
Abstract
Study design
Descriptive radiographic analysis of a prospective multi-center database.
Objective
This study aims to provide normative values of spinopelvic parameters and their correlations according to age and pelvic incidence (PI) of subjects without spinal deformity.
Methods
After Institutional Review Board (IRB) approval, 1540 full spine radiographs were analyzed. Subjects were divided into 3 groups of PI: low PI < 45°, intermediate PI 45–60°, high PI > 60°, and then stratified by age (20–34, 35–49, 50–64, > 65 Y.O). Pelvic and spinal parameters were measured. Statistical analysis between parameters was performed using Bayesian inference and correlation.
Results
Mean age was 53.5 years (845 females, 695 males, range 20–93 years).
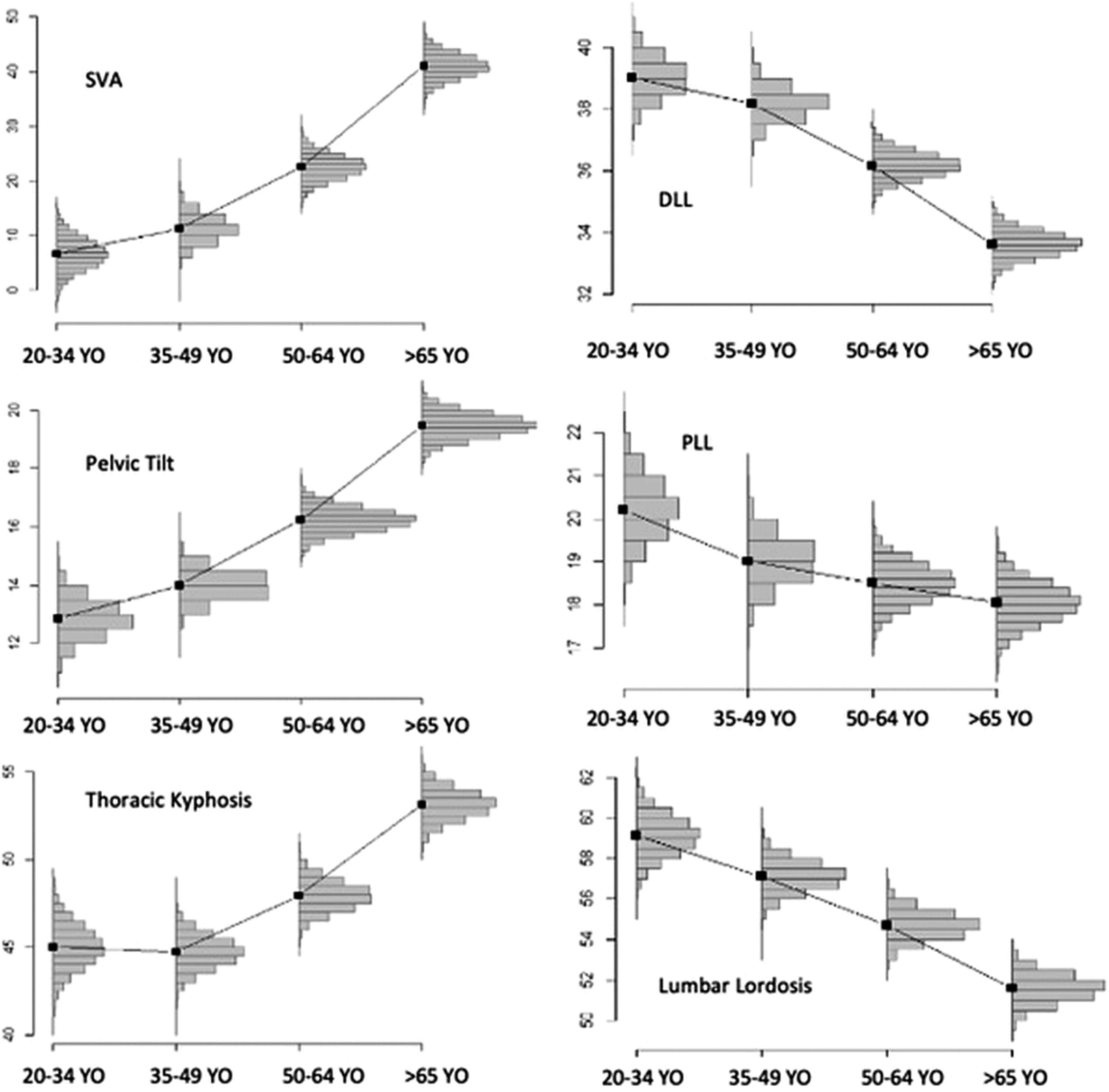
In low PI group, lumbar lordosis (LL) decrease was mainly observed in the 2 younger age groups.
