
Abstract
Study Design
A retrospective observational study.
Objective
The purpose of this study was to evaluate the Global Alignment and Proportion (GAP) score and mechanical failure (MF) following corrective fusion surgery with planned 2-stage surgery using lateral lumbar interbody fusion in patients with adult spinal deformity (ASD).
Methods
Fifty-four patients (2 men, 52 females, aged 70.3 years) were included. MF, proximal junctional failure (PJF), and rod breakage (RB) occurred in 46.3% (25/54), 22.2% (12/54), and 29.6% (16/54) of patients, respectively. The immediate postoperative GAP scores were compared between patients with MF and without MF (MF+ and MF-, respectively). GAP scores in groups with and without PJF or RB were also compared.
Results
Patients were grouped according to the GAP score for spinopelvic alignment: 23 (42.6%) as proportioned, 22 (40.7%) as moderately disproportioned, and 9 (16.7%) as severely disproportioned. The pre- and postoperative spinopelvic parameters did not differ significantly between the MF- and MF+ groups except pelvic incidence. Postoperatively, the mean pelvic incidence—lumbar lordosis changed to <10° in both groups. The GAP score and 3 categories of GAP scores did not differ significantly between the PJF- and PJF+ groups or between the RB+ and RB- groups.
Conclusion
Multiple factors can cause PJF and RB, and the patient’s background may affect the ability to use the GAP score to predict MF. Further research may be needed in the future using modified GAP scores with additional factors in ASD patients.
Keywords
Introduction
Corrective surgery may be performed in patients with adult spinal deformity (ASD) because of its effects on quality of life. 1 The surgical management of ASD presents a surgical challenge to spine surgeons. For example, the operation must achieve the proper sagittal alignment for the correction of ASD while avoiding mechanical complications such as proximal junctional kyphosis (PJK), proximal junctional failure (PJF), and rod breakage (RB).1-5 Formulas for ensuring sagittal correction have been reported, and the ideal postoperative alignment of ASD is known.6-8 In the sagittal plane, the surgical plan must consider both the global alignment and distribution of spinal curves according to pelvic incidence (PI) and/or the Roussouly classification. 9 However, even with good alignment, a high incidence of mechanical failure (MF) and requirement for unplanned reoperation has been reported after ASD surgery. 10
The Global Alignment and Proportion (GAP) score has been developed as a new PI-based proportional method for analyzing the sagittal plane and predicting MF after surgery for ASD. 11 The GAP score is the first system to consider the proportional analysis of the spinopelvic alignment. Setting surgical goals according to the GAP score may decrease the prevalence of MF. The GAP score has been validated in a few studies, and its scores tend to be higher in patients with MF, although others have found no strong correlation between GAP scores and MF.12-17 Yagi et al. found no association between the GAP score and the incidence of MF or revision surgery in an Asian cohort of patients with ASD, and they concluded that additional validation studies from multiple countries and adjustments to the scoring system might be necessary. 17
Many factors are considered in the GAP score, but it is undeniable that the definition of MF may influence the GAP score. The definition of MF generally includes PJF, RB, distal junctional failure (DJF), and other implant-related complications. 11 PJF is defined as a fracture of the upper instrumented vertebra (UIV) or the vertebra above and is associated with greater pain, gait disturbance, and pullout or failure of the UIV fixation by PJK, and neurological defects requiring revision surgery. 3 RB usually happens when a pseudoarthrosis or nonunion is present. 18 Fusion ending at L5 has been reported to be a significant risk factor for the postoperative occurrence of DJF. 19 However, given that corrective alignment is not the only cause of each type of failure, it is important to evaluate the relationship between the GAP score and the occurrence of PJF, RB, and DJF individually. The purpose of this study was to evaluate the relationships between the radiographic outcomes results and the GAP score for each MF-causing factor, particularly PJF and RB.
Methods
Study Design
We conducted a retrospective observational study of a cohort of consecutive patients diagnosed with ASD who underwent corrective spinal surgery. The study was approved by our institutional review board (application No. 21R-237). Because this study was retrospective, the requirement for informed consent was waived.
Patients were considered candidates for thoracolumbar correction if fusion was indicated because of ASD and if an entire course of conservative care had been exhausted. The preoperative deformity criteria for enrollment were identical to those of the original GAP study: age >20 years and ≥1 of the following parameters: coronal Cobb angle >20°, the sagittal vertical axis (SVA) > 5 cm, pelvic tilt (PT) > 25°, or thoracic kyphosis (TK) > 60°. 11 Patients with a minimum of four fused vertebrae and complete 1-year follow-up data were included.
Characteristics of the Subjects in the Present Study.
