
Abstract
Study Design
Retrospective National Database Study
Objectives
The aim of this study was to investigate the national trend of lumbar disc arthroplasty (LDA) utilization from 2005 to 2017.
Methods
Patients undergoing primary LDA between 2005 and 2017 were identified in the National Inpatient Sample (NIS) database. Year of the procedure, demographic, socioeconomic, hospital, and cost parameters were analyzed. The data was weighted using provided weights from the NIS database to generate national estimates of LDA procedure incidence. Lastly, we assessed the incidence of cervical disc arthroplasty (CDA) between 2005 and 2017 to serve as a historical comparison.
Results
An estimated 20 460 patients underwent primary LDA in the United States between 2005 and 2017. There was an initial decrease in LDA procedures between 2005 and 2006 and then a plateau between 2006 and 2009. From 2010 to 2013, there was a significant year-over-year decrease in annual LDA procedures performed, followed by a second plateau from 2014 to 2017. Overall, LDA procedures decreased 82% from 2005 to 2017. Over the same time, the annual incidence of CDA utilization increased 795% from approximately 474 procedures in 2005 to 4245 procedures in 2017 (P < .01).
Conclusions
Lumbar disc arthroplasty utilization decreased 82% from 2005 to 2017, with a significant decrease in the rate of utilization noted after 2010. The utilization of LDA to treat selected degenerative lumbar conditions has not paralleled the increasing popularity of CDA, and, in fact, has demonstrated a nearly opposite utilization trend.
Introduction
Lumbar degenerative disc disease (DDD) is a common cause of lower back pain and disability in the United States.1-5 Nonoperative management is indicated in the majority of patients, but in patients with continued symptoms refractory to nonoperative treatment, surgical intervention may be indicated. 6 The operative management of lumbar DDD is without consensus to date. 7 Fusion has long been the procedure of choice. However, studies on outcomes of lumbar fusion in the setting of isolated DDD are mixed, with some showing no benefit as compared to nonoperative treatment, 8 and others showing substantial improvement with certain indications.9-11 Posterior only fusion, interbody fusion, or circumferential fusion are all accepted in the operative treatment of lumbar DDD. 10 However, because the lumbar spine is naturally mobile, fusion carries with it the risk of adjacent segment disease and pseudarthrosis.12-15
Lumbar disc arthroplasty (LDA) was introduced to preserve motion at the diseased segment, theoretically decreasing risk of adjacent segment disease and eliminating the risk of pseudarthrosis.16-20 The modern LDA was originally designed in early 1980s, and underwent several revisions before FDA approval in 2004.21,22 Initial results were promising, with early randomized control trials showing improved results compared to fusion with 2-year follow-up.23,24 However, narrow indications, technical challenges, and decreased insurance reimbursement have possibly led to decreased enthusiasm for LDA.25-29 The aim of this study was to investigate the national trend of LDA utilization from 2005 to 2017.
Methods
Database Description
The current study was conducted using the National Inpatient Sample (NIS) database, which is the largest available hospital care database in the United States. Sponsored by the Agency for Healthcare Research and Quality (AHRQ) and developed for the Healthcare Cost and Utilization Project (HCUP), the database has a 20-percent stratified sample of all discharges from U.S. community hospitals (excluding rehabilitation and long-term acute care hospitals) that participated in HCUP from 1988to 2017. The NIS database includes patients from varying types of insurance: Medicare, Medicaid, private insurance, and no insurance. All patient and physician identifiers are removed in the database. Approval for the institutional review board was not required for this investigation.
Patient Selection
The International Classification of Diseases (ICD) system was utilized to query the NIS database. Patients who underwent primary LDA from 2005to 2017 were identified by ICD-9 procedure code 84.65 and ICD-10 procedure codes 0SR40JZ and OSR20JZ. The temporal trend of cervical disc arthroplasty (CDA) was identified during the same time period to serve as a concurrent comparison. ICD-9 procedure code 84.62 and ICD-10 procedure codes 0RR30JZ were used to query NIS for CDA. NIS provides demographic, hospital, and socioeconomic information such as age, gender, race, payment method, household income, bed size, hospital ownership, hospital region, and teaching status. These descriptive characteristics were collected in this study as well.
