
Abstract
Study Design:
Single-center retrospective review.
Objectives:
The cervicothoracic junction (CTJ) is typically difficult to visualize using traditional radiographs. Whole-body stereoradiography (EOS) allows for imaging of the entire axial skeleton in a weightbearing position without parallax error and with lower radiation doses. In this study we sought to compare the visibility of the vertebra of the CTJ on lateral EOS images to that of conventional cervical lateral radiographs.
Methods:
Two fellowship-trained spine surgeons evaluated the images of 50 patients who had both lateral cervical radiographs and EOS images acquired within a 12-month period. The number of visible cortices of the vertebral bodies of C6-T2 were scored 0-4. Patient body mass index and the presence of spondylolisthesis >2 mm at each level was recorded. The incidence of insufficient visibility to detect spondylolisthesis at each level was also calculated for both modalities.
Results:
On average, there were more visible cortices with EOS versus XR at T1 and T2, whereas visible cortices were equal at C6 and C7. Patient body mass index was inversely correlated with cortical visibility on XR at T2 and on EOS at T1 and T2. There was a significant difference in the incidence of insufficient visibility to detect spondylolisthesis on EOS versus XR at C7-T1 and T1-2, but not at C6-7.
Conclusions:
EOS imaging is superior at imaging the vertebra of the CTJ. EOS imaging deserves further consideration as a diagnostic tool in the evaluation of patients with cervical deformity given its ability to produce high-quality images of the CTJ with less radiation exposure.
Introduction
The unique anatomy and biomechanical features of the cervicothoracic junction present challenges in the evaluation and surgical treatment of spinal pathology. Cervicothoracic alignment is increasingly understood as a driver of patient reported outcomes in adult spinal deformity surgery. 1,2 In cervical spondylotic myelopathy, the presence of spondylolisthesis at the C7-T1 junction has been shown to correlate with functional disability. 3 Despite its importance, the cervicothoracic spine is typically a difficult area to visualize using traditional radiographs. Swimmer’s and oblique radiographs have been described for this purpose but generally provide suboptimal visualization. 4,5 Computed tomography and magnetic resonance imaging are capable of generating high-quality images of the cervicothoracic junction, but are generally performed supine without physiologic loading and such imaging is subject to motion artifact.
Whole-body stereoradiography (EOS Imaging, Paris, France) allows for imaging of the entire axial skeleton in a weightbearing position without parallax error and with on average 5.6 times lower radiation doses compared with conventional cervical spine radiographs. 6,7 These advantages have led to its rapid adoption in the evaluation of pediatric and adult spinal deformity. EOS images of the entire spine can be obtained in as little as 4 seconds and are acquired simultaneously in the lateral and frontal planes. 8
EOS image quality has been shown to be superior to conventional radiographs for lateral spine imaging but can vary depending on the region of the body being imaged. 6,9 To our knowledge, no prior study has evaluated the relative visibility of the cervicothoracic junction using EOS. In this study, we sought to compare the visibility of the vertebra of the cervicothoracic junction on lateral EOS images to that of conventional lateral cervical radiographs. The relative ability of EOS and conventional cervical radiographs to detect spondylolisthesis as well as the influence of neck position in flexion/extension on vertebral body visibility were also studied.
Methods
A prospectively collected institutional database was used to identify patients who had both lateral cervical spine radiographs and EOS imaging within a 12-month time period. Patients with age less than 18 years or those who had interval cervical or thoracic spine surgery between studies were excluded. This study was approved by the institutional review board at the New York University School of Medicine. The lateral cervical radiograph and lateral EOS image with the patient in a neutral upright position were viewed side by side on the same monitor by 2 fellowship-trained spine surgeons. Using a modification of the methodology described by Horton et al, 10 scores ranging from 0 to 4 were assigned to the vertebral bodies of C6, C7, T1, and T2, according to the number of cortices visible (ie, anterior, posterior, superior, inferior). Patient body mass index (BMI) was also recorded. Given that EOS imaging included full length images of the spine, it was not possible to blind the raters to modality type during scoring. Cortical visibility scores were compared using a general estimating equation model. Linear regression analysis was used to evaluate for the effect of BMI on cortical visibility. Cohen’s kappa was used to judge interrater reliability.
