
Abstract
Study Design
Retrospective cohort study.
Objectives
(1) To compare the risk of Spinal Epidural Hematoma (SEH) associated with specific pre-operative and post-operative anticoagulation (AC) and antiplatelet medications (APM). (2) To define the incidence of SEH and identify risk factors for SEH in our population.
Methods
Thoracolumbar surgeries between October 2009 and March 2020 were collected. Patients who underwent incision and drainage of a symptomatic SEH were identified. AC and APM was recorded 14 days pre-operatively and post-operatively. Demographics and intra-operative factors were recorded. Relative risk with 95% confidence interval was used, with Bonferroni-corrected P-values <.05 used for significance.
Results
9307 surgeries were identified. 177 (1.9%) patients returned to the OR within 30 days, 37 of whom (.39%) returned due to SEH. Seven patients were on either AC or APM pre-op, and sixteen post-op. Five were on aspirin pre-operatively (RR 3.2, 95% CI 1.25–8.22, P = .015). Risk was not increased in patients on multiple agents. No AC or APM demonstrated increased risk of hematoma post-operatively, despite trends toward significance with multiple agents. The use of a drain and complicated hypertension were associated with increased risk of SEH.
Conclusions
Pre-operative aspirin is associated with increased risk of SEH, even when appropriately discontinued. Appropriately dosed post-operative anticoagulation does not increase the risk of SEH, though being on multiple agents trends toward statistical significance and should be better studied. Surgeons should be vigilant and carefully monitor patients on pre-operative antiplatelet medications for spinal epidural hematoma.
Keywords
Introduction
Spinal epidural hematoma (SEH) is a rare but devastating clinical entity which can occur either spontaneously or in the post-operative setting. SEH was first described in 1682 by G. J. Duverney and first diagnosed clinically in 1869 by Jackson, however, operative management was not described until 1911.1,2 It is marked by severe axial back pain at the site of the hematoma with radiation into the extremities, followed by progressive sensory deficits, motor deficits, and urinary retention. Motor deficits usually come in the form of flaccid paralysis and hyporeflexia. Symptom onset can vary widely from 3 hours to several days, and if decompression is not performed in an expeditious manner, permanent disability can result.2,3
Spontaneous and post-traumatic SEH are significantly more common than post-operative SEH, representing about 1% of all space occupying lesions in the spine. 4 The body of literature surrounding their incidence, risk factors, and outcomes is therefore more complete than their post-operative counterparts.5,6
Several studies have demonstrated that the overall incidence of asymptomatic post-operative SEH is high, ranging from 33 to 100% in MRI-based studies.7-9 The incidence of clinically significant post-operative SEH, however, is much lower, with estimates ranging from .1 to .24%.10-16 Risk factors include pre-operative coagulopathy, history of previous spinal surgery, and multilevel surgery.10,11 Other risk factors identified in a large database study by Awad et.al. included pre-operative NSAIDS, Rh-positive status, age >60, intra-operative blood loss>1L, Hemoglobin <10g/dL, >5 levels, and supratherapeutic post-operative anticoagulation. Drain use and well controlled post-operative anticoagulation did not increase the risk of SEH, however, hypertension, high drain output, and the use of gelfoam to cover the dura have all been found to be associated with an increased risk.17,18
There is not, to our knowledge, any literature looking at specific anticoagulation (AC) or antiplatelet medications (APM) and how they relate to SEH. In our experience, those patients recently on APM like aspirin or clopidogrel, even if appropriately discontinued, tend to “ooze” more than those on AC. The primary goal of this study is to identify the effect that APM has on the risk of SEH and compare it to other AC, both pre-operatively and post-operatively. Our hypothesis is that APM will confer a higher risk of post-operative hematoma compared to AC that do not interfere with platelet function. Secondary goals include defining the incidence of post-operative SEH in our cohort and identifying additional risk factors that portend a higher risk for developing SEH.