Statistics
Adjustment with the sampling weight provided by the NIS database allowed for the generation of national estimates of LDA procedure incidence. LDA trends from 2005to 2017 were analyzed with linear regression, which demonstrated a clear decrease in the absolute value of the slope between 2009 and 2010. Thus, 2 temporal groups were created: one ranging from 2005to 2009 and the other from 2010 to 2017. Descriptive statistics provided by NIS were compared between these two time periods. Furthermore, the most common primary diagnoses code associated with the LDA procedure were recorded. Continuous variables were compared using independent t-tests and discrete variables were compared using Chi-square tests. All analyses were conducted using STATA Version 16.1 (Stata Corporation). A two-tailed P-value of <.05 was considered as statistically significant.
Results
Our query resulted in a weight estimated of 20 460 patients who underwent LDA between 2005 and 2017. When LDA was initially approved by the FDA in 2005, there was a relatively high utilization, which increased between 2005 and 2006 (Figure 1A). This was followed by a plateau from between 2006 and 2009, and then a sharp decline in the amount of LDA’s performed in the years of 2010–2013. Between the years of 2013 and 2017, there was a second, lower, plateau in utilization (Figure 1A). Overall, there was an 82% decrease in LDA utilization over the study period, with 3650 procedures in 2005 and 640 procedures in 2017. We see an opposite trend in the CDA cohort (Figure 1B). From 2004 to 2009, there was a steady increase, followed by a drop in utilization from 2009 to 2012. From 2012 to 2016, we again see an increase in national incidence, after which the values begin to plateau. Over the entire study period, we see a net increase of 795% of CDA use, beginning at 474 procedures in 2005 and ending at 4245 procedures in 2017. (A) The national incidence of lumbar disc arthroplasty from 2005 to 2017. (B) The national incidence of cervical disc arthroplasty from 2005 to 2017.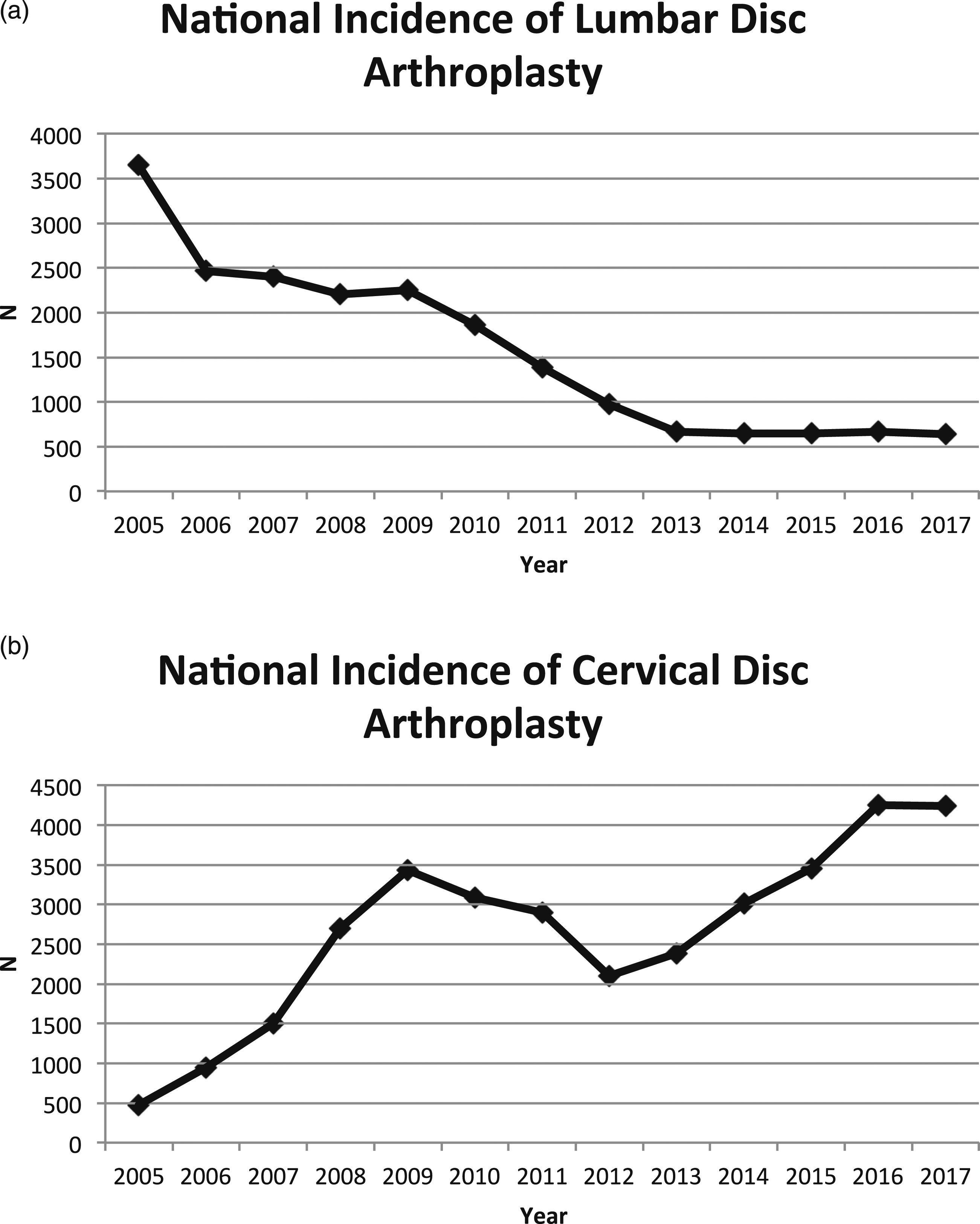