An additional secondary analysis was performed to evaluate for any effect of neck position on vertebral visibility and to compare the relative ability of each modality to detect spondylolisthesis. To do so, an additional cohort of patients was identified within the database who met the aforementioned criteria but who also underwent both dynamic cervical radiographs and dynamic EOS imaging. Cortical visibility was then assessed in flexion and extension within each modality as described above. Comparisons were then made between modalities using multiple 2-way analyses of variance while controlling for neck position for all levels (C6 to T2). The incidence of spondylolisthesis (measuring ≥2 mm) on dynamic imaging was then calculated at the C6-7, C7-T1, and T1-T2 disc levels using each modality. When visibility of vertebral cortices was inadequate to determine presence or absence of a spondylolisthesis at a particular level, this fact was noted. From this data, the incidence of studies with insufficient visibility to detect listhesis was calculated within each modality. The incidence of insufficient visibility was then compared both for each disc level individually as well as for all cumulative levels using a chi-square test of independence.
Results
Fifty consecutive patients (21 males, 29 females) were identified meeting inclusion criteria for the analysis of neutral position imaging. The mean age of the patients was 56.7 years and the mean BMI of the cohort was 29.0 kg/m2. Vertebral body visibility was significantly better at T1 (2.8 ± 1.3 vs 2.3 ± 1.6, P = .03) and T2 (2.5 ± 1.4 vs 1.1 ± 1.6, P < .01) on EOS imaging as compared to conventional lateral radiographs (XR). Visibility of the C6 and C7 vertebral bodies on EOS imaging was equivalent to XR (Table 1). Vertebral body visibility was inversely correlated with BMI on EOS at both T1 and T2 vertebrae (r = −0.29, P = .04 and r = −0.33, P = .02, respectively). On XR, an inverse correlation with BMI was found only at the T2 vertebral body (r = −0.35, P = .01). Cohen’s kappa demonstrated moderate interrater agreement on cortical visibility for both modalities (XR, 0.44; EOS, 0.42).
Comparison of Cortical Visibility Score on Lateral Cervical Radiographs Versus Lateral EOS Images in Neutral Neck Position.
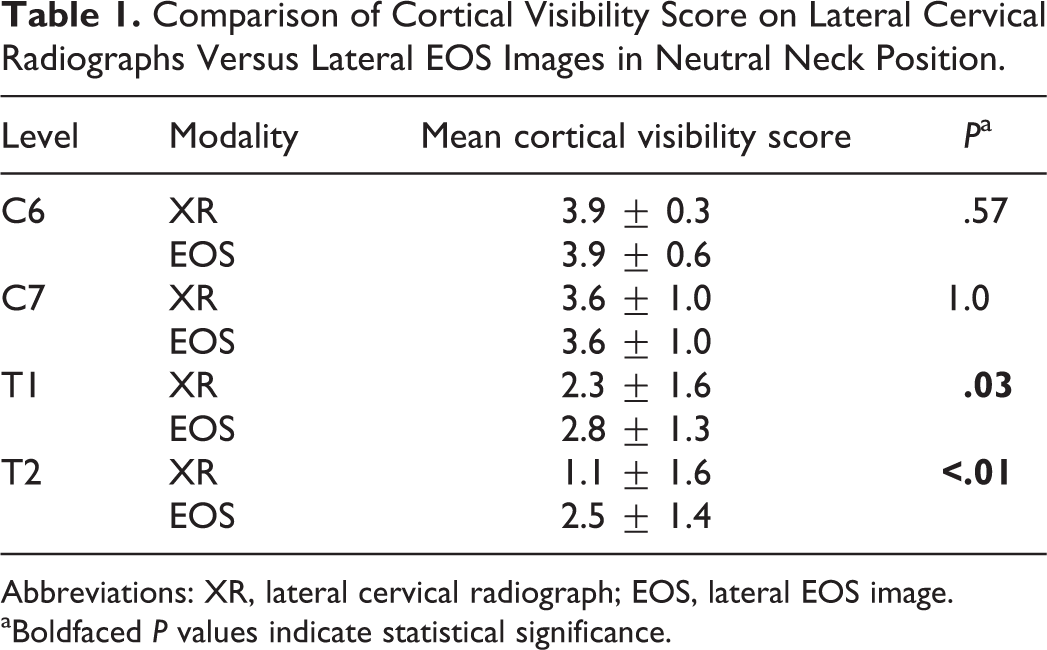
Abbreviations: XR, lateral cervical radiograph; EOS, lateral EOS image.
aBoldfaced P values indicate statistical significance.