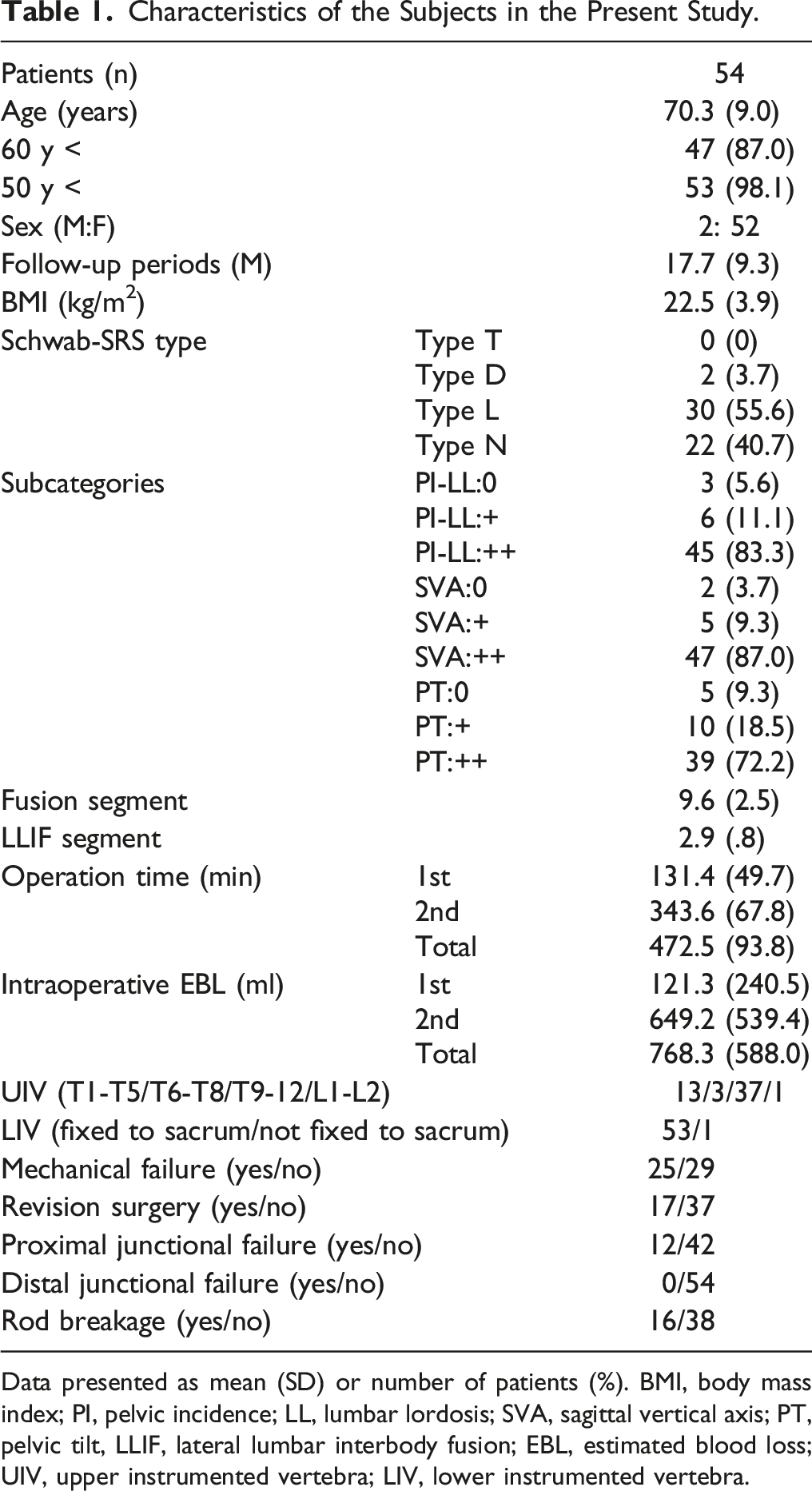
Data presented as mean (SD) or number of patients (%). BMI, body mass index; PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis; PT, pelvic tilt, LLIF, lateral lumbar interbody fusion; EBL, estimated blood loss; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra.
Radiological Measurements
Radiographic data consisted of full-length lateral radiographs obtained before and immediately after the operation and at 1 year postoperatively. The images were obtained with the patient in a free-standing posture with the fingers placed on the clavicles.
The spinopelvic parameters measured included the following measurements: SVA, lumbar lordosis (LL), LL at L4-S1, TK at T5-L1, sacral slope (SS), PT, PI, and global tilt (GT). GT was defined as the sum of the PT and the C7 vertical tilt or the angle created by the intersection of 2 lines: the first drawn from the center of the C7 vertebra to the center of the sacral endplate, and the second from the center of the femoral head to the center of the sacral endplate. 20
GAP Score
Five components of the GAP score were calculated using early postoperative radiographic parameters (average 8.1 ± 7.0 weeks) following the methods previously described by adding the scores for relative pelvic version (RPV), relative lumbar lordosis (RLL), lordosis distribution index (LDI), relative spinopelvic alignment (RSA), and age; the score ranged from 0 to 13 points. Age was stratified into two subgroups: <60 and ≥60 years. A GAP score of 0 to 2 was categorized as proportioned; 3 to 6, as moderately disproportioned; and ≥7 as severely disproportioned spinopelvic alignment. 11
Surgical Procedure
The anterior-posterior staged surgery used to correct degenerative kyphoscoliosis was performed as follows. First, we performed lateral lumbar interbody fusion (LLIF) of 2–4 intervertebral discs via a lateral approach. Large cages (cage height: 8–12 mm, angle: 10°) were inserted to correct and stabilize the intervertebral bodies. The patient was allowed to ambulate on the day after the first surgery, and the spine was reevaluated to plan the second posterior operation. One week later, posterior corrective fusion along with transforaminal lumbar interbody fusion (TLIF) at L5/S1 was performed using a pedicle screw system.
