
Abstract
Study Design
Retrospective Cohort Study
Objectives
To determine if decreased preoperative symptom duration is associated with greater clinical improvement in function and myelopathic symptoms after posterior cervical decompression and fusion (PCDF).
Methods
All patients over age 18 who underwent primary PCDF for cervical myelopathy or myeloradiculopathy at a single institution between 2014 and 2020 were retrospectively identified. Patient demographics, surgical characteristics, duration of symptoms, and preoperative and postoperative patient reported outcomes measures (PROMs) including modified Japanese Orthopaedic Association (mJOA), Neck Disability Index (NDI), Visual Analogue Scale (VAS) Neck, VAS Arm, and SF-12 were collected. Univariate and multivariate analyses were performed to compare change in PROMs and minimum clinically important difference achievement (%MCID) between symptom duration groups (< 6 months, 6 months–2 years, > 2 years).
Results
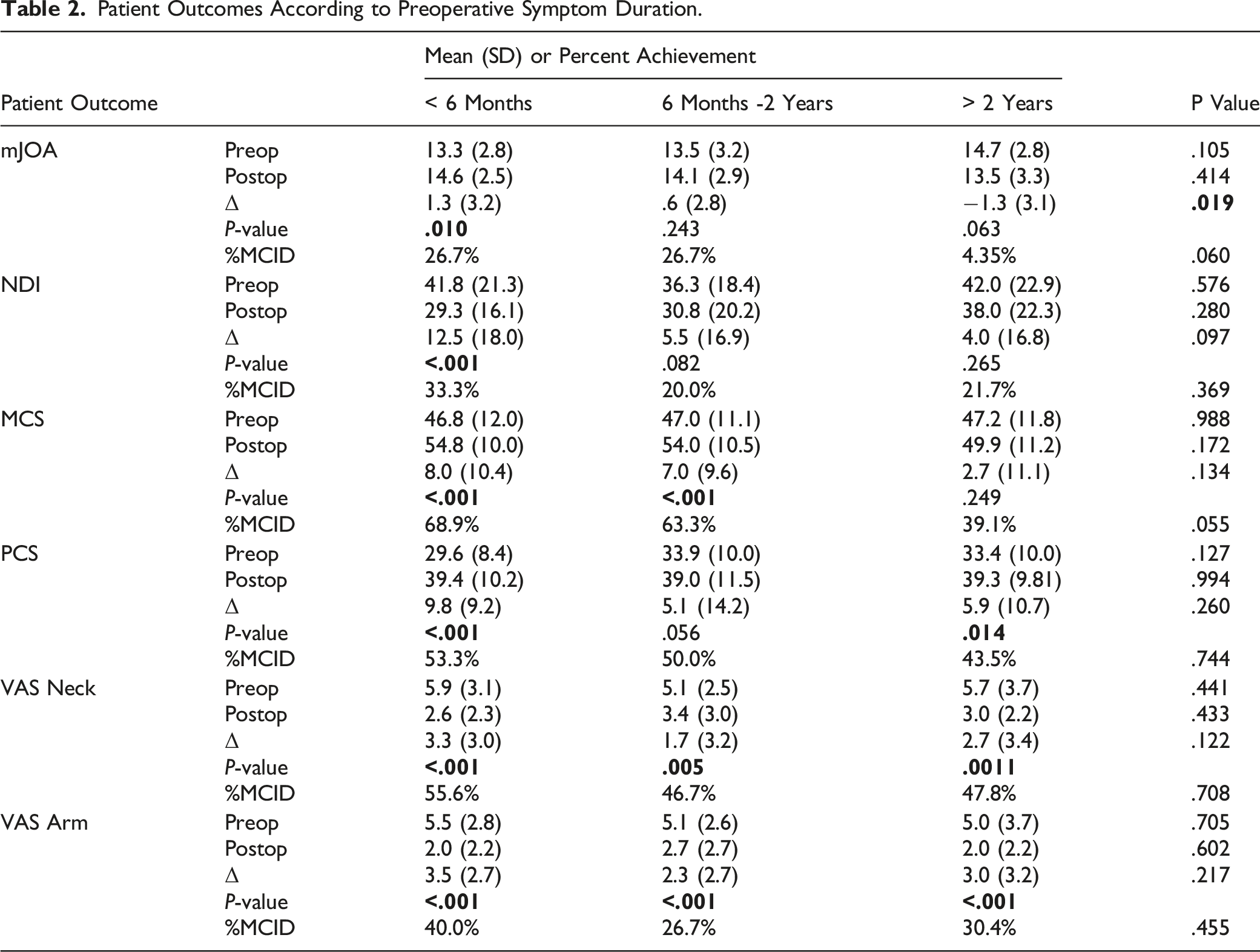
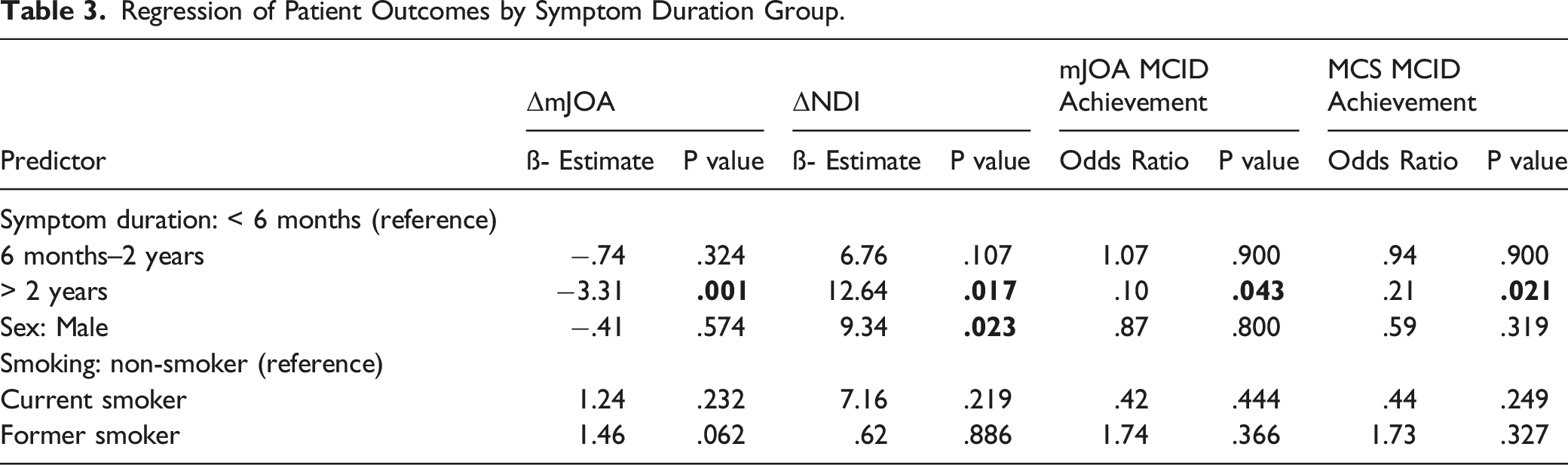
Preoperative symptom duration groups differed significantly by sex and smoking status. Patients with < 6 months of preoperative symptoms improved significantly in all PROMs. Patients with 6 months–2 years of preoperative symptoms did not improve significantly in mJOA, Physical Component Scores (PCS), or NDI. Patients with > 2 years of symptoms failed to demonstrate significant improvement in mJOA, NDI, or Mental Component Scores (MCS). Univariate analysis demonstrated significantly decreased improvement in mJOA with longer symptom durations. Increased preoperative symptom duration trended toward decreased %MCID for mJOA and MCS. Regression analysis demonstrated that preoperative symptom duration of > 2 years relative to < 6 months predicted decreased improvement in mJOA and NDI and decreased MCID achievement for mJOA and MCS.