Thirty patients (17 males, 13 females) were identified in the database who met inclusion criteria for the secondary analysis on dynamic EOS and XR imaging. All patients had flexion and extension images on file for both modalities. Images taken in flexion and extension again demonstrated superior visualization of the T1 and T2 vertebral bodies in both positions with minimal to no difference in visibility at C6 and C7 (Tables 2 and 3). The incidence of spondylolisthesis was low across all levels and did not demonstrate any statistically significant differences between modalities (Table 4). XR was more frequently insufficient to detect listhesis across all levels combined (C6-7, C7-T1, and T1-T2) than was EOS imaging (43.9% vs 32.8%, P = .02). On analysis of the individual levels, statistically significant differences in the ability to detect spondylolisthesis between modalities was found at C7-T1 and T1-2 but not at C6-7 (Table 4).
Comparison of Cortical Visibility Score on Lateral Cervical Radiographs Versus Lateral EOS Images in Neck Flexion.
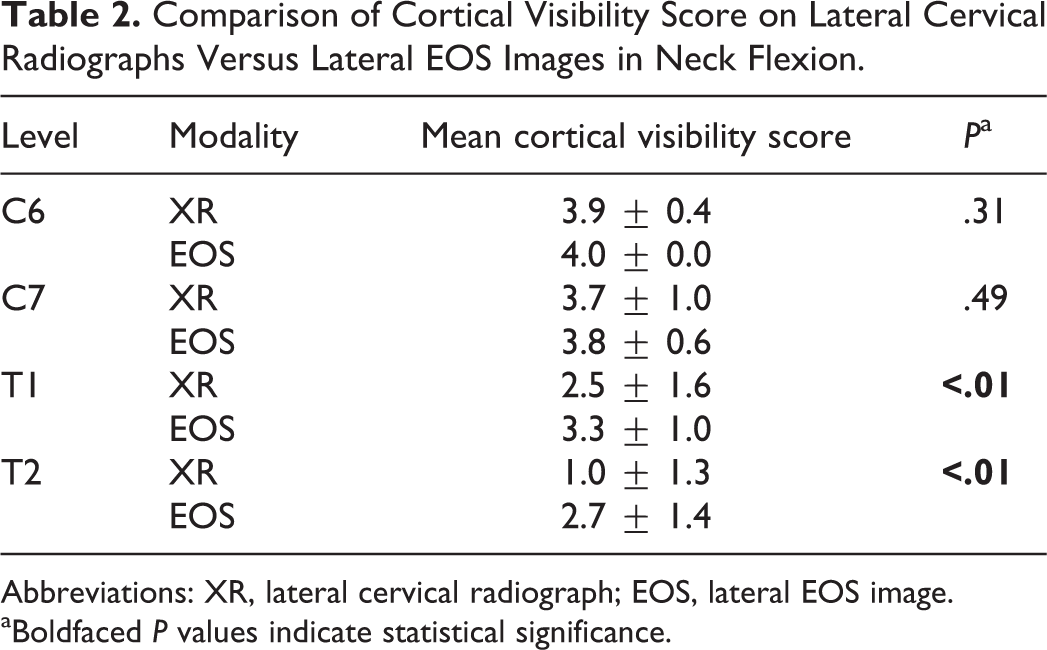
Abbreviations: XR, lateral cervical radiograph; EOS, lateral EOS image.
aBoldfaced P values indicate statistical significance.
Comparison of Cortical Visibility Score on Lateral Cervical Radiographs Versus Lateral EOS Images in Neck Extension.