Types of MF Included
This study defined MF as PJF, DJF, and RB, with or without revision surgery. We included all types of MF found on radiographs and developed after the operation (PJF, DJF, RB, and other implant-related complications). PJF and DJF represent more severe clinical symptoms associated with MF and increased risk of neurologic injury, deformity, and pain.21,22
Following the definition of Yagi et al., 23 we also defined PJF and DJF as symptomatic PJK and DJK requiring all types of revision surgery. The patients were categorized into two groups: those who had any MF (MF+ group) and those who were free of MF (MF- group). The GAP scores with and without PJF or RB were also compared.
Statistical Analysis
The data was analyzed using IBM SPSS Statistics (version 23.0; IBM Corp, Armonk, NY, USA). All values are expressed as the mean ± standard deviation. We first used the Kolmogorov-Smirnov test to test all continuous variables for a normal distribution. Next, we investigated the relationships between the two groups using the chi-squared test for categorical variables, t-test analysis of variance for continuous variables, and the Mann–Whitney U test. For all statistical analyses, the type 1 error was set at 5%, and P < .05 was assumed to be significant.
Results
Table 1 presents the general characteristics of the included patients. Most were female (96.3%), and the mean age was 70.3 years (±9.0). 98.1% of patients (53/54 patients) were over 50 years old. The mean follow-up was 17.7 months (±9.3), and all patients had >1-year follow-up. The mean BMI was 22.5 kg/m2 (±3.9).
Patients were categorized according to the SRS-Schwab classification. None of the 54 patients had thoracic curve type (T type), 3.7% had double curve type (D type), 55.6% thoracolumbar or lumbar curve type (L type) deformities, and 40.7% had a pure sagittal deformity (N type).