Demographic comparisons between the 2 temporal groups (2005–2009 vs 2010–2017). *Denotes significance. ◆Payment utilized is not recorded in the NIS Database.
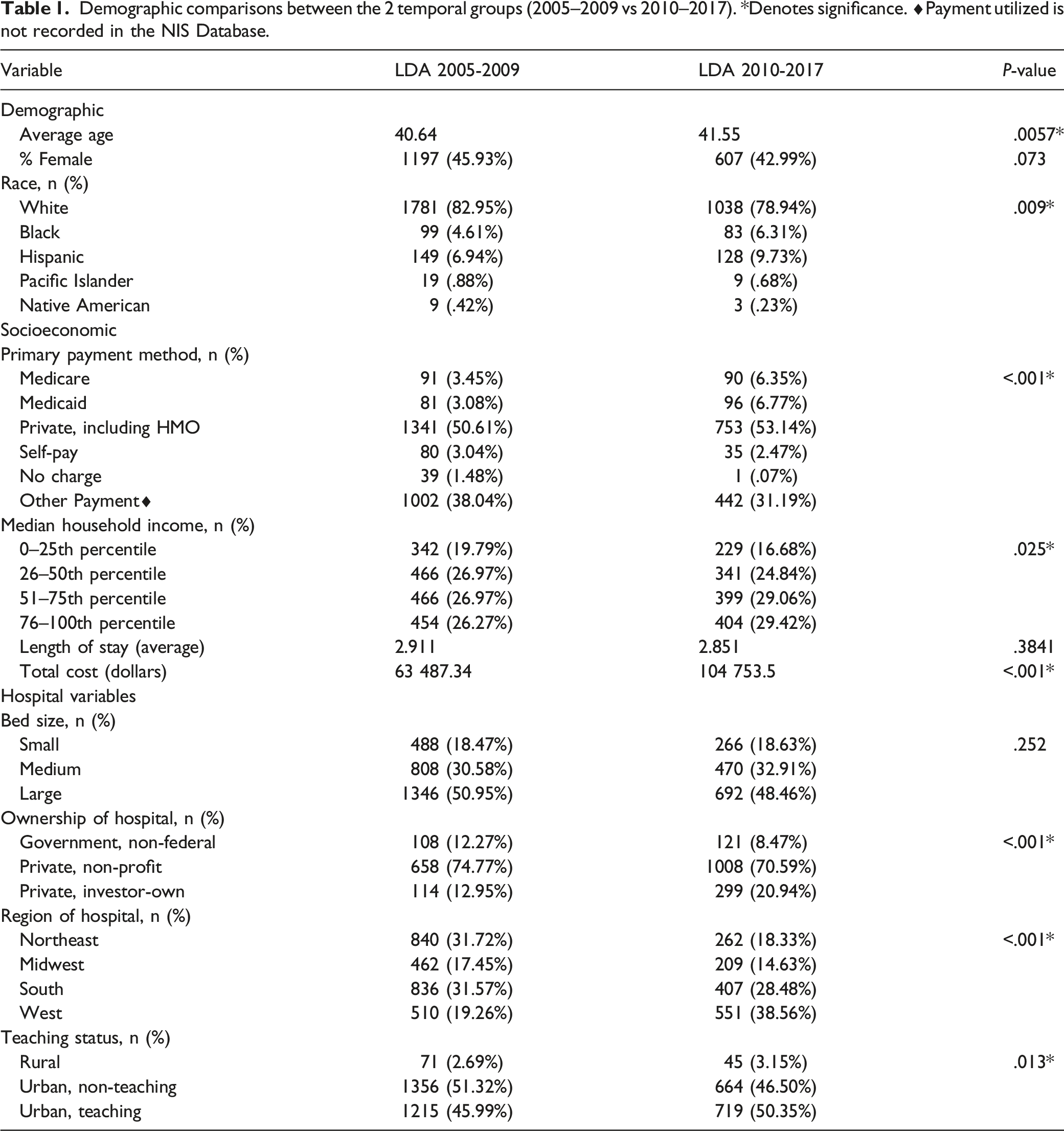
The region of hospital location performing LDA displayed significant differences across both temporal periods as well. Hospitals in the Northeast, Midwest, and South demonstrated significant decrease in LDA incidence (P < .001) (Table 1). By contrast, the number of LDA procedures performed in the West remained relatively constant before and after 2010.
Lastly, the two temporal cohorts demonstrated similar diagnosis codes indicated for LDA, with the top four ICD diagnosis codes the same in both temporal groups. The two most common ICD codes for both cohorts were 72 252, Degeneration of Lumbar or Lumbosacral Intervertebral Disc, and 72 210, Displacement of Lumbar Intervertebral Disc without Myelopathy.
Discussion
In the present study, we found that the rate of LDA decreased by 82% from 2005 to 2017. There was an initial increase in utilization after FDA approval from 2005 to 2006, followed by a plateau from 2006 to 2009. After 2009, there was a steep decline until 2013, after which the utilization stayed relatively stable. This is in comparison to rates of CDA, which exponentially increased over the same time period. There was a significant decrease in LDA utilization in the Northeast, Midwest, and South, while utilization in the West remained relatively constant when comparing 2005–2009 and 2010–2017. The relatively constant use in