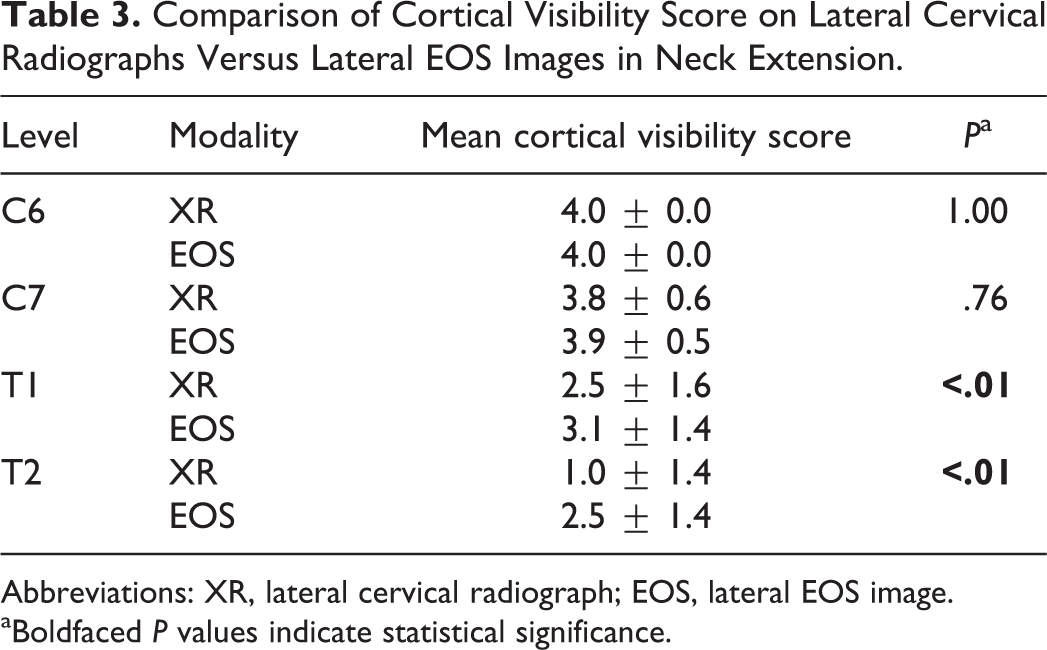
Abbreviations: XR, lateral cervical radiograph; EOS, lateral EOS image.
aBoldfaced P values indicate statistical significance.
Incidence of Insufficient Visibility to Detect Listhesis on Dynamic Imaging, XR Versus EOS Images.
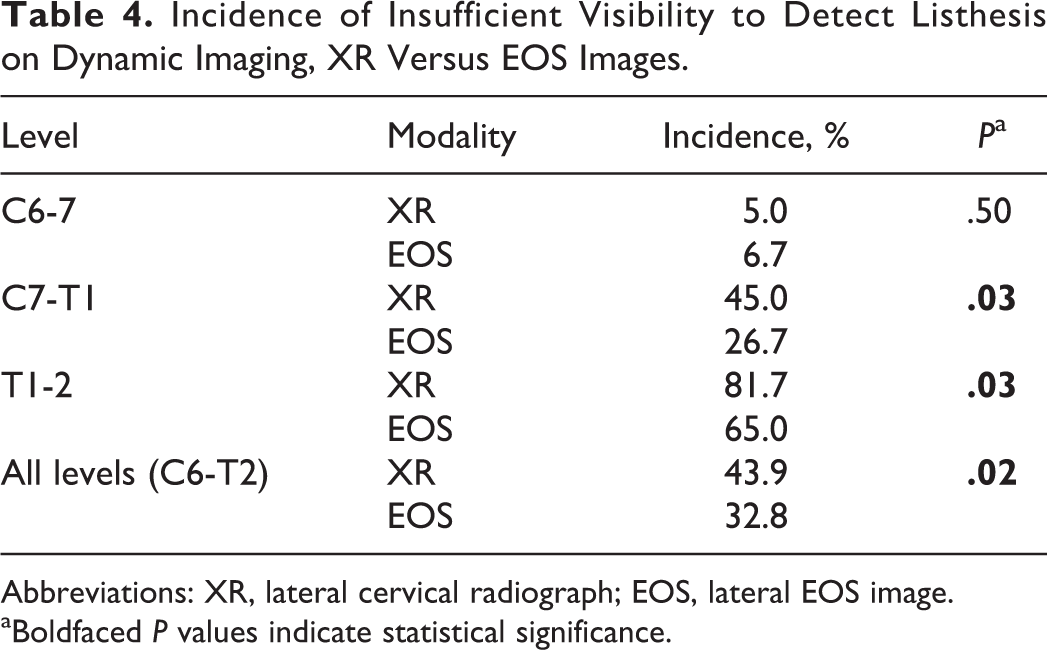
Abbreviations: XR, lateral cervical radiograph; EOS, lateral EOS image.
aBoldfaced P values indicate statistical significance.
