
Abstract
Study Design
Systematic review and Meta-analysis.
Objective
This systematic review seeks to compare fusion, reoperation and complication rates, estimated blood loss (EBL), and surgical time between multi-level instrumented fusions with LIVs (lowest instrumented vertebra) in the cervical spine and those that extend into the thoracic spine.
Summary of Background Data
Several studies address the question of whether to extend a long-segment, posterior cervical fusions, performed for degenerative disease, into the upper thoracic spine. Recommendations for appropriate LIV continue to vary.
Methods
A comprehensive computerized literature search through multiple electronic databases without date limits up until April 3rd, 2020 using combinations of key search terms and sets of inclusion/exclusion criteria was performed.
Results
Our comprehensive literature search yielded 3852 studies. Of these, 8 articles consisting of 1162 patients were included in the meta-analysis. In 61.2% of the patients, the fusion did not cross the cervicothoracic junction (CTJ) (cervical LIV, CLV). In the remaining 38.8%, the fusion extended into the upper thoracic spine (thoracic LIV, TLV). Overall, mean patient age was 62.5 years (range: 58.8-66.1 years). Our direct analysis showed that odds of fusion were not statistically different between the CLV and TLV groups (OR: .648, 95% CI: .336-1.252, P = .197). Similarly, odds of reoperation (OR: 0.726, 95% CI: 0.493-1.068, P = .104) and complication rates were similar between the 2 groups (OR: 1.214, 95% CI: 0.0.750-1.965, P = .430). Standardized mean difference (SMD) for the blood loss (SMD: .728, 95% CI: 0.554-.901, P = .000) and operative (SMD: 0.653, 95% CI: .479-.826, P = .000) differed significantly between the 2 groups. The indirect analysis showed similar fusion (Effect Size (ES)TLV: .892, 95% CI: .840-.928 vs ESCLV:0.894, 95% CI:0.849-.926); reoperation rate (ESTLV:0.112, 95% CI: 0.075-.164 vs ESCLV: .125, 95% CI: .071-.211) and complication rates (ESTLV: .108, 95% CI: .074-.154 vs ESCLV:0.081, 95% CI: .040-.156).
Conclusions
Our meta-analysis showed that fusion, complication, and reoperation rates did not differ significantly between patients in whom multi-level posterior fusions ended in the cervical spine vs those of which was extended into the thoracic spine. The mean blood loss, operative time and length of stay were significantly lower in patients with CLV at C6 or C7, compared to their counterparts. These data suggest that, absent focal, C7-T1 pathology, extension of long, posterior cervical fusions into the thoracic spine may not be necessary.
Keywords
Introduction
Spine surgeons have been taught that long, posterior cervical fusions ending at C7 risk subjacent failure at the cervicothoracic junction. In recent years, a number of studies have sought to compare the outcomes of surgeries ending in the lower cervical spine vs those extended into the upper thoracic spine. These studies have offered conflicting results and recommendations.
In biomechanical terms, the mobile, lordotic cervical spine, that allows the head to remain over the body and facilitates forward gaze, meets the stiffer thoracic kyphosis, designed to facilitate lung expansion.1,2 The abrupt change in alignment and mobility at the cervicothoracic junction (CTJ) is thought to pre-dispose patients with long posterior cervical fusion to early subjacent failure. In response, many surgeons have recommended extension of these constructs into the upper thoracic spine.1,3
The results of extant studies comparing the radiographic outcomes of different caudal end levels have been contradictory. Some studies show that revision rates are up to 17% higher when the construct ends at C7 as opposed to T1 or T2, 1 while others show no significant difference in revision rates.3,4 In fact, various studies have shown no statistically significant difference in fusion rates, complications rates and radiological parameters between constructs ending cervically vs those that cross the CTJ.2,4
In our previous work, we suggested that clear benefits of extension into the thoracic spine were limited and that this approach was best limited to patients with poor bone quality, poor C7 fixation potential, or significant spondylosis, instability or deformity at C7-T1. We noted that thoracic extension was associated with a significant increase in surgical time and blood loss.5,6
In this meta-analysis, our goal was to compare fusion, reoperation and complication rates along with estimated blood loss (EBL), surgical time and length of stay (LOS) between constructs with cervical LIV and those that extend into the thoracic spine.
Materials and Methods
Study Design
A systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) Statement for Reporting Systematic Reviews. 7 The study was Institutional Review Board exempt.
Search Criteria
We conducted a comprehensive computerized literature search through multiple electronic databases without date limits up until April Week 3, 2020 using combinations of key search terms. Initial searches were designed to be all encompassing and capture as many articles as possible. Project lead and team members then narrowed the results using the inclusion/exclusion criteria below. MEDLINE searches employed both PubMed and Ovid engines; Web of Science was also queried for potential studies. PubMed included biomedical literature from MEDLINE and additional life science journals (1947-Present). The Ovid search included: Ovid MEDLINE(R) (1946-Present). Web of Science collections searched included: Science Citation Index Expanded (SCI-EXPANDED) (1900-present) and Emerging Sources Citation Index (ESCI) (2005-present). The search strategy used for PubMed, OVID Medline, and Web of Science are shown in Supplemental Digital Content (SDC).
Search Terms
Our search strategy focused on the combinations of key terms: “posterior cervical fusion,” “posterior cervical decompression,” “cervicothoracic fusion,” “discectomy,” “diskectomy,” “anterior cervical fusion,” “sagittal alignment,” “thoracolumbar alignment,” “cervical alignment,” “posterior instrumentation,” “vertebral segmentation,” “cervical vertebrae/diagnostic,” “imaging,” “cervical vertebrae surgery,” “spinal fusion,” “cervicothoracic deformity,” “ossification of the posterior longitudinal ligament,” “cervical spondylotic myelopathy,” “intervertebral disc degeneration,” “radiculopathy,” “horizontal gaze,” “vertebral segmentation,” “Roussouly,” “subaxial cervical spine,” “adjacent-segment pathology,” “sagittal balance,” “adjacent segment disease,” “adjacent segment degeneration,” “pseudarthrosis,” “spinal stenosis,” “spondylitis,” “spondylosis,” “C7,” “T1,” “cervicothoracic,” “cervico-thoracic,” “cervical-thoracic,” and “multi-level cervical.”
Inclusion/Exclusion Criteria
Articles were screened using inclusion criteria: full-text studies published in peer-reviewed journals in English or translated into English and studies with patients undergoing multi-level posterior cervical fusions or combined anterior and posterior cervical fusion involving C7, with primary diagnosis of degenerative cervical spine disease.
Studies with the following criteria were excluded: 1) non-English; 2) patients undergoing single-level fusion, 3) indication for surgery was trauma, tumor, fracture or infection, 4) the primary procedure was arthroplasty, laminoplasty, corpectomy, or anterior cervical discectomy and fusion only, and 6) any case reports, reviews, editorials, and abstracts.
