
Abstract
Spinal cord infarction (SCI) is a catastrophic neurologic deficit following spine surgery. Because of the opposite management regimens used for SCI and acute epidural hematoma, accurate diagnosis of SCI is of great importance to maximally reserve neurologic functions and improve outcomes. A 21-year-old man developed acute paralysis and sensory deficits of the bilateral lower limbs shortly after undergoing two-stage combined posterior and anterior multilevel en bloc corpectomy. An emergency second-look surgery revealed wide-spectrum blackness of the thecal sac with no signs of an epidural hematoma. The patient underwent anticoagulation therapy, ventilation support, microcirculation perfusion, and fluid optimization. He regained an ambulatory status without other severe complications. Upon discharge, his muscle strength had returned to grade 4 and his Eastern Cooperative Oncology Group performance score had decreased to 0. At the final 48-month follow-up, the implants were in good position without local recurrence, and the patient was able to lead an independent life and work in his full capacity. An epidural hematoma did not appear to be the cause of SCI after spinal tumor surgery in this case; however, SCI was a possible reason for the acute paralysis. Anticoagulation treatment with adjuvant therapies may be an effective option in managing SCI.
Keywords
Introduction
Postoperative neurologic deterioration is a catastrophic complication of spine surgery. Compared with epidural hematomas, spinal cord infarction (SCI) is a relatively rare cause of such neurologic deterioration. 1 Definitive diagnosis and effective management of SCI are challenging but of high priority. However, a therapeutic protocol for SCI is lacking because of the rarity of this condition. We herein report the successful management of acute SCI after multilevel en bloc corpectomy. Related studies are also reviewed.
Case presentation
A 21-year-old man was referred to our center on an emergency basis because of acute loss of ambulatory status. The patient denied any medical history of cancer or coagulation disorders. Physical examination revealed hyperreflexia of the bilateral knees and ankle jerks and a positive Babinski sign. Contrast-enhanced thoracic magnetic resonance imaging (MRI) indicated abnormal signals in the T4–7 vertebral bodies and the T5/6 appendices as well as severe spinal cord compression at the T5/6 levels. Positron emission tomography–computed tomography (CT) showed an isolated high-uptake lesion at T4–7 (standardized uptake value, 13.4) with no visceral malignancy (Figure 1). The patient had a spinal instability neoplastic score of 14 and Eastern Cooperative Oncology Group performance score (ECOG-PS) of 4.

Preoperative images of the patient. (a) Sagittal manifestation of T1-weighted magnetic resonance imaging with contrast enhancement indicated abnormal signals at T4–7. (b) Whole-body positron emission tomography–computed tomography revealed an isolated lesion with high 18FDG uptake at T4–7 with no visceral malignancy.
After a thorough examination and evaluation, emergency T4–7 total laminectomy was performed for effective spinal cord decompression. The patient thereafter exhibited obvious improvements in his ambulatory and sensory status. The pathological report revealed aggressive osteoblastoma (OST+, Ki67 10%+). Fifty days later, the patient underwent four-level en bloc corpectomy with a three dimensional-printed implant and pedicle screw-rod fixation (Figure 2). Somatosensory evoked potential monitoring 2 revealed no abnormal signs during the whole procedure. The patient’s condition remained stable until approximately 18 hours after the operation, at which time he developed weakness of his lower limbs. Physical examination revealed that the muscle strength of the dorsalis pedis and triceps surae had decreased to grade 1 with significant weakening of ankle reflection. The patient’s body temperature was 37.3°C, and his blood pressure was normal (105/71 mmHg). He did not have polypnea (his respiratory rate was 20 breaths/minute), and his pulse was regular (80 beats/minute). The drainage tube was unobstructed and produced 120 mL of dark red bloody fluid. Urgent laboratory tests demonstrated a fibrinogen concentration of 1.78 g/L (reference range, 2.0–4.5 g/L), D dimer concentration of 3880 µg/L (<500 µg/L), and fibrinogen degradation product concentration of 9.7 mg/L (<5.0 mg/L). No deep venous thrombosis was detected in the lower limbs by B-mode ultrasound. The patient did not undergo an emergency MRI examination because of his critical weakness.