Discussion
Whole spine stereoradiography utilizing the EOS imaging platform has become widely adopted at large medical centers with a focus on treating spinal deformity. While it has excellent utility for evaluating global spinal alignment, EOS stereoradiography may also have additional applications in the treatment of cervical pathology. A recent study demonstrated excellent interrater reliability in the measurement of cervical alignment parameters. The authors suggested that EOS imaging may serve as viable alternative to conventional radiographs as it is able to image the entire spine quickly with minimal radiation. 11
Upright imaging of the cervicothoracic spine is challenging using conventional techniques, primarily due to the adjacent bony and soft tissue structures of the shoulder girdle. Series in the literature suggest that a significant proportion of traumatic cervicothoracic injuries are diagnosed in a delayed fashion. 12,13 Modified techniques, included swimmer’s, oblique, and weighted arm views are sometimes utilized to improve visualization on traditional radiographs but have significant limitations. Swimmer’s view has been shown to be inadequate in as many as 45% of radiographs. 5 Both the swimmer’s and weighted arm views confound an accurate assessment of alignment as they are not performed in a natural standing position. Oblique views may visualize the cervicothoracic junction, but distort the evaluation of spinal segments as they are not true lateral images. Supine advanced imaging (such as computed tomography or magnetic resonance imaging) offers superior resolution of the cervicothoracic junction but is not performed in the standing position and thus does not offer information about upright alignment in the position of physiologic loading. These modalities also come with the disadvantages of increased cost and, in the case of computed tomography, significant radiation exposure.
