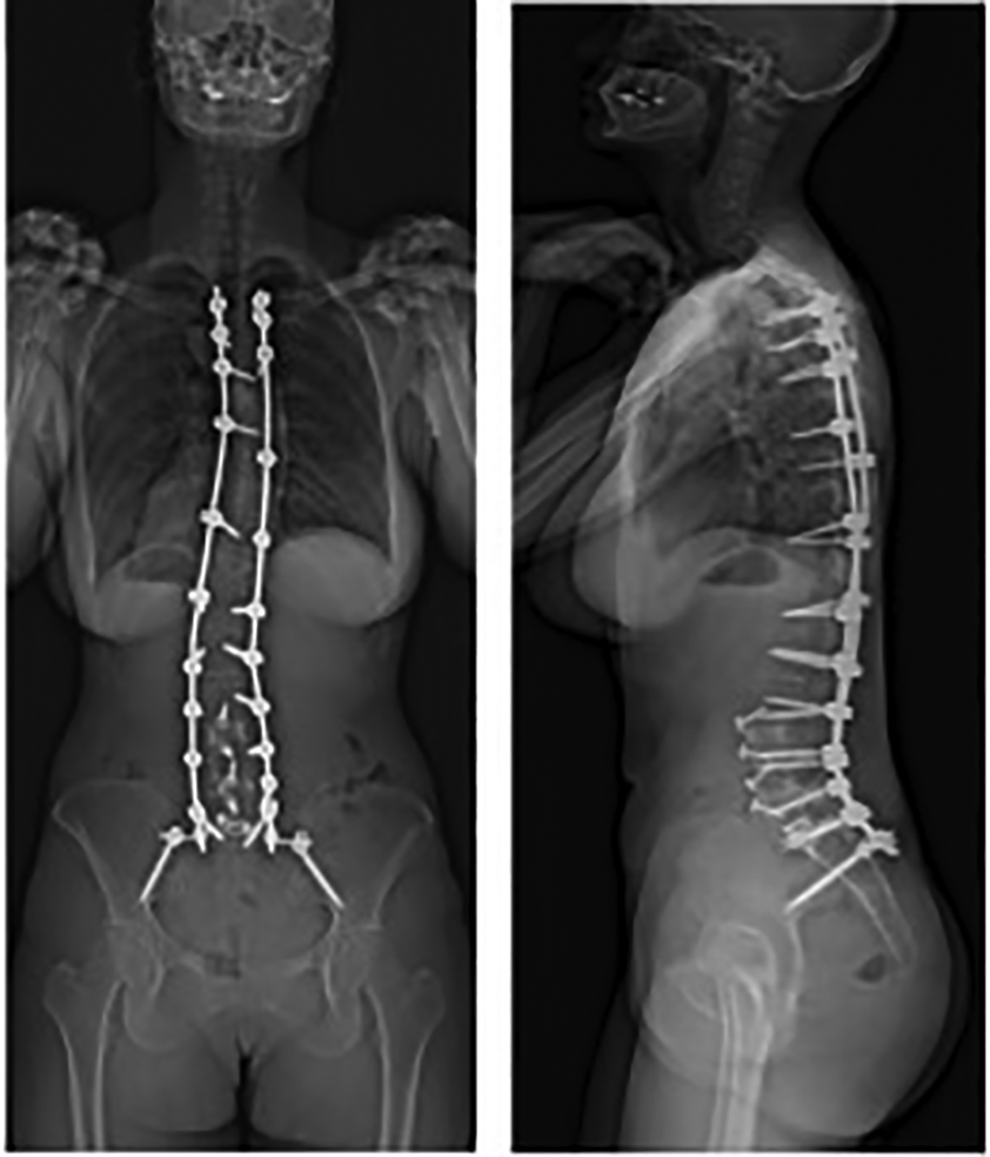
AP and lateral radiographs of a dual-rod construct.