Data Extraction
Two research librarians (DE and HL) and 2 researchers (DS and AD) performed the electronic database search. Two authors (MG and JS) independently reviewed potentially these studies to be included in the systematic review. Disagreements on the inclusion of a study between the 2 authors were resolved by a third author (ET). In addition, we also performed manual searches of review bibliographies and reference lists of primary studies not captured by the electronic searches. To further avoid missing studies not referenced in our original papers’ bibliographies or our literature searches, we sought additional recommendations from prominent researchers in the field. Additional full text references were then obtained and analyzed for inclusion. Figure 1 shows the PRISMA flowchart for search methodology. Flow chart of systematic review.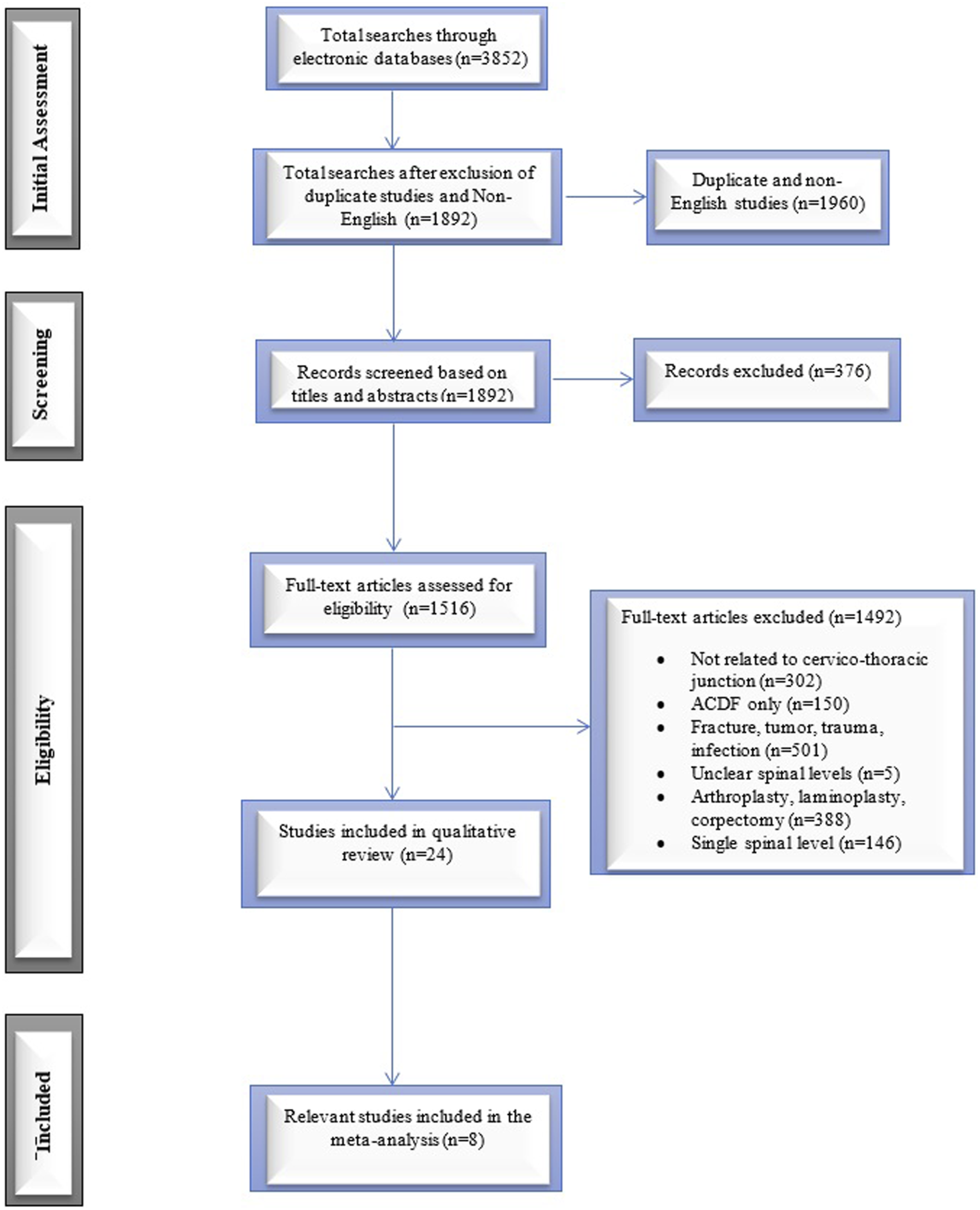
Two authors independently extracted the following data from the studies: demographic such as sex and age; sample size, study design, minimum posterior levels, caudal levels, surgical approach (such as posterior or combined anterior and posterior approach), length of follow-up, and fusion assessment details. The primary outcomes of the study were: fusion, complication, and reoperation rates. Our secondary outcomes were: estimated blood loss, operative time, complication details, and patient reported outcomes.
Meta-Analysis
We conducted both direct and indirect meta-analysis. These analyses were performed for fusion rate, reoperation rate, complication rate, estimated blood loss, and operative time. For the discreet variables, the direct meta-analysis outcomes were reported using odds ratios (ORs) with 95% confidence intervals (CIs). The outcomes for continues variables were expressed as standardized mean difference with 95% CIs. The outcomes for the indirect analysis were expressed as pooled proportions of events. All meta-analysis was conducted using random-effects model to account for high variability between the studies. 8 Level of significance was set at α = .05. All the meta-analyses were performed using Comprehensive Meta-Analysis version 3.3.070 (Biostat Inc., NJ, USA).
Quality and Publication Bias Assessment
The quality assessment was performed using Newcastle–Ottawa Quality Assessment Scale 9 and GRADE (Grading for Recommendations, Assessment, Development and Evaluations) criteria 10 . Publication bias were represented as funnel plots. Besides examining for obvious asymmetry, 11 Begg and Mazumdar rank correlation, 12 and Egger’s regression intercept 13 tests were used to investigate the significance of the publication bias for discreet and continuous variables, respectively.
Number Needed to Harm Assessment
In an effort to understand the benefit/harm of crossing vs not crossing the CJT, we assessed the number of patients, on average, with a cervical LIV in order for 1 patient to require reoperation for subjacent degeneration over the course of 2 years follow-up. NNH was calculated as the reciprocal of absolute risk increase (i.e., the negative impact of a treatment in a given patient population).
Results
Our comprehensive literature search yielded 3852 studies. Of these, we excluded those (1960 studies) identified as duplicate or non-English language articles. After screening the titles and abstracts, a total of 1516 full-test articles were assessed for eligibility. Based on inclusion/exclusion criteria, we further excluded 1492 articles. A total of 24 studies were included in full-text analysis. Eight articles were included in the meta-analysis.6,4,14,2,5,15,1,3 All 8 included studies compared the surgical outcomes for patients undergoing multi-level posterior cervical fusion (PCF) crossing the CTJ with those ending in the lower cervical spine. Figure 1 shows the PRISMA search strategy.
Demographic and Study Details.
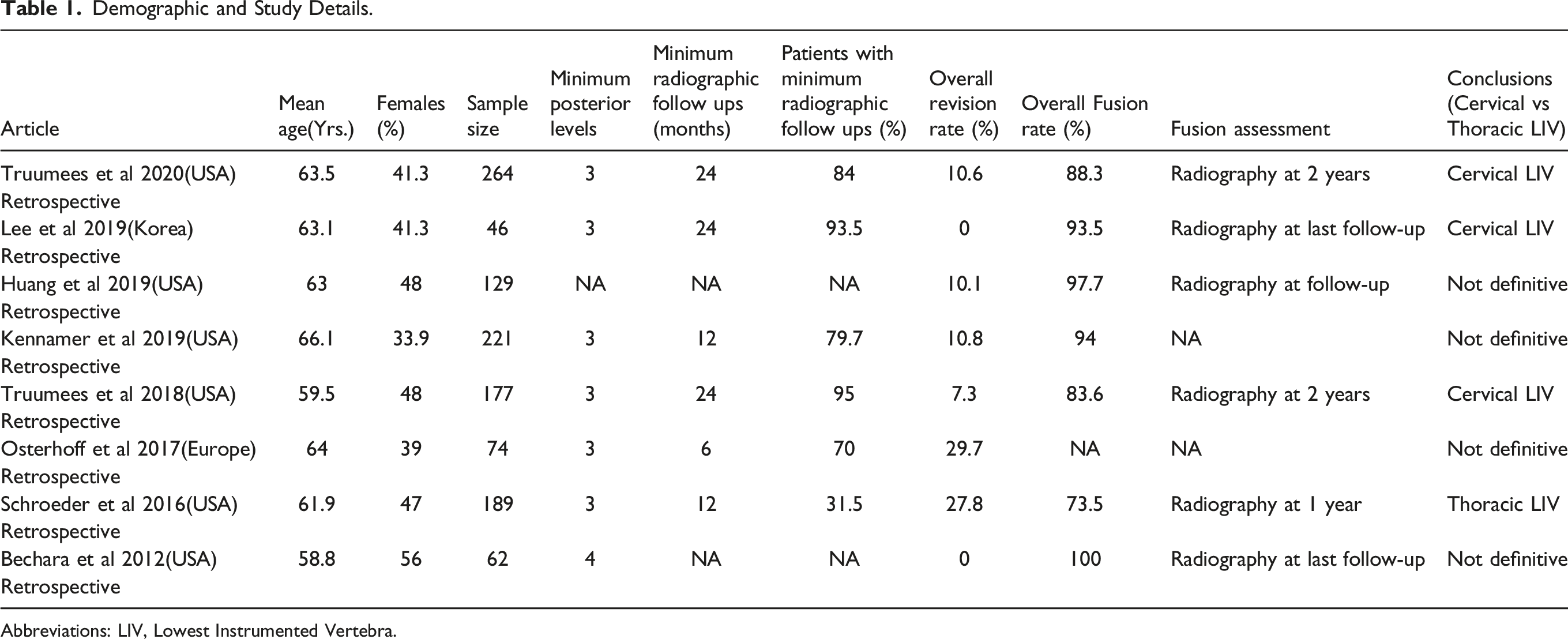
Abbreviations: LIV, Lowest Instrumented Vertebra.
