
Abstract
Study Design
Case report.
Objectives
To describe a case of delayed-onset spinal hematoma following the breakage of a spinal epidural catheter.
Methods
The authors describe the clinical case review.
Results
A 64-year-old woman had undergone epidural anesthesia 18 years before she was referred to our hospital because of lower-back pain and lower neurologic deficit with leg pain. The clinical examination showed the presence of a fragment of an epidural catheter in the thoracolumbar canal, as assessed by computed tomography, and a spinal hematoma that compressed the spinal cord at the same spinal level, as assessed by magnetic resonance imaging. Surgical removal of the epidural catheter and decompression surgery were performed. The patient exhibited substantial clinical improvement 1 month after surgery; she achieved a steady gait without the need for a cane and had no leg pain.
Conclusion
This is the first report of delayed onset of spinal hematoma following the breakage of an epidural catheter. Generally, when the breakage of an epidural catheter occurs without symptoms, follow-up alone is recommended. However, because spinal hematoma might exhibit a late onset, the possibility of this complication should be considered when deciding whether to remove the catheter fragment. We believe that in our patient, there could be a relationship between the catheter fragment and subdural hematoma, and catheter breakage could have been a risk factor for the spinal hematoma.
Introduction
Epidural analgesia is commonly used for perioperative anesthesia, postoperative pain control, chronic pain, and cancer-related pain. 1 , 2 Epidural catheters are mostly inserted or removed without complications. However, breakage of epidural catheters occurs, albeit rarely, because of inflicted trauma during the insertion or removal procedures. 1 , 3 , 4 , 5 , 6 , 7 , 8 , 9 To our knowledge, this is the first report of delayed-onset spinal interdural hematoma following epidural catheter breakage; we also discuss its management.
Case Report
History and Examination
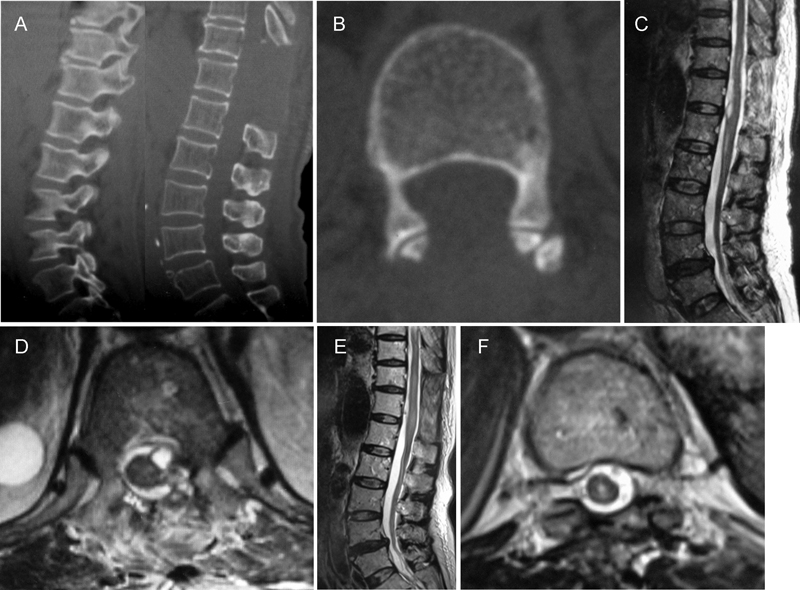
A 64-year-old woman presented with lower-back pain. She had visited another hospital and had undergone lumbar radiography. The following day, her severe lower-back pain worsened, and she presented neurologic motor and sensory deficit in both legs. She went to another general hospital, where thoracolumbar computed tomography (CT) acquired in the sagittal and axial views showed a foreign material in the spinal canal between T11 and L1 (Fig. 1). In addition, the foreign body exhibited a large loop on the left side of the spinal canal. As spinal disease caused by a foreign material was suspected, she was immediately transferred to our hospital for examination by spinal surgeons.