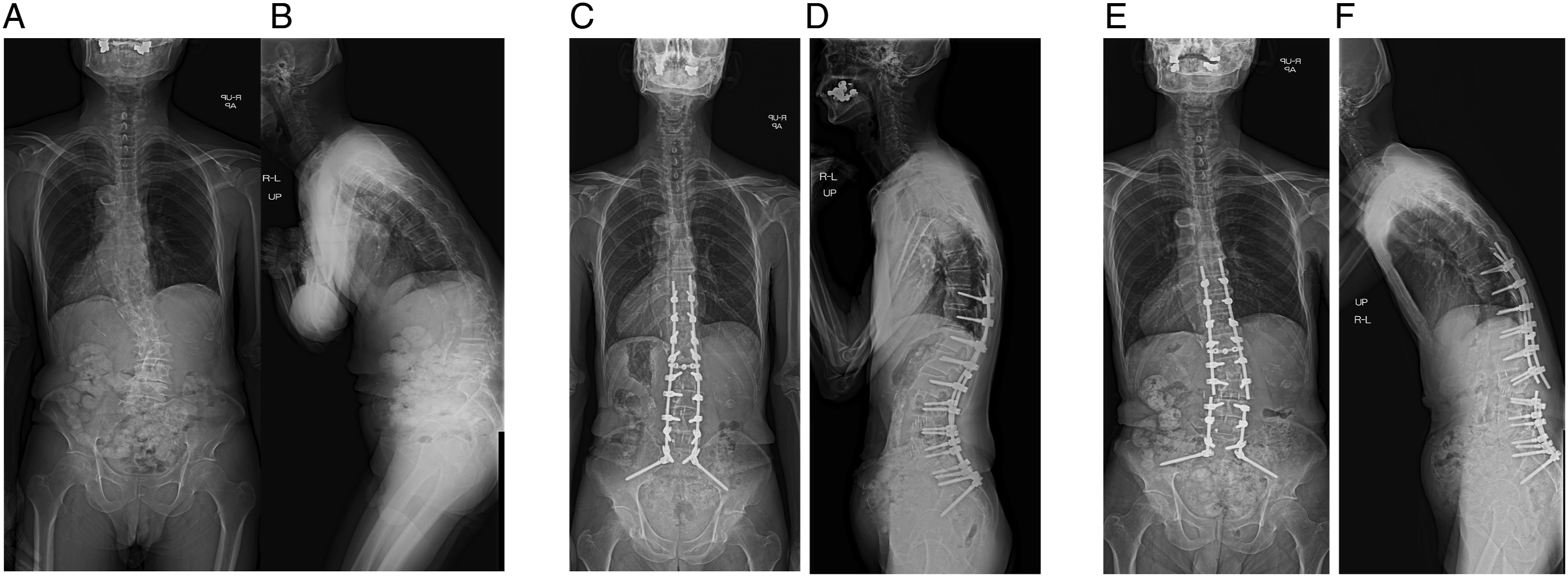
Of the 54 patients, the numbers and percentages of patients with a severe modifier grade (++) were 45 (83.3%) with PI-LL, 47 (87.0%) with SVA, and 39 (72.2%) with PT. The number of levels fixed was 9.6 (±2.5), and 2.9 (±.8) had LLIF to the intervertebral discs. The numbers of patients with each complication were as follows: 12 patients (22.2%) with PJF, none with DJK (0%), and 16 patients (29.6%) with RB. RB was diagnosed on average 11.3 months after surgery and most often occurred on L4/5 (7 patients). Revision surgery because of MF was needed by 17 patients (31.4%) and resulted from PJF in 9 patients (16.7%) (Figure 1), RB in 5 patients (9.3%) (Figure 2), and PJF and RB in 3 patients (5.6%). Case of proximal junctional failure (PJF). A 69-year-old female underwent lateral lumbar interbody fusion from L2/3 to L4/5, transforaminal interbody fusion at L5/S1, and posterior segmental spinal instrumented fusion from T10 to the pelvis ASD. (A, B) Preoperative radiographs. (C, D) Postoperative radiographs 8 weeks after surgery. GAP score = 2. (E) Follow-up radiographs 10 months after surgery showing that PJF had occurred. Case of rod breakage (RB). A 72-year-old man underwent lateral lumbar interbody fusion from L2/3 to L4/5, transforaminal interbody fusion at L5/S1, and posterior segmental spinal instrumented fusion from T10 to the pelvis ASD. (A, B) Preoperative radiographs. (C, D) Postoperative radiographs 8 weeks after surgery. GAP score = 3. (E, F) Follow-up radiographs 8 months after surgery showing that bilateral RB (arrows) at L3/4 had occurred.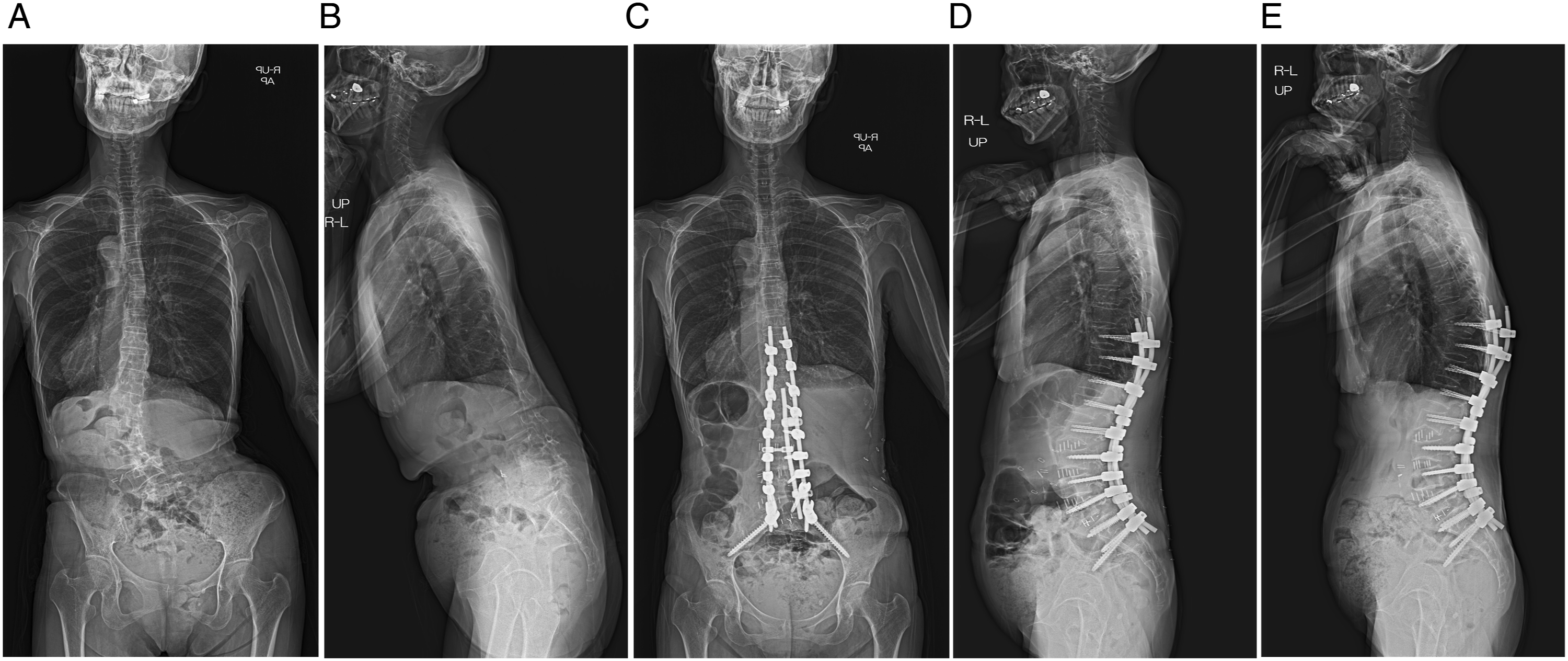
Surgical Factor Characteristics in the MF (−) and MF (+) groups.