Direct Meta-Analysis
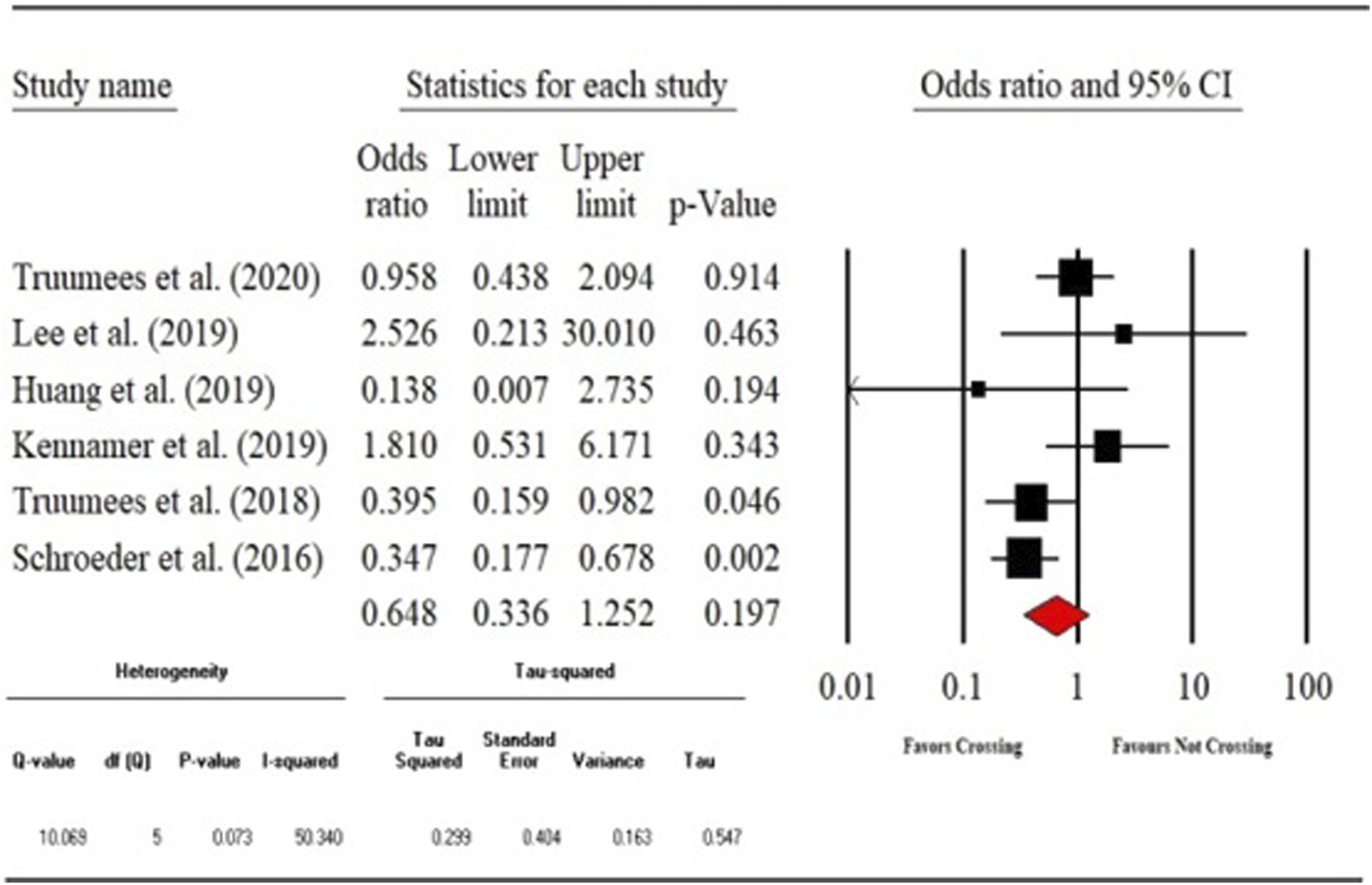
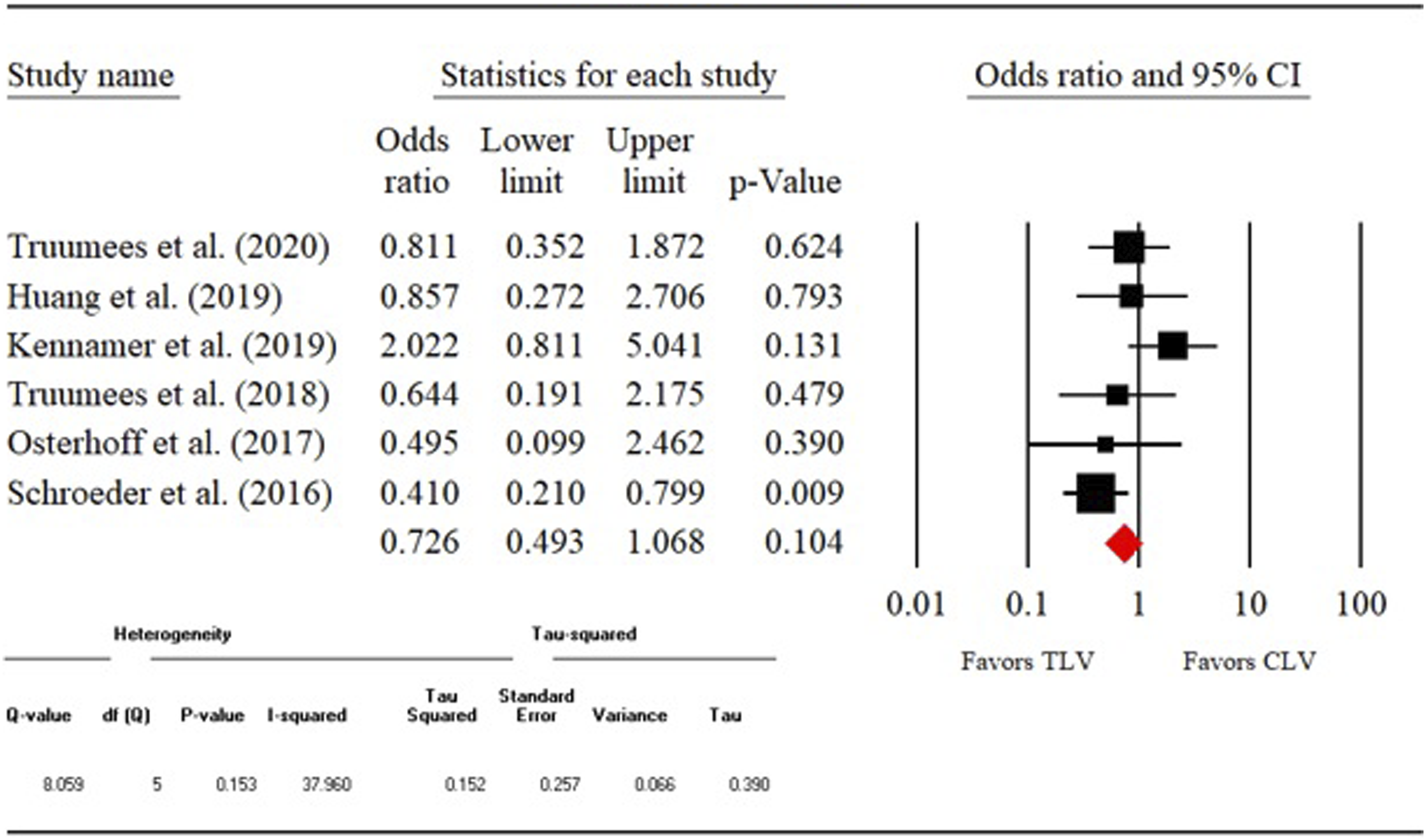
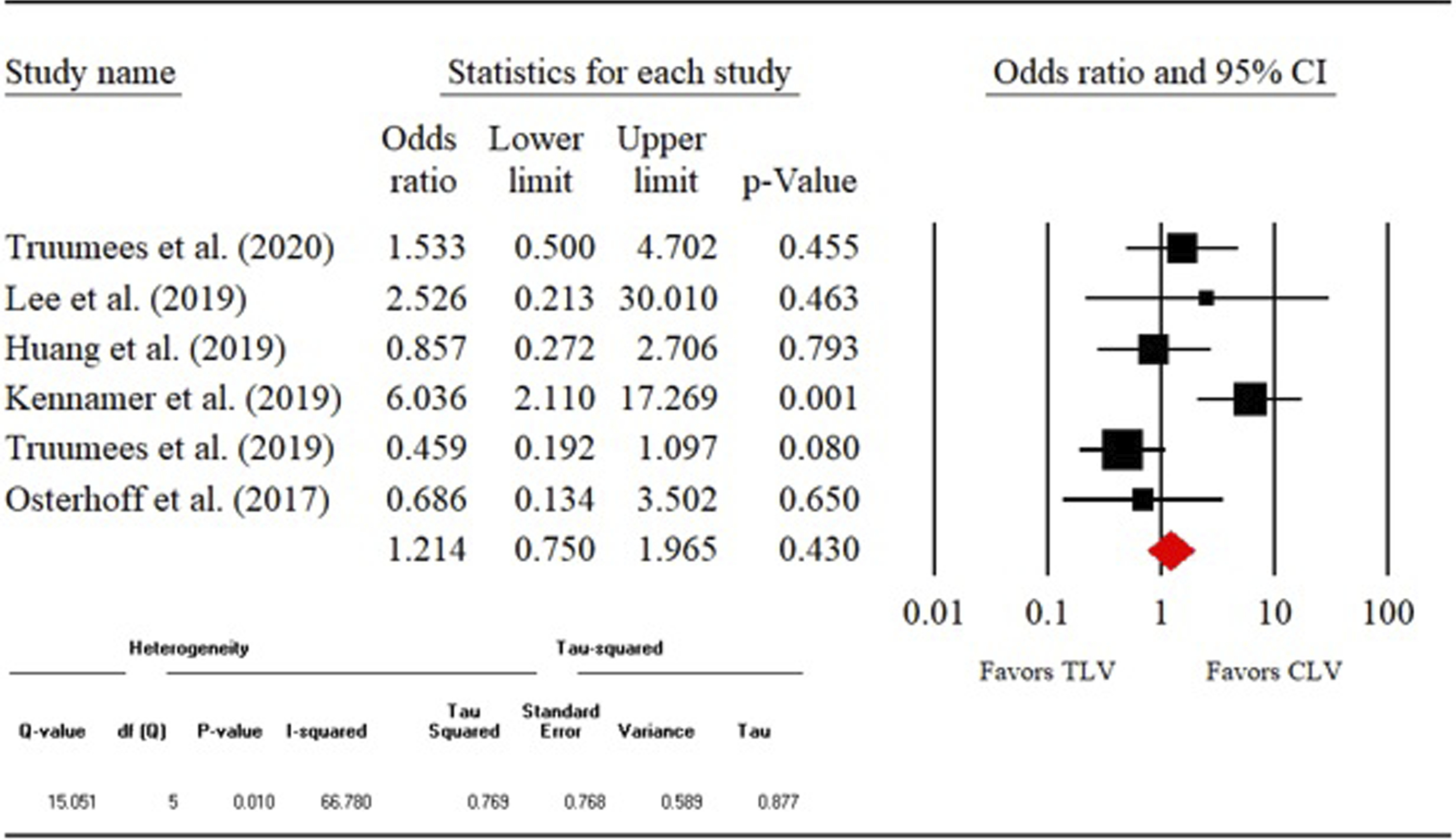
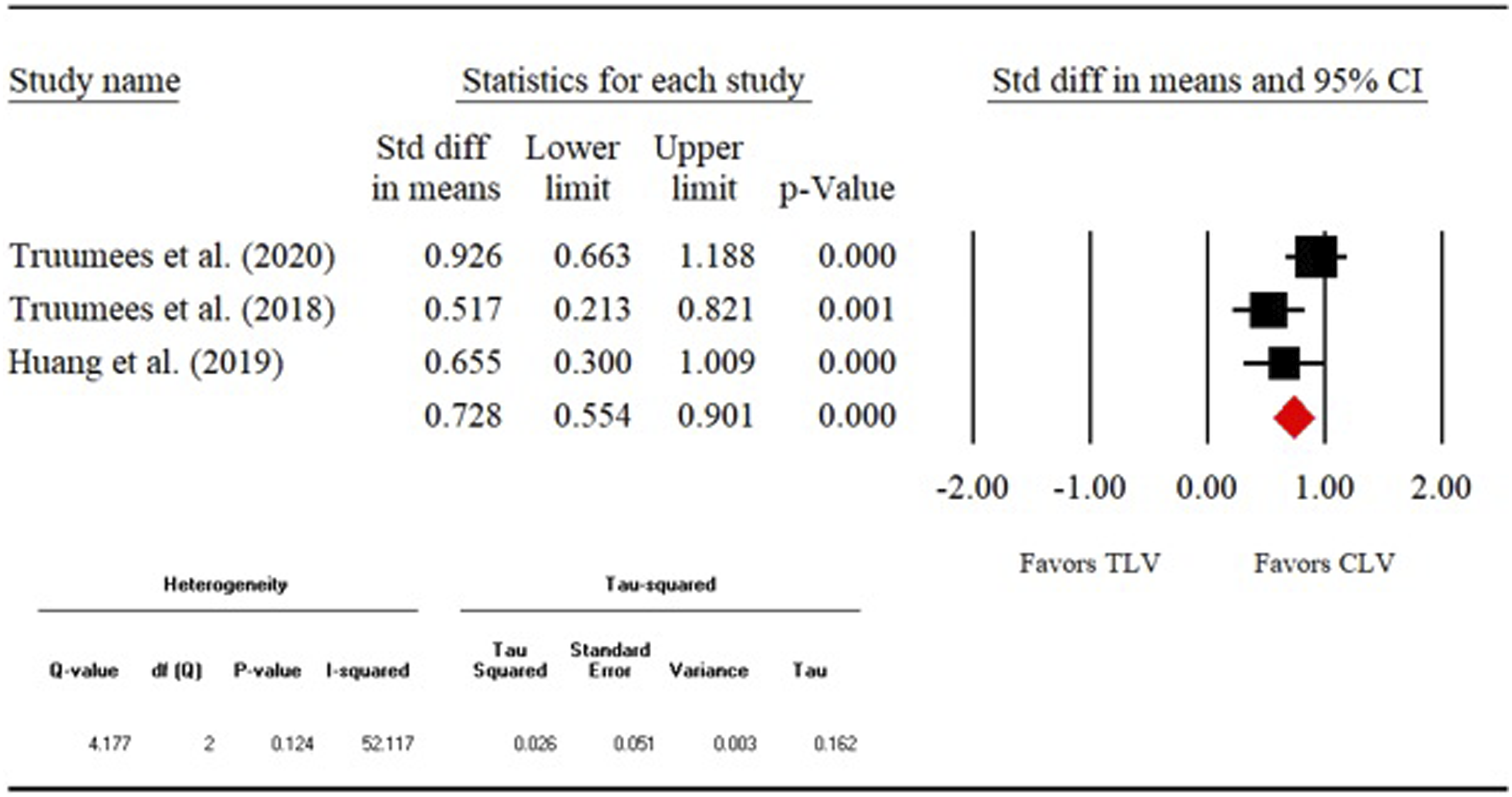
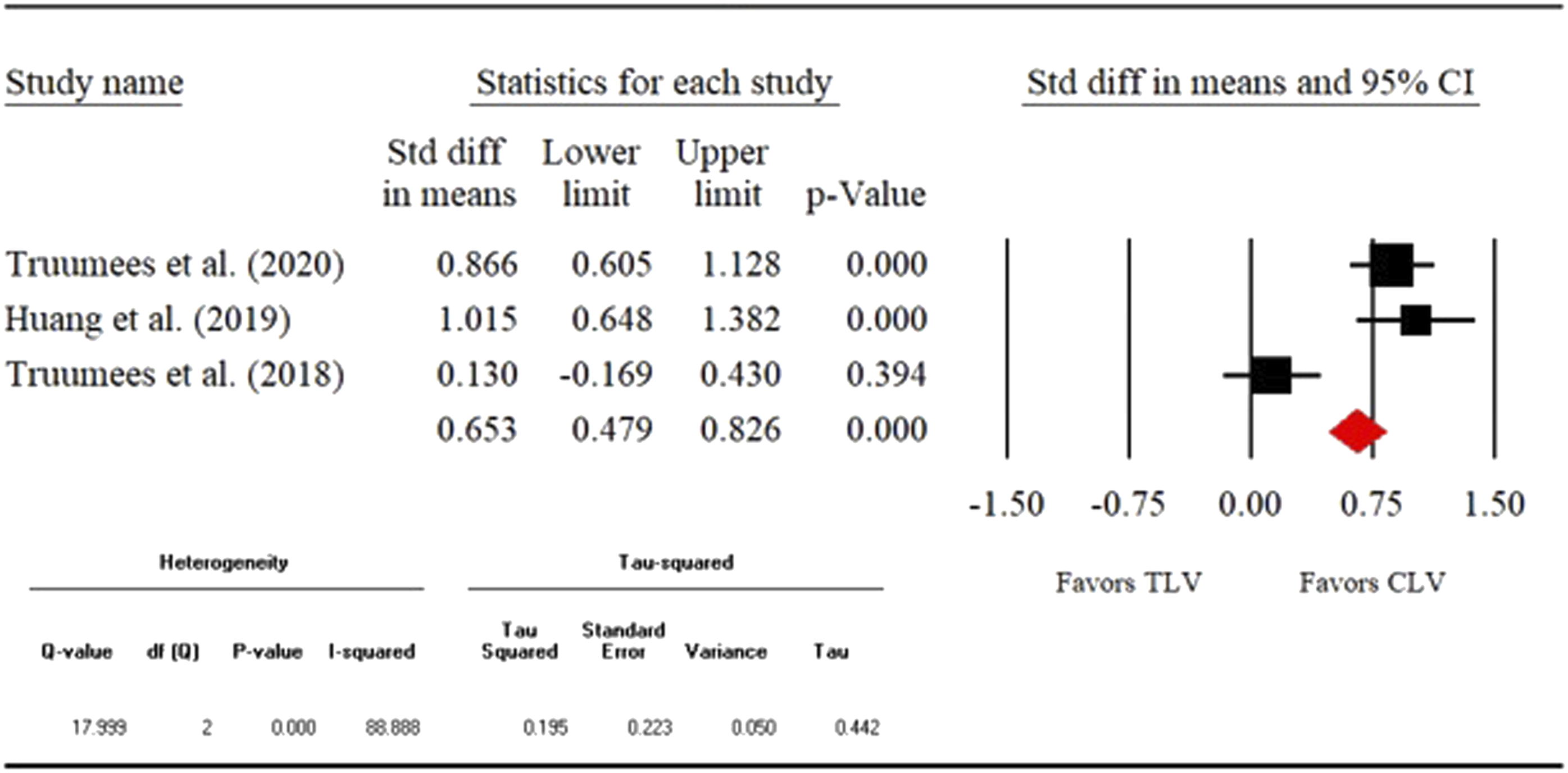
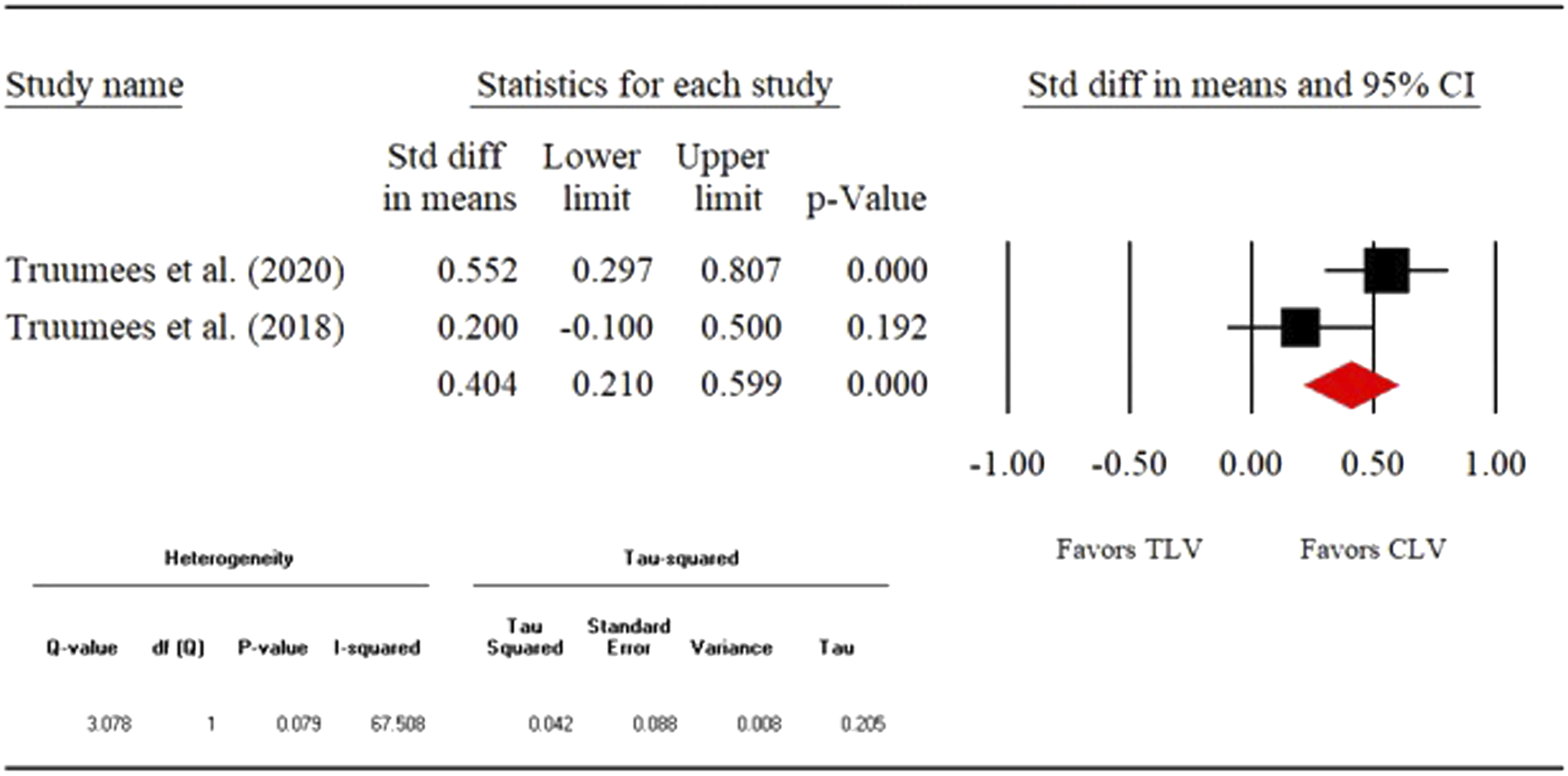
1) Fusion rate- Direct (CLV vs TLV) fusion rate was compared among 6 different studies with the total sample size of 1026 patients. The overall fusion rate was 87.4% (n = 897). Four of the 6 studies assessed the fusion radiographically. The remaining 2 studies did not report this information. Our analysis showed that odds of fusion were not statistically different between crossing vs not crossing the CTJ groups (OR: .648, 95% CI: .336-1.252, P = .197). The detailed results are shown in the forest plot in Figure 2. 2) Reoperation rate- 6 studies (n = 1054) were compared directly to assess the reoperation rates between CLV and TLV groups. The overall reoperation rate was 13.6% (n = 143). As seen from the forest plot (Figure 3), the odds of reoperation did not differ significantly between the 2 groups (OR:0.726, 95% CI:0.493-1.068, P = .104). 