the West may be due to several high volume centers in that region and a difference in marketing and visibility. However, this is not possible to analyze based on the structure of the NIS dataset. From 2010 to 2017, there was a relative increase in utilization of LDA in Black and Hispanic patients, patients with mean household income above the 50th percentile, and teaching hospitals. Cost of the procedure also increased over the study period.
Several other studies have looked at national trends of LDA. Saifi et al. also used the NIS database to look at trends of primary and revision LDA from 2005 to 2013. 30 They found that over this time period, primary LDA decreased 86% from 3059 procedures in 2005 to 420 in 2013. In our study, we found a similar decrease in utilization of 82% from 2005 to 2017, with a plateau in utilization from 2013 to 2017. Since the publication of Saifi et al.’s data, we found that there has not been a significant change in LDA utilization per year. Awe et al. 31 assessed the effects of LDA on surgical management of lumbar DDD from 2000 to 2008, and found that LDA only comprised 2% of lumbar spine surgeries over the study period. In addition, they found that LDA decreased from 2005 to 2009, while the total number of lumbar fusions increased. A similar study by Yoshihara et al. looking at surgical treatment of lumbar DDD found increasing rates of surgical management form lumbar DDD, with a significant increase in number of fusions performed; however, population-adjusted incidence of LDA did not change over their study period. 32 Our results, using the most recent NIS data available, confirm the conclusion noted in these aforementioned studies whereby rates of LDA have decreased since initial FDA approval, with a relative plateau at around 600 cases per year from 2013 to 2017.