Patients who underwent a multiple rod construct all had a single rod placed on either side of the spinal column, with bilateral S1 and iliac screws. They additionally had at least 1 satellite or kickstand rod placed on either side of the spinal column. In all cases, the additional rods spanned the levels of pseudarthrosis being addressed. All rods were of 5.5 mm in diameter, and of cobalt chrome material. Local autograft, allograft, and rh-BMP2 were used. See Figure 2A for an example of a patient who received a multiple rod configuration with satellite rods, and 2B for an example of a patient who received a multiple rod configuration with multiple satellite rods.
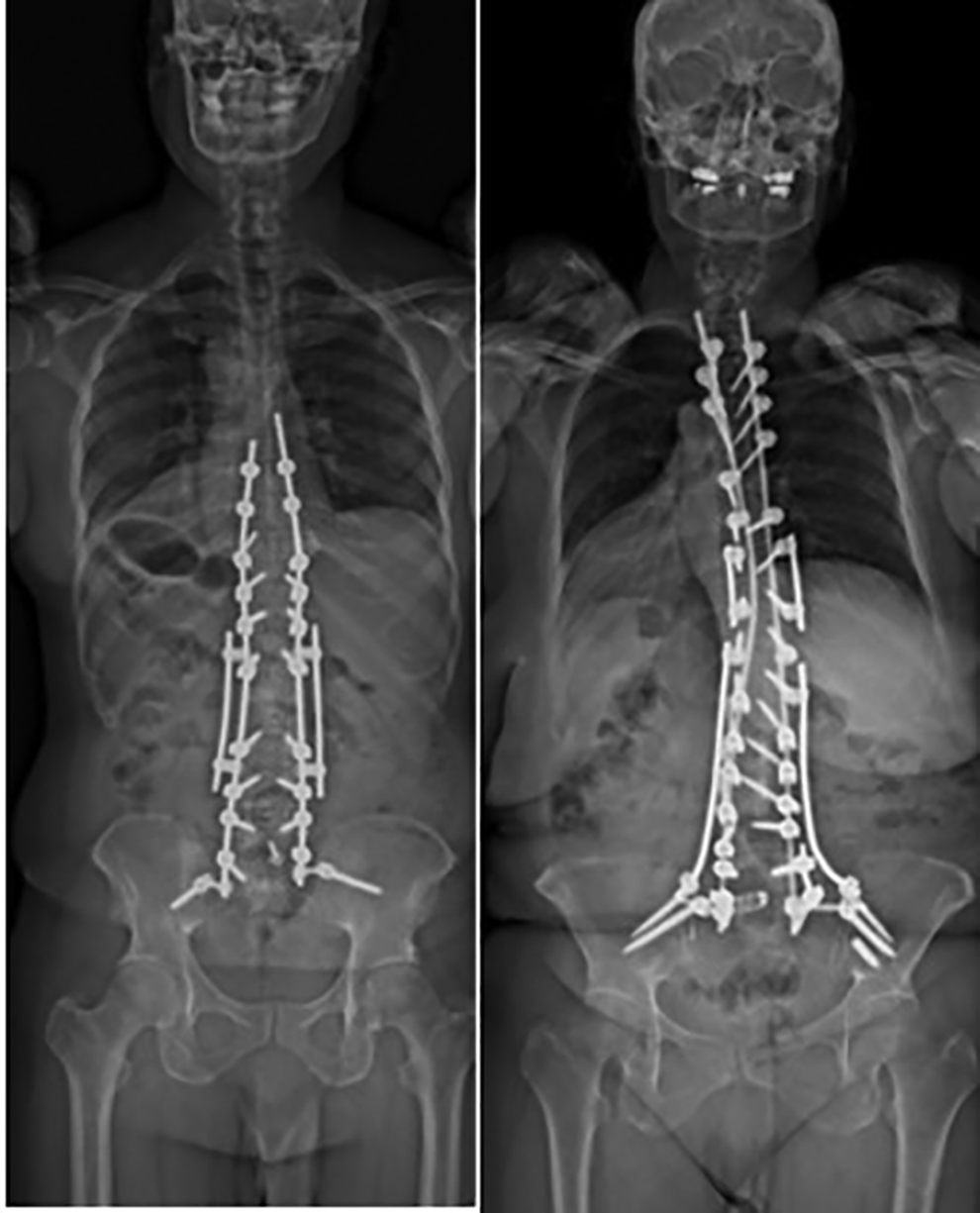
AP and lateral radiographs of a multiple-rod construct; (A) satellite rod construct, (B) multiple satellite rod construct.