This analysis demonstrates the enhanced ability of EOS stereoradiography to image the cervicothoracic junction in the upright position, specifically the vertebral bodies of T1 and T2 (Figure 1). Superior visualization of the T1 and T2 vertebrae was found in neutral, flexed, and extended neck positions, suggesting improved utility in dynamic analysis of cervicothoracic alignment (Figure 2). This study also shows that EOS images are more often adequate to detect spondylolisthesis at the cervicothoracic junction than on cervical lateral radiographs. This information is potentially valuable to surgeons planning instrumentation levels for posterior constructs. Surgeons may not wish to end a construct at the C7-T1 or T1-T2 levels in the presence of a spondylolisthesis as this may indicate susceptibility to adjacent segment disease and/or junctional failure.
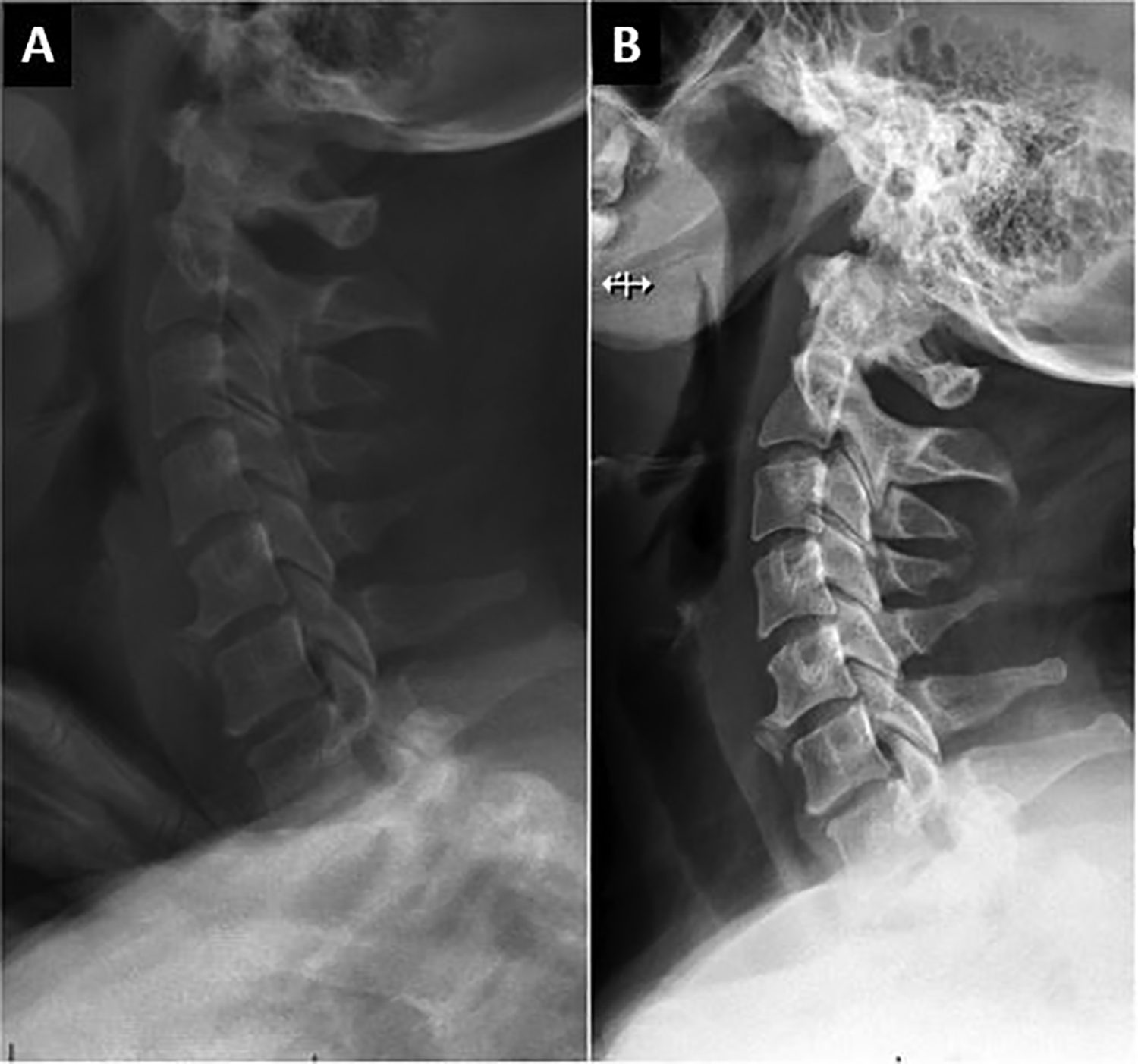
A study patient with static lateral EOS image (A) and lateral conventional radiograph (B).
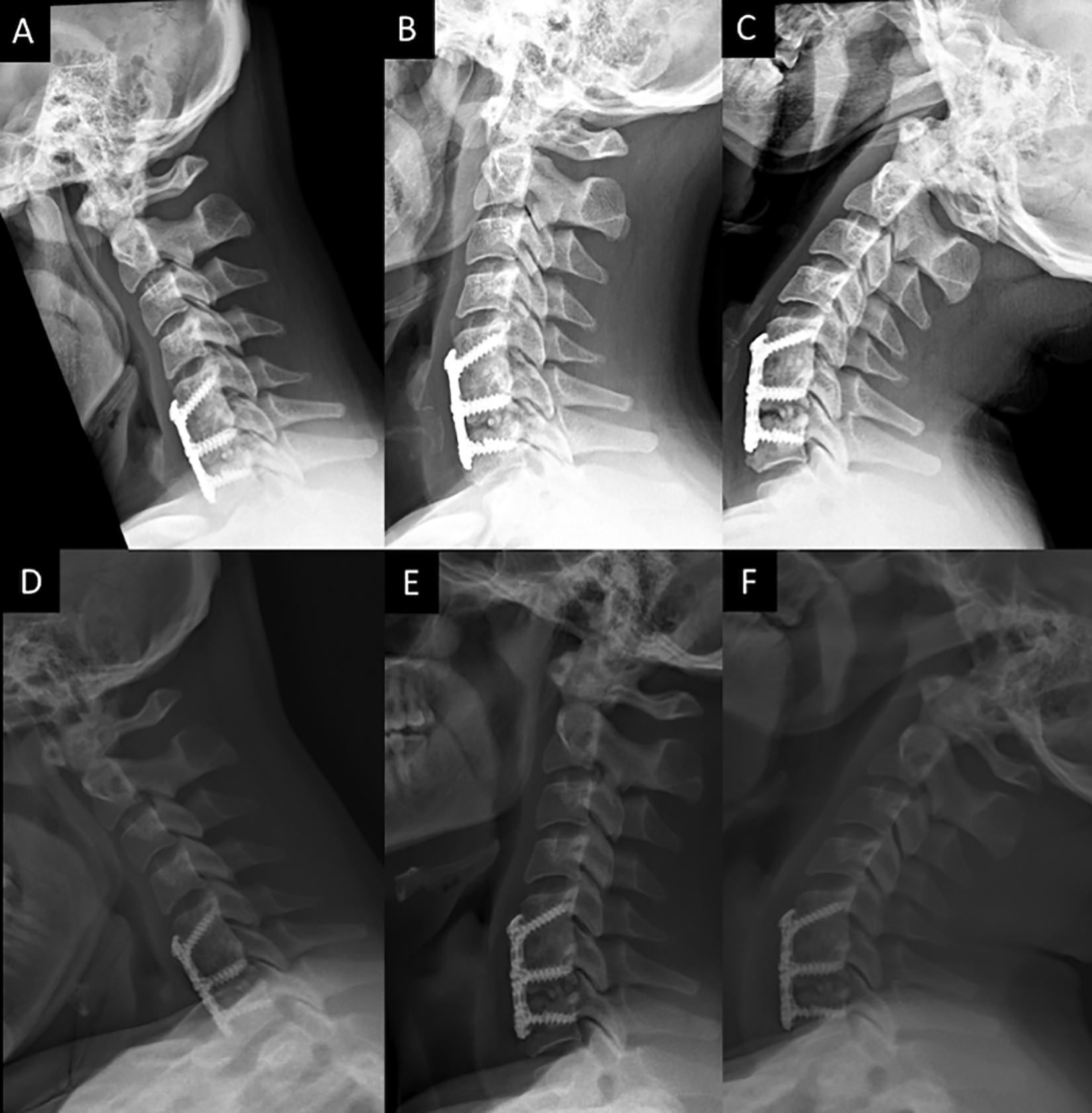
A study patient with a symptomatic pseudarthrosis at C6-7 and at C7-T1 spondylolisthesis on dynamic imaging. Lateral conventional radiographs in (A) flexion, (B) neutral, and (C) extension with lateral EOS images in (D) flexion, (E) neutral, and (F) extension.
This study is not without limitations. The overall incidence of spondylolisthesis is low in the study population making it difficult to design a study with enough power to definitely demonstrate an enhanced ability to detect spondylolisthesis using EOS. Based on our data, radiographs are often inadequate to show the C7-T1 (45%) and T1-T2 (82%) disc levels. This was much less common on EOS images (C7-T1 27%, T1-T2 65%) suggesting that in a large population, the ability to detect spondylolisthesis would be enhanced. The inability to control for arm position is another limitation of our analysis. At our institution, arm position is not standardized for lateral cervical