Materials and Methods
Approval was obtained from our hospital system IRB prior to case collection, approval number EH17-292. This project received an exemption from the IRB for informed consent, therefore, informed consent was not obtained. All decompressions and fusions of the thoracolumbar spine between October 2009 and March 2020 were identified based on the CPT and OR procedure codes included in the supplementary files. All cases were performed by board certified spine surgeons in a private suburban hospital system which includes 4 hospitals and a surgery center. Surgeons were from both the department of neurosurgery and orthopedic surgery. Initially, we identified all patients who returned to the OR within 30 days of the index surgery. From these, we then identified all cases concerning for post-operative epidural hematoma through a diagnosis of hematoma complicating a procedure (ICD-9 code 998.12). This was confirmed by manual chart review.
Data collected for each patient included age, sex, BMI, ASA class, operative levels, estimated blood loss, operative time, use of a drain, medical comorbidities, smoking status, and alcohol consumption. Any pre-operative or post-operative AC (enoxaparin, heparin, or warfarin) or APM (aspirin or clopidogrel) was recorded for each patient.
Patient demographics were reported as a mean for continuous variables and a percentage for categorical variables. Relative risk was calculated for each AC or APM, and statistical significance was determined based on 95% confidence intervals and Bonferroni-corrected P-values. Similar analysis was performed for gender, drain use, and elixhauser comorbidities.
Results
Incidence and Demographics
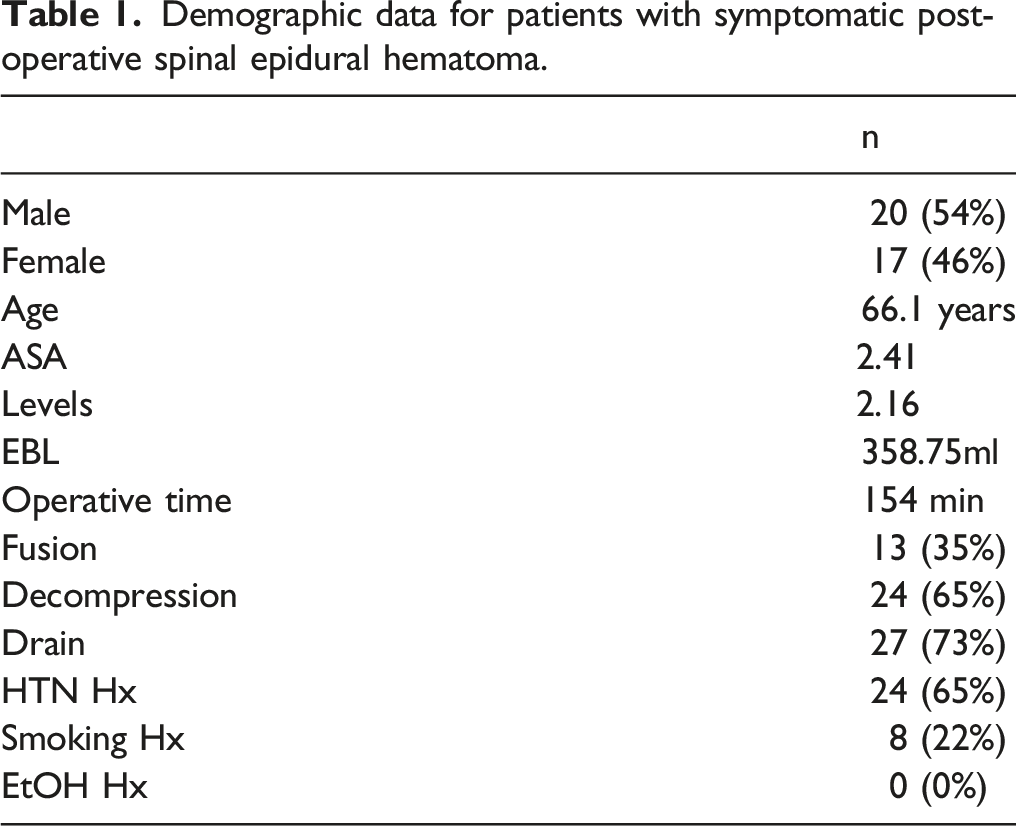
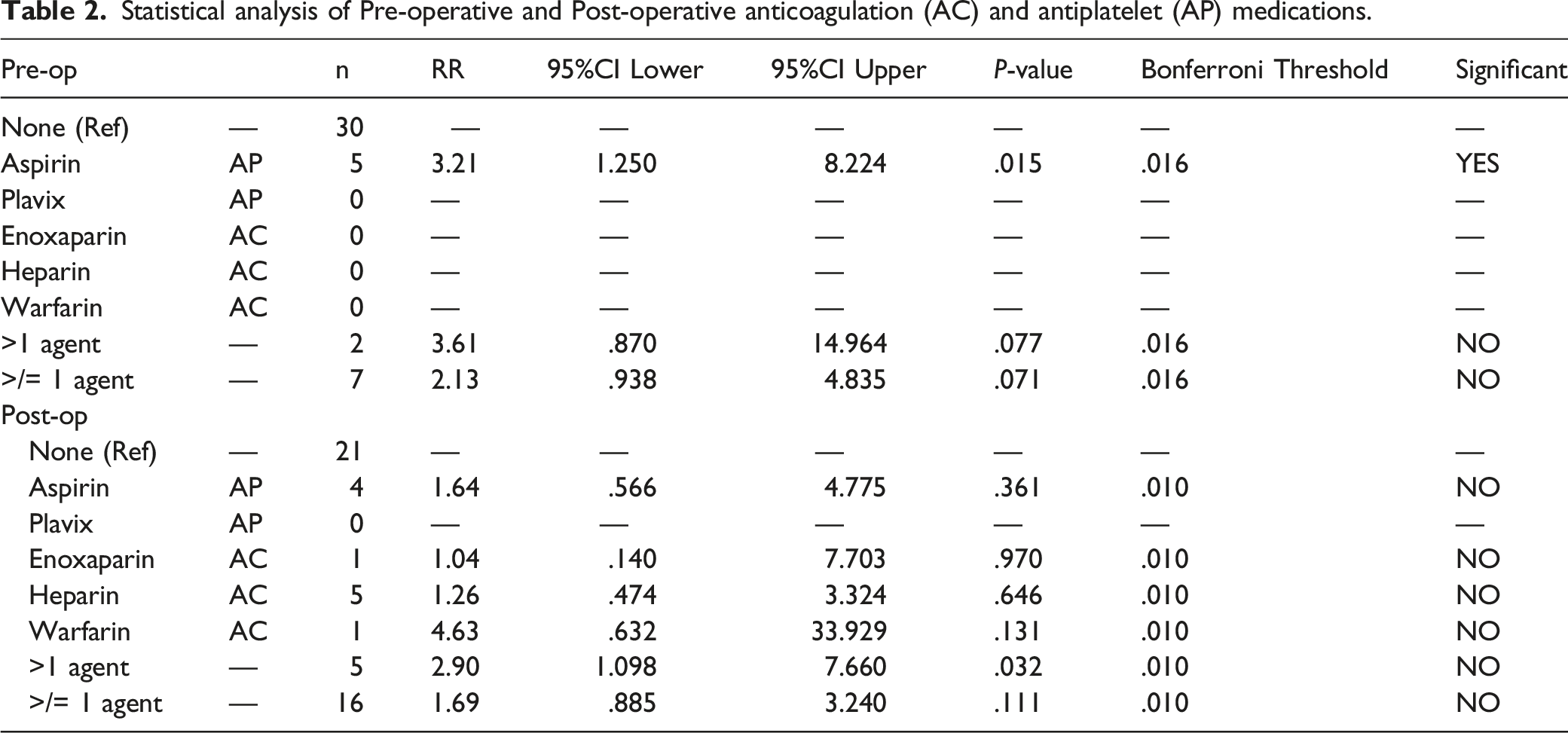
9307 thoracolumbar spinal operations were performed by either the senior author or one of 20 board certified spine partners practicing in the hospital system from October 2009 to March 2020. Of the 9307 cases, 177 (1.9%) patients returned to the OR within 30 days of the index surgery. Of these, the reason for reoperation was incision and drainage of a symptomatic post-operative epidural hematoma in 37, corresponding with in an incidence of .39% (Figure 1). In our SEH cohort, there were 20 males (54%) and 17 females (46%). 