Patient and Surgical Characteristics
The primary indication for the revision surgery was pseudarthrosis at a previously instrumented level, with pain and disability for which prolonged nonoperative treatment had failed. We used the clinical database and patient’s medical records to ascertain patient characteristics including age, sex, and ASA (American Society of Anesthesiologists) score. Based on a validated 5-item frailty index, a modified frailty index (mFI) was calculated for each patient, with 5 categories of frailty ranging from 1 (lowest) to 5 (highest). 16
Surgical parameters collected included number of levels fused, the use of pelvic fixation, interbody fusion, and multi-rod construct. Each case was assigned a Mirza invasiveness index, 17 based on published criteria, for the purposes of assessing surgical complexity between the 2 groups.
Primary Outcomes
The primary outcomes assessed were 2-year fusion grades at the level previously treated for pseudarthrosis, the 2-year rate of rod fracture or pseudarthrosis in the 2 groups, and 2 year rate of reoperation for pseudarthrosis, rod fracture, wound infection, hardware prominence, or PJK/PJF.
Statistical Analysis
The 2 groups were compared with the t test statistic or Mann-Whitney nonparametric statistic for continuous parameters. Chi-square tests were used for categorical data when all the expected counts had 5 or more observations, and Fisher’s exact tests were used for categorical data when any of the expected counts had fewer than 5 observations.
