
Abstract
Study Design
A retrospective single-center study.
Objective
The present study investigated whether postoperative cervical alignment changes, in addition to preoperative patient backgrounds, imaging parameters, and disease severity, affect outcomes 1 year after laminoplasty.
Methods
One hundred and three cervical spondylotic myelopathy (CSM) patients who underwent laminoplasty were enrolled. Preoperative and postoperative (1-year) Japanese Orthopedic Association (JOA) scores, cervical alignment, and balance on X-rays were assessed. Patients were classified into 2 groups for a univariate analysis according to the status of the recovery rate (RR) of the JOA score ≥50%. A multiple logistic regression analysis was performed to identify factors associated with good surgical outcomes a.
Results
The mean RR of the JOA score was 47.5% and the loss of cervical lordosis in the neutral position was 5.5°. The univariate analysis revealed slight differences in age, sex, and the duration of disease. Preoperative C2-7 angles were not significantly different. The C2-7 angle during flexion after surgery was significantly smaller in Group F. In the multiple logistic regression analysis, significant factors associated with the status of RR≥50% were a younger age (OR: .75, 95%CI: .59–.96), shorter duration of disease (OR: .94, 95%CI: .89–.99), and a lordotic C2-7 angle during neck flexion after surgery (OR: 1.47, 95%CI: 1.1–1.95).
Conclusion
We retrospectively assessed the surgical outcomes of laminoplasty in 103 CSM cases. In addition to an older age and longer duration of disease, postoperative deteriorations in cervical kyphosis during neck flexion had a negative impact on outcomes.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) is a disease with many treatment opportunities in an aging society and affects the activities of daily living. It is an indication for surgery when symptoms progress, and outcomes are generally good, even in the elderly.1-4 Posterior cervical spine surgery, such as laminoplasty, has fewer perioperative complications than anterior cervical spine surgery. 5 The mid-to-long-term outcomes of posterior decompression surgery generally remain stable.6,7 Therefore, posterior decompression surgery, represented by laminoplasty, has widely been used in Japan in which acquired developmental spinal canal stenosis and elderly patients account for the majority of cases. 8 Age, duration of disease, and preoperative severity are well-known factors affecting surgical outcomes.2,3,9-11 Posterior surgery sacrifices the posterior muscles, lamina, and nuchal ligament, which alters the posterior support elements of the neck. Although cervical lordosis is generally maintained after laminoplasty, a few patients develop kyphotic deformities. The deterioration of cervical alignment and balance after laminoplasty has been shown to have a negative impact on surgical outcomes 12 ; however, few studies have included an evaluation of postoperative changes in cervical alignment.
Therefore, the present study investigated whether postoperative cervical alignment changes, in addition to preoperative patient backgrounds, imaging parameters, and disease severity, affect outcomes 1 year after surgery.
Patients and Method
