
Abstract
Study design
Retrospective Cohort Study.
Objectives
Rod fracture (RF) is a frequent mechanical complication in adult spinal deformity (ASD) surgery, often requiring revision and impairing quality of life. Despite improved alignment strategies and surgical techniques, RF risk remains. This study aimed to identify predictors of RF and evaluate the protective effect of multi-rod constructs.
Methods
We retrospectively reviewed 140 ASD patients who underwent posterior spinal fusion between 2015 and 2023. Demographic, radiographic, and operative data were collected. Logistic regression was used to identify predictors of RF and their impact on outcomes.
Results
Univariate analysis showed that higher pelvic incidence (PI) (56.5° vs 60.5°, P = .037) and pelvic tilt (PT) (25.8° vs 28.7°, P = .042) were significantly associated with RF. Inadequate correction of PI–lumbar lordosis mismatch (P = .041) also predicted RF. Anterior column manipulation with anterior lumbar interbody fusion (ALIF, P = .004) or anterior column realignment (ACR, P = .045) increased RF risk, whereas multi-rod constructs reduced it (P = .012). On multivariate analysis, ALIF/ACR remained the only independent predictor (OR 4.69, 95% CI 1.66-13.25, P = .004). Clinically, RF correlated with prolonged opioid use (P = .016) and higher Oswestry Disability Index scores (P = .003), reflecting functional impairment, though not directly with pain scores.
Conclusion
RF in ASD surgery is influenced by spinopelvic parameters, surgical technique, and construct design. High PI and PT and poor sagittal correction elevate risk, but anterior column manipulation (particularly ALIF/ACR) is the most robust independent predictor. Multi-rod constructs provide significant protection. Clinically, RF is associated with extended opioid use and functional decline.
Keywords
Introduction
Adult spinal deformity (ASD) is a complex condition characterized by sagittal and coronal plane misalignment, often leading to significant pain, functional limitations, and decreased quality of life. 1 With an aging population and growing awareness of sagittal balance, the demand for surgical correction of ASD has increased. The primary goal of surgical intervention is to restore spinal alignment, relieve pain, and improve function through a combination of posterior spinal fusion and osteotomies, sometimes supplemented with interbody fusion techniques. 2 Despite advancements in surgical approaches and instrumentation, mechanical complications remain a significant challenge, with rod fracture (RF) being one of the most common implant failures.3,4
RF occurs due to mechanical fatigue, inadequate sagittal alignment correction, inadequate fusion or stress concentration on the implant. Reported RF rates in ASD surgery vary widely, with studies indicating incidences ranging from 5% to over 30%, depending on patient factors, surgical techniques, and follow-up periods. Poor sagittal alignment can place excessive mechanical stress on spinal instrumentation, leading to an increased risk of RF. Surgical interventions aimed at restoring sagittal balance prioritize proper load, implementing different types of multi-rod constructs and utilizing tailored and durable instrumentation.3-9
The consequences of RF are substantial, often requiring revision surgery and leading to prolonged pain management, increased opioid dependence, and worsened functional outcomes. Patients with RF have been shown to experience higher disability scores and a greater risk of subsequent mechanical complications.10,11 Additionally, RF can impose a prolonged strain on a patient’s personal and professional life, leading to extended work absences, diminished social interactions, and increased financial burdens. The economic implications extend beyond the individual, placing additional strain on healthcare systems and workforce productivity.12-14 Given these implications, identifying the key predictors of RF and optimizing surgical strategies to mitigate its occurrence remain essential for improving patient outcomes and reducing the broader societal and economic impact.
This study aims to explore the factors contributing to RF and its broader implications on patient recovery and long-term spinal stability. By assessing different stabilization techniques, including the use of multi-rod constructs, the study seeks to highlight strategies that may reduce RF risk and improve patient outcomes. A better understanding of these elements will contribute to advancing surgical planning and optimizing treatment approaches for ASD correction.
Methods
Study Design and Patient Population
This retrospective cohort study analyzed adult patients who underwent spinal deformity surgery at a single academic medical center between 2015 and 2023. The primary objective was to identify predictors of RF and assess its impact on postoperative outcomes. Data were extracted from electronic medical records and supplemented by imaging studies. Preoperative and postoperative imaging of the RF and non-RF group, including the post-RF imaging is shown in Figure 1. Pre- and Postoperative X-ray Images. Displayed are Anteroposterior (1) and Lateral (2) Preoperative (A and C) and Postoperative X-ray Images (B and D) of Patients Undergoing Adult Spinal Deformity Correction. Images A and B Show a Patient From the Non-RF Group and C and D, a Patient From the RF Group. Image E Shows the Imaging of the Patient after the RF. The Arrows Show the Point of Fracture in the Rod. RF: Rod Fracture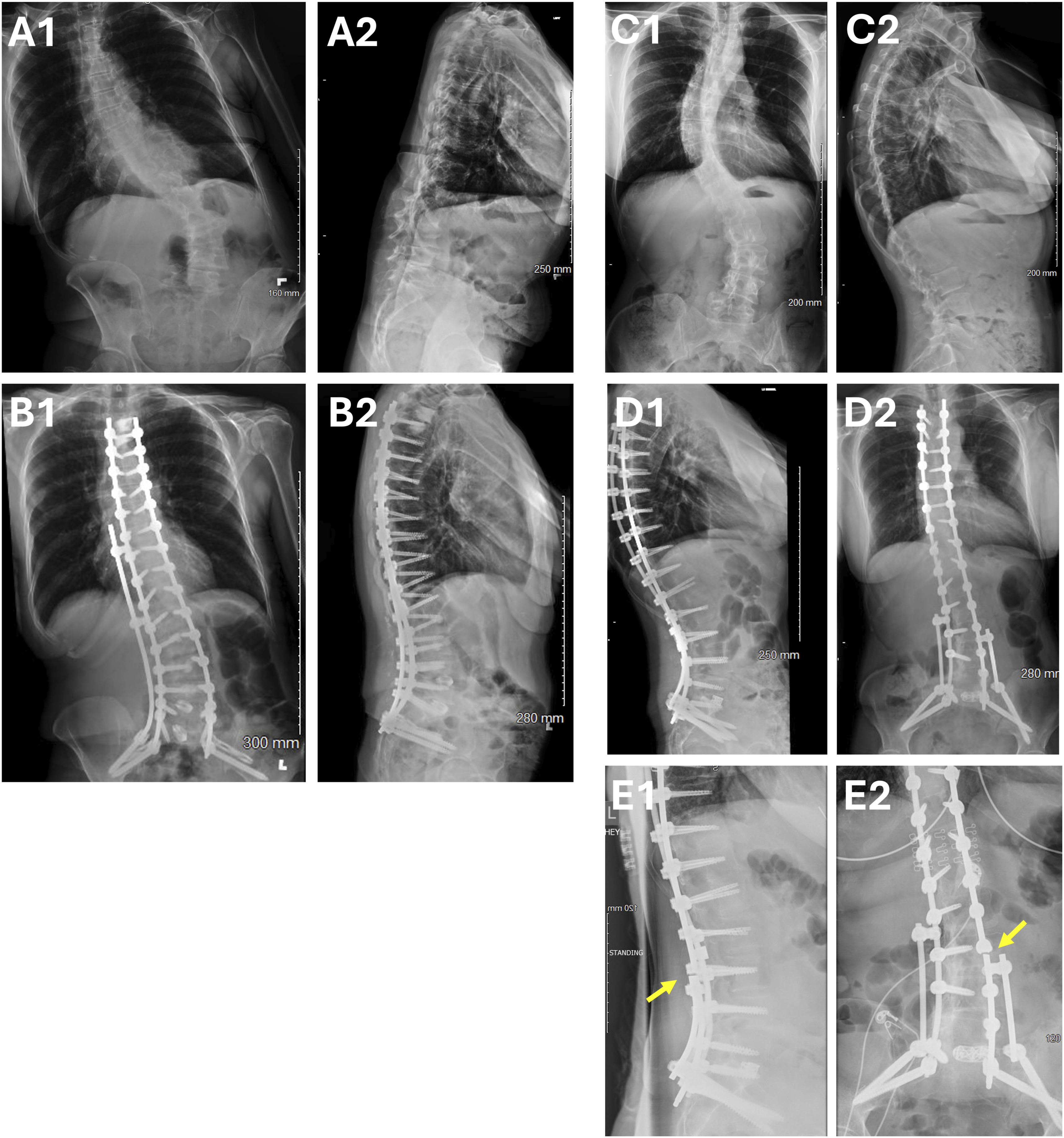
Inclusion and Exclusion Criteria
Patients were included if they had undergone posterior spinal instrumentation and fusion for ASD. Primary binary logistic regression revealed a significant association between the number of instrumented levels and RF risk (odds ratio (OR) = 1.182, 95% CI: 1.055-1.324, P = .004). This suggests that each additional instrumented level increases the odds of RF by approximately 18%. Given these results, to ensure greater cohort uniformity and enhance the reliability of statistical comparison, only long construct fusions were assessed, which encompass fusions bypassing the thoracolumbar fusion. The lowest upper instrumented level in these patients is at T11 to bypass the thoracolumbar junction. Since all our patients had their lowest instrumented level at the pelvis, this led to the inclusion of patients who only had 7 or more fused levels. RF was diagnosed with X-rays. After stratification, the number of instrumented levels no longer significantly influenced RF risk (OR = 1.07, 95% CI: 0.940-1.218, P = .306).