Descriptive statistics were calculated with SPSS version 25 software (IBM, Armonk, NY), R statistical software, and Microsoft Office Excel software (Microsoft Corp., Redmond, Washington).
Results
Patient Population
Included in the study were 47 patients with complete surgical and inpatient admission data, who underwent revision ASD surgery for pseudarthrosis. Twenty-four patients underwent revision surgery with a dual rod construct and 23 patients underwent revision surgery with a multiple rod construct.
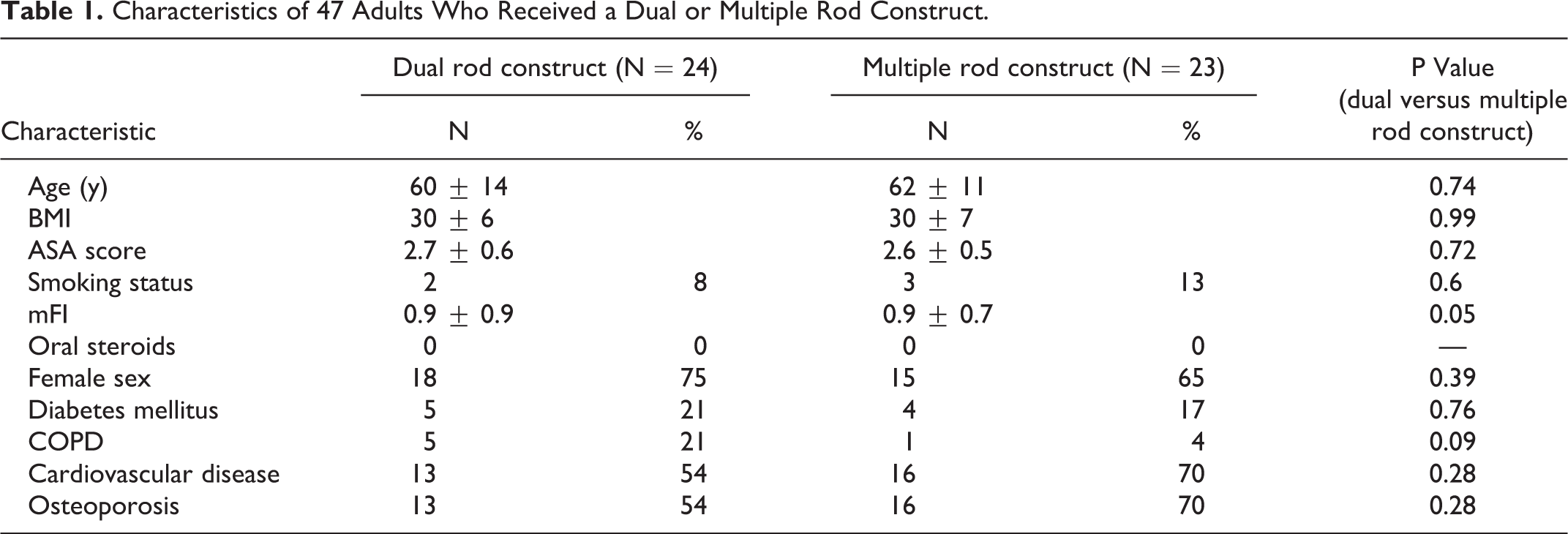
There were no significant differences found between the 2-rod and multiple rod construct group, with regard to preoperative characteristics. There was no difference with respect to age, BMI, or frailty score: (2-rod construct: Age 60 ± 14, BMI 30 ± 6, mFI 0.96 ± 0.96; multiple-rod construct: Age: 62 ± 11, BMI 30 ± 7, mFI 0.91 ± 0.67). There were no differences seen in rate of comorbidities between the groups including diabetes mellitus, COPD, CHF, hypertension, and thromboembolic complications. Full demographic data for the study population is presented in Table 1.
Characteristics of 47 Adults Who Received a Dual or Multiple Rod Construct.
Surgical Characteristics
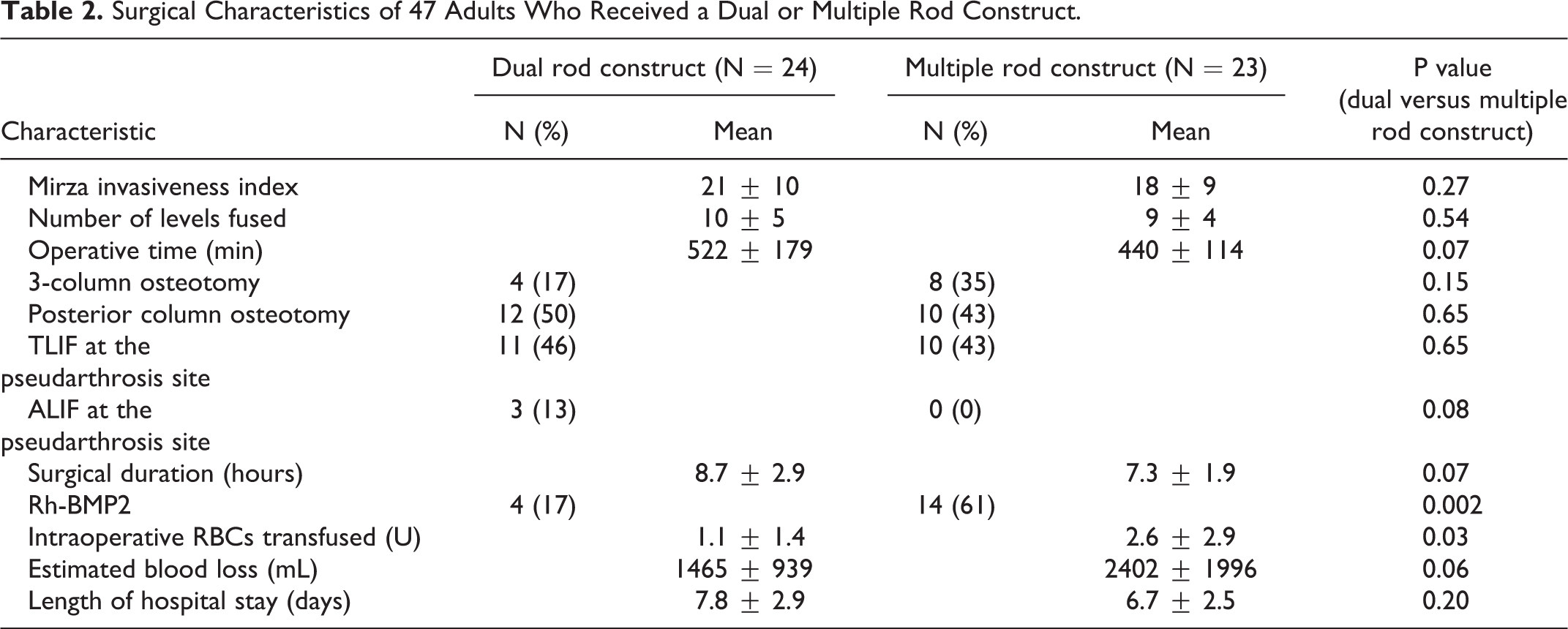
In terms of surgical characteristics, there was no significant difference in number of levels fused or percent of 3 column osteotomy procedures done in each group (2-rod construct: Levels 10 ± 5, 3CO:17%; multiple-rod construct: Levels 9 ± 4, 3CO:30%). Rh-BMP2 was used more commonly in the multiple rod construct group (64% vs. 17%, p = 0.002), with no difference