Five hundred and fifty-five patients with cervical spine diseases underwent cervical spine surgery between October 2009 and July 2020 at our institution. All patients were retrospectively evaluated based on clinical findings, backgrounds, and radiological examinations. Patients with ossification of the posterior longitudinal ligament in the cervical spine, upper cervical diseases, a history of cervical spine surgery, cervical spondylotic radiculopathy, spinal tumors, and spinal cord injury were excluded. We also excluded patients who underwent anterior decompression and fusion and those lost to the follow-up less than 1 year after surgery. Therefore, we ultimately evaluated 103 patients with CSM in the present study (62 males, 41 females; mean age at the time of surgery: 72.7 years, range: 42–92 years). (Figure 1) All patients underwent MRI of the cervical spinal cord before surgery, and cervical laminoplasty was performed with or without short-segment instrumented fusion. The neurological severity of patients was assessed using the Japanese Orthopedic Association (JOA) score, which is specific for cervical myelopathy. The highest total JOA score without any deficits was 17 points. Inclusion criteria. ELAP; expansive (C3 to C7) laminoplasty, SLAP; selective laminoplasty.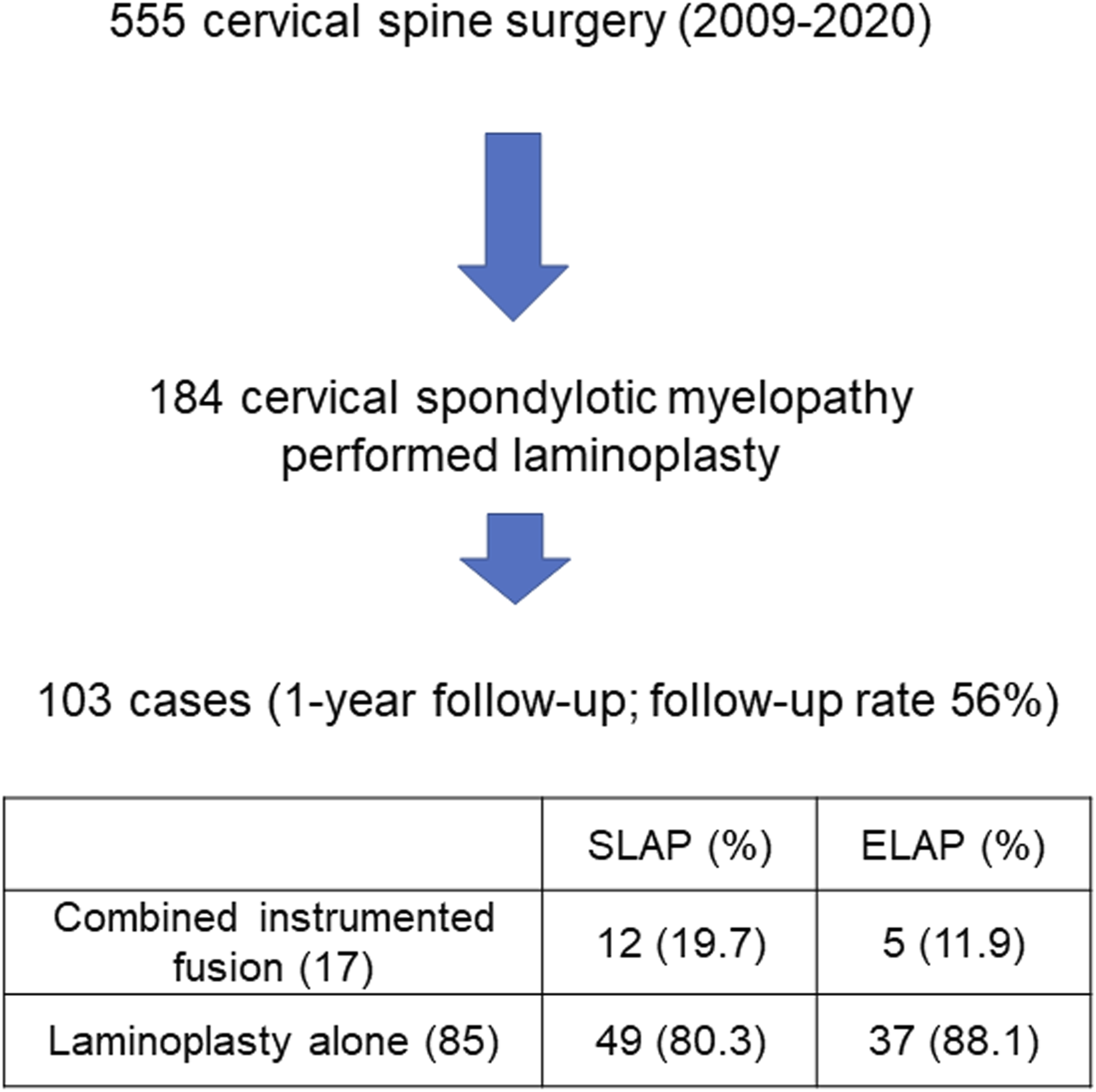
Written informed consent for imaging examinations was obtained from all patients with our institution’s approval. Patients who fulfilled the criteria outlined below were included in the present study. The diagnosis of myelopathy was based on 1) symptoms: numbness in the extremities, clumsy hands, and gait disturbances, 2) neurological examinations: increased deep tendon reflexes in the lower extremities and pathological reflexes, and 3) imaging findings: obvious spinal cord compression on MRI. A diagnosis was reached when symptoms, neurological findings, and imaging results were consistent. In the present study, double-door laminoplasty (the Kirita–Miyazaki method) was performed from C3 to C7 (expansive laminoplasty; ELAP), while 61 patients underwent selective laminoplasty (SLAP) at the affected level using intraoperative spinal cord evoked potentials. 14 Combined posterior instrumented fusion was selected based on the modified K-line, a straight line connecting the midpoints of the spinal cord at C2 and C7 on MRI. 15 Posterior instrumented fusion was additionally performed on 17 cases in which the distance between the modified K-line and anterior compression factor was <4 mm and the K-line was (-). The aim was not to correct the alignment, but to control local dynamic factors by in situ fixation.
The study design was approved by Yamaguchi University hospital’s Institutional Review Board (Control Number: H2020-025).
Evaluation
Information on age, sex, body mass index (BMI), the duration of disease at the time of surgery, presence of diabetes mellitus, history of smoking, pre- and 1-year postoperative JOA scores, the incidence of postoperative C5 nerve palsy and the recovery rate (RR) was collected from patient records. The method established by Hirabayashi et al. was used to calculate the RR of the JOA score. 16 Based on previous findings showing that the RR of the JOA score >50% satisfied the minimum clinically important difference, 17 RR ≥50% was classified as Group G and <50% as Group F.
Radiological Analysis
Plain X-rays
Plain lateral radiographs were taken in the neutral, flexion, and extension positions. The Cobb method was employed to measure the C2-7 angle and C2-7 range of motion (ROM). Positive and negative values were considered to indicate lordosis and kyphosis, respectively. The C2-7 sagittal vertical axis (SVA) (the horizontal distance between the posterosuperior corner of the C7 vertebra and the plumb line of the C2 vertebra) and C7 slope (the angle between the upper endplate of C7 and a horizontal reference line) were evaluated in the neutral position. (Figure 2) Measurement of the C2-7 sagittal vertical axis, C7 slope, and C2-7 angle.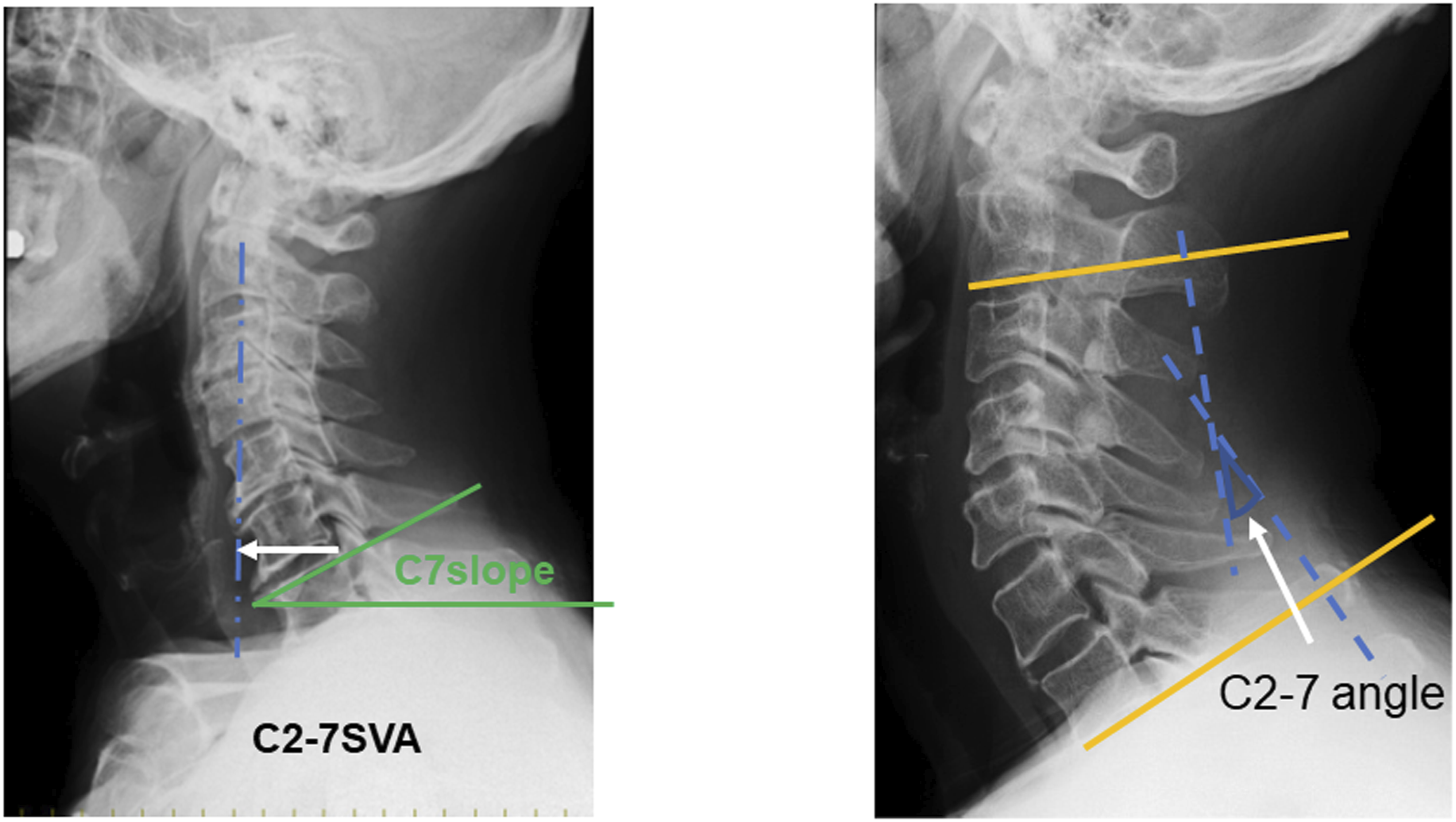
These radiological parameters were obtained before and 1-year after surgery. The loss of lordosis was calculated using the following formula: (preoperative C2-7 angle—postoperative C2-7 angle).