3) Complication rate-We compared 6 studies (n = 911) directly to measure the complication rates between CLV and TLV groups. The overall complication rate was 9.5% (n = 87). The odds of complication were similar between the 2 groups (OR:1.214, 95% CI:0.0.750-1.965, P = .430). The detailed analysis is shown in the forest in Figure 4. 4) Mean estimated blood loss- 3 studies (n = 570) were directly compared with respect to the mean estimated blood loss between CLV and TLV groups. Our analysis showed that the standardized mean difference (SMD) was significant between the 2 groups (SMD: .728, 95% CI:0.554-.901, P = .000). As seen from the forest plot (Figure 5), crossing the CTJ during the PCF resulted in significantly greater blood loss compared to the CLV group. 5) Mean operative time- Direct comparison (CLV vs TLV) of mean operative time was performed among 3 studies (n = 570). As seen from the forest plot (Figure 6), the SMD differed significantly between the 2 groups (SMD:0.653, 95% CI: .479-.826, P = .000). This shows that crossing the CTJ resulted in significantly longer mean operative time than not crossing the CTJ. 6) Mean length of stay- 2 studies (n = 441) were directly compared with respect to the mean length of stay for the CLV and TLV groups. SMD was significant between the 2 groups (SMD: .404, 95% CI:0.210-.599, P = .000). The data suggests that PCF with a TLV resulted in longer LOS compared to the CLV group (Figure 7). Fusion rate. Reoperation rate. Complication rate. Mean estimated blood loss. Mean operative time. Mean length of hospital stay.
Indirect Meta-Analysis
1) Fusion rate- 7 studies reported the fusion rate (n = 1088). There were 422 patients (38.8%) in TLV group and 666 patients (61.2%) in the CLV group. The rates of successful fusion were 90.0% and 86.9%, respectively. As seen from the forest plot SDC (Supplemental Appendix A4), fusion rates between the 2 groups were comparable (Effect Size (ES)TLV: .892, 95% CI: .840-.928 vs ESCLV:0.894, 95% CI:0.849-.926). 2) Reoperation rate- The rate of fusion was reported in 8 studies (n = 1162). Patients sample size of the TLV and CLV groups was 438 (37.7%) and 724 (62.3%), respectively. A total of 48 patients (10.96%) in TLV group underwent a reoperation. The reoperation rate in the CLV