in rate of interbody fusion performed at the nonunion level during revision surgery (64%: multiple rod construct vs. 58%: 2-rod construct). There was no difference in Mirza invasiveness index between the 2 groups. Patients in the multiple rod construct were transfused a greater volume of packed red blood cells (pRBCs) intraoperatively (2.6 ± 2.9 vs. 1.1 ± 1.5 U, p < 0.0001). There was no difference in operative time between the 2 groups. See Table 2 for complete surgical characteristics of the 2 groups.
Surgical Characteristics of 47 Adults Who Received a Dual or Multiple Rod Construct.
Two-Year Outcomes in Fusion and Need for Revision Surgery.
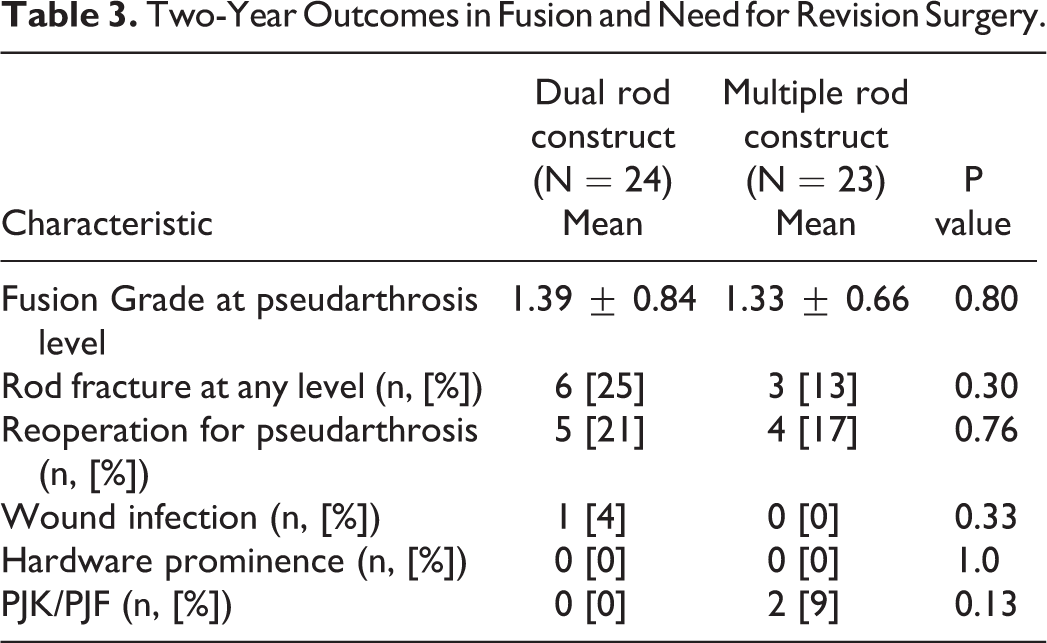
Two-Year Fusion and Reoperation Rates
There was no difference in fusion grade at the previous level of pseudarthrosis between the 2 groups at 2-year follow up. The mean fusion grade in the 2-rod group at the previous pseudarthrosis level was 1.4 at 2-year follow up; 19 patients had a grade 1 fusion, 2 patients had a grade 2 fusion, 2 patients had a grade 3 fusion, and 1 patient had a grade 4 fusion. The mean fusion grade in the multiple-rod group at the previous pseudarthrosis level was 1.3 at 2-year follow up; 18 patients had a grade 1 fusion, 3 patients had a grade 2 fusion, and 2 patients had a grade 3 fusion.
At 2 years, 5 of 24 (20.8%) patients in the 2-rod construct group required revision surgery for persistent pseudarthrosis, and 4 of 23 patients (17.8%) in the multiple-rod construct group required revision surgery for persistent pseudarthrosis. This was not significantly