24 patients underwent decompression alone, while 13 underwent decompression and fusion with or without instrumentation. 27 patients had at least one drain placed post-operatively, and 2 of these 27 patients were sent home with a drain with plans to pull in the office. 24 patients had a diagnosis of hypertension. 8 patients were current smokers, and none endorsed alcohol intake greater than 2 drinks per day (Table 1). The breakdown of pre-operative and post-operative AC/APM can be found in Table 2. Five patients were on APM alone prior to surgery, while 2 patients were on more than one agent. After surgery 4 patient were on APM alone, while 7 were on some form of AC and 5 were on greater than one agent. In all cases, AC/APM was appropriately discontinued a full 7 days prior to surgery, confirmed through their pre-operative history and physical and well as pre-operative instructions that were documented in the electronic medical record. Flow diagram illustrating data collection and identification of the 37 patients who underwent incision and drainage for symptomatic post-operative SEH. Demographic data for patients with symptomatic post-operative spinal epidural hematoma. Statistical analysis of Pre-operative and Post-operative anticoagulation (AC) and antiplatelet (AP) medications.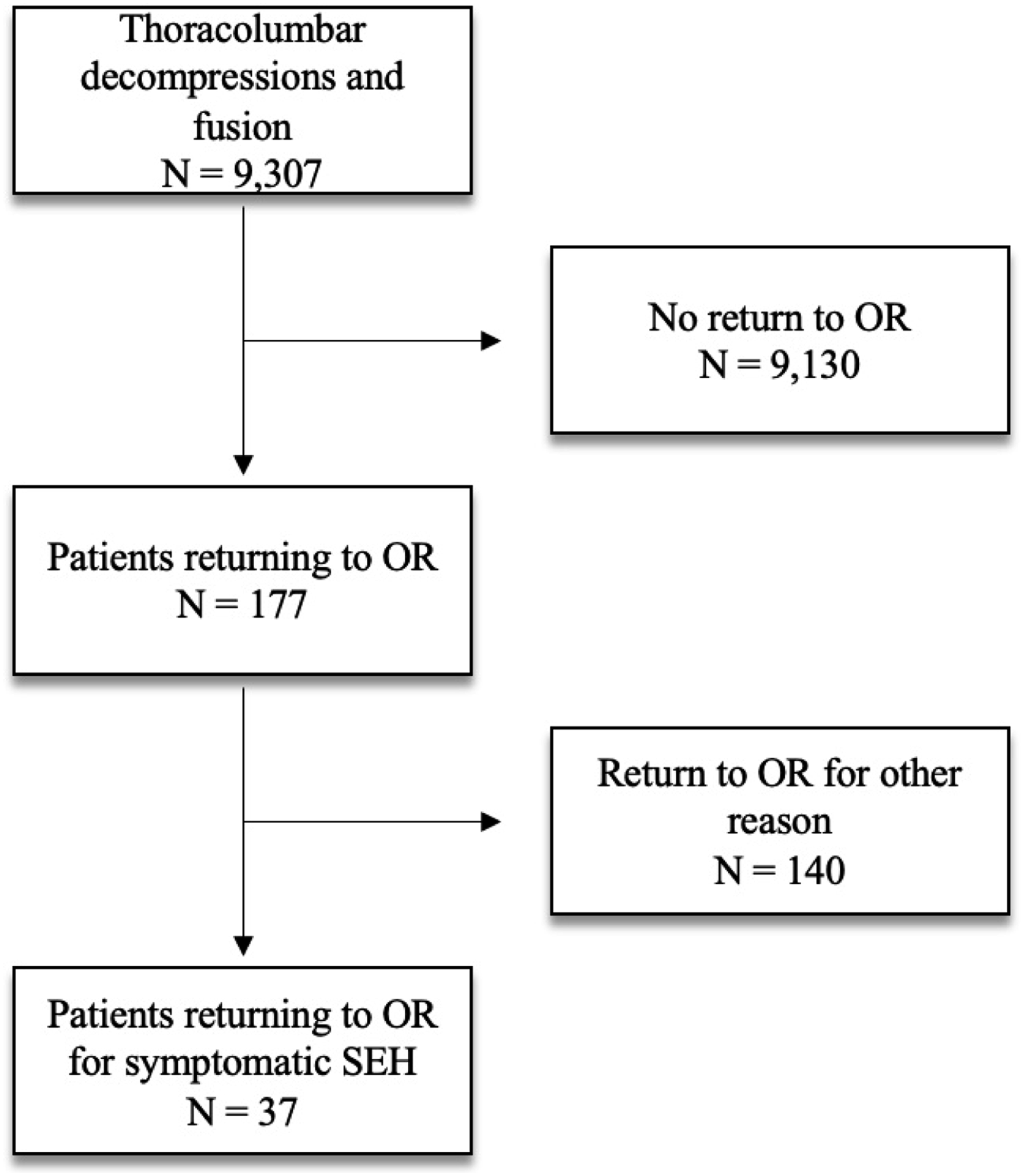
Pre-Operative Anticoagulation
Statistical analysis of the AC/APM can be found in Table 2. Five patients who developed a post-operative hematoma had been on aspirin pre-operatively as a single agent, representing a relative risk of 3.2 (95% CI 1.25–8.22, P = .015). No patients were on clopidogrel, enoxaparin, heparin, or warfarin pre-operatively as a single agent. There were 2 patients who were on greater than one agent pre-operatively. In these patients, the relative risk of developing a hematoma was 3.61 (95% CI .93–4.84, P = .078), so while there was a trend toward an increased risk of hematoma, it fell short of statistical significance, especially when Bonferroni correction is considered. In a similar non-significant trend, patients who were on at least one agent had a relative risk of 2.12 (95% CI .94–4.84, P = .071).
Post-Operative Anticoagulation
Statistical analysis of gender and drain as predictors of post-operative spinal epidural hematoma.