The follow-up ranged between 2 and 9 years, with a median follow-up of 5.2 years.
Overall, 50 (35.7%) of the patients showed RF, of which 6 patients had bilateral fractures at the time of diagnosis. The median time to RF diagnosis was 761 days (IQR: 423-1207).
Data Collection
Demographic and clinical characteristics, including age at surgery, sex, body mass index (BMI), comorbidities, preoperative opioid use, and pain scores (measured using the Visual Analog Scale (VAS)), were collected. Functional disability was assessed preoperatively and postoperatively using the Oswestry Disability Index (ODI).
Sarcopenia was assessed using MRI scans and ImageJ software. We calculated the Psoas L4 vertebral index to assess central sarcopenia. Surgical details, including the number of Cobalt-Chromium rods implanted (multi-rod constructs: >2 satellite rods placed), the number of instrumented spinal levels, and the use of interbody fusion techniques such as transforaminal lumbar interbody fusions (TLIF), anterior lumbar interbody fusions (ALIF) and lateral lumbar interbody fusion (LLIF), were recorded. Additional variables included different types of osteotomies conducted, such as anterior column realignment (ACR) or three-column osteotomies (3COs), such as pedicle subtraction osteotomy (PSO), or intradiscal osteotomy (IDO). The rate of Pseudoarthrosis was also assessed but not included in further analysis due to low CT imaging rates of non-symptomatic patients, to minimize bias.
All cases were performed by board certified or board eligible spine surgeons. Utilization of fusion and osteotomy techniques was based on surgeon’s practice, patient characteristics and disease severity. To minimize bias caused by disease severity in these, a multivariate analysis was performed encompassing available deformity severity parameters.
ALIF were performed via a standard retroperitoneal approach in collaboration with access surgeons, most commonly at L5-S1 and occasionally at L4-L5. Structural support was achieved with lordotic PEEK or titanium cages packed with autograft and demineralized bone matrix. ACR procedures were performed through a lateral approach, involving ALL release and the placement of hyperlordotic cages to restore segmental lordosis. These procedures were selectively utilized in patients requiring significant sagittal correction.
Cases encompassing two rods, had one rod placed on each side. Cases encompassing three rods, had one rod on each side and an accessory rod on one side. Cases encompassing 4 rods, had one main and one accessory rod on each side. If only one accessory rod was utilized, it was placed along lumbosacral junction, extending to the thoracic spine. If two accessory rods were utilized, at least one of them was placed along the lumbosacral junction. Rods were connected side to side by connectors. Interbody cages were placed at one or more high stress levels (L3-L4, L4-L5 and L5-S1). All utilized rods were 5.5 mm cobalt chrome rods.
Surgimap (2.3.2.1) was used to measure radiographic parameters from preoperative and postoperative standing film X-rays, including pelvic incidence (PI), pelvic tilt (PT), lumbar lordosis (LL), and pelvic incidence-lumbar lordosis mismatch (PILL). Changes in these parameters (Δ PT, Δ LL, Δ PILL) were also calculated. This method of measurement was previously described by Rueden et al. 15 Rod fractures were defined as imaging-confirmed breakage of at least one rod, as observed on follow-up radiographs or CT scans. Postoperative outcomes included the need for opioids after discharge (rate), duration of opioid use, postoperative VAS scores, and ODI scores, all of which were analyzed to determine the impact of RF on recovery and functional status.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Institutional review board (IRB) approval was obtained prior to the initiation of the study, under No. Pro00023643. Patient data was anonymized to ensure confidentiality, and no identifiable information was included in the analysis. As this was a retrospective study, the requirement for informed consent was waived by the IRB. All data were collected and stored in compliance with institutional and regulatory guidelines to maintain the privacy and security of patient information.
Statistical Analysis
All statistical analyses and visualizations were conducted using R (version 4.4.1) and IBM SPSS Statistics (version 27.0.1). Descriptive statistics were reported as means ± standard deviation (SD) or medians with interquartile ranges (IQR) for continuous variables, and as frequencies for categorical data.
Binary logistic regression was used to assess the risk of RF in relation to the number of instrumented levels, with results presented as ORs and 95% confidence intervals (CIs). Categorical variables, including sex, fusion techniques, and the use of osteotomies, were compared using chi-square or Fisher’s exact tests, as appropriate.
Spearman’s correlation was applied to explore associations between preoperative predictors such as PI, PT, ODI, opioid use, and sarcopenia. Differences in spinopelvic parameters before and after surgery were analyzed using independent t-tests or Mann–Whitney U tests, depending on data distribution. Multivariate binary regression analysis was performed to evaluate for confounders.
Multiple regression analysis was conducted to evaluate the impact of rod fracture on postoperative ODI scores and the duration of opioid use. A (P < .05) was considered statistically significant.
Results
Anterior Column Disruption is Associated with Higher Rod Fracture Rates
After excluding patients with <7 fused levels, 140 patients were included and our cohort showed there to be no difference between the number of levels fused (9.84 vs 10.32, P = .343). This allowed us to exclude the number of levels as a possible confounder in our cohort.