MRI
T1-and T2-weighted axial and sagittal images (slice thickness of 5 mm with an inter-slice interval of 2 mm) were acquired in the neutral position using a 1.5-tesla MRI scanner. The classification of spinal cord signal intensities on T2-weighted sagittal images was performed using a previously developed system (grade 0, none; grade 1, light; grade 2, intense). 18 T2-weighted images were examined to establish 1) whether a single or multiple high signal intensities were detected in the sagittal view and 2) if the snake eye appearance was present in the axial view. Evaluations were performed by 4 spine specialists.
Statistical Analysis
Summary values for numerical variables are shown as means ± SD, and those for categorical or ordinal variables as frequencies and percentages. The Mann–Whitney U test was used to examine between-group differences in values for numerical or ordinal variables, and the chi-squared or Fisher’s exact test for categorical variables using a 2 × 2 contingency table. In the univariate analysis, P < .05 indicated a significant difference. A univariate analysis was performed for the following comparisons: 1) outcome: Group G versus Group F, 2) surgical procedures: SLAP alone (n = 49), ELAP alone (n = 37), and laminoplasty combined with posterior instrumented fusion (n = 17), and 3) the deterioration of cervical lordosis: the postoperative loss of lordosis in a neutral position ≥10° versus <10°.
A multiple logistic regression analysis was performed using the stepwise parameter selection method (P < .1 was set as the criterion for inclusion in the regression model) to identify factors associated with the status of Group G and the postoperative loss of lordosis ≥10°. StatFlex 7.0 was used for all statistical analyses with P < .05 indicating a significant difference.
Results
Demographic Data.
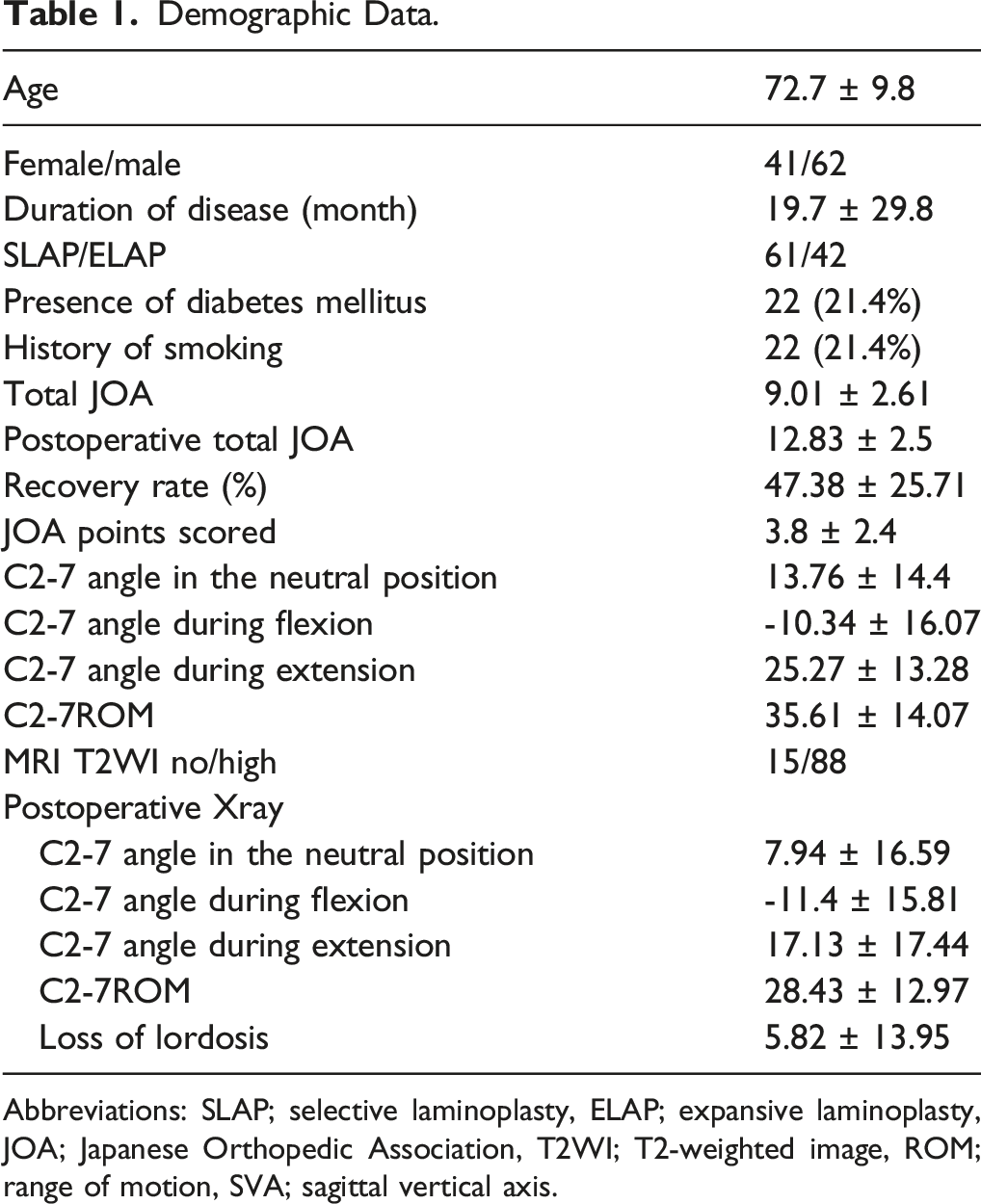
Abbreviations: SLAP; selective laminoplasty, ELAP; expansive laminoplasty, JOA; Japanese Orthopedic Association, T2WI; T2-weighted image, ROM; range of motion, SVA; sagittal vertical axis.