Other Risk Factors
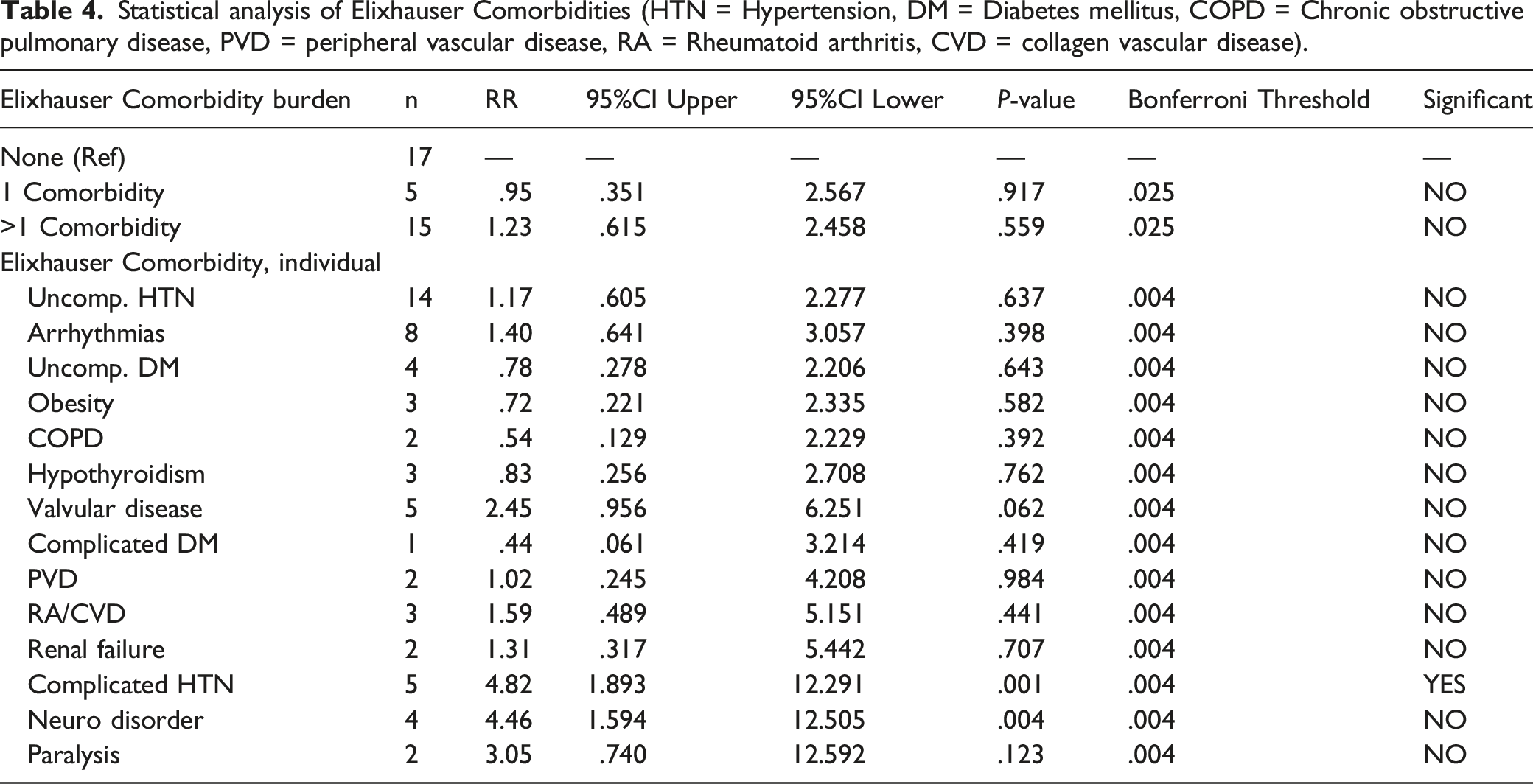
Statistical analysis of Elixhauser Comorbidities (HTN = Hypertension, DM = Diabetes mellitus, COPD = Chronic obstructive pulmonary disease, PVD = peripheral vascular disease, RA = Rheumatoid arthritis, CVD = collagen vascular disease).
Discussion
Post-operative spinal epidural hematoma is a rare complication which can significantly affect patients’ long-term function, and early recognition and decompression is essential to maximize neurologic recovery.3,5 It is therefore useful to understand the risk factors for development of post-operative SEH, as they can be used to dictate and modify peri-operative protocols and will allow the surgeon to better identify those patients who may require closer monitoring.
Current pool of literature concerning risk factors for development of post-operative spinal epidural hematoma.