The sharp decline in LDA utilization, starting in 2009 and plateauing in 2013 can possibly be explained by several factors, most important of which may be clinical outcomes. Initial randomized control trials showed promising results after LDA. In 2004 and 2005, 2-year results were published comparing LDA to lumbar fusion and demonstrated equivalent outcomes and complication rates to fusion, but better overall patient satisfaction after LDA.33,34 These results may have driven some of the initial enthusiasm for LDA as higher LDA incidence was noted in the earlier temporal cohort (2005–2009). Data regarding adjacent segment degeneration after LDA has been mixed and a systematic review in 2008 supported the lowest tier of recommendation for arthroplasty versus fusion to decrease adjacent segment disease rates. 19 Several papers discussing the complication profile and revision risk were published between 2006 and 2010 which may partly explain the significant decline in LDA utilization noted in 2009–2010.28,35-37
In part, due to the clinical studies citing complications, equivalent outcomes, and strict inclusion criteria, Medicare began denying coverage for LDA in 2007, citing that it was neither necessary nor reasonable in patients over the age of 60. 38 Other insurance companies followed suit, with some large insurance companies completely denying coverage and others having stringent inclusion criteria.39-41 The lack of clear evidence to support the superiority of clinical outcomes comparing LDA versus fusion, the possibly increased revision and complication risk compared to fusion, and the subsequent difficulty in obtaining insurance authorization for LDA are likely major contributing factors to the significant decline seen in LDA utilization starting in 2009–2010 as well as the overall 82% decrease in LDA utilization from 2005 to 2017.
While LDA was FDA approved before CDA, the incidence of LDA utilization has demonstrated a nearly opposite trend in comparison to CDA based on the results of this study. Studies on CDA have demonstrated mostly non-inferior or superior results to anterior cervical decompression and fusion (ACDF) with regards to clinical outcomes and lower rates of adjacent segment disease.42-46 The data on LDA, as previously mentioned, has been less consistent and is likely a major contributing factor to the opposite utilization trends of the two procedures. In addition, the indications for CDA continue to expand beyond the initial FDA IDE trial inclusion criteria. Recent studies are now examining the efficacy of CDA in patients with cervical spondylosis, myelopathy, or kyphotic alignment, and the expansion of indications is developing growing interest given the relatively consistent outcomes noted in the initial FDA IDE studies now with long-term follow-up.47-50 While the indications for CDA continue to expand, the indications for LDA remain relatively narrow, and generally consist of patients aged 18–60 with symptomatic DDD in one level from L4-S1, refractory to nonoperative management. A paucity of studies attempting to expand the use of LDA to patients with two-level disease and mild facet arthrosis exist,51,52 but overall, the indications remain fairly limited, in comparison to CDA.
While the results of this study demonstrate significant temporal findings, the study has several limitations. Firstly, this is a national database study, and granular patient data is lacking. This leaves our study susceptible to bias and errors associated with the use of administrative databases for clinical analysis. 53 In addition, reasons for the decreasing trend can only be assumed and not directly reported. Secondly, database studies are reliant on medical coders and are vulnerable to human error. Thirdly, the NIS database is an inpatient-only database, and therefore patients who underwent same day surgery were not captured in our estimates.
In conclusion, LDA utilization decreased 82% from 2005 to 2017, which is in exact opposition to CDA trends over the same time period in the same population. The reasons for this declining popularity are likely due to inconsistent clinical results, difficulties with insurance authorization, concerning complications, and narrow inclusion criteria without recent studies attempting to expand the indications for LDA, as has been seen with CDA.
Footnotes
Declaration of Conflicting Interests
Emily S. Mills, Tara Shelby, and Gabriel J. Bouz have no conflicts to declare. Raymond J. Hah is a paid consultant for Nuvasive. He is on the editorial boards for Global Spine Journal, Clinical Spine Surgery, and The Spine Journal. Jeffrey C. Wang receives royalties from Biomet, Seaspine, and Synthes. He owns investments or options in Bone Biologics, Pearldiver, Electrocore, and Surgitech. He is on the Board of Directors for AO Foundation, Society for Brain Mapping and Therapeutics, and the American Orthopaedic Association. He is on the editorial board for Spine, The Spine Journal, Clinical Spine Surgery, and Global Spine Journal. His institution receives fellowship funding from AO Foundation. Ram K. Alluri is a paid consultant and receives royalties from HIA Technologies Incorporate.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.