Patients were divided into 2 groups, the no RF group and RF group. The demographics were nearly identical. Both groups had a similar male sex distribution (47.8% vs 48.0%), age (63.4 vs 63.4) and BMI (30.1 vs 29.6). Among osteotomy techniques, ACR procedures were significantly more common in the RF group (18.0%) compared to the no RF group (6.9%), suggesting a notable increase in the risk for RF (χ2 = 4.015, P = .045). On the other hand, performing 3COs such as IDO (18.9% vs 10.2%, χ2 = 1.796, P = .18) and PSO (23.3% vs 16.3%, χ2 = 0.943, P = .331) showed no significant association with the risk of RF.
Rod Fracture Risk by Instrumented Levels
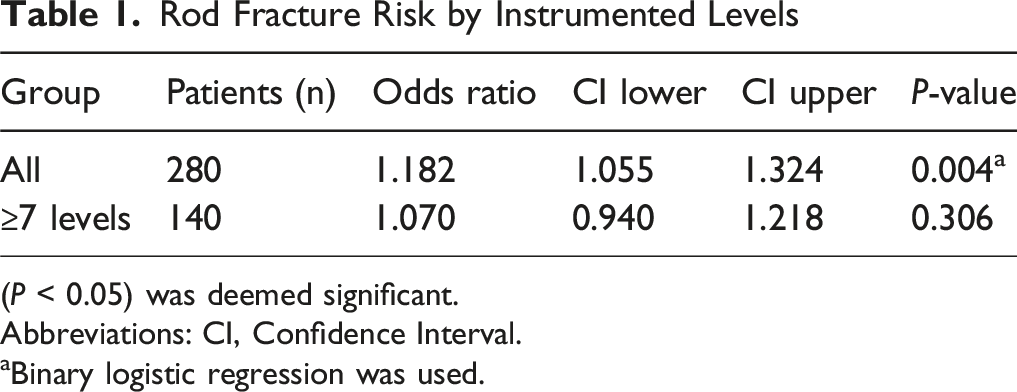
(P < 0.05) was deemed significant.
Abbreviations: CI, Confidence Interval.
aBinary logistic regression was used.
Patient Demographics and Clinical Characteristics
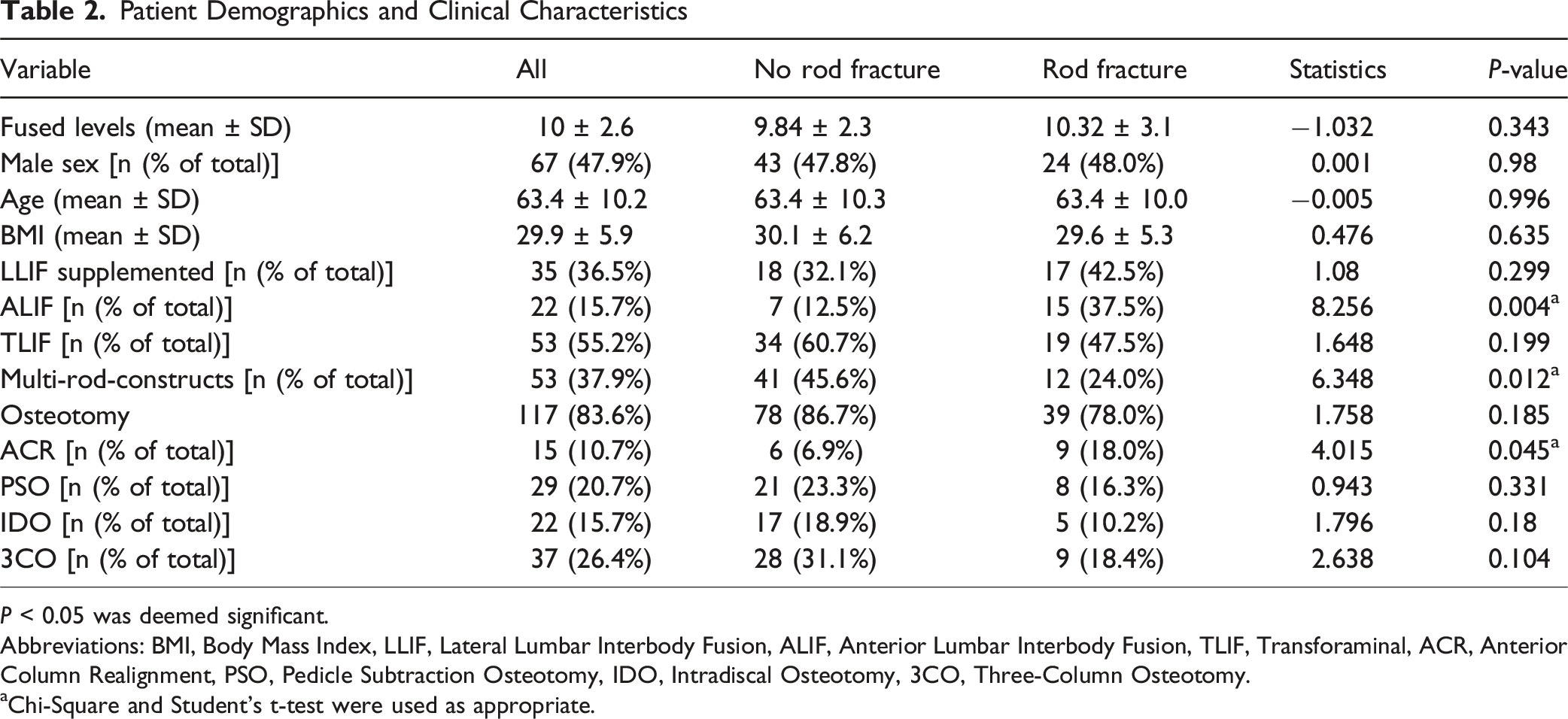
P < 0.05 was deemed significant.
Abbreviations: BMI, Body Mass Index, LLIF, Lateral Lumbar Interbody Fusion, ALIF, Anterior Lumbar Interbody Fusion, TLIF, Transforaminal, ACR, Anterior Column Realignment, PSO, Pedicle Subtraction Osteotomy, IDO, Intradiscal Osteotomy, 3CO, Three-Column Osteotomy.
aChi-Square and Student’s t-test were used as appropriate.
More Rods, More Endurance
Analysis of preoperative predictors showed no significant association between RF and patient specific characteristics such as age at surgery (rho = −0.016, P = .851), BMI (rho = −0.046, P = .592), sarcopenia (rho = 0.072, P = .502), ODI (rho = −0.151, P = .089) and frailty score (rho = 0.078, P = .361), did not show to affect the RF rate. Also, patient reported preoperative average (rho = 0.152, P = .620) and maximum pain (rho = 0.159, P = .459) did not prove to be a factor in the occurrence of the postoperative RF rates.