different. Persistent pseudarthrosis was defined as pseudarthrosis at the same level as the initial pseudoarthrosis and the same diagnostic criteria for the initial pseudarthrosis was applied. The rate of rod fracture was not significantly different between the 2 groups. 6 of 24 patients in the 2-rod construct group sustained a rod fracture (25%), versus 3 of 23 patients in the multiple-rod construct group (13%).
The rate of PJK was not statistically different between the 2 groups, though higher in the multiple-rod construct group – 0% in the 2-rod group, and 8.7% in the multiple-rod construct group. There was no difference in wound infection, or symptomatic hardware prominence between the 2 groups at 2 years.
Complication Rates
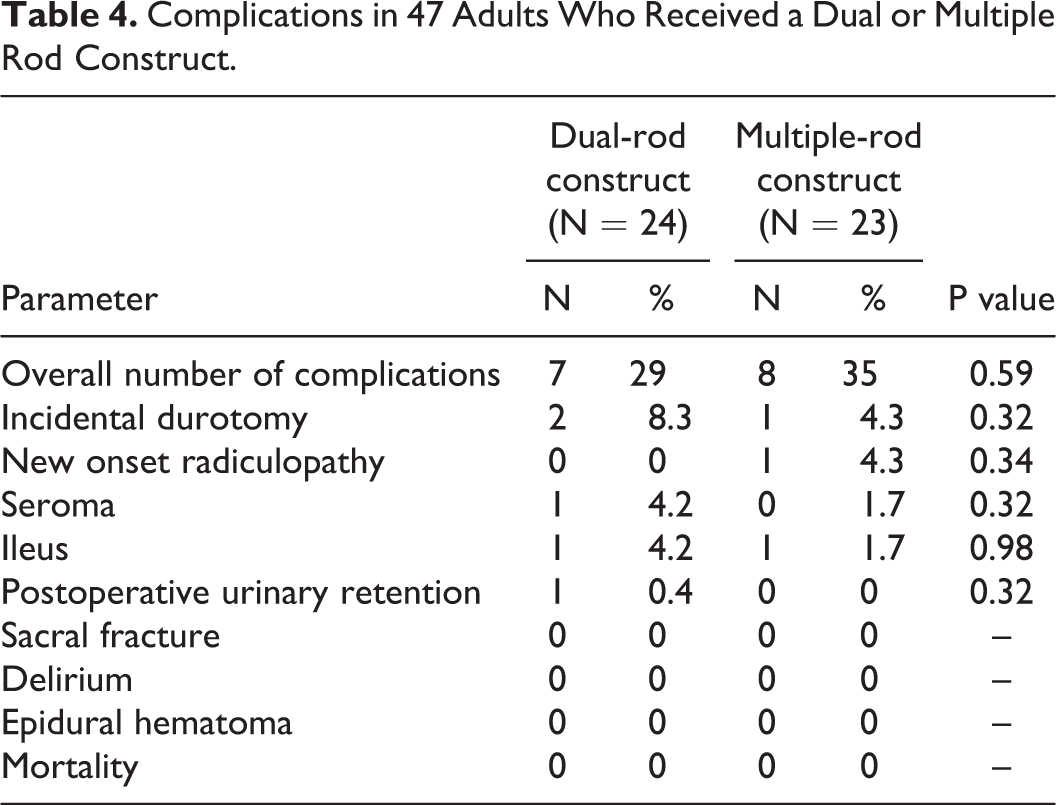
In terms of major and minor complications, there were 2 intraoperative incidental durotomies in the 2-rod construct group (8.3%), that were primarily repaired. One patient in the 2-rod construct group developed a seroma that resolved with a single sterile aspiration (4.2%). In the multiple-rod construct group there was 1 intraoperative incidental durotomy (4.3%), that was primarily repaired. One patient (4.3%) in the multiple-rod construct had to return to the operating room within 90 days of the index procedure for revision of a malpositioned screw. Two additional patients (8.7%) developed postoperative exacerbation of preoperative radiculopathy, that resolved with time and physical therapy, and did not require operative intervention.
See Table 4 for a complete list of complications in the 2 groups.