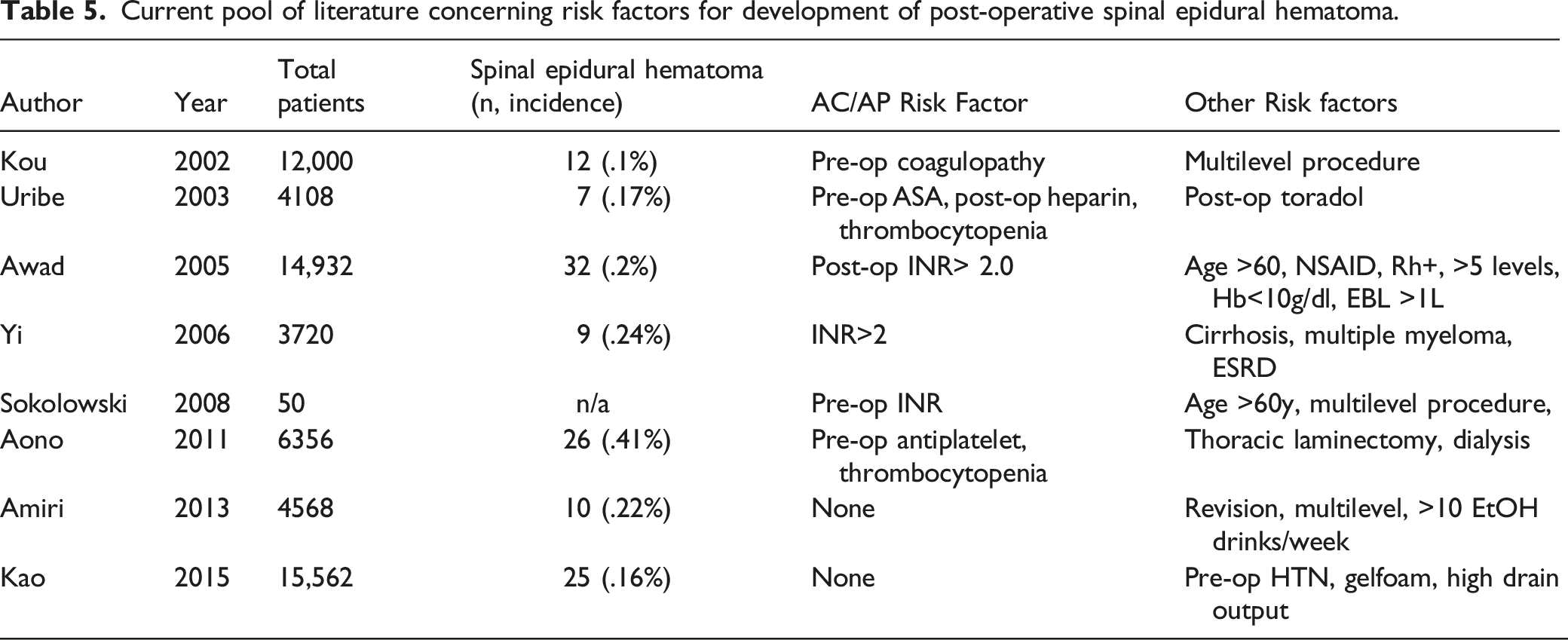
The current study did not find any increase in the risk of SEH for those patients taking well controlled AC. In general, this does seem to support what has been shown previously in the literature, where only poorly controlled anticoagulation with INR >2 increases a patients’ risk for hematoma.12,17,19 Kou was the first to point to pre-operative coagulopathy as a cause of post-operative hematoma in 2002, which was supported by a larger study by Awad in 2005 and another small study by Yi in 2006.10,12,17 Sokolowski was able to correlate the size of asymptomatic post-operative hematoma with the INR in a unique MRI-based study. 19
Secondary analysis demonstrated that complicated hypertension was the only comorbidity which carried an increased risk of hematoma. A similar finding was found in a 2015 paper by Kao, where hypertension was identified as an independent risk factor for the development of SEH amongst 15,562 patients with a hematoma incidence of .16%. 18 Intuitively this makes sense given the frequently observed breakthrough bleeding seen when patients’ intra-operative pressures are poorly maintained.