Notably, the number of rods implanted during surgery demonstrated a statistically significant negative correlation with RF occurrence (rho = −0.211, P = .012). Suggesting the presence of more rods to lead to higher stability, endurance and lower RF rates. A separate analysis stratifying patients into a single-rod (one on each side) and multi-rod group (3 or 4 rods total), confirmed these results, showing a significantly lower RF rate in the multi-rod group (χ2 = 6.348, P = .012) (Figure 2). Preoperative Predictors of Rod Fracture. While Most Predictors Showed no Significant Correlation, the Number of Rods after Surgery was Significantly Associated With Rod Fracture Occurrence (ρ = −0.211, P = .012), Indicating a Potential Protective Effect of Increased rod Support. Abbreviations: (BMI) Body Mass Index, (ODI): Oswestry Disability Index; ρ: Spearman’s rho, P-value < .5 was Deemed Significant*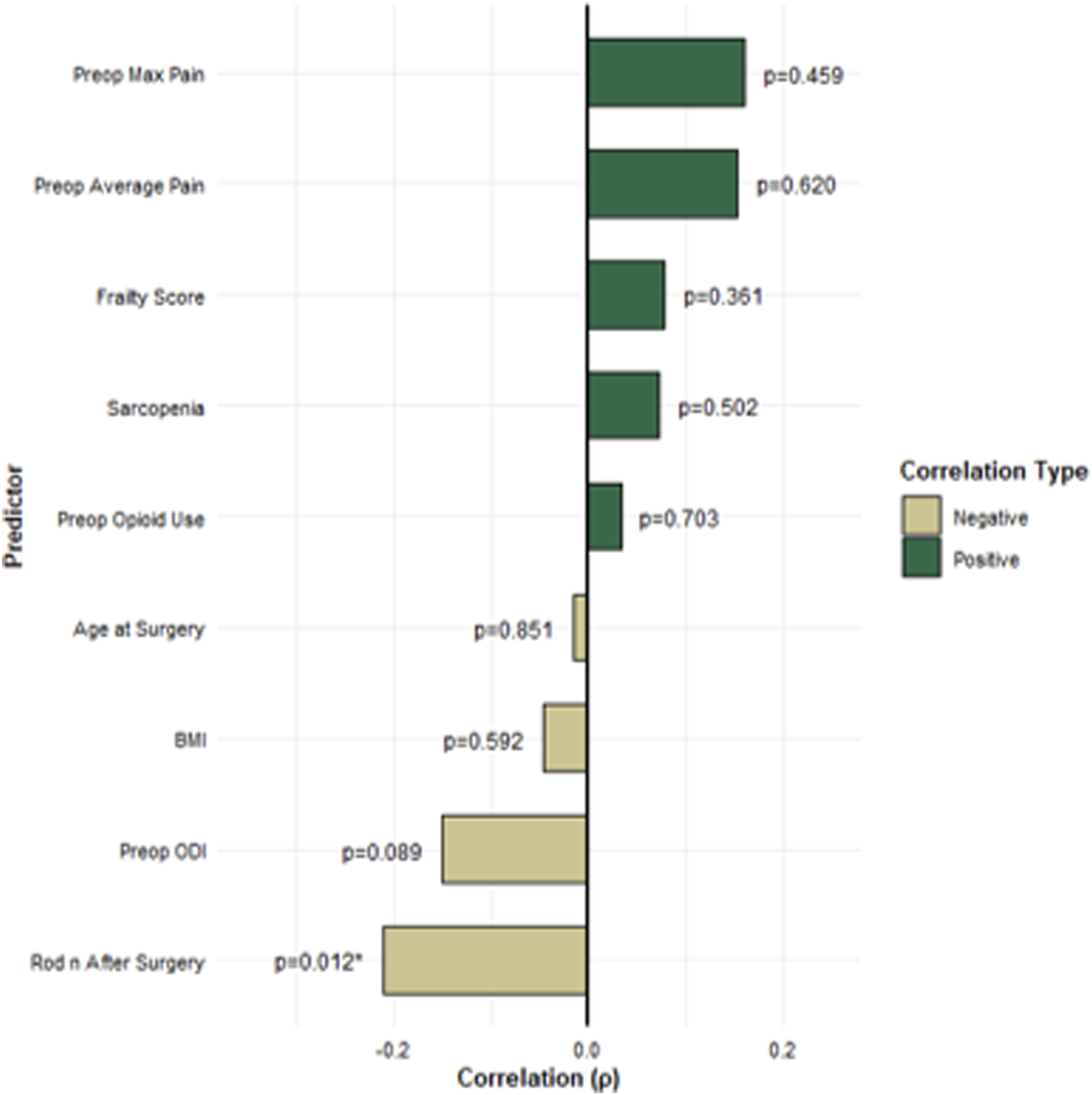
Preoperative Spinopelvic Parameters as Predictors of Rod Fracture Rates
Our study revealed that patients who developed RF exhibited significantly higher preoperative PI. Specifically, the mean PI in the RF group was 60.52° ± 10.53, whereas the non-RF group had a mean PI of 56.53° ± 10.85 (P = .037). A similar trend was observed in preoperative PT, where patients who experienced RF had higher PT (28.71° ± 7.59) in contrast to those without RF (25.79° ± 8.8; P = .042).
Preoperative Spinopelvic Parameters and Rod Fractures
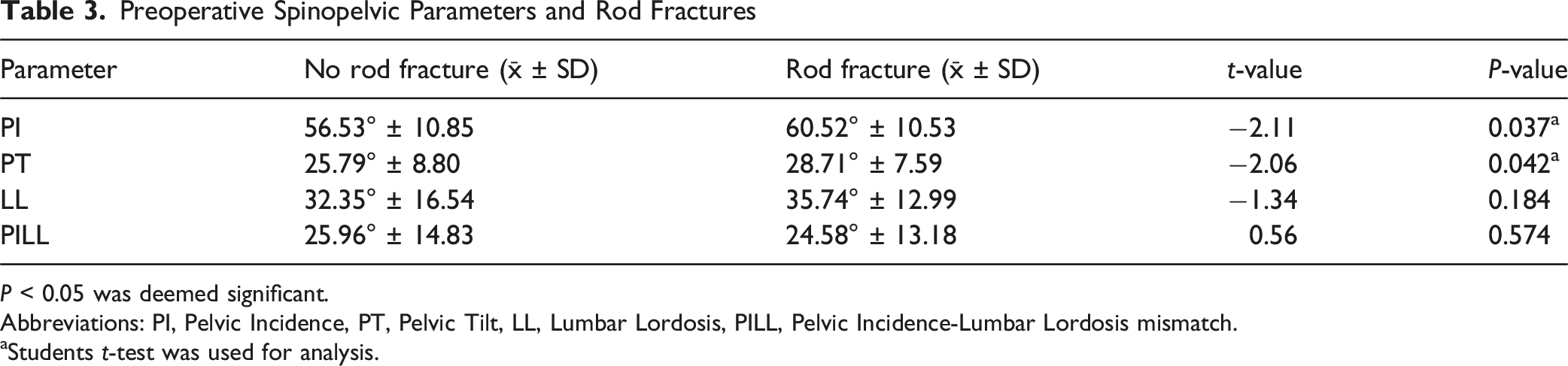
P < 0.05 was deemed significant.
Abbreviations: PI, Pelvic Incidence, PT, Pelvic Tilt, LL, Lumbar Lordosis, PILL, Pelvic Incidence-Lumbar Lordosis mismatch.
aStudents t-test was used for analysis.