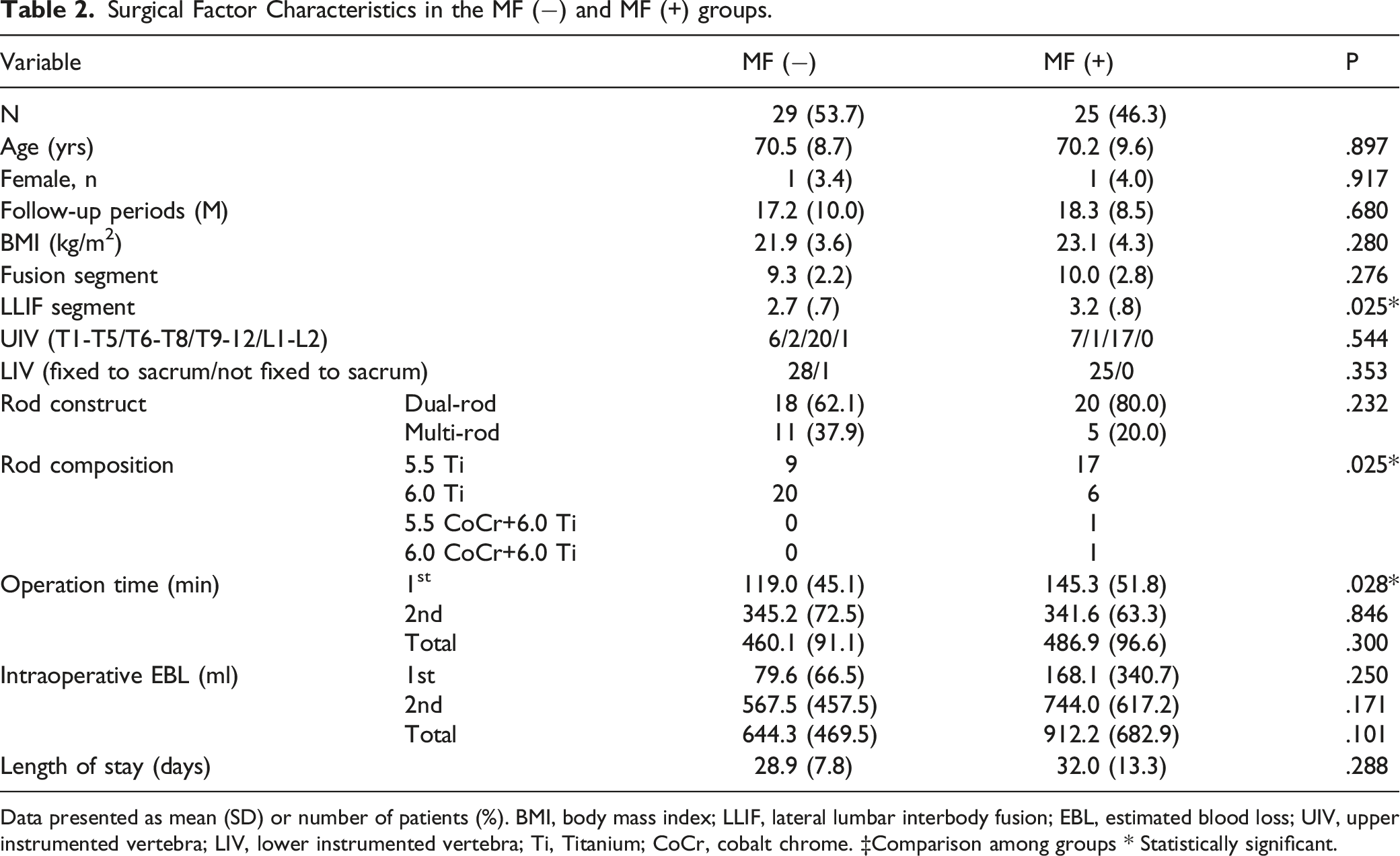
Data presented as mean (SD) or number of patients (%). BMI, body mass index; LLIF, lateral lumbar interbody fusion; EBL, estimated blood loss; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra; Ti, Titanium; CoCr, cobalt chrome. ‡Comparison among groups * Statistically significant.
Preoperative and Postoperative Spinopelvic Parameters in the MF (−) and MF (+) Groups.
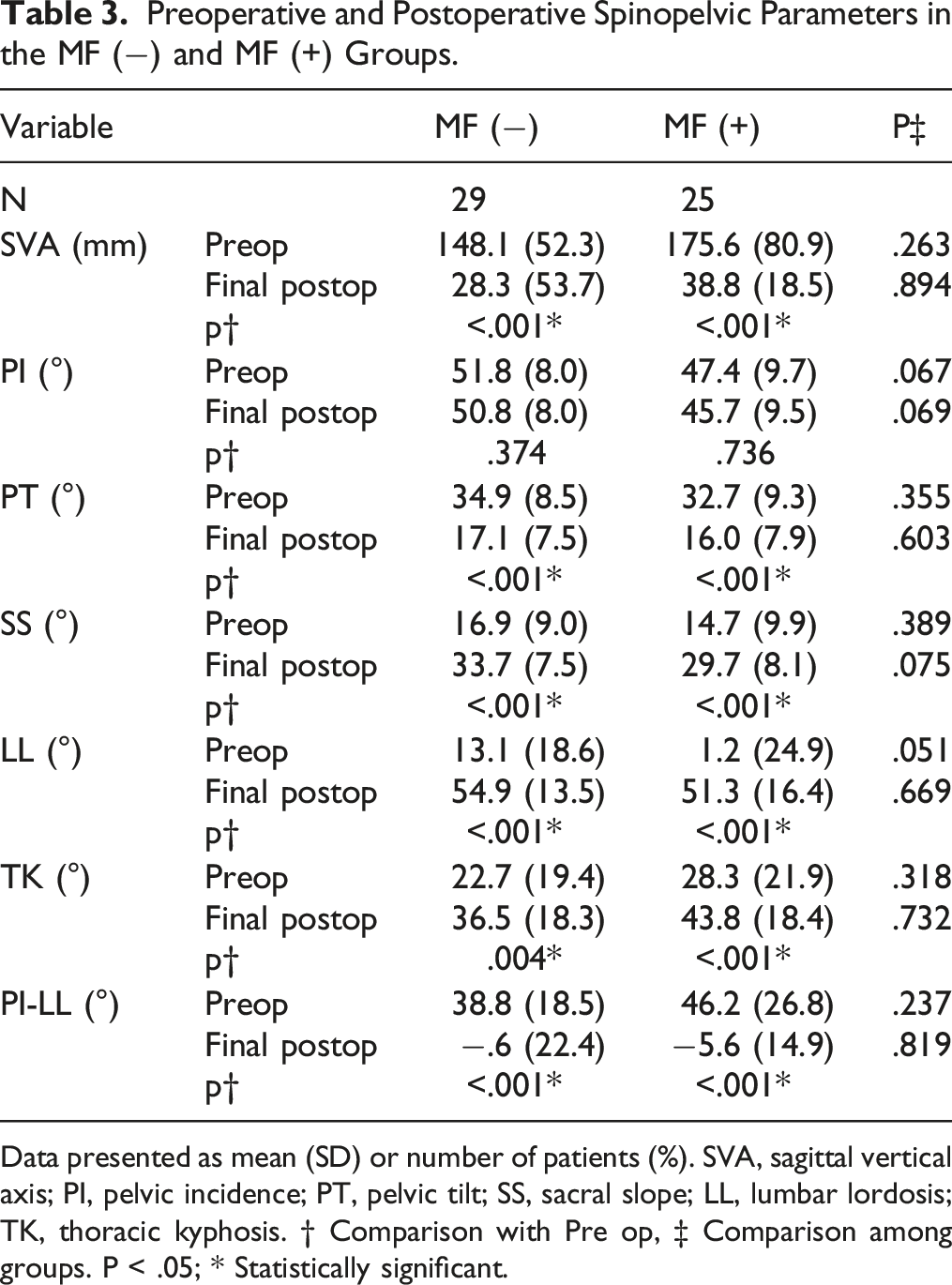
Data presented as mean (SD) or number of patients (%). SVA, sagittal vertical axis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; LL, lumbar