Conclusion
Increased duration of preoperative symptoms (> 2 years) before undergoing PCDF was associated with decreased postoperative improvement in myelopathic symptoms.
Introduction
Degenerative cervical myelopathy represents the most common cause of spinal cord dysfunction in adults with annual hospitalization rates estimated at 4.04/100,000 person-years. 1 Cervical spondylotic myelopathy (CSM) arises due to degeneration of the intervertebral disc, facet joints, and ligamentous complexes resulting in spinal canal narrowing and symptoms of central compression which may occur concomitantly with radicular pain.1–3 Myelopathy is associated with progressive disability and reduced quality of life.1,2,4 Though the rate of symptomatic progression is often unpredictable, CSM is rarely responsive to non-operative modalities.1,2,5 Surgical decompression using a variety of surgical techniques is performed to arrest progression and potentially enable functional improvement. 6 Posterior cervical decompression and fusion (PCDF) is often performed in patients with multilevel disease involving the posterior elements and normal or neutral cervical alignment.7,8 Currently the preoperative factors associated with clinical outcome improvement after PCDF for patients with cervical myelopathy have yet to be fully elucidated.
The impact of preoperative myelopathic symptom duration on patient outcomes after PCDF remains unknown.4,9–21 In the literature, the effects of preoperative symptom duration on patient-reported outcomes measures (PROMs) are shown to vary by anatomic region, preoperative diagnosis, and operative intervention.4,12,15,22 In the lumbar spine, multicenter studies have demonstrated worse clinical outcomes for patients after lumbar discectomy and/or fusions when preoperative spinal stenosis, degenerative spondylolisthesis, or disc herniation symptom durations surpassed 6 months.11,13,16,22,23 Likewise, in the cervical spine, preoperative radiculopathy symptom durations more than 6 months adversely affected postoperative disability after anterior cervical discectomy and fusion (ACDF). 20 Furthermore, investigations of patients with CSM have identified increased symptom duration prior to ACDF and laminoplasty as a predictor of decreased improvement in myelopathic symptoms.4,18,19 However, there is a dearth of clinical evidence evaluating the effects of symptom duration on clinical outcomes after PCDF for myelopathy (with or without radiculopathy) to help define the optimal timing for surgical intervention. The purpose of this study is to determine if decreased preoperative symptom duration is associated with greater improvement in patient function and myelopathic symptoms after PCDF.
Methods
After approval from the Institutional Review Board (Control #19D.508), a retrospective cohort study was conducted on all patients over age 18 who underwent primary PCDF for cervical spondylosis associated with myelopathy or myeloradiculopathy at a single academic institution between 2014 and 2020 were retrospectively identified. Our study was deemed exempt from needing informed consent by the Institutional Review Board. Additional inclusion criteria required complete patient demographic profiles, surgical characteristics, preoperative symptom duration, and preoperative and postoperative PROMs with minimum one-year follow-up. Patients with a traumatic injury, infection, malignancy, revision, or combined anterior/posterior procedures were excluded. Patients were also excluded if their medical records or outcome measures were incomplete.