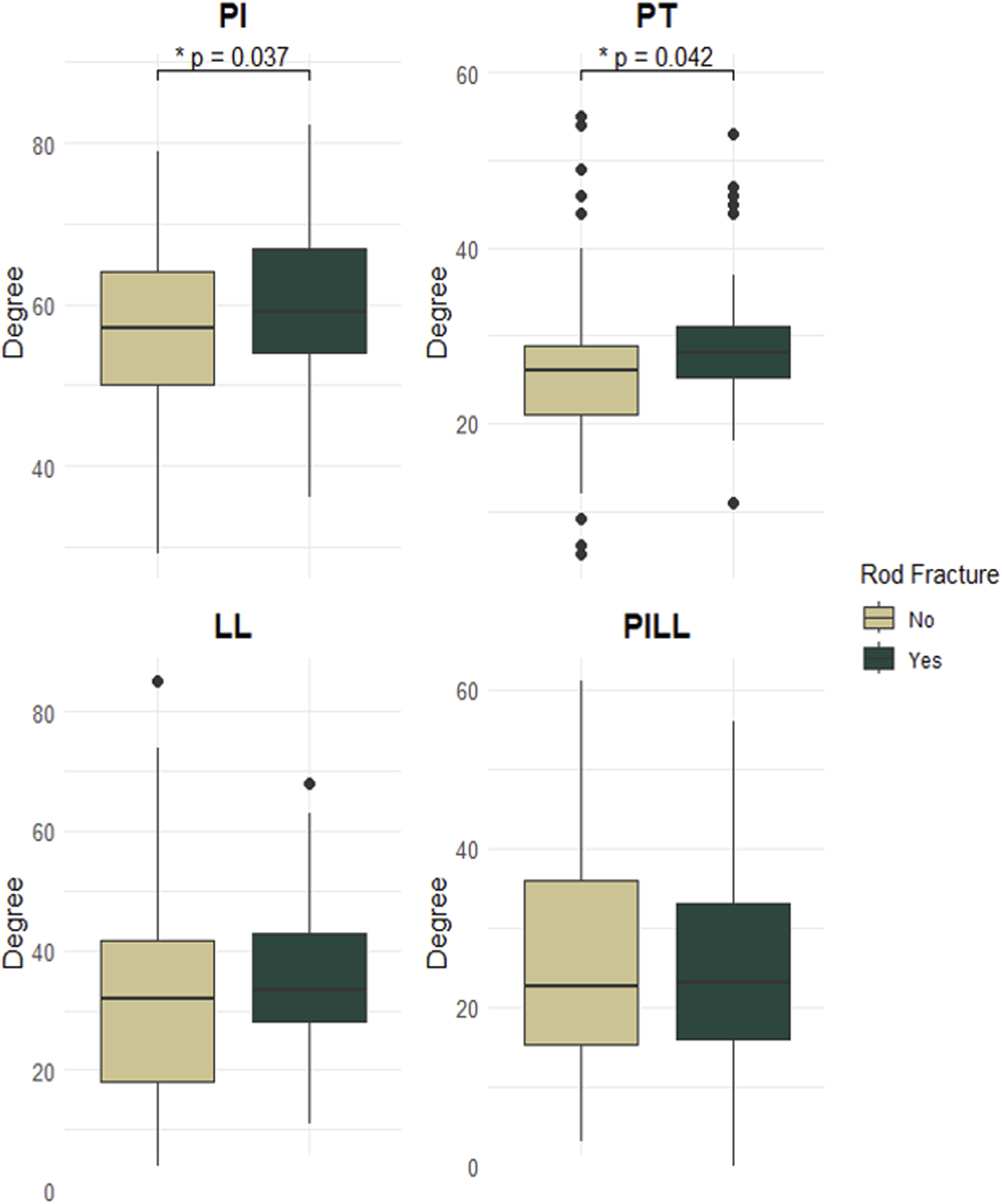
Preoperative Spinopelvic Parameters and Rod Fractures. Displaying the Results From Table 3. Patients who Sustained Rod Fractures had Significantly Higher Preoperative PI (P = .037) and PT (P = .037). Abbreviations: PT: Pelvic Tilt, PI: Pelvic Incidence, LL: Lumbar Lordosis, PILL: Pelvic Incidence Lumbar Lordosis, SD: Standard Deviation. P-value < .5 was Deemed Significant*
Lack of Improvement in Pelvic Incidence-Lumbar Lordosis Mismatch Increases Rod Fracture Rates
While postoperative spinopelvic parameters such as postoperative PT with 21.57° ± 7.73 in the RF group vs 19.83° ± 8.81 in the non-RF group (P = .229), LL 50.36° ± 11.31 vs 48.3° ± 8.97 (P = .273), and PILL 11.92° ± 11.06 vs 9.69° ± 6.93 (P = .264) did not individually predict RF occurrence, the degree of improvement in PILL was shown to be a significant predictor. Patients who experienced lower improvement in PILL (−15.27° ± 12.08) had higher RF rates compared to those with greater improvement (−19.92° ± 13.8; P = .042).
Preoperative Spinopelvic Parameters and Rod Fractures
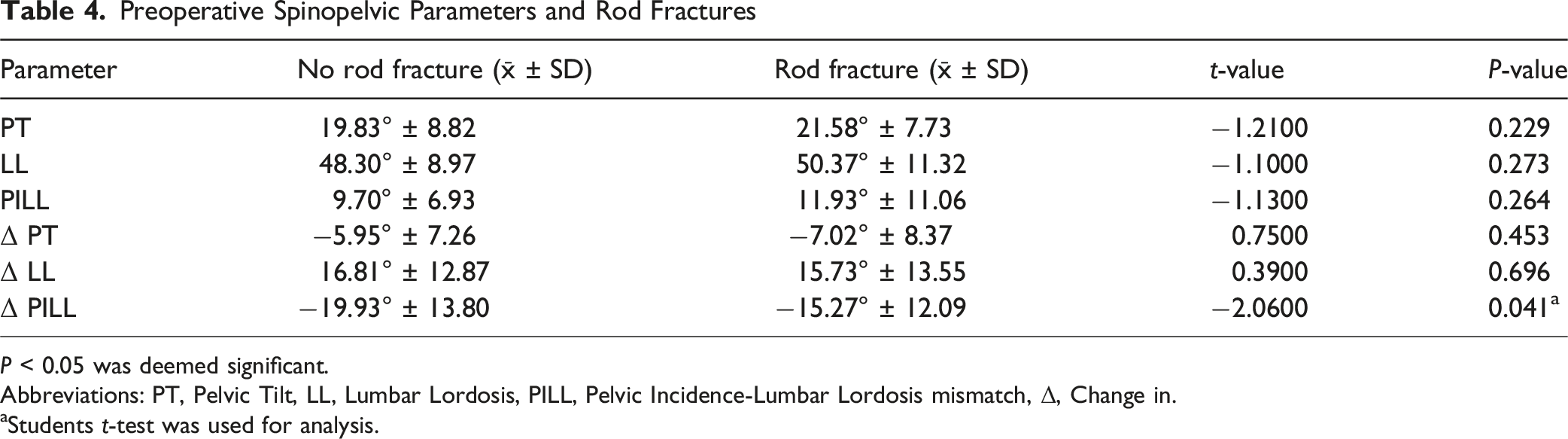
P < 0.05 was deemed significant.