group was 13.12% (95 of 724). The 2 groups had similar overall reoperation rate (ESTLV:0.112, 95% CI:0.075-.164 vs ESCLV: .125, 95% CI: .071-.211). The details of the analysis are shown in the forest plot SDC (Supplemental Appendix A5).
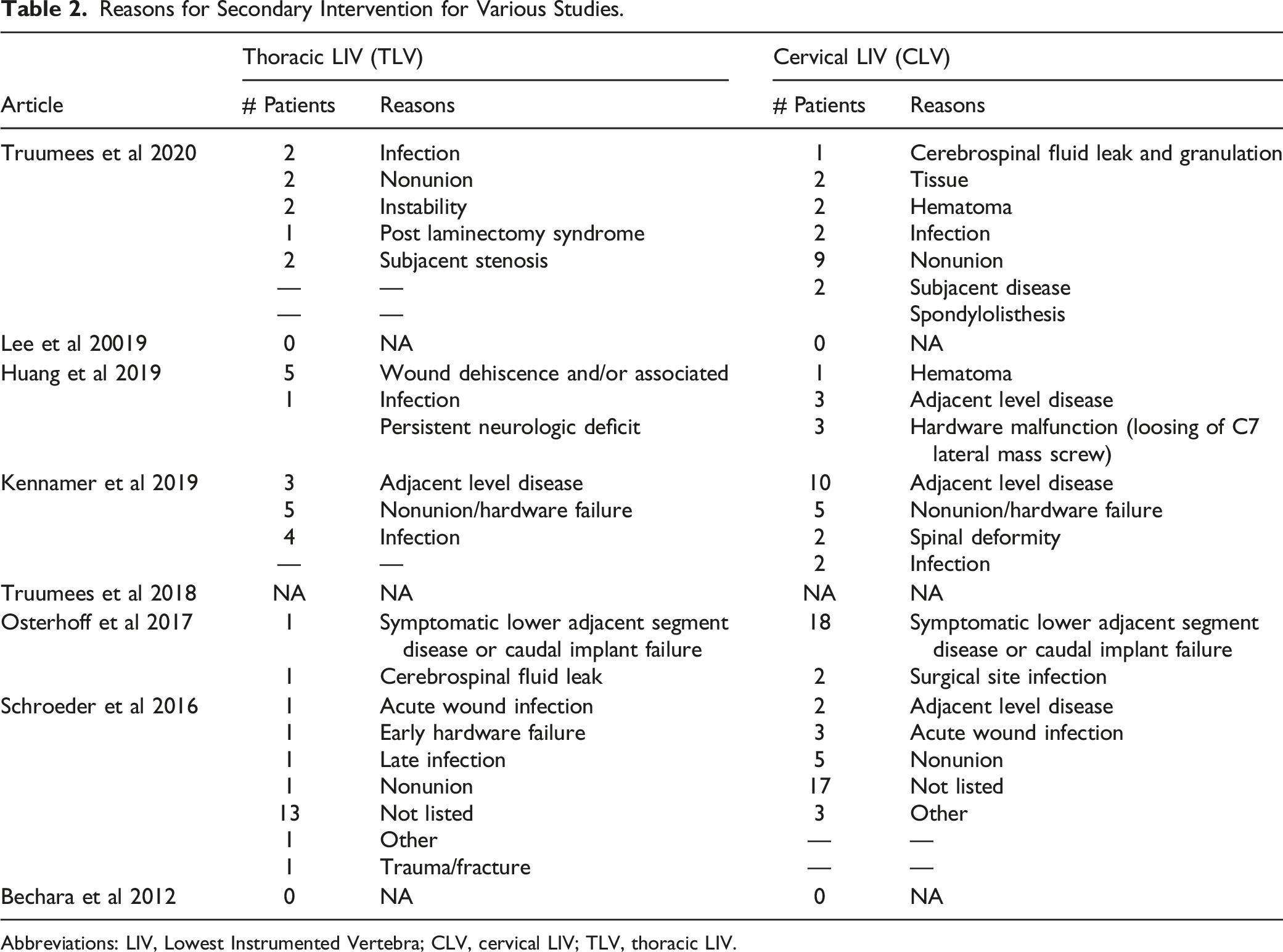
Table 2 summarizes the indications for secondary interventions from the various studies. For the TLV group; there were 13 cases of infection, 13 were not listed, 9 nonunion, and 5 cases of adjacent segment disease (ASD). In the CLV group, there were 42 cases of ASD, 17 not listed, 12 nonunion, and 9 cases of infection. 3) Complication rate- 7 studies consisting of 973 patients were evaluated for reported complication rates. The complication rates for the TLV vs CLV groups were 9.9% and 8.5%, respectively. SDC (Supplemental Appendix A6) forest plot shows the detailed analysis. As seen, complication rates between the 2 groups were similar (ESTLV: .108, 95% CI: .074-.154 vs ESCLV:0.081, 95% CI: .040-.156). Reasons for Secondary Intervention for Various Studies. Abbreviations: LIV, Lowest Instrumented Vertebra; CLV, cervical LIV; TLV, thoracic LIV.