We did find that that the risk of hematoma was increased in patients who had a drain post-operatively. This is likely not a causative relationship, but rather confounded by the fact that drain use is more common in larger multilevel surgeries, as well as those involving fusion and larger EBL. Therefore, we do not believe these findings should dictate the use of a drain. Prior studies which have looked at the effects of drain use have been largely inconclusive. Awad studied multiple risk factors for the development of symptomatic SEH and determined that a drain was neither protective nor detrimental. 17 High drain output has been identified as a risk factor for hematoma formation by Kao, but not the presence of a drain itself, supporting the idea that a drain is likely a confounding factor, used in those surgeries where either the amount of bleeding or the number of levels already place the patient at risk for hematoma. 18
The present study provides a unique addition to the current body of literature on SEH by evaluating the role specific anticoagulation and antiplatelet medication plays in the formation of compressive SEH. While poorly controlled anticoagulation and thrombocytopenia have been previously implicated in the development of SEH, no papers have directly compared the hematoma risk carried by different AC and APM. To the best of our knowledge, this represents the largest number of hematomas identified in any single cohort, which is important for the study of SEH given its extremely low incidence. Additionally, we included multiple surgeons across four hospitals and an outpatient surgery center, adding heterogeneity and generalizability to the study.
There are several shortcomings of this study that could not be overcome based on design. Perhaps the most obvious is the lack of data regarding newer anticoagulants. This is for two reasons. First, during much of the collection period, many of the novel anticoagulants (i.e., Apixaban, rivaroxaban, dabigatran) were not regularly in use, therefore the decision to exclude them was out of a desire to minimize bias. Secondly, due to the inability to monitor and control levels in the peri-operative period, these novel agents are usually discontinued far before surgery and replaced by one of the monitorable anticoagulants in the peri-operative period if anticoagulation is deemed medically necessary. Therefore, they seldom are found as an active medication during chart review of the peri-operative period. Additionally, due to the retrospective and non-randomized nature of the study, there is always the possibility that unidentified confounders might be introduced. Finally, due to the low incidence of SEH, there were several situations where specific anticoagulants fell just short of statistical significance. To conclude definitively that these anticoagulants do not increase risk of SEH is likely inaccurate, and it would require much larger numbers or different study design to make a solid conclusion.
Next steps in the study of SEH might include a further dive into the novel anticoagulants, as several of these agents have been implicated in excessive post-operative bleeding, wound complications, and infection following total joints.20,21 Additionally, there were several trends in this study that fell just shy of statistical significance, most prominently, those patients who were on multiple agents pre-operatively and post-operatively. As mentioned above, this is likely the result of the very low incidence of SEH. Therefore, we would like to see additional investigation into those patients on multiple anticoagulants in a larger study, perhaps a multi-center effort. Alternatively, this may be one subject that could be appropriately studied using a large insurance database, where incredibly large cohorts can be used to study events with very low incidence.
Conclusion
Post-operative SEH is a rare but dreaded complication of spinal surgery which requires urgent decompression to maximize the chances of successful recovery. Despite the low incidence, there have been several factors previously identified which increase the risk of post-operative SEH. Here we demonstrate that pre-operative antiplatelet medication in the form aspirin increases the risk of SEH, even when appropriately discontinued, while anticoagulation does not appear to have the same effect. We confirm the effect that uncontrolled hypertension has on the risk of developing post-operative hematoma and shed additional light on the association of drain use with increased hematoma risk. The surgeon should be extra vigilant with these patients in the post-operative period to observe for signs and symptoms of SEH, and if possible, might consider an extended aspirin drug vacation in these patients to decrease the chances of a serious post-operative complication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Illinois Bone and Joint Institute.
IRB Approval
This study was approved by the NorthShore University Health System IRB, Approval number EH17-292. The device(s)/drug(s) is/are FDA-approved or approved by corresponding national agency for this indication.