Abbreviations: PT, Pelvic Tilt, LL, Lumbar Lordosis, PILL, Pelvic Incidence-Lumbar Lordosis mismatch, Δ, Change in.
aStudents t-test was used for analysis.
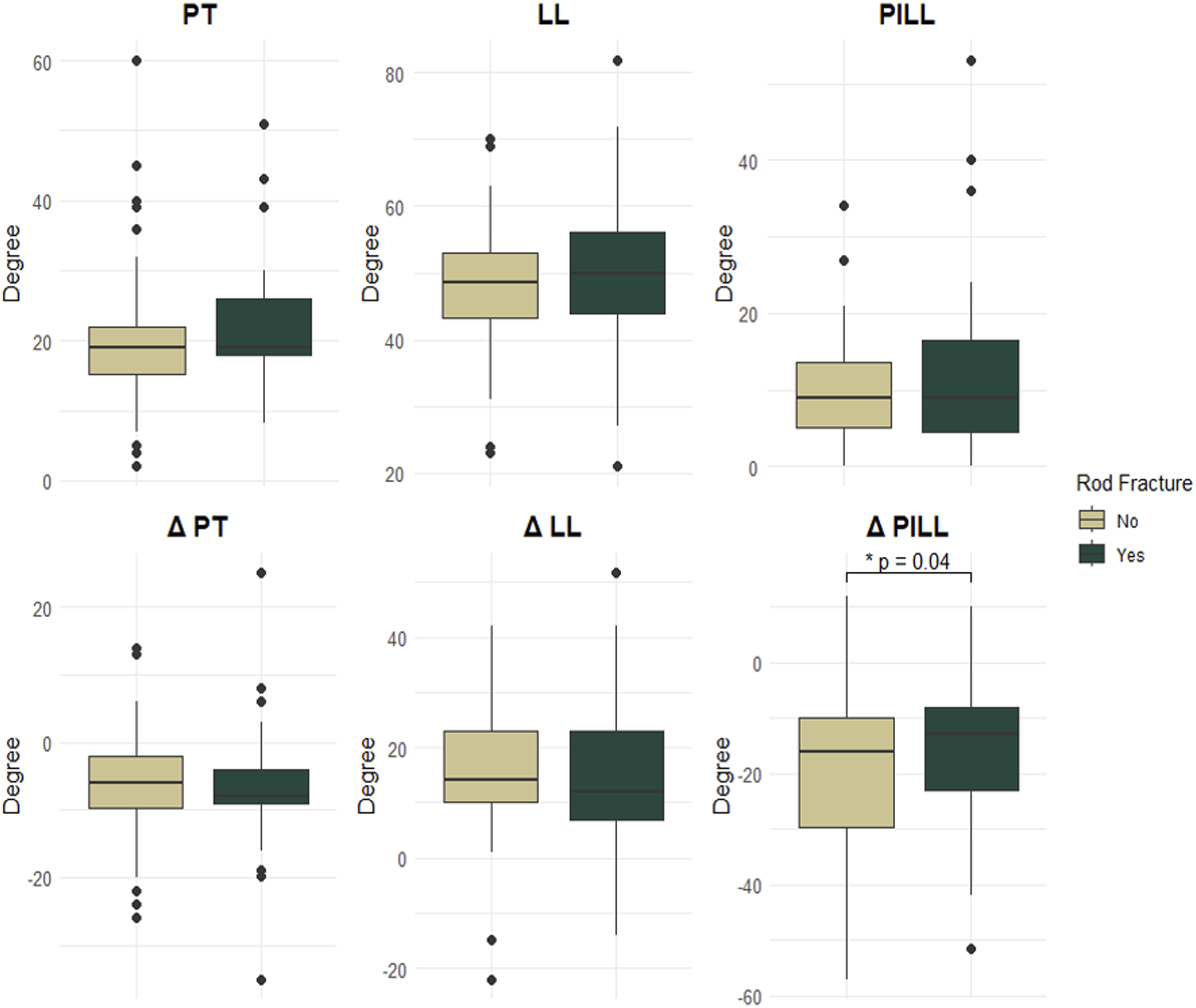
Postoperative Spinopelvic Parameters and Rod Fractures. Displaying the Results From Table 4. Patients who Sustained rod Fractures, Showed to Have had a Significantly Lower Postoperative PILL Correction (P = .041). PT: Pelvic Tilt, PI: Pelvic Incidence, LL: Lumbar Lordosis, PILL: Pelvic Incidence Lumbar Lordosis, SD: Standard Deviation. Δ: Change in; P-value > .5 was Deemed Significant*
Multivariate Analysis Marks Anterior Column Procedures as a Strong Independent Contributor to Rod Fractures
To minimize bias, a multivariate analysis was performed including the presence of ALIF and/or ACR together with available spinopelvic parameters. The analysis demonstrated that ALIF/ACR was a strong and independent predictor of rod fractures (OR 4.69, 95% CI 1.66-13.25, P = .004), whereas PI, PT, LL, and PILL did not reach statistical significance (Figure 5). Anterior Column Procedures Stand out as an Independent Risk Factor for Rod Fractures. ALIF and ACR