radiographs. For EOS image acquisition, a finger-on-clavicle position is standard protocol but is sometimes modified if a patient is unable to maintain that position safely within the scanner. The authors consider it unlikely that this accounted for the observed differences in visibility as the bony structures of the proximal humerus and scapula remain immediately adjacent to the upper thoracic spine regardless of arm position. However, controlling for arm position should be incorporated into any future prospective studies comparing these modalities.
Conclusions
It is apparent from this analysis that EOS imaging is superior at imaging the vertebra of the cervicothoracic junction. This has significant implications for the preoperative evaluation of sagittal alignment at the cervicothoracic junction and may result in enhanced ability to detect spondylolisthesis in this region of the spine. This finding is important for spine surgeons evaluating patients with cervical and thoracic disorders and has the potential to influence planning of instrumentation levels. EOS imaging deserves further consideration as a diagnostic tool in the evaluation of patients with cervical spinal deformity given its ability to produce high quality images of the cervicothoracic junction with very low radiation exposure.
Footnotes
Authors’ Note
Part of this study were presented at the annual meeting of the North American Spine Society, Orlando, FL, October 25, 2017 and at the CSRS Annual Meeting, Hollywood, FL, November 3, 2017.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that there is no conflict of interest related to the submitted work. Outside the submitted work, one or more of the authors report consulting fees and IP royalties. The senior author, TSP, is a consultant for Globus, Stryker K2, Nuvasive, Medicrea and receives Royalties from Altus, none of which are directly related to this work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.