Complications in 47 Adults Who Received a Dual or Multiple Rod Construct.
Discussion
Pseudarthrosis after ASD surgery almost invariably requires operative intervention, to address a patient’s pain and worsening function, as well as to address concomitant loss of alignment or implant failure.18,19 The revision strategy for pseudarthrosis after ASD surgery can be widely variable, depending on the pathology. Strategies to address pseudarthrosis in the lower lumbar region and at the lumbosacral junction include anterior column support with interbody fixation from an anterior or lateral approach, addition of pelvic fixation such as iliac or S2AI screws to offload stress on S1 screws, and the use of BMP-2 or autogenous iliac crest bone graft to augment posterolateral fusion.15,19,20 Experienced deformity surgeons often utilize multiple rod constructs in revision ASD surgery to provide more stable fixation across a pseudarthrosis level, as an adjunct to the use of interbody devices and biologics to attempt to achieve a solid fusion.14,21,22
In the present study we found no difference in fusion grades at the previous level of pseudarthrosis, the rate of rod fracture or pseudarthrosis between the 2 groups, or rate of reoperation for pseudarthrosis, rod fracture, wound infection, hardware prominence, or PJK/PJF over a 2 year follow-up period, between patients who underwent revision surgery with a 2-rod construct versus a multiple-rod construct. There were no significant differences in baseline patient or surgical characteristics between the 2 groups.