are Significant Risk Factors of rod Fractures (P = .004), as Shown in This Multivariate Analysis including Spinopelvic Parameters. ALIF: Anterior Lumbar Interbody Fusion, ACR: Anterior Column Realignment; P value > .5 was Deemed Significant*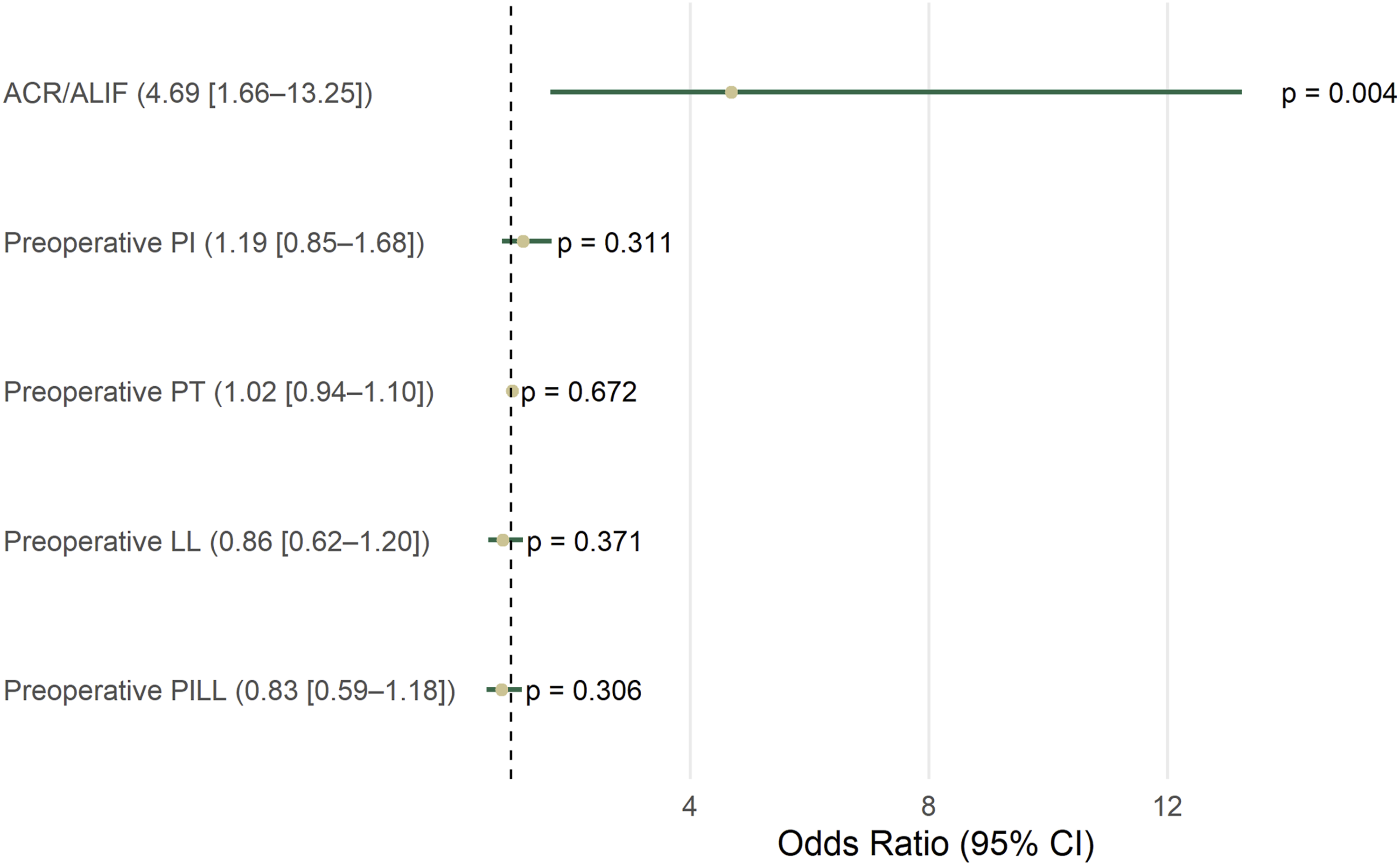
PI and PILL Improvement Are Weak but Sensitive Predictors of RF
Although the overall predictive accuracy of the ROC analyses was modest, both preoperative PI and improvement in PI–LL mismatch demonstrated high sensitivity at their respective optimal cutoffs (52.5 and −26.3) for predicting rod fracture occurrence (Figure 6). PI and PILL Improvement are Weak but Sensitive Predictors of Rod Fracture. Preoperative PI at a Cutoff of 52.5 (AUC = 0.60) and PILL Improvement at a Cutoff of −26.3 (AUC = 0.59), Showed to be Sensitive Predictors of rod Fractures. PI: Pelvic Incidence, PT: Pelvic Tilt, PILL: Pelvic Incidence Lumbar Lordosis, AUC: Area Under the Curve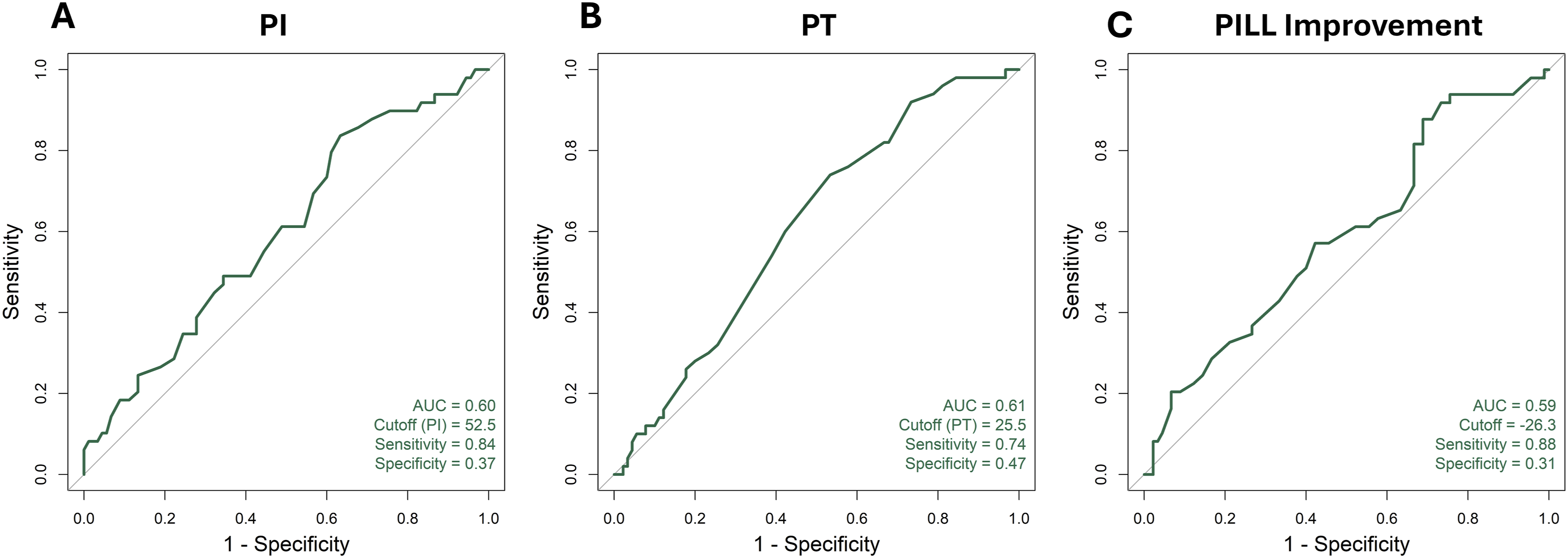
Rod Fractures Lead to Longer Opioid Use and Worsened Functional Outcome
Postoperative Outcome
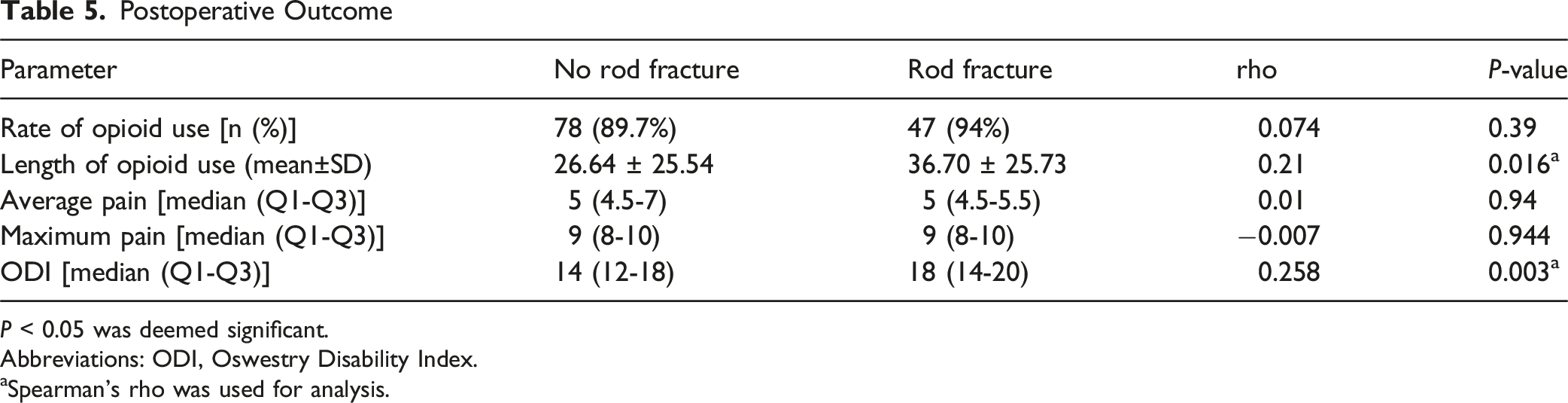
P < 0.05 was deemed significant.