Patient demographic and medical data including age, sex, smoking status (never, former, current), body mass index (BMI), Charlson Comorbidity Index (CCI), diabetic status, depression and/or anxiety history, and duration of follow-up were recorded via chart review. Surgical factors including number of levels fused and estimated blood loss (EBL) were recorded. Duration of symptoms was extracted from the preoperative clinical visit note in the electronic medical record (EMR) or from patient questionnaires through the institution’s recording software (OBERD, Columbia, MO). Preoperative and postoperative health-related quality of life outcomes included the modified Japanese Orthopaedic Association (mJOA), Neck Disability Index (NDI), Visual Analogue Scale (VAS) Neck pain, VAS Arm pain, and Short Form-12 (SF-12) with embedded Physical and Mental Component Scores (PCS and MCS). Outcome scores at greater than one-year follow-up were obtained from the institution’s recording software or by phone call. Individual patient delta (Δ) scores were calculated by subtracting their preoperative score from postoperative score for each respective outcome measure. Achievement of the minimum clinically important difference (MCID) was determined according to established values for the PROMs studied: PCS-12: 8.1 points, MCS-12: 4.7 points, NDI: 17.3% points, VAS Neck: 2.6 points, and VAS Arm: 4.1 points, mJOA: 2.71 points.24,25
Statistical Methods