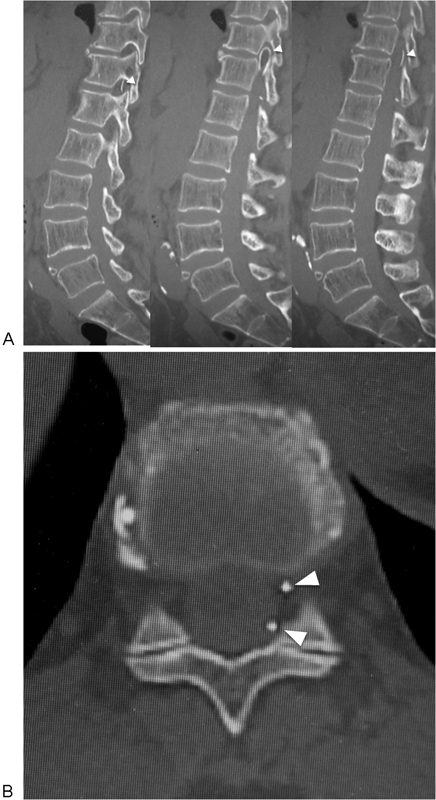
Computed tomography scan of the thoracolumbar spine. The images show a foreign looped material (arrowhead) located between T11 and T12 in the spinal canal on sagittal views (A) and axial views (B).
At the time of presentation to our hospital, the patient was unable to walk because of severe sciatica and paralysis (manual muscle testing [MMT], 2 to 4/5) of her lower limb, without clear rectal disturbance. Her Japanese Orthopedic Association (JOA) score was 2/29. 10
She had a history of hypertension, rheumatoid arthritis, and arrhythmia. In addition, she had a history of ileal conduit diversion performed under epidural anesthesia 18 years prior to this incident. She had also been taking an anticoagulant drug (aspirin) for over 9 years.
Magnetic resonance imaging (MRI) of the spine was performed (Fig. 2). Sagittal T1- and T2-weighted images acquired on the day of admission revealed a mass lesion (diameter, 12 mm) that extended from T12 to L1; this mass presented a low signal that was similar to the spinal cord signal on the T1-weighted images and a high signal on the T2-weighted images. The axial T1- and T2-weighted images showed that this mass was localized on the left side of the spinal canal and displaced the spinal cord toward the right, with normal positioning of the epidural fat. The MRI performed on the day after admission showed that the hyperintense area became hypointense on axial T2-weighted images. Moreover, contrast-enhanced MRI showed no contrast enhancement at the lesion. The hyperintense area corresponded to the cerebrospinal fluid that encircled the hematoma, and no centromedullary edema and perimedullary dilated vessels (flow void findings) were observed on T2-weighted and contrast-enhanced MRIs. Thus, it was defined as a spinal hematoma due to a residual broken catheter retained 18 years before. In addition, blood examination on the day of admission did not show any abnormality. Specifically, her prothrombin time international normalized ratio was normal (0.98).
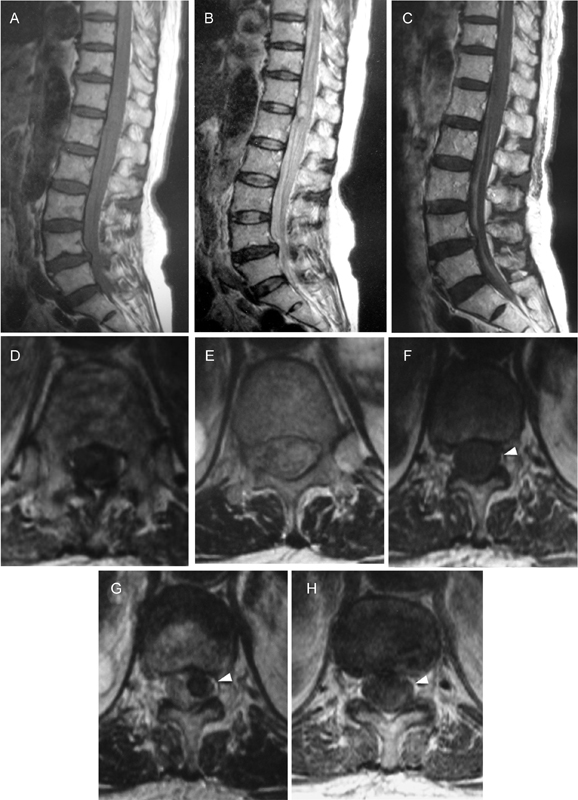
Sagittal T1-weighted (A) and T2-weighted (B) magnetic resonance images (MRIs) acquired on the admission day reveal a lesion (diameter, 12 mm) at T12–L1 that presented as a low-signal mass, similar to the spinal cord signal, on a T1-weighted image (A) and a high-signal mass on a T2-weighted image (B). Axial T1-weighted (D) and T2-weighted (E) images acquired on the admission day reveal a low-signal mass on a T1-weighted image and a high-signal mass on T2-weighted images; the mass was localized on the left side of the spinal canal and displaced the spinal cord toward the right. An axial T1-weighted (F) image acquired on the second day after admission reveals a low-signal mass that was similar to those seen on images acquired on the previous day. However, a T2-weighted (G) image acquired on the second day after admission demonstrates a change from high to low signal intensity, with normal positioning of epidural fat (arrowhead). On the contrast-enhanced T1-weighted MRI (C, H), there is no enhancement of the lesion. In addition, no centromedullary edema and perimedullary dilated vessels (flow void findings) were observed on any T2-weighted and contrast-enhanced MRIs.