Intraoperative image of circumferential reconstruction with utilization of a pedicle screw-rod system and customized three-dimensional-printed prosthesis.
An urgent second-look surgery was conducted because of a suspected acute epidural hematoma, which is a major complication after spine surgery that causes postoperative neurologic deterioration. 3 However, wide-spectrum blackness of the thecal sac was detected with no evidence of an epidural hematoma (Figure 3). Low-dose anticoagulation therapy was administered using fraxiparine (2850 IU/day subcutaneously) in conjunction with ventilation support, microcirculation perfusion, and fluid optimization. Sulperazone was administrated according to the manufacturer’s instructions to prevent infection, and adequate nutritional support therapy was conducted to maintain the nitrogen balance. Upon discharge after 1 week of uneventful treatment, the patient’s muscle strength had returned to grade 4 and his ECOG-PS had decreased to 0. At the 12-month follow-up, CT revealed that the implants were in good position without local recurrence (Figure 4). At the 48-month follow-up, bony fusion was present between contacts as shown by contrast-enhanced CT (Figure 5), and the patient led a normal life and returned to work in his full capacity. Based on the findings throughout the 4-year follow-up, the initial neurological deficit did not impose a negative impact on the patient’s long-term outcomes.

Wide-spectrum blackness of the thecal sac during the emergency second-look operation.

Radiographic images at the 12-month follow-up. The X-ray examination (anteroposterior and lateral) and computed tomography scan (sagittal and coronal) showed that the hardware was in a good position with no failure.
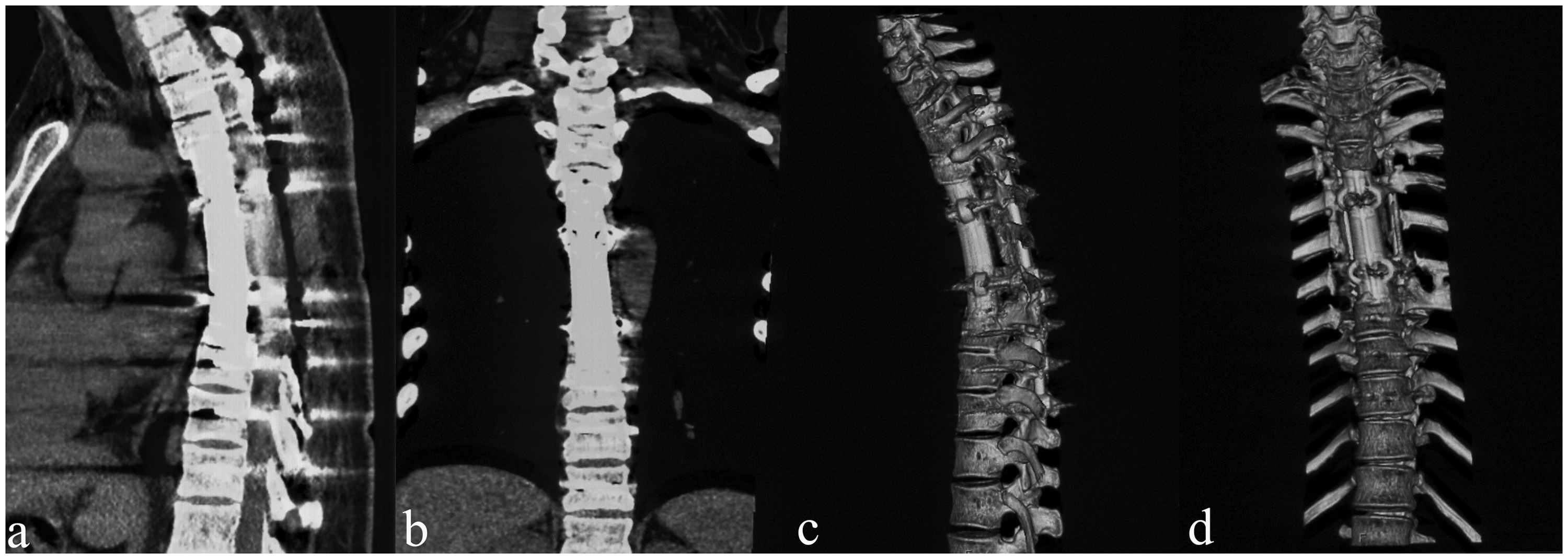
Radiographic images at the 48-month follow-up. The computed tomography scan (sagittal and coronal) and reconstruction images indicated favorable bony fusion of the contact surface between T3 and T8.
Discussion
SCI is a devastating disease that accounts for 1% of all strokes. 4 Like aortic surgery, spine surgery is a common cause of SCI. Although an acute epidural hematoma is the most significant cause of postoperative neurologic deterioration, SCI cannot be overlooked in operations involving multilevel procedures. The most significant manifestation of SCI is loss of motor function, which partly presents as anterior spinal artery syndrome. 5 Table 1 shows the relevant publications1,6–9 reporting the diagnosis and/or treatment of SCI after spine surgery. As shown in the table, the cervical spine is the region most commonly affected by SCI after surgery, and hypotension is the most direct risk factor resulting in SCI. The number of involved segments is associated with the probability of SCI. Ischemic SCI may occur if four or more consecutive segmental arteries are interrupted.10,11
Published studies of spinal cord infarction after spine surgery.