Patients were divided into groups based on previously established cut-offs for preoperative symptom duration (< 6 months, 6 months – 2 years, > 2 years).12,15,17,19,20,23 Descriptive statistics were used to compare patient demographics and outcomes in terms of mean and standard deviation or number of occurrences and percent of total. Continuous and categorical variables were analyzed with t-tests and chi-square tests or the corresponding non-parametric tests, respectively. Paired univariate analysis tested for significant preoperative to postoperative changes in PROMs within each group. Multivariate linear and logistic regression models were developed to isolate the effect of preoperative symptom duration on ΔPROMs and PROM MCID achievement at one-year follow-up. All statistical analysis was performed with R Studio Version 4.0.2 (Boston, MA). A P-value < .05 was considered statistically significant.
Results
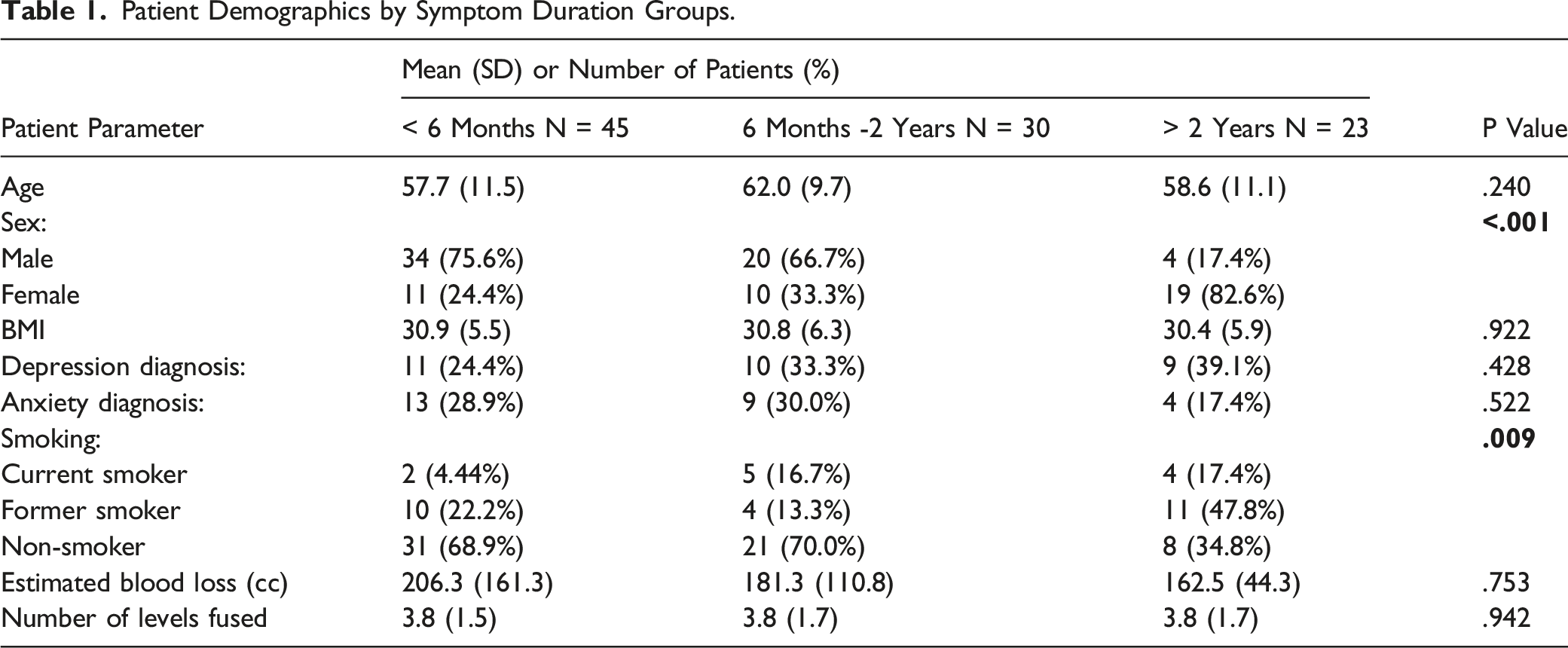
A total of 98 patients met the inclusion/exclusion criteria as detailed in Figure 1. The average follow-up time was 17.10 (7.46) months. The number of patients in each preoperative symptom duration cohort were as follows: < 6 months – 45 patients, 6 months to 2 years – 30 patients, > 2 years – 23 patients. Preoperative symptom duration groups differed significantly by sex (P = <.001), where a greater percent of females experienced symptoms for more than 2 years (female: 82.6% vs male: 17.4%). Smoking status also differed significantly between groups (P = .009) where a greater