Treatment
First, she had motor dysfunction with MMT 2 to 3 in both legs, and hence, we considered conservative treatment and observed her neurologic states. Her neurologic dysfunction improved only very slightly in the few days after the onset. Thus, we decided to remove the catheter and evacuate the hematoma. On the sixth day after admission, a laminectomy from T11 to L1 was performed. We located and removed the fragment of the epidural catheter with the surrounding granulation formation (Fig. 3). However, there was no epidural hematoma. Intraoperative ultrasonographic examination showed the presence of a hyperechoic lesion located dorsal to the spinal cord in the sagittal view and around the spinal cord in the axial view, but the spinal cord was decompressed completely (Fig. 4). Thus, we established a diagnosis of subarachnoid hematoma or subdural hematoma and concluded that the removal of the lamina without durotomy decompressed the spinal cord sufficiently. Additional examination of the catheter removed from the patient showed that it was cut by something sharp.
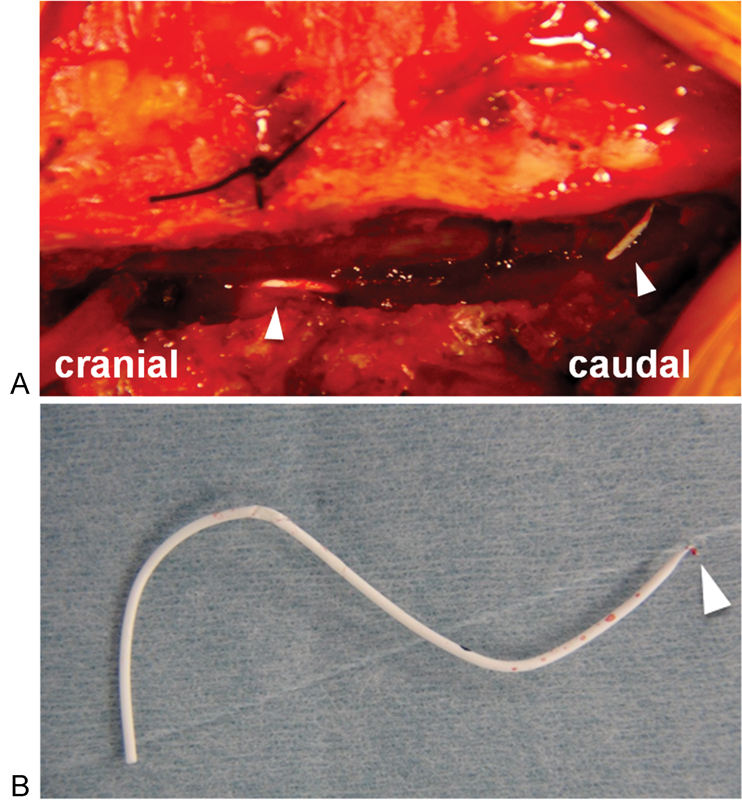
Intraoperative photographs. After removal of the lamina, the fragment of the broken epidural catheter was exposed next to the T12 pedicle (A). The fragment of catheter was removed from the spinal canal (B). The arrowhead indicates the tip of the breakage.