Strength of Evidence
GRADE Assessment.
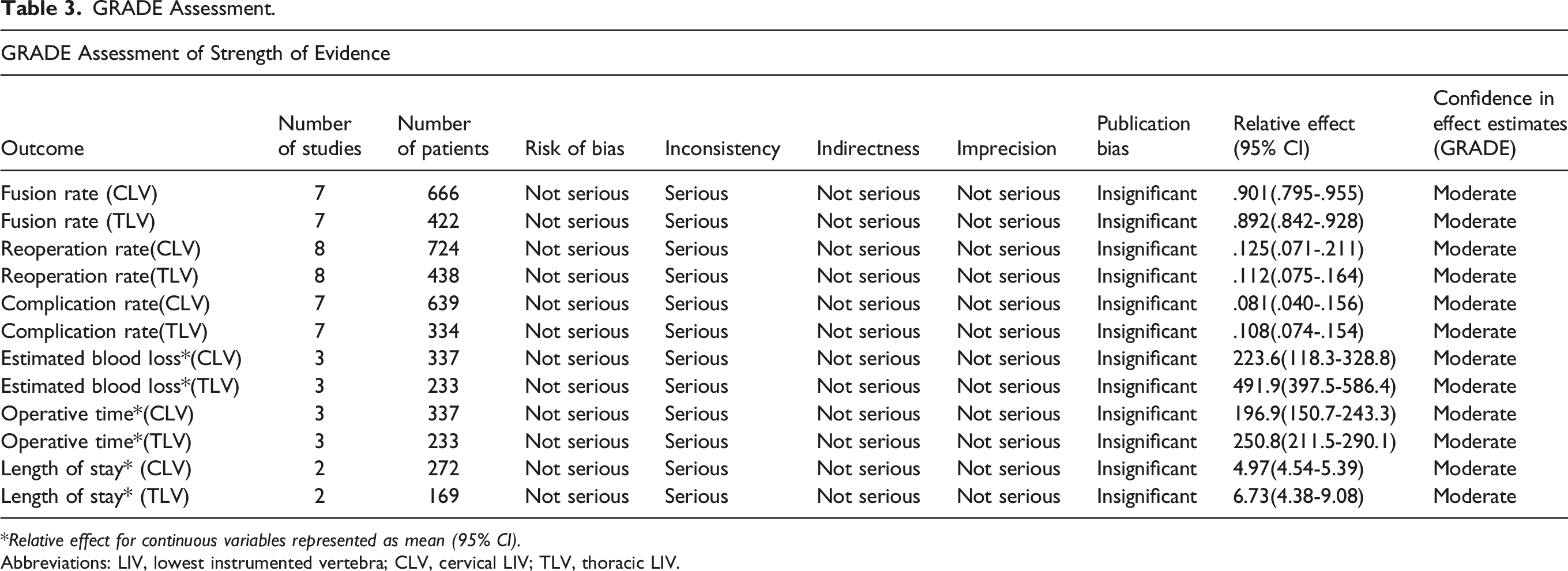
Relative effect for continuous variables represented as mean (95% CI).
Abbreviations: LIV, lowest instrumented vertebra; CLV, cervical LIV; TLV, thoracic LIV.
Quality of Studies
Quality Assessment.
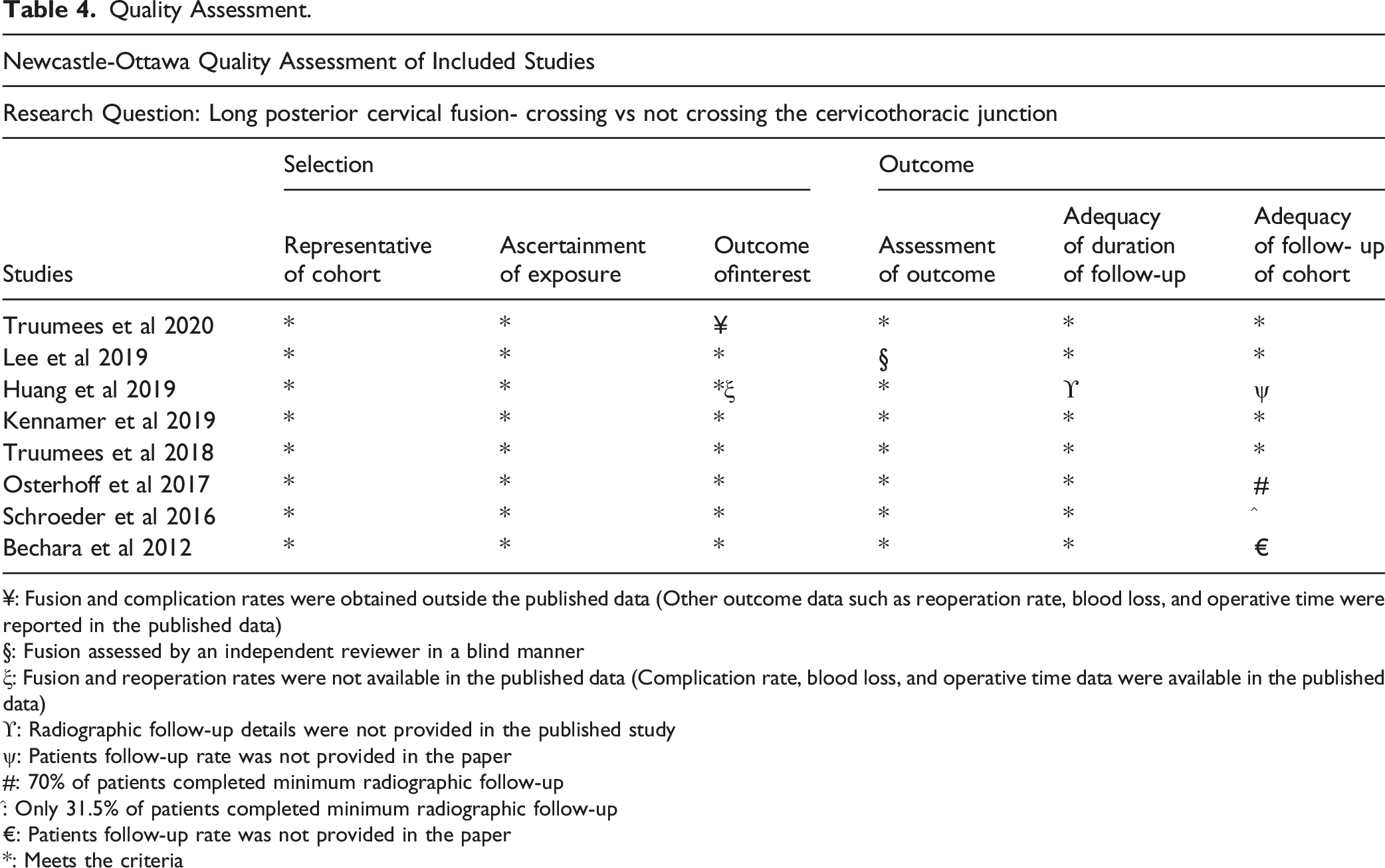
¥: Fusion and complication rates were obtained outside the published data (Other outcome data such as reoperation rate, blood loss, and operative time were reported in the published data)
§: Fusion assessed by an independent reviewer in a blind manner
ξ: Fusion and reoperation rates were not available in the published data (Complication rate, blood loss, and operative time data were available in the published data)
ϒ: Radiographic follow-up details were not provided in the published study
ψ: Patients follow-up rate was not provided in the paper
#: 70% of patients completed minimum radiographic follow-up
^: Only 31.5% of patients completed minimum radiographic follow-up
€: Patients follow-up rate was not provided in the paper
*: Meets the criteria
Publication Bias
The publication bias was assessed using the funnel plots. SDC (Supplemental Appendix A7-A10) show these details. As seen, there were no obvious asymmetry. This was further tested using egg and Mazumdar rank correlation and Egger’s regression intercept. Based on these analysis, we found that the publication bias was insignificant for all funnel plots (P > .05).