proportion of those in the 6 months to 2 years and > 2 years groups were current smokers (Table 1). Patient age, BMI, depression and anxiety history, number of fusion levels, EBL, and follow-up duration did not significantly differ between symptom duration groups (Table 1). Patient inclusion/exclusion criteria diagram. Patient Demographics by Symptom Duration Groups.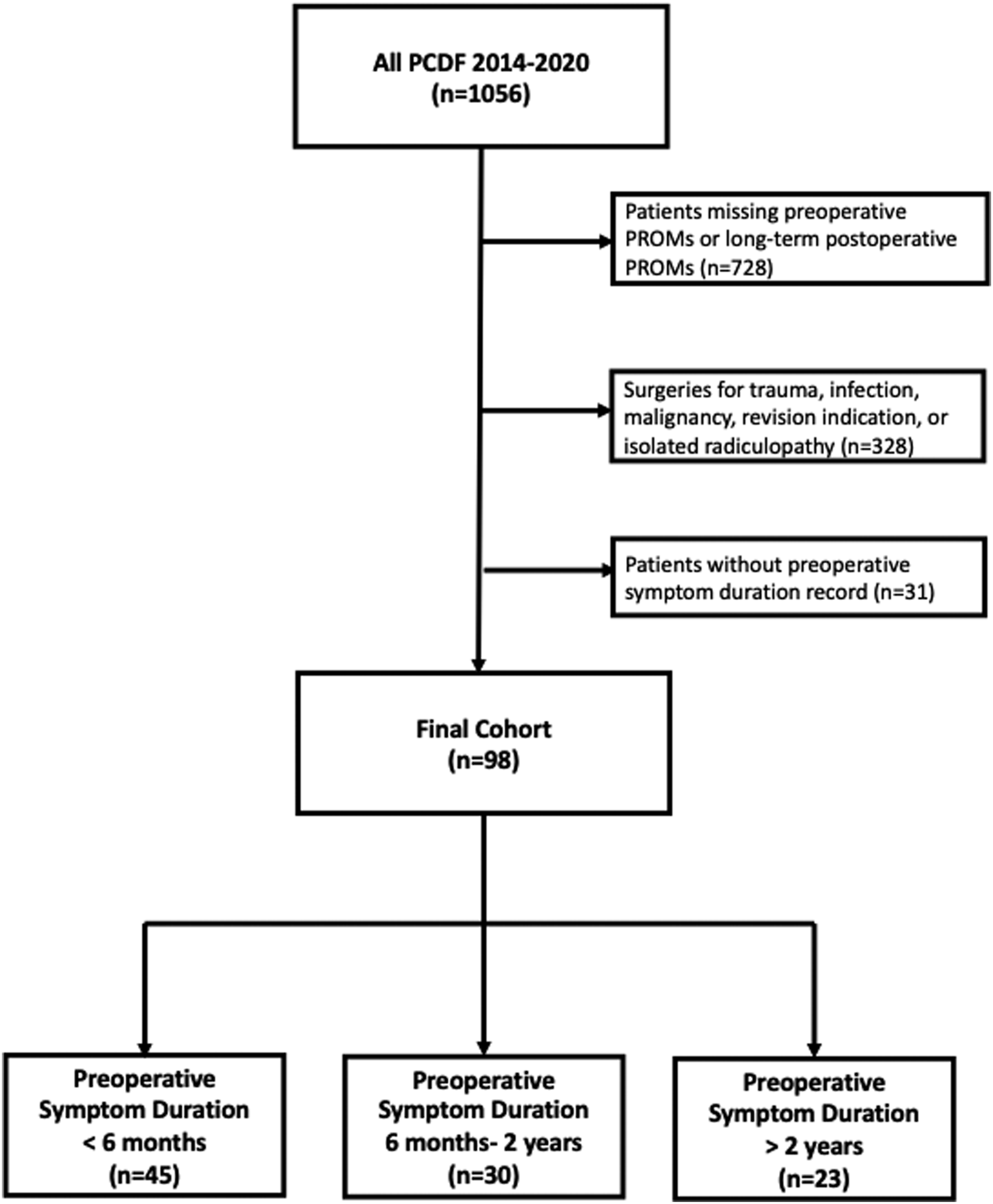
Patient Outcomes According to Preoperative Symptom Duration.
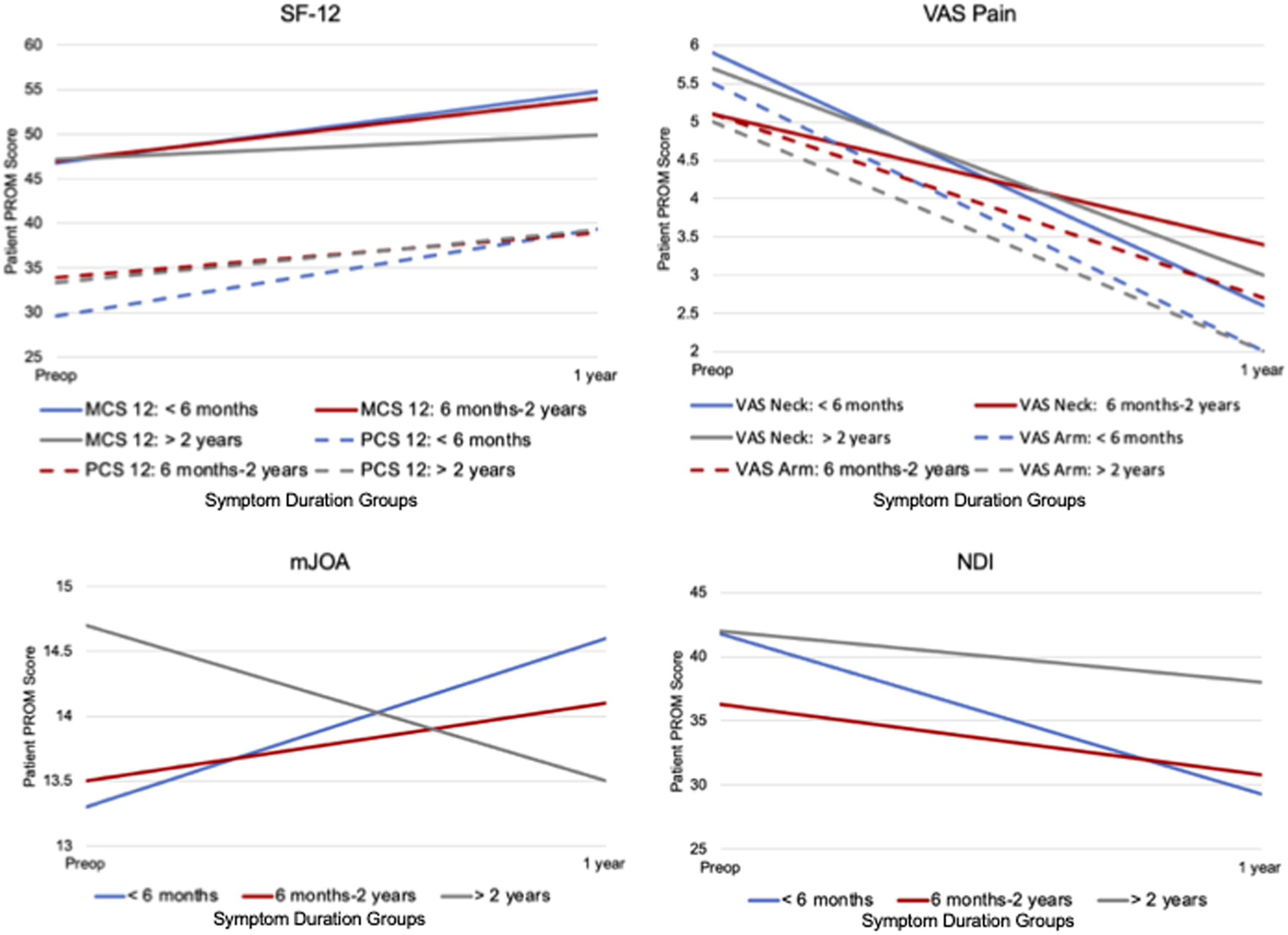
Patient outcome trajectory by symptom duration.
Univariate analysis demonstrated significantly decreased improvement in mJOA (P = .019) with longer symptom durations (Table 2). No significant differences in ΔNDI, ΔPCS, ΔMCS, ΔVAS Neck, ΔVAS Arm were demonstrated across symptom duration groups. However, ΔNDI (P = .097) trended toward statistical significance where decreased NDI improvement was evident with longer symptom durations. The proportion of patients meeting the MCID did not differ meaningfully across groups for any of the PROMs studied (Table 2). Increased preoperative symptom duration was associated with a trend toward decreased %MCID for mJOA (P = .060) and MCS (P = .055).
Regression of Patient Outcomes by Symptom Duration Group.
Discussion
It is estimated that the number of PCDF surgeries in the United States will increase by 19.3% between 2020 and 2040, with the largest increases seen in patients 75 to 84 years of age. 26 Myelopathy represents one of the most common and debilitating cervical conditions requiring surgery. However, no prior study has investigated the duration of preoperative CSM symptoms and patient outcomes after PCDF. Our study suggests that prolonged CSM symptoms of greater than 2 years may result in worse clinical outcomes after PCDF. While patients undergoing PCDF with over 2 years of preoperative symptoms may demonstrate improvements in pain relief, they experience less improvement in physical function parameters. These findings help optimize the timing for surgical intervention and set patient expectations regarding postoperative outcomes.
The overall incidence of CSM has been reported higher in males, which was reflected in our combined cohort’s demographics. 27 However, when stratified by preoperative symptom duration, patients with prolonged symptoms were disproportionately female and/or current smokers. The reasons behind this are unclear, yet females have been shown to have a higher rate of discharge to post-acute care facilities after PCDF which has been associated with a greater likelihood of adverse events postoperatively. 28 Likewise, preoperative smoking has also been associated with adverse outcomes after PCDF, namely, poor wound healing and pseudoarthrosis. 29 Our findings demonstrating higher prevalence of prolonged myelopathic symptoms in females and current smokers highlight a patient population who may benefit from closer attention and expedited care from providers to minimize debilitation.