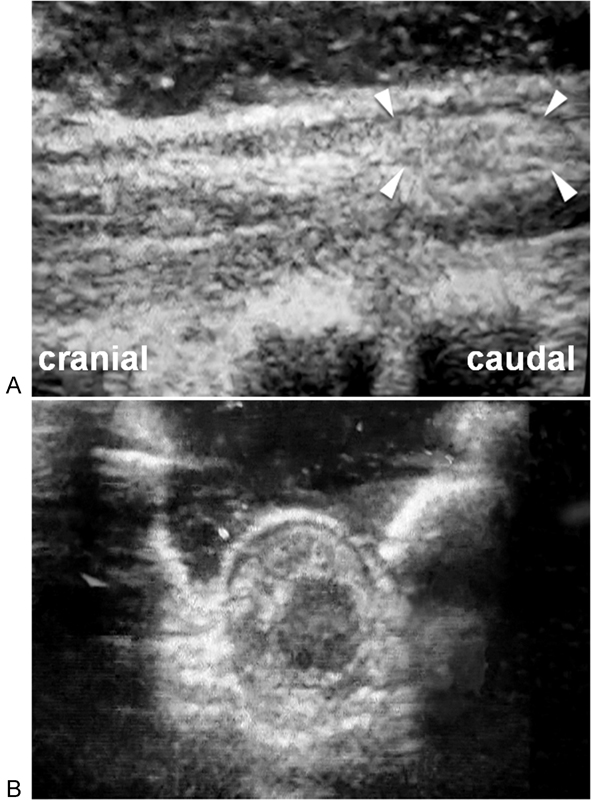
Intraoperative ultrasonographic images obtained in the sagittal (A) and axial (B) views. A hyperechoic lesion is located dorsal to the spinal cord (arrowhead) in the sagittal image (A) and around the spinal cord in the axial image (B).
Postoperatively, there was good improvement in her severe leg pain and motor deficit. Four days after the operation, her leg pain improved to two-tenths of her maximum pain, and her paralysis improved gradually. She also started training to walk. On postoperative day 10, she exhibited motor improvement (MMT 4/5) in her legs and achieved a steady gait using a cane. One month after the operation, her gait was stable without the use of a cane, and her JOA score improved to 19/29. MRI 3 days after the surgery showed no evidence of the catheter fragment and expansion of the dura and subarachnoid space due to laminectomy, but some subdural hematoma remained. Postoperative MRIs acquired 2 months after the surgery showed that the hematoma had disappeared (Fig. 5). At postoperative 3 months, she had no leg pain, but slight numbness persisted in the foot region.
Computed tomography scan of the thoracolumbar spine obtained 2 months after the operation. Sagittal view (A) and axial view (B) demonstrating the removal of the fragment of the epidural catheter. Postoperative magnetic resonance images (MRIs) 3 days after surgery show the absence of the catheter fragment and the expansion of the dura and subarachnoid space due to laminectomy; however, some subdural hematoma remained ventral to the spinal cord in a sagittal T2-weighted view (C) and in a T11–T12 axial T2-weighted view (D). Postoperative MRIs acquired 2 months after the surgery show sufficient decompression and disappearance of the hematoma in a sagittal T2-weighted view (E) and in a T11–T12 axial T2-weighted view (F).
Discussion
Breakage and retention of an epidural catheter happens rarely, with an estimated frequency of 0.0017 to 0.04%. 11 , 12 In addition, few reports have documented complications resulting from residual broken epidural catheters (Table 1). 4 , 6 , 8 Blanchard et al reported a 34-year-old woman with L3 root nerve syndrome because of a residual catheter. 4 Staats et al reported a 64-year-old man who presented pain and lower-extremity weakness resulting from the compression of the thecal sac by a catheter fragment in the spinal canal; this fragment was retained from a surgery performed 18 months before. 8 Demiraran reported a 25-year-old man who exhibited swelling in the lumbar region and presented subcutaneous effusion due to a residual epidural catheter. 6 In two of these cases that presented neurologic deficit, 4 , 8 the symptoms had presented more than 6 months after the primary operation and worsened gradually. Fortunately, in all three cases, the symptoms improved after the removal of the broken epidural catheter. The present report differs significantly from the previous reports in that: (1) the catheter had been inserted 18 years earlier; (2) the onset pattern was acute-on-chronic, followed by the acute-onset symptoms due to hematoma; (3) the symptoms were caused by a hematoma in the subarachnoid space and/or intraepidural spaces; and (4) the patient had severe neurologic defects.