lordosis; TK, thoracic kyphosis. † Comparison with Pre op, ‡ Comparison among groups. P < .05; * Statistically significant.
GAP Score of the MF (−) and MF (+) Group.
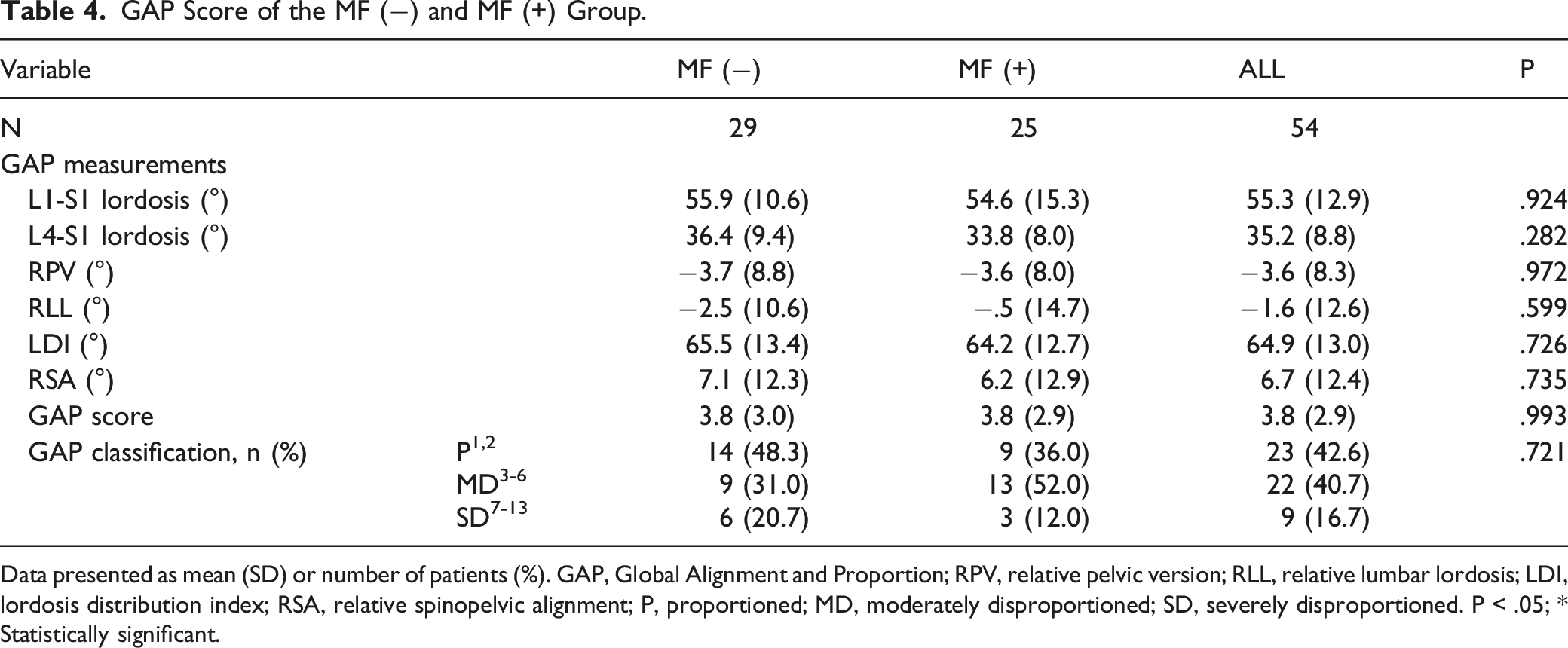
Data presented as mean (SD) or number of patients (%). GAP, Global Alignment and Proportion; RPV, relative pelvic version; RLL, relative lumbar lordosis; LDI, lordosis distribution index; RSA, relative spinopelvic alignment; P, proportioned; MD, moderately disproportioned; SD, severely disproportioned. P < .05; * Statistically significant.