In medium and high PI groups, loss of lordosis was linear during aging and occurred mainly on the distal arch of lordosis. Moderate PI group had a stable lordosis apex and thoracolumbar inflection point. High PI group had a stable thoracolumbar inflection point and a more distal lordosis apex in elderly subjects.
For all subjects, kyphosis and pelvic tilt (PT) increased with age.
There was a constant chain of correlation between PI and age groups. Proximal lumbar lordosis (PLL) was correlated with kyphosis and sagittal vertical axis (SVA C7), while the distal lumbar lordosis (DLL) was correlated with PI and PT.
Conclusion
This study provides a detailed repository of sagittal spinopelvic parameters normative values with detailed analysis of segmental kyphosis and lordosis distribution according to gender, age, and PI.
Introduction
The evolution toward bipedalism required a specific organization of the axial skeleton. This organization is characterized by different pelvic and spinal parameters introduced by Duval-Beaupère et al., 1 which define a so-called “balanced” position between the pelvis and the spine. The existence of a spinopelvic imbalance, projecting the body’s axis of gravity forward or backward from the sustentation triangle, represents a cause of premature aging of the axial skeleton. 2
However, a modification of sagittal alignment during aging is physiological, which will lead to an adaptation of spinal and pelvic parameters, thus allowing an upright position, walking, and maintenance of a horizontal gaze. 3 In daily life, sagittal alignment measured on radiographs is more a matter of dynamic sagittal balance, maintained by adaptive mechanisms during aging.
Radiographic parameters defining sagittal alignment are well described in the literature4-6 and an attempt of description of sagittal alignment in degenerative spine based on sacral slope has been reported. 3 However, considering that lumbar lordosis (LL) is established between L1 and S1, thoracic kyphosis (TK) between T1 and T12 and that standard normative values can be applied to any subject regardless of age can be a source of error. 7 The Scoliosis Research Society (SRS)-Schwab classification 8 gives global correction objectives in patients with spinal deformity, but it does not consider the patient’s age or pelvic incidence (PI). Adult spinal deformity (ASD) correction surgeries have high complication rates 9 and postoperative under-correction is strongly correlated with clinical deterioration and an increased incidence of mechanical complications.8,10 On the other hand, over-correction can also lead to an increased risk of preoperative neurological injury or postoperative proximal junctional kyphosis (PJK).10-12 Precise knowledge about sagittal alignment in different age groups and the definition of normative values according to PI, seem to be crucial when planning ASD surgery.4,13
In the elderly subjects, a loss of LL and an increase in TK have been identified, leading to pelvic retroversion in order to compensate physiological changes in sagittal alignment. We hypothesized that changes of spinopelvic parameters and their associated compensatory mechanisms will depend on patient’s PI.
This study aims to provide normative values of sagittal spinopelvic parameters according to age and PI of subjects without spinal deformity. These normative values can, in a further step, potentially serve as a frame for planning ASD surgical correction.
Methods
This is a descriptive study of a prospective multi-center database, including patient data from 16 spinal surgery centers. Institutional review board approval (FC/2019-91) was obtained.
Study Population
All patients older than 20 years who received a full spine EOS radiography (EOS imaging, Paris, France) during clinics in orthopedic surgery or neurosurgery for an acute complaint or systematic screening were selected. Before inclusion, each eligible subject received explanations and gave an informed consent.
Exclusion criteria were: absence of informed consent from the patient or his legal representatives in the case of a patient under guardianship, the presence of a deformity of the spine or lower limbs, history of vertebral or pelvic fracture, the presence of vertebral metastasis or infection, an osteoporotic spine with vertebral compression fractures, history of spinal surgery other than microdiscectomy. Degenerative changes as intervertebral disc degeneration, facet joint osteoarthritis and degenerative spondylolisthesis were considered as normal aging process and radiographs were only excluded if multiple level spondylosis or discopathy led to spinal deformity.
Study Protocol
All patients included in the study had performed EOS biplanar radiographs performed from September 2019 to March 2020 and all radiographic parameters were measured using KEOPS software (SMAIO, Lyon, France) on lateral full spine images (Figure 1). KEOPS(r) software has demonstrated better reproducibility than standard manual radiological measurements.
14
Each radiograph was analyzed and reconstructed by 2 independent senior spine surgeons to minimize interobserver errors. These investigators set anatomic key points to determine of pelvic and spinal parameters using the KEOPS software. Example of an EOS full spine radiograph reconstruction using KEOPS software (left) and measurements of main parameters (PI, LL, PLL, DLL, TK, and SVA) (right).