Summary of the cases with complications following residual broken epidural catheter
Breakage of epidural catheters has been reported to occur during their insertion and/or withdrawal. 3 , 7 The insertion of a catheter too deeply through the epidural needle increases the potential risk of breakage. It leads to catheter flexure in the spinal canal and induces injury due to the sharp tip of the needle or the kinking and/or knotting of the catheter. 5 , 11 During catheter withdrawal, entrapment by the supraspinous and intraspinous ligaments may lead to catheter breakage. 13 , 14 Thus, in the current case, catheter breakage might have happened during insertion.
In our case, the CT findings clearly indicated the presence and the location of the catheter fragment, similar to those described in the previous reports. 9 , 15 , 16 These findings may play a significant role in the diagnosis and management of this condition. Therefore, we recommend CT examination in cases with possible catheter breakage or in suspected cases of spinal hematoma with a history of epidural anesthesia.
There are no reports of spinal hematoma because of a retained epidural catheter; therefore, the mechanism underlying the current case of hematoma is not completely understood. Intraoperative findings revealed a granulation formation around the catheter and inflammatory signs on the dura. Thus, chronic inflammation due to the fragment of the epidural catheter may have occurred, which might have caused vascular proliferation and vascular fragility. In addition to this condition, the anticoagulation therapy might have led to the spinal hematoma. 17 , 18 , 19 As is well known, most cases of spinal hematoma are idiopathic. The second major cause is the anticoagulant therapy, and the third is vascular malformations, according to Kreppel et al. 18 Because we did not perform spinal angiography in this case, we cannot deny the possibility of spinal arteriovenous fistula. Moreover, this patient had undergone anticoagulant therapy, which is a risk factor for spinal hematoma. However, spinal hematoma is a rare condition and catheter breakage is also rare. We believe that there is a relationship between the catheter fragment and the subdural hematoma and that this catheter fragment could have been a risk factor for the spinal hematoma. However, unfortunately, there has not been any evidence of this mechanism either in this study or reported previously. Thus, in patients who have hematoma with catheter breakage, other possible reasons for hematoma should be considered during their management.
Previous studies have shown that complications, including neural disorders resulting from retained broken catheters, occurred chronically. 4 , 8 Therefore, the previous literature and case reports of epidural catheter breakage recommend that the broken catheter fragment need not be removed in asymptomatic patients unless there is a possibility of infection, 6 an overly long retention of the catheter (in cases of children), 20 or a mass that is sufficiently large to exert a direct effect on neural structures. 21 Catheter removal by a surgeon is recommend when the patient presents symptoms due to the residual catheter fragment. 22 To our knowledge, this is the first case that presented spinal hematoma due to a broken catheter and was characterized by acute episodes of neural defects. We hypothesized the following mechanism for subdural hematoma due to catheter fragment: compression due to the catheter fragment led to inflammation and granulation around the spinal cord, and as a result, a fragile chronic neovascularity appeared around the spinal cord. Additionally, anticoagulant therapy could have disrupted the fragile vascularity. Therefore, we propose that the possibility of a hematoma causing severe neurologic defects be considered as a late complication when discussing strategies for the management of patients with residual broken catheters. Based on this experience alone, we cannot conclusively state that the catheter fragment was the only reason for the late-onset spinal hematoma. Therefore, we cannot strongly recommend the removal of the broken catheter in all cases. However, based on this case, we can recommend the removal of broken catheters in patients who have already taken anticoagulant drugs, have the possibility of starting anticoagulant therapy, or have coagulation defects. Furthermore, according to our case, when managing the patient with spinal hematoma, catheter breakage should be considered as a possible reason. CT examination would help in the diagnosis of resident catheter fragments. In addition, when catheter breakage is in the spinal canal, we recommend its removal to prevent the recurrence of spinal hematoma due to catheter breakage.
Disclosures
Yoshimoto Ishikawa, none
Shiro Imagama, none
Zenya Ito, none
Kei Ando, none
Momokazu Gotoh, none
Kimitoshi Nishiwaki, none
Yoshimasa Nagao, none
Naoki Ishiguro, none