Univariate Analysis of Groups G and F
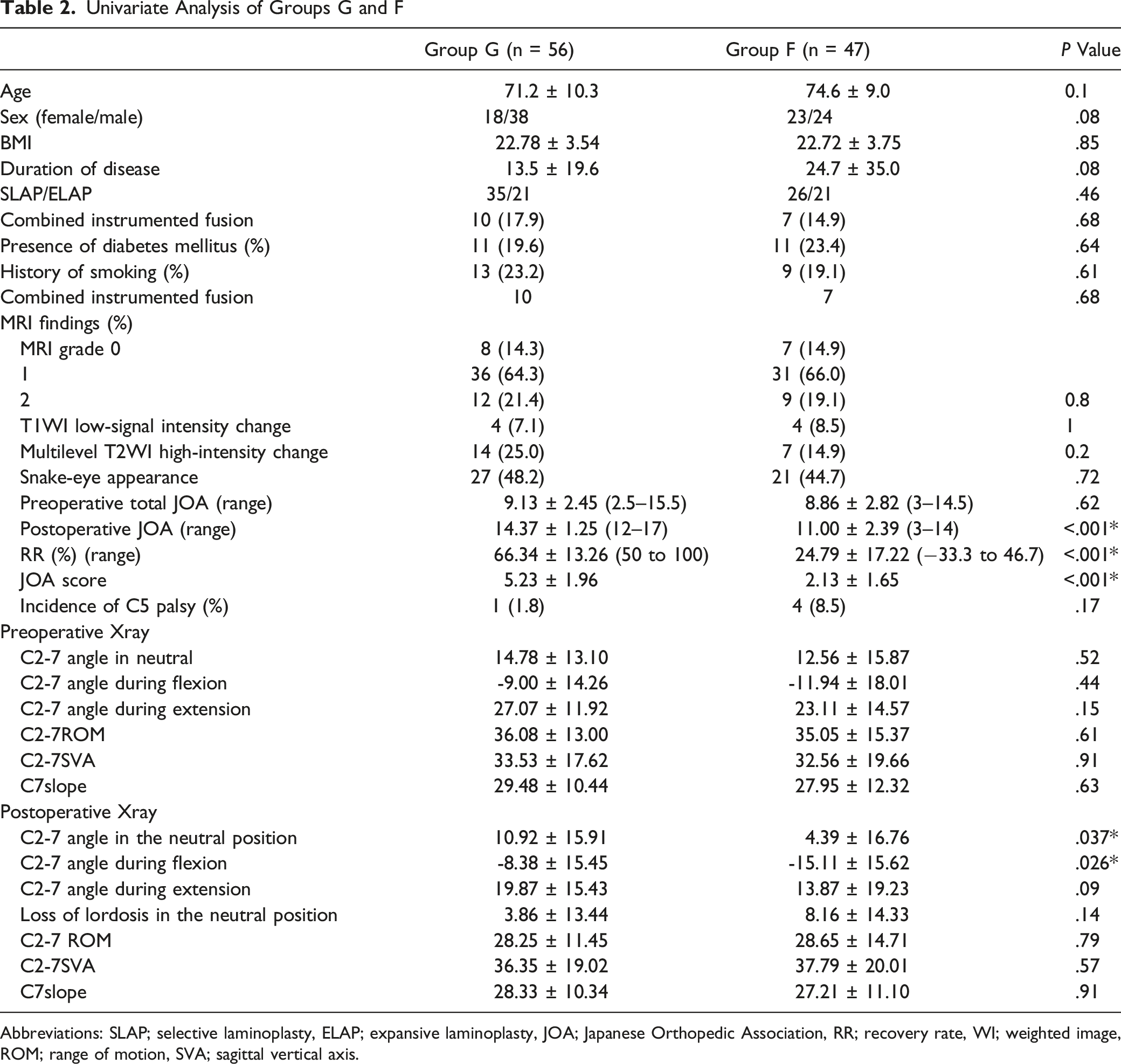
Abbreviations: SLAP; selective laminoplasty, ELAP; expansive laminoplasty, JOA; Japanese Orthopedic Association, RR; recovery rate, WI; weighted image, ROM; range of motion, SVA; sagittal vertical axis.
Comparison With Surgical Procedures
Demographic Data of the Type of Surgical Procedures.