Comparison of GAP Scores in PJF (A) and RB(B).
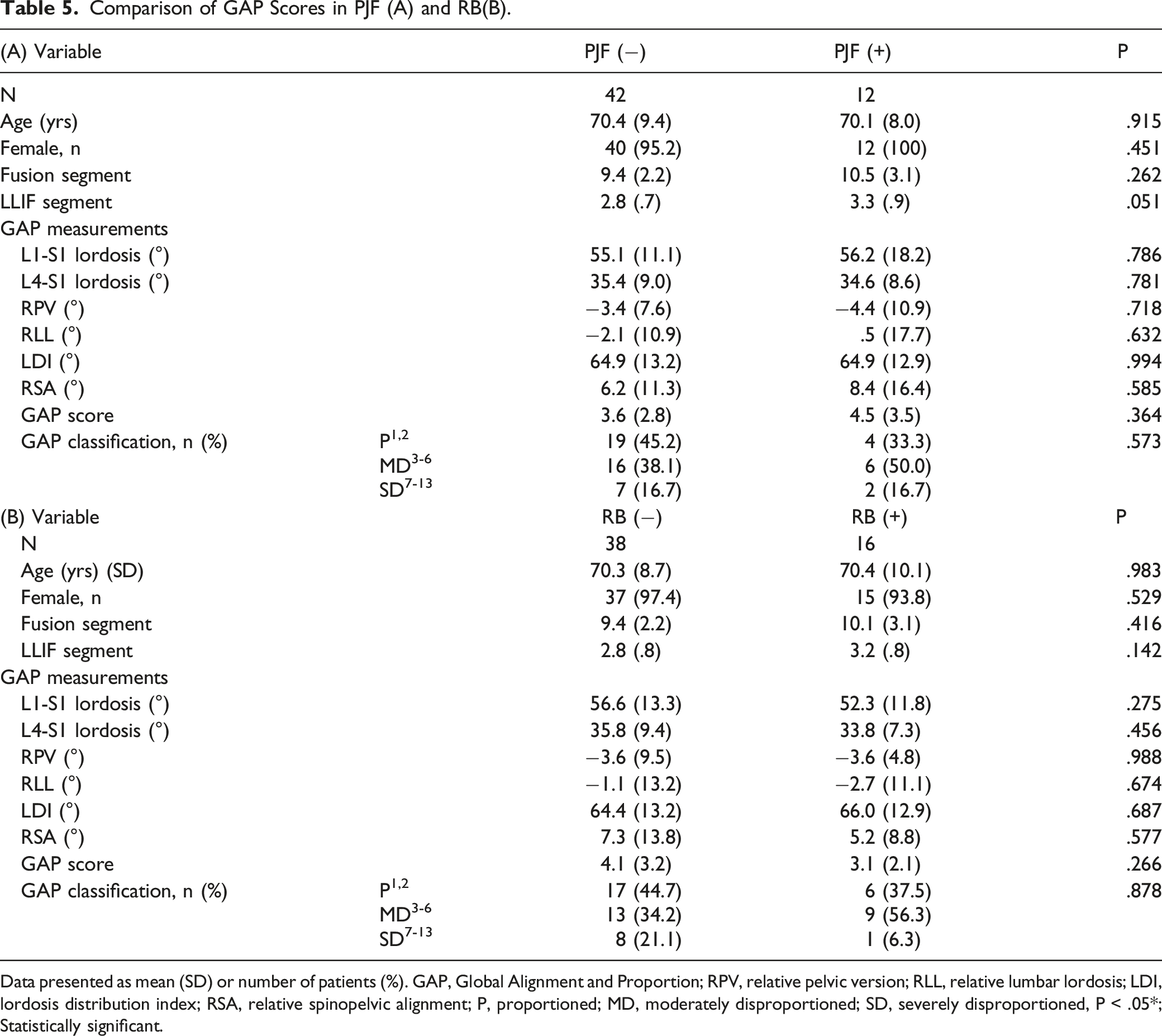
Data presented as mean (SD) or number of patients (%). GAP, Global Alignment and Proportion; RPV, relative pelvic version; RLL, relative lumbar lordosis; LDI, lordosis distribution index; RSA, relative spinopelvic alignment; P, proportioned; MD, moderately disproportioned; SD, severely disproportioned, P < .05*; Statistically significant.
Discussion
Previous studies have investigated postoperative complications and their risk factors following corrective surgery for ASD,4,24,25 and the postoperative complication rates (8.4%–42%) and revision rates (9%–17.6%) for ASD remain high.26,27 Thus, elucidation of the factors related to the risk of surgical complications is essential for making appropriate decisions regarding the treatment of ASD, especially in the elderly. GAP scores based on earlier validation studies have been reported to help plan corrective surgery for patients with ASD.12,14,28 The main advantage of the GAP score is that it can distinguish normal from pathological standing sagittal alignment and shape in a single score for every magnitude of PI. However, we found no significant difference in GAP scores between patients who did and did not experience MF in this study. Other reports have also found that GAP score was not associated with MF after ASD surgery.15,17 Therefore, disagreement remains as to whether the GAP scoring system can predict MF.