In our analysis, mJOA scores demonstrated significant improvement in patients with less than 6 months of symptoms and a trend toward worse mJOA scores in those with greater than 2 years of symptoms. Additionally, the presence of symptoms over 2 years preoperatively was associated with a worse mJOA score and decreased likelihood of MCID achievement suggesting that patients with less than 6 months of symptoms may benefit from surgery from an objective functional standpoint. However, rates of CSM progression are patient-specific and difficult to predict, often based upon disease specific factors such ossification of posterior longitudinal ligament. 30 It has been suggested that patients undergoing posterior cervical decompression and/or anterior decompression and fusion had a 5–22% decreased probability of scoring at least 16 on mJOA (corresponding to mild myelopathic symptoms) at 1 year postoperatively if preoperative symptoms were present between three and 6 months, compared to less than 3 months.4,18,19 Likewise, a prospective investigation identified preoperative symptom duration of 4 months as the optimal cut-off for diminishing returns in mJOA improvement (.8) when including all surgeries for CSM. 31 Although prior studies failed to separate CSM patients undergoing PCDF from other cervical procedures, our study highlights further detriment in functional outcomes for symptoms lasting over 2 years in patients undergoing PCDF.
Patients with less than 6 months of symptoms were the only group demonstrating a statistically significant improvement in NDI. Male sex and preoperative symptom duration over 2 years were associated with a relative decrease in NDI improvement. It is unclear exactly why males were less likely to improve in neck disability; one explanation could be a greater proportion of manual labor occupations among males. 32 The NDI’s work and recreation domains have been shown to be significant predictors of PCS change after surgery for CSM, implying a psychological basis to how patients grade their physical function with greater weight placed on recreational and work capabilities vs objective measures used by clinicians. 33 CSM patients with shorter symptom durations may experience maximal disability improvement from PCDF surgery reinforcing the idea of a permanent time-limited functional decline in CSM.
The majority of patients with symptoms less than 2 years achieved clinically significant improvements in PCS and MCS postoperatively, however, there was no significant difference in the %MCID for these metrics when comparing across duration groups. The results suggest that physical function may improve even with prolonged symptom durations. On multivariate analyses, preoperative symptom duration over 2 years was associated with decreased odds of meeting MCS MCID, underscoring the predictive value of symptom duration for mental health status. Moreover, all groups demonstrated improvements in VAS Neck and VAS Arm pain scores with no significant differences in delta scores or %MCID, suggesting that PCDF in CSM patients may provide neck and arm pain relief regardless of symptom duration. It is possible that postoperative neck and arm pain reduction may represent pain relief from radiculopathy often co-occurring with myelopathy in the setting of cervical spondylosis, which has been found to improve in all patients regardless of radiculopathy duration.10,20,33,34
Our study is not without limitations. Although patients were included in a systematic method, potentially relevant cases were identified based on follow-up parameters, introducing a selection bias. Since patients with myelopathy and myeloradiculopathy were included, the individual contribution of radicular symptoms on pain and disability improvement are difficult to interpret. While the reasons for varying durations of preoperative symptoms are undetermined, the lack of difference in preoperative symptom severity between groups suggests that severity of presentation was unlikely to influence timing for surgical management. Furthermore, variations in the granularity of patient symptom duration in medical records did not allow for analysis of continuous timing parameters. Although symptom duration groups were selected according to literature time standards, the use of categorical analysis may impart bias and the symptom duration associated with for adverse PROM may occur before the selected time threshold. 15 Further prospective studies are required to better differentiate outcomes based on shorter time intervals. Finally, MCID thresholds in our study were selected based upon ACDF literature, as none exist for PCDF.
Conclusion
The results of our study suggest that prolonged and untreated symptoms of CSM greater than 2 years may result in worse clinical outcomes after PCDF. Patients undergoing PCDF greater than 2 years after the onset of symptoms may demonstrate improvements in pain relief, but experience significantly less improvement in disability and myelopathy disease-specific physical function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.