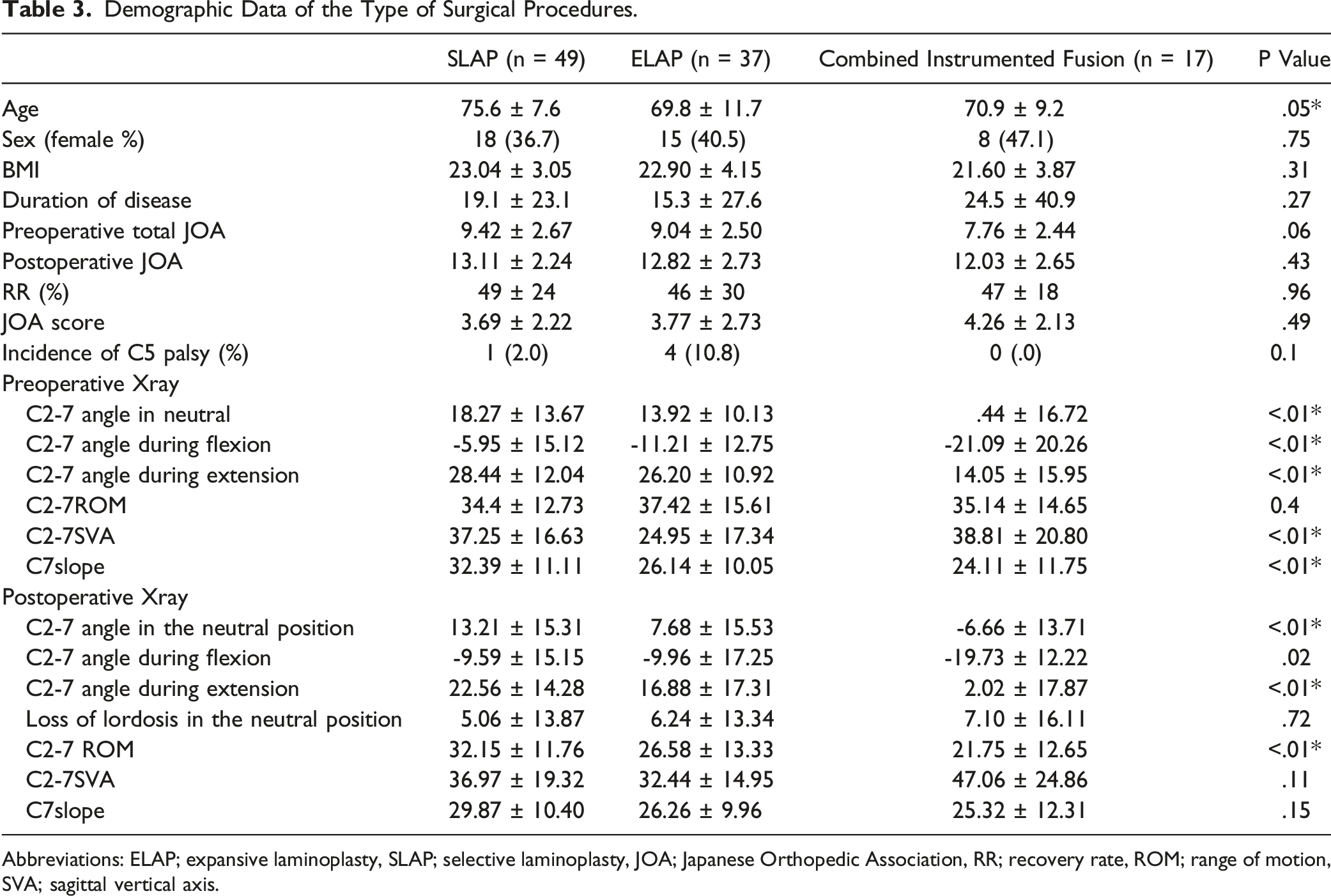
Abbreviations: ELAP; expansive laminoplasty, SLAP; selective laminoplasty, JOA; Japanese Orthopedic Association, RR; recovery rate, ROM; range of motion, SVA; sagittal vertical axis.
Univariate analysis of Groups G and F by the type of surgical procedures.
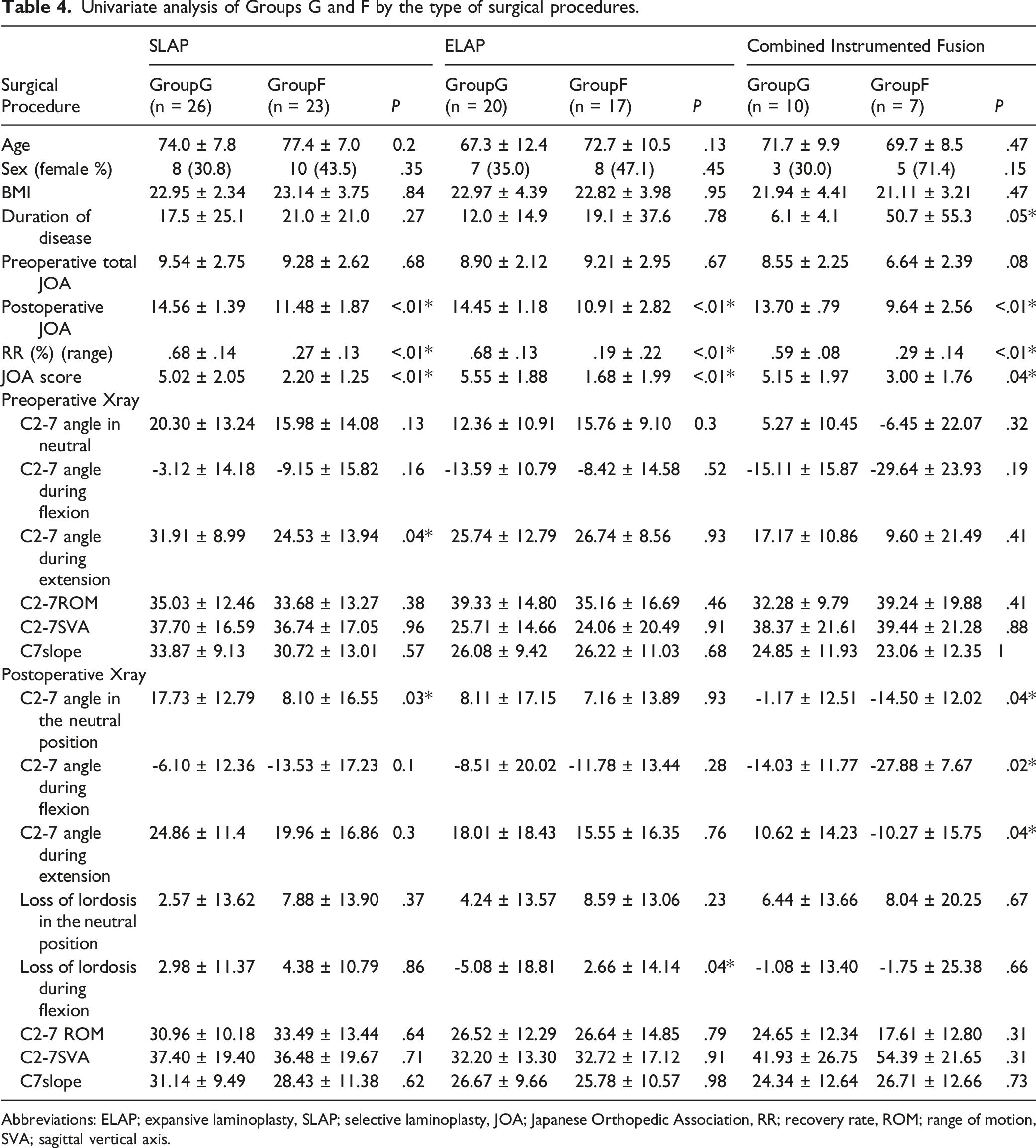
Abbreviations: ELAP; expansive laminoplasty, SLAP; selective laminoplasty, JOA; Japanese Orthopedic Association, RR; recovery rate, ROM; range of motion, SVA; sagittal vertical axis.