There are several possible reasons for this difference between study results. First, differences between studies of GAP scores may reflect differences in the patients’ age, ethnicity, and spinal alignment. Some studies have proposed formulas to calculate the ideal LL to establish the optimal surgical strategy for ASD patients. However, even in a normal recovery of LL, it is not uncommon for patients to have poor outcomes after spinal correction surgery. The average age of patients in our study was 70 years, and many of them had severe sagittal deformities; 83.3% (45/54) were considered to have a variant of the Schwab-SRS PI-LL subcategory (++), and these patients needed a large amount of sagittal correction to achieve the target spinal alignment. Therefore, we performed surgery to obtain a large LL according to the Schwab-SRS formula. 29 In our patients, the postoperative PI-LL mismatch improved, but 46.3% of them developed MF after surgery. This suggests that factors other than a PI-LL mismatch can affect MF after ASD surgery.
In our study, the rod composition and numbers of LLIF segments differed between the MF- and the MF+ groups. Moreover, the PI is a structural characteristic of the sacrum and pelvis and is not modified by posture, although a previous study reported that the PI increases linearly after skeletal maturity and continues to do so throughout the lifespan. 30
We note that the mean age of the original GAP study population was younger (52.2 ± 19.3 years) than our cohort and that the inclusion criteria for the original cohort were not limited to ASD, which might cause heterogeneity in terms of disease etiology. 11 A second possible reason for differences between studies is that surgical factors may influence the GAP score. ASD surgery can include different surgical methods, posterior instrumentation fusion range, and rod material properties (elastic modulus and Poisson’s ratio). Previous studies have included patients who have undergone 3-column osteotomy or LLIF to obtain adequate LL with the use of posterior instruments. We included patients who underwent 2-stage surgery using LLIF. In addition, the UIV involved mainly T9-12 levels, and the LIV was the pelvis except for 1 patient. Variations in the UIV or LIV settings can also affect the results.14-16
A third possible reason for differences between studies is that the GAP scores were obtained from radiographs obtained 6 weeks postoperatively in the previous studies, and the MFs were evaluated two years after the surgery.11,23 That is, the timing of the GAP score calculation may be an issue.
The fourth reason is bone quality. The presence of osteoporosis is also important as a risk factor of MF. Osteoporosis prevalence has been reported as greater than 50% in women age >50 years undergoing spine surgery compared with a 15% rate in men. 31 In our case, 98.1% of patients (53/54 patients) were over 50 years old. As with age, differences in bone mineral density (BMD) may affect the cause of MF. Dual-energy x-ray absorptiometry (DXA) is currently considered the gold standard for assessing BMD, but DXA is not necessarily part of regular preoperative examinations. 32 In addition, DXA has been shown to underestimate spinal bone loss and may not always be accurate given the amount of degeneration obscuring the true values. As such, unfortunately, not all of our patients have could evaluate BMD in this study.
Finally, even if MF occurs, it is difficult to identify the factors causing PJF, RB, DJF, and other outcomes, and the definition of MF itself may vary between studies. In our study, the GAP scores were investigated separately in patients with or without PJF, and with or without RB, but the scores did not differ significantly between these groups. The risk factors for PJK can be classified according to patient-related, radiological, and surgical factors. The risk factors for RB include older age, greater sagittal alignment correction, PI-LL mismatch, deformity correction using osteotomy, constructs across both the thoracolumbar and lumbosacral junctions, and the rod contour.33,34 Therefore, we suggested that it is difficult to predict MF from the GAP score because MF involves multifactorial factors.
The present study has several limitations. First, we did not assess osteoporosis, muscle volume, or other age-related disorders that may have affected the results. The GAP scores have limitations on patient characteristics such as bone quality and muscle mass, which can significantly impact surgical outcomes, especially in elderly patients with ASD. 35 Yagi et al. have reported that BMD and BMI are risk factors for MF. 36 However, the problem is that the GAP score cannot evaluate these factors. Therefore, reassessment using modified GAP scores after ASD surgery by adding BMD and BMI may be necessary.35
Second, the survey period was short: an average of 17.7 months after surgery. However, previous studies have reported that most PJF and RB occur early after surgery; PJF occurs early in the postoperative period and often within the 6 months following surgery. 37 RB occurred in 18 (9.0%) of 200 ASD patients at an average of 14.7 months in 1 report 38 and 25 months in 47 of 178 ASD patients (26%) in another report. 18 Third, because it was a retrospective study, there were variations in the surgical procedures, and the number of cases was small. Further research with a stronger study design is needed.
Conclusion
We found no significant difference in GAP scores between the MF- and MF+ groups. Multiple factors can influence the incidence of PJF and RB, and the patient’s background seems to affect the ability to use the GAP score to predict MF. Further research may be needed in the future using modified GAP scores with additional factors such as BMD and BMI in ASD patients.
Footnotes
Authors’ Note
This study does not have any prior or duplicate submissions or publications elsewhere of any part of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.