Abbreviations: ODI, Oswestry Disability Index.
aSpearman’s rho was used for analysis.
Discussion
Rod fracture remains a notable mechanical complication following ASD surgery, with significant implications for construct durability, patient function, and the need for revision procedures. This large-scale study identified several key preoperative and perioperative predictors of RF, as well as its postoperative consequences. Specifically, higher PI and PT, inadequate correction of the PILL, and anterior column manipulation, particularly through ALIF or ACR, were significantly associated with increased RF risk. In contrast, the use of multi-rod constructs was found to be protective. Furthermore, RF was associated with prolonged postoperative opioid use and higher ODI scores, underlining its negative impact on recovery and functional outcomes.
Patients with elevated preoperative PI and PT had a significantly higher incidence of RF in univariate testing. While PI also showed high sensitivity in ROC analysis, neither PI nor PT remained significant after multivariate analysis, suggesting their effects may be mediated through surgical strategy and alignment correction rather than acting as independent predictors. Prior work has consistently linked high PT to mechanical failure, but evidence for PI has been inconclusive, with some studies reporting no association.16-20 Our findings suggest that PI, like PT, may still serve as useful markers of risk in preoperative assessment, but their predictive value appears subordinate to surgical approach once confounders are controlled for.
In addition to preoperative parameters, insufficient correction of PILL mismatch emerged as a significant predictor of RF in univariate analysis. Patients with less improvement in PILL postoperatively were more likely to experience rod breakage, suggesting that residual sagittal malalignment contributes to sustained mechanical stress across the construct. However, ΔPILL did not remain significant in multivariate analysis, indicating that the method of achieving sagittal correction, particularly when anterior column procedures are used, may be more decisive than the absolute degree of correction itself. These results are consistent with findings from Lyu et al. and Martin et al., who identified high residual PILL as a contributing factor to RF.21,22 Interestingly, Smith et al. 18 reported an opposite trend, where larger PILL corrections were associated with increased RF rates, possibly due to overcorrection and increased rod strain. Taken together, this variability highlights the importance of patient-specific spinopelvic optimization and the risk of both under- and overcorrection in ASD surgery.
Our study also reinforced the protective role of multi-rod constructs. The addition of accessory rods significantly reduced the incidence of RF, likely due to enhanced biomechanical load distribution. This supports biomechanical data demonstrating that multi-rod configurations reduce stress across individual rods, thereby decreasing fatigue failure rates.23-25 These findings are consistent with current literature advocating for multi-rod strategies, especially in long-segment constructs or in high-risk patients.26-29
Most notably, anterior column manipulation through ALIF or ACR emerged as the strongest independent risk factor for RF after multivariate adjustment. While ALIF has traditionally been associated with improved sagittal correction and lower rates of posterior mechanical failure, 30 our results suggest that its use may introduce new failure points. This could be due to the increased curvature and contouring demands placed on the rods at ALIF or ACR levels, or due to micromotion caused by disruption of the anterior longitudinal ligament during anterior approaches.31,32 It is also possible that ALIF is more frequently selected for patients with greater sagittal deformity and larger PILL mismatch, factors already associated with higher RF risk. 33 These findings emphasize the need to better understand the biomechanical implications of anterior column approaches and to optimize construct stability when used.
While prior literature has implicated higher age, BMI, and male sex as risk factors for RF,7,18 our study did not find statistically significant associations with these demographic variables. This is in line with other studies that have also failed to show consistent links between demographics and RF risk.34,35 These conflicting findings suggest that the influence of demographic variables may vary across populations, surgical techniques, or alignment goals.
From an outcome’s standpoint, RF did not correlate directly with higher pain scores postoperatively. However, it was significantly associated with prolonged opioid use and higher ODI scores. This may be due to the delayed nature of RF development and the morbidity associated with subsequent revision surgeries. These findings echo previous reports demonstrating the negative impact of RF on overall function, patient satisfaction, and quality of life. 7
Limitations
This study is subject to the inherent limitations of retrospective cohort designs. All patients were treated at a single academic center, which may limit generalizability to other institutions with differing patient populations or surgical practices. Although the overall cohort size is robust, certain subgroups may remain underpowered. As pseudoarthrosis is a studied cause of RF, it could not be evaluated in this study since fusion assessments (using CT-scan) were not performed in asymptomatic patients or those without RF. The long duration of the study may also introduce variation in results, as surgical techniques and technology have advanced over time. While multiple alignment scores were incorporated into the analysis, other metrics such as the GAP score and L1/T4 ratio should be considered in future research to provide a more comprehensive assessment. Similarly, the number of LLIF procedures performed may influence RF risk, and this should be evaluated in future investigations as suggested by prior work. 36 Furthermore, while ODI, pain scores, and opioid use were analyzed, additional patient-reported outcomes such as the SRS-22 could be utilized in future studies to better capture the impact of RF on patient quality of life. Future prospective, multicenter studies with standardized operative protocols are needed to validate these findings and clarify their clinical implications.
Conclusion
Rod fracture continues to pose a substantial challenge in adult spinal deformity surgery, with significant consequences for recovery and long-term function. In univariate analyses, higher preoperative PI and PT, inadequate correction of PILL mismatch, and anterior column manipulation were associated with increased RF risk, while multi-rod constructs were protective. However, after multivariate adjustment, anterior column manipulation (ALIF/ACR) emerged as the sole independent predictor of RF. RF was also associated with prolonged opioid use and increased disability as measured by ODI, despite not directly correlating with pain scores. These findings reinforce the importance of meticulous surgical planning, sagittal alignment optimization, and the judicious use of multi-rod constructs to mitigate the risk of mechanical failure. Future research should continue to refine our understanding of biomechanical and alignment strategies to enhance construct longevity and patient outcomes in ASD surgery.
Footnotes
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. Institutional review board (IRB) approval was obtained prior to the initiation of the study. Patient data was anonymized to ensure confidentiality, and no identifiable information was included in the analysis.
Consent to Participate
As this was a retrospective study, the requirement for informed consent was waived by the IRB. All data were collected and stored in compliance with institutional and regulatory guidelines to maintain the privacy and security of patient information.
Author Contributions
chahin Salmanian: Conceptualization, Methodology, Formal analysis, Investigation, Data Curation, Writing – Original Draft, Visualization; Jay Kumar: Investigation, Writing – Original Draft; César Carballo Cuello: Investigation, Writing – review and editing; Diego Soto Rubio: Data Curation, Writing – Original Draft; Mark Greenberg: Writing – review and editing; Erik Hayman: Writing – review and editing; Mohsen Rostami: Investigation, Writing – Original Draft; Puya Alikhani: Writing – review and editing, Supervision, Project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study contain patient information and are therefore not publicly available. However, de-identified data can be provided by the corresponding author upon reasonable request and with appropriate institutional ethics committee approval.
IRB Approval
Institutional Review Board Under (No. Pro00023643).