Postoperative Loss of Cervical Lordosis ≥10°
Univariate Analysis of Postoperative Loss of Lordosis≥10 and <10.
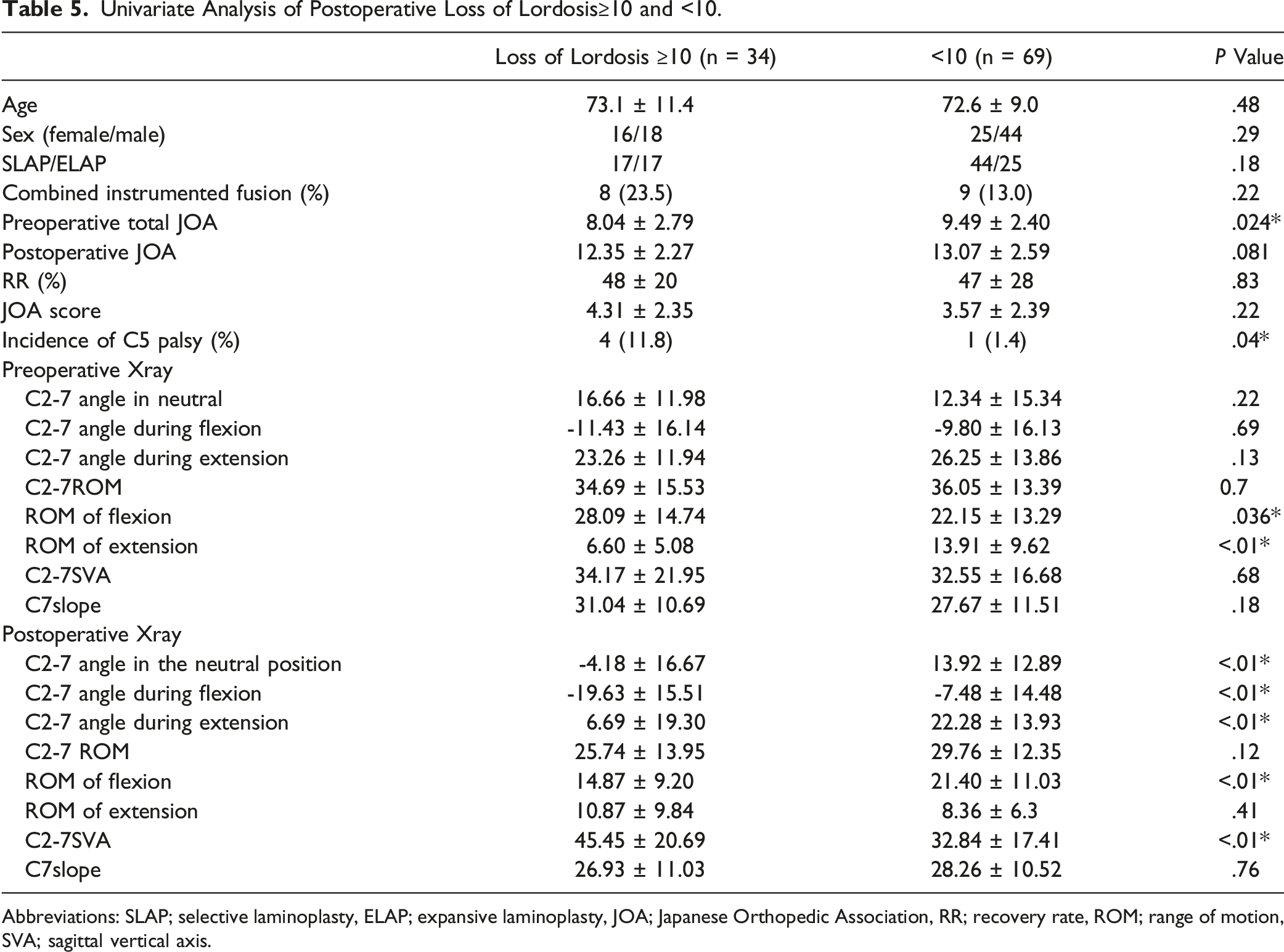
Abbreviations: SLAP; selective laminoplasty, ELAP; expansive laminoplasty, JOA; Japanese Orthopedic Association, RR; recovery rate, ROM; range of motion, SVA; sagittal vertical axis.
The Multiple Logistic Regression Analysis
Multivariate logistic analysis.