To date, there are no studies demonstrating that the use of multiple rods improves the clinical outcome and rate of fusion at the previous pseudarthrosis levels. A few studies have demonstrated that in the setting of performing a 3 column osteotomy, multiple rod constructs may decrease the rate of osteotomy site failure, defined as osteotomy pseudarthrosis or rod fracture at the osteotomy site.11,21 Reports of dual rod constructs for complex spine reconstruction similarly demonstrate a low rate of rod fractures requiring revision surgery, and no screw fractures.12,23 Importantly, it is possible that increased stiffness of multiple-rod constructs may increase the incidence of PJK, as a greater differential is created between stiffness of the multiple rod construct and the proximal native bone. This differential is likely enhanced in patients with moderate to severe osteoporosis. Our study demonstrated a 0% PJK rate in the 2-rod construct group, and 8.7% in the multiple-rod construct group. While this difference was not statistically significant, future study in larger populations will lend more insight into any differences in rate of PJK of PJF between 2-rod and multiple rod constructs in ASD surgery. However, it is important to note that in the present study all rods used in the multiple-rod construct group, both main and satellite/kickstand, were of cobalt chrome. Multiple studies have demonstrated that the use of cobalt chrome rods may increase the rate of PJK/PJF, compared with the use of titanium rods.24,25 To that end, in some cases, use of a titanium rod as the satellite rod, in conjunction with cobalt chrome main rods, can decrease stiffness of the overall construct. The role that rod material plays within the multiple-rod strategy, with regards to PJK/PJF rates, requires further investigation and long term follow up.
Nine patients in both groups had persistent pseudarthroses after revision surgery. While the small number precluded any significant statistical analysis, in trying to better characterize this group, we noted that 7 of the 9 patients had pseudarthroses in the lower lumbar region, while 2 patients had lower thoracic pseudarthroses between T10 and T12. Of the 7 patients who had a persistent lower lumbar pseudarthrosis, one had undergone an anterior lumbar interbody fusion with femoral allograft performed through a retroperitoneal approach at the pseudarthrosis level. Two of the 7 patients had undergone a transforaminal interbody fusion with titanium cage performed at the pseudarthrosis level, either de novo or by inserting the second cage adjacent to a previous cage. The remaining 5 patients were treated with posterior augmentation of the fusion mass at the pseudarthrosis level. Overall, no specific parameters could be found that clearly characterized the group of 9 patients with persistent pseudarthrosis. However, as anterior column support and interbody fusion can be powerful adjuncts to achieving a solid union, it’s possible the lower rate of interbody fusion performed at the pseudarthrosis level in this group predisposed to persistent pseudarthrosis.
Prior reports have demonstrated that risk factors for recurrent pseudarthrosis include multiple levels of pseudarthrosis, longer fusions, increasing thoracolumbar kyphosis, and sagittal malalignment.26-29 It has yet to be demonstrated that the use of multiple rods and increasing implant stiffness is protective against development of recurrent pseudarthrosis. Our data demonstrate no difference in fusion grade, or rates of rod fracture, pseudarthrosis, or revision at 2 years after utilization of a 2-rod versus multiple rod construct in revision ASD surgery for pseudarthrosis. Volume of pRBCs transfused was higher in the multiple rod construct group. The low complication rates seen with either configuration warrants further investigation with a multi-center study to further define the optimal instrumentation configuration.
Conclusion
We found no difference in fusion grade, or rates of rod fracture, pseudarthrosis, or revision at 2 years, after utilizing a 2-rod versus multiple rod construct in revision ASD surgery for pseudarthrosis. Patients who received multiple rod constructs were transfused a greater volume of pRBCs intraoperatively. Larger studies may be warranted to evaluate the effectiveness of a multiple rod strategy in revision ASD surgery for pseudarthrosis.
Footnotes
Authors’ Note
This study was approved by the NYU Langone Health Institutional Review Board, IRB number i17-01327. As this is a retrospective study of de-identified data, it was exempt from informed consent.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Passias reports other from Allosource, personal fees from Globus Medical, personal fees from Medicrea, personal fees from Royal Biologics, personal fees from SpineWave, personal fees from Terumo, personal fees from Zimmer, other from Cervical Scoliosis Research Society (cSRS), outside the submitted work;. Dr. Errico reports personal fees from Stryker, personal fees from K2 M, outside the submitted work; Dr. Kebaish reports other from Depuy Synthes, other from Depuy Synthes, other from Stryker, other from Spinecraft, other from Orthofix, outside the submitted work; .
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.