NNH Assessment
Based on the NNH calculation, we found that on average 18 and 21 patients would need to be treated with posterior cervical fusion ending at C7 in order for 1 patient to have subjacent degeneration or reoperation over the course of 2 years follow-up, respectively.
Discussion
Posterior cervical decompression and fusion surgery is commonly performed for patients with multi-level cervical spondylotic myelopathy. There is a lack of consensus when choosing a LIV in long (more than 4 segment) fusions. Concerns about early subjacent failure have led to the suggestion that these fusions be carried into the upper thoracic spine. Our group has previously performed 2 multicenter studies comparing outcomes of patients in which the fusion crossed the CTJ vs those in whom it did not.5,6 These studies reported similar clinical and radiographic outcomes among the 2 groups. The studies also showed lower EBL, OR, and LOS in patients in which the fusion did not cross the CTJ. Based on our research, we have concluded that it is reasonable to choose C6 or C7 as a caudal fusion level if good anchorage is achieved at the caudal level and in the absence of C7-T1 pathology.
In this meta-analysis, we analyzed our own patients’ data along with the data from several other studies. In line with our findings, some studies show drawbacks to crossing the CTJ. Huang et al concluded “crossing the CTJ was associated with increased surgical time, estimated blood loss, and the rates of wound dehiscence.” 14 Some of the differences in this study of 129 patients were dramatic. Mean EBL was over 350 mL greater in the TLV group. Lee et al found similar clinical and radiographic outcomes in TLV patients and those in which C7 was the caudal fusion end level. 4 Based on these findings, they determined that “multi-level PCF stopping at C7 does not negatively affect C7-T1 segment failure.” They concluded “it is unnecessary to extend the long PCF levels caudally across the healthy CTJ for fear of development of adjacent segment disease at the C7-T1 segment.”
Other studies, however, recommend crossing the CTJ. In a review of 74 patients with at least 6 months of follow-up, Osterhoff and colleagues found a higher rate of re-operation in a group of patients in which constructs terminated at C7 compared to their TLV group. 15 They concluded that, even in the absence of C7-T1 pathology, “one may consider bridging the cervicothoracic junction and to end the instrumentation at T1 or T2.” Schroeder et al also recommend extending multi-level cervical fusions to T1. They noted the odds of revision were 2.29 times greater when surgery stopped at C7 compared to operations that crossed the CTJ. 1
All of the studies mentioned, including our recent study of 264 patients, are significantly underpowered. A previous meta-analysis in 2019 from Goyal and others attempted to answer this question. They included 6, 2 1-arm and 4 comparative studies consisting of 530 patients. 16 We performed a power analysis and concluded that a sample size of over 700 patients would be required to detect a 2% difference in revision rates among our 2 groups at a power of .80. To enable stronger recommendations for surgical strategy in this context, we conducted this meta-analysis.
In this meta-analysis, we looked at several different outcomes in 1162 patients from 8 studies. Fusion rates between the 2 groups were comparable, and the mean fusion rate was 87.4%. The odds of fusion were not statistically different in crossing vs not crossing the CTJ. The incidence of reoperation was similar in both groups, and the odds of a postoperative complication were similar between the 2 groups.
The aggregate data suggests similar re-operation rates, but, perhaps, a lower subjacent degeneration rate in the TLV group. To study this further, we calculated a NNH. We found that about 20 patients would have to undergo posterior cervical fusion with a CLV in order for 1 patient to have require additional surgery for subjacent degeneration over the course of 2-year follow-up. This number would likely be substantially increased if, at the time of index surgery, those with significant degeneration, deformity, instability at C7-T1, or poor anchorage at C7 were offered surgery with a TLV. The small C7 lateral mass is often unsuitable as caudal end-level fixation. 17 In most cases, a C7 pedicle screw would be recommended, but this option may be ill-advised in patients of small, sclerotic or highly osteoporotic C7 pedicles. This setting, the larger T1 (and/or T2) pedicles offer safer, mechanically stronger end level fixation. In this setting, no separate C7 anchor is required.17
Utilizing a CLV for long posterior cervical fusions decreases morbidity, as measured by lower EBL and shorter operative times. CLV are also associated with shorter hospital LOS which has both health and cost advantages.
While we were unable to do a direct cost analysis, it would be reasonable to extrapolate decreased costs with CLV surgery given both the reduced length of stay and reduced implant utilization.
Limitations and Strengths
The major limitations of this study include its retrospective nature and heterogenous patient populations. Across the 8 studies, individual surgeons may have different indications for the various surgical techniques, including concomitant anterior surgery and LIV. There may also be differences in the 2 groups in terms of their baseline co-morbidities and spinal pathologies. Once critical variable was the percentage of patients who had anterior cervical fusions and the number of levels over which those fusions were carried. Most of those anterior fusions did not include the C6-7 and very few included the C7-T1 level. Truumees et al (2018 & 2020) studies showed that overall 17.2 % and 12.4% of the patients in TLV and CLV groups had both anterior/posterior fusions, respectively. These may have contributed to increased morbidity, as measured by higher EBL, longer operative times and hospital LOS in the TLV group. Another limitation of the analysis is variability in the fusion assessments of these studies which were measured at different time points. This limits some generalizability from the long-term follow-ups.
While the meta-analysis enabled us to include the largest number of patients reported, inconsistent reporting still resulted in some variables with lower patient numbers. Some of the studies did not report at all on certain variables such as length of stay and follow-ups. This resulted in an analysis of only 441 patients for length of stay.
Patient reported outcomes are not included in this study, which is another limitation. Inconsistent reporting across the 8 studies prevented our ability to analyze this measure. In the 2 studies in which PROMS were reported, no differences were seen between CLV and TLV constructs. There is also insufficient data in these studies to report on pre-operative and post-operative measures of alignment, such as the C2-C7 sagittal vertical axis. A growing body of literature suggests these parameters may influence post-operative outcomes. The available data utilized different measures of local and global spinal balance. Within those studies, no significant differences in alignment were noted with CLV and TLV constructs. Future research in this arena should include more vigorous reporting of patient reported outcome measures and sagittal balance measures.
Some of the strengths of our study include: 1) systematic review and meta-analysis using PRISMA guidelines; 2) greater sample size as compared to previous published study; 3) robust quality assessment using Newcastle–Ottawa Scale and GRADE guidelines; and 4) NNH assessment of our data.
Conclusions
Based on our current study, we have concluded that it is reasonable to choose C6 or C7 as the LIV if good anchorage can be achieved and in the absence of C7-T1 pathology. Utilizing a CLV for long posterior cervical fusions decreases morbidity, as measured by lower EBL and shorter operative times. CLV are also associated with shorter hospital LOS which has both health and cost advantages.
Supplemental Material
Supplemental Material - Bridging the Cervicothoracic Junction During Multi-Level Posterior Cervical Decompression and Fusion: A Systematic Review and Meta-Analysis
Supplemental Material for Bridging the Cervicothoracic Junction During Multi-Level Posterior Cervical Decompression and Fusion: A Systematic Review and Meta-Analysis by Eeric Truumees, MD, Devender Singh, PhD, Darlene Ennis, Heather Livingston, Ashley Duncan, RN, William Lavelle, MD, Ron Riesenburger, MD, Anthony Yu, MS, Matthew Geck, MD, Thomas Mroz, MD, and John Stokes, MD in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.