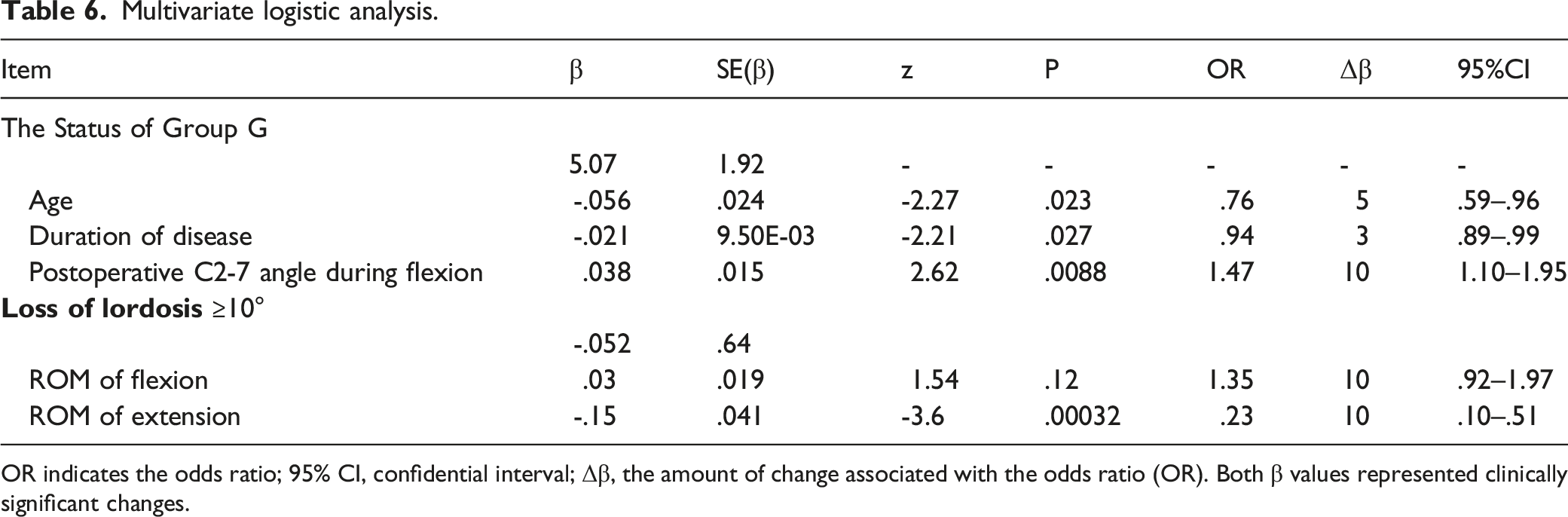
OR indicates the odds ratio; 95% CI, confidential interval; Δβ, the amount of change associated with the odds ratio (OR). Both β values represented clinically significant changes.
In an illustrative case of a 71-year-old woman with a preoperative C2-7 angle of 23°, (Figure 3) the C2-7ROM of extension and flexion were 10 and 34°, respectively. One year after surgery, RR was 31% and the postoperative C2-7 angle was kyphosis of 15°. A 70-year-old female patient underwent C3-4 selective laminoplasty. The duration of disease was 3 months and the preoperative JOA score was 7.5 points. However, the preoperative C2-7 lordotic angle in the neutral position was 23 degrees and the postoperative C2-7 kyphotic angle was 15 degrees. The postoperative JOA score was 10.5 points and the recovery rate was 31%.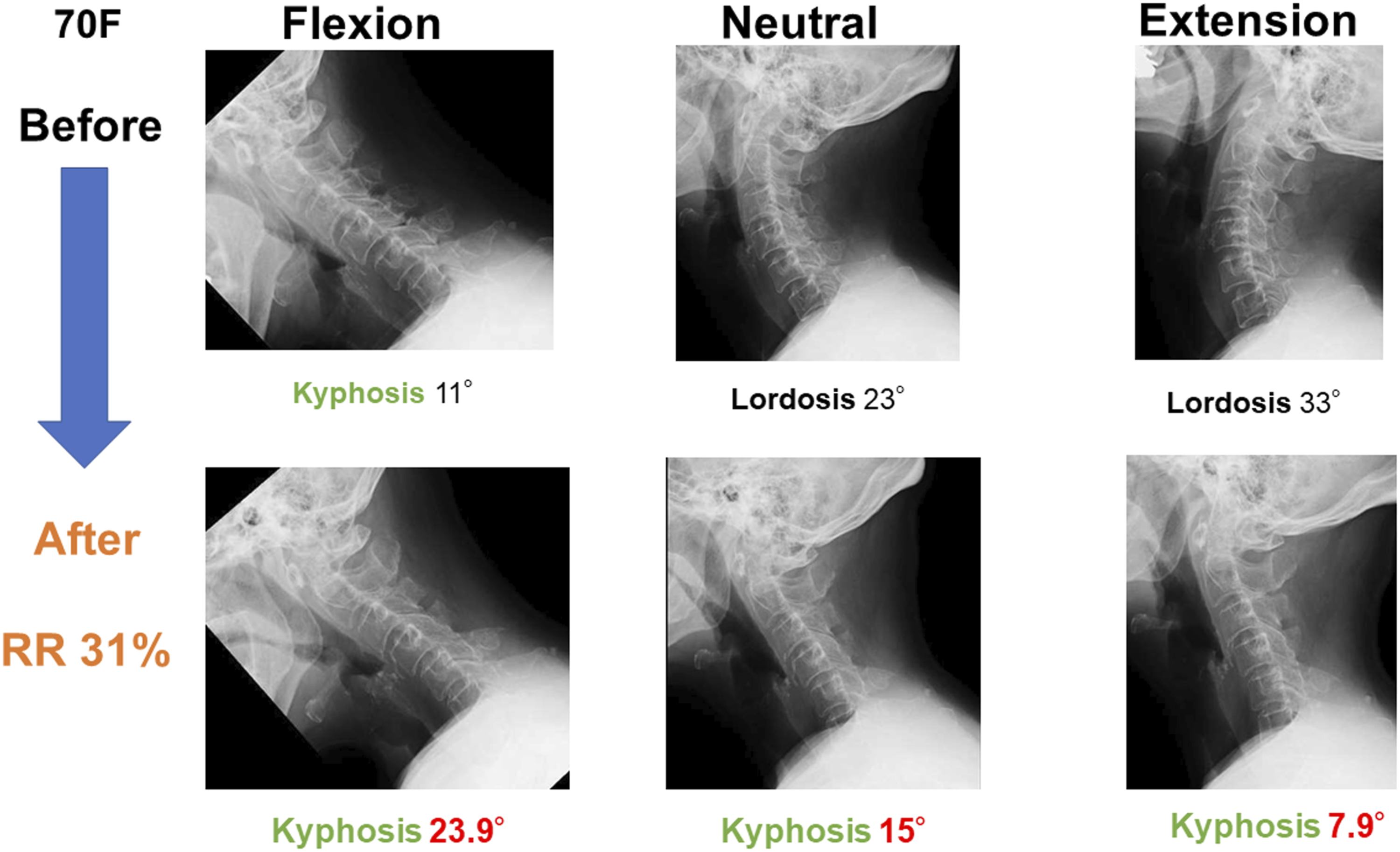
Discussion
The major result of the present study was that in addition to an older age and longer duration of disease, postoperative cervical kyphotic alignment during neck flexion resulted in poor surgical outcomes after 1 year.