MRI, magnetic resonance imaging; M, male; F, female; OPLL, ossification of posterior longitudinal ligament; LE, lower extremity; UE, upper extremity.
The differential diagnosis between an epidural hematoma and SCI is of great importance because the treatments of these two conditions are completely opposite. The definitive diagnosis of SCI requires high-resolution and consecutive MRI, which reveals T2 hyperintensity in the ischemic area (central cord more than peripheral cord).12,13 Additionally, the typical signs of “owl’s eyes” or “snake eyes” can be detected on T2 transverse MRI if the infarction is restricted to the gray matter of the anterior horn. However, the detection rate is only 67% of all suspected cases. 12 Moreover, some patients might fail to undergo an MRI examination because of their urgent situation and critical weakness. Therefore, an emergency second-look operation should be considered in such cases because of the low detection rate of SCI by MRI. In the present case, the patient’s critical condition did not allow us to conduct MRI to detect possible intramedullary changes. Alternatively, an exploratory surgery was performed to determine the cause of his symptoms, and a clinical diagnosis was made based on his chief complaints, physical examination findings, laboratory test results, and blackness of the thecal sac found during the surgery.
Because a standard therapeutic protocol is lacking, treatment of SCI is mainly based on the guidelines for acute ischemic stroke resulting from cerebral ischemia and spinal cord injury.14,15 The key treatment focuses on the prevention of secondary infarction. Anticoagulation therapy using heparin for thromboprophylaxis is recommended for at least 3 months after spinal cord injury. 16 Other treatments include supportive ventilation management, optimized microcirculation perfusion, and control of vital signs such as body temperature and blood pressure. Corticosteroid usage remains controversial given the lack of evidence-based studies. One multicenter study showed that the outcomes of SCI were associated with the initial severity of the neurological deficits. 17
Conclusions
This case illustrates the possibility of acute SCI after multilevel spine surgery. Exclusion of an acute postoperative epidural hematoma warrants MRI examination and second-look surgery. Anticoagulation therapy and intensive care are urgently required for thromboprophylaxis.
Footnotes
Ethics approval and consent to participate
The reporting of this study conforms to the CARE guidelines. 18 This study was approved by the Institutional Review Board of Changzheng Hospital, and written informed consent was obtained from the patient. The corresponding author had full access to all the data and the final responsibility to submit for publication.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by a grant from the National Natural Science Foundation of China (grant no. 82072971). The funding source had no role in the study design; data gathering, analysis, and interpretation; writing of the report; or the decision to submit the report for publication.