The Impact of Deteriorating Cervical Kyphosis on Surgical Outcomes
Cervical spine alignment is a factor that needs to be considered when selecting surgical procedures, but is not absolute. Previous studies reported that kyphosis up to approximately 13–14° preoperatively may be improved by laminoplasty,19,20 and that non-lordotic alignment did not necessarily result in poor outcomes. 21 Posterior decompression surgery provides indirect decompression by shifting the spinal cord posteriorly in lordotic alignment, but may be inadequate for kyphosis or large anterior compression factors. Further deteriorations in cervical alignment and balance were recently observed in elderly patients with large CGH-SVA who underwent laminoplasty, resulting in poor outcomes. A cadaver study showed that intramedullary spinal cord pressure increased with kyphosis, with pressure being moderate up to 20°, but significantly increasing over 21°. 22 Based on these findings, excessive kyphosis above the threshold may result in spinal cord compression and ischemia. Previous studies revealed that severe spinal cord compression due to kyphosis or anterior compression factors may cause severe lower limb dysfunction.23,24 Therefore, in cases at risk of excessive kyphosis, additional long segmental posterior instrumented fixation, anterior fixation, or a combination of anterior and posterior surgery may be warranted. The addition of a fusion procedure increases the complication rate and cost of care over those of laminoplasty alone; therefore, surgeons may need to consider procedures based on the number of intervertebral levels to be operated on, age, and comorbidities.5,25
The Reason why Alignment Evaluations During Neck Flexion Are Useful
As cervical kyphosis progresses, the horizontal gaze becomes more difficult; therefore, neck extension is used to compensate and allow for the horizontal gaze. 26 In this alignment, the neck is already assumed to be extended to some degree in order to maintain the neutral position. Therefore, the ROM of extension is reduced, while that of flexion is increased. (Figure 3) Previous studies reported that CSM patients with these characteristics were more likely to develop kyphotic deformities following posterior surgery.27,28 The risk factor for the loss of cervical lordosis in the present study, namely, a small ROM of extension, was consistent with these findings. (Table 6) The flexion position, without horizontal gazing, allows for a more direct assessment of the degree of kyphosis because it eliminates the effects of compensation, and this may explain why some studies found no significant differences in outcomes based on whether patients had kyphosis after posterior surgery.
Age and Duration of Disease
The outcomes of elderly patients were previously shown to be inferior to those of younger patients,3,4,9,11 and they were also more likely to have the inferior recovery of lower limb function. 29 Furthermore, elderly patients are characterized by the rapid progression of symptoms and lower JOA scores. 30 Patients with vascular diseases are more likely to have rapid progression. 31 Even in the elderly, similar JOA scores were obtained after surgery, 29 suggesting that it is an effective and recommended intervention.
Inferior outcomes are associated with a longer duration of disease and may be attributed to spinal cord symptoms being partly caused by worsening spinal cord blood flow, which is irreversible if the appropriate surgical timing is missed. Therefore, surgeons need to understand the condition of a patient, inform the patient of their condition and the expected course of the disease, and intervene at the appropriate time.
Characteristics and Outcomes due to the Type of Surgical Procedure
No significant differences were observed in RR among the types of surgical procedures. The ELAP group achieved greater lordosis during flexion postoperatively, which was consistent with previous findings. 32 Interestingly, Group G in the ELAP group achieved more lordosis during flexion after surgery. In the other 2 groups, a significant difference was observed in the postoperative C2-7 angle between Groups G and F. The combined instrumented fusion group had less preoperative lordosis and a greater kyphotic change after surgery, which may have had more negative effects on outcomes. The SLAP group was older, had a larger C7 slope and C2-7 SVA before surgery, and was able to maintain ROM better after surgery, which may have made it more difficult for this group to maintain lordosis during flexion postoperatively than the ELAP group.
MRI Findings
In the present study, MRI findings did not correlate with postoperative outcomes.
Nouri et al. reported that the addition of MRI findings to the preoperative assessment of a patient’s condition did not improve the accuracy of predictions. 33 Machino et al also demonstrated that a high T2WI signal intensity change on preoperative MRI was not associated with surgical outcomes 34 ; however, other studies showed that patients with the postoperative resolution of signal intensity changes had better outcomes.35,36 Low-signal intensity changes on T1WI, which indicate irreversible changes, such as spinal cord necrosis, have been associated with poor postoperative outcomes.37,38 However, since the prevalence of low-signal intensity changes on T1WI is low, it may not have been significant in the present study, which examined a small number of cases.
Severity of Symptoms
Preoperative severity has been suggested to affect surgical outcomes.9,11 In the present study, no significant differences were observed in preoperative JOA scores, which may have been because we generally selected surgery based on a JOA score of <11–12 points and the number of extremely severe or mild cases was small. Another reason may be that the MCID study on JOA score 17 was not statistically powered for preoperative severity.
Surgical Outcomes of CSM Are Influenced by Multiple Factors
Previous studies identified factors associated with surgical outcomes based on preoperative patient backgrounds, cervical spine alignment, and MRI findings.12,13,15,18-20 Although various factors influence outcomes, as described above, few studies have examined the impact of postoperative cervical spine alignment. The strength of the present study is that the multivariate analysis revealed that more advanced postoperative cervical kyphosis deformity during neck flexion was associated with greater difficulties achieving RR ≥50%. This is consistent with the findings of a cadaver study showing that intraspinal pressure was significantly increased only after excessive kyphosis. 22 It may also explain why non-lordosis adequately recovered with laminoplasty. In addition to the degree of kyphotic deformity, age and the duration of disease may affect the outcomes of surgery.
Limitations
This was a retrospective single-center study involving uncontrolled clinical observations, the number of cases was small, and the follow-up rate was not high. Our facility is in a rural area in Japan with one of the highest number of elderly individuals, which may explain why many patients are lost to the follow-up in our institution after surgery. Furthermore, it was challenging to obtain consent for postoperative MRI examinations from all patients, making evaluations difficult. Since the number of cases was not large in the present study, we did not perform a multivariate analysis of each type of surgery. Further studies are needed to clarify the factors associated with the outcomes and postoperative alignments of each procedure. Moreover, the only assessment component was the JOA score, patient-reported outcomes were not examined.
Conclusion
We retrospectively assessed the surgical outcomes of laminoplasty in 103 CSM cases. Postoperative deteriorations in cervical kyphosis during neck flexion affected outcomes, in addition to an older age and longer duration of disease. We consider the present results to provide useful information that will facilitate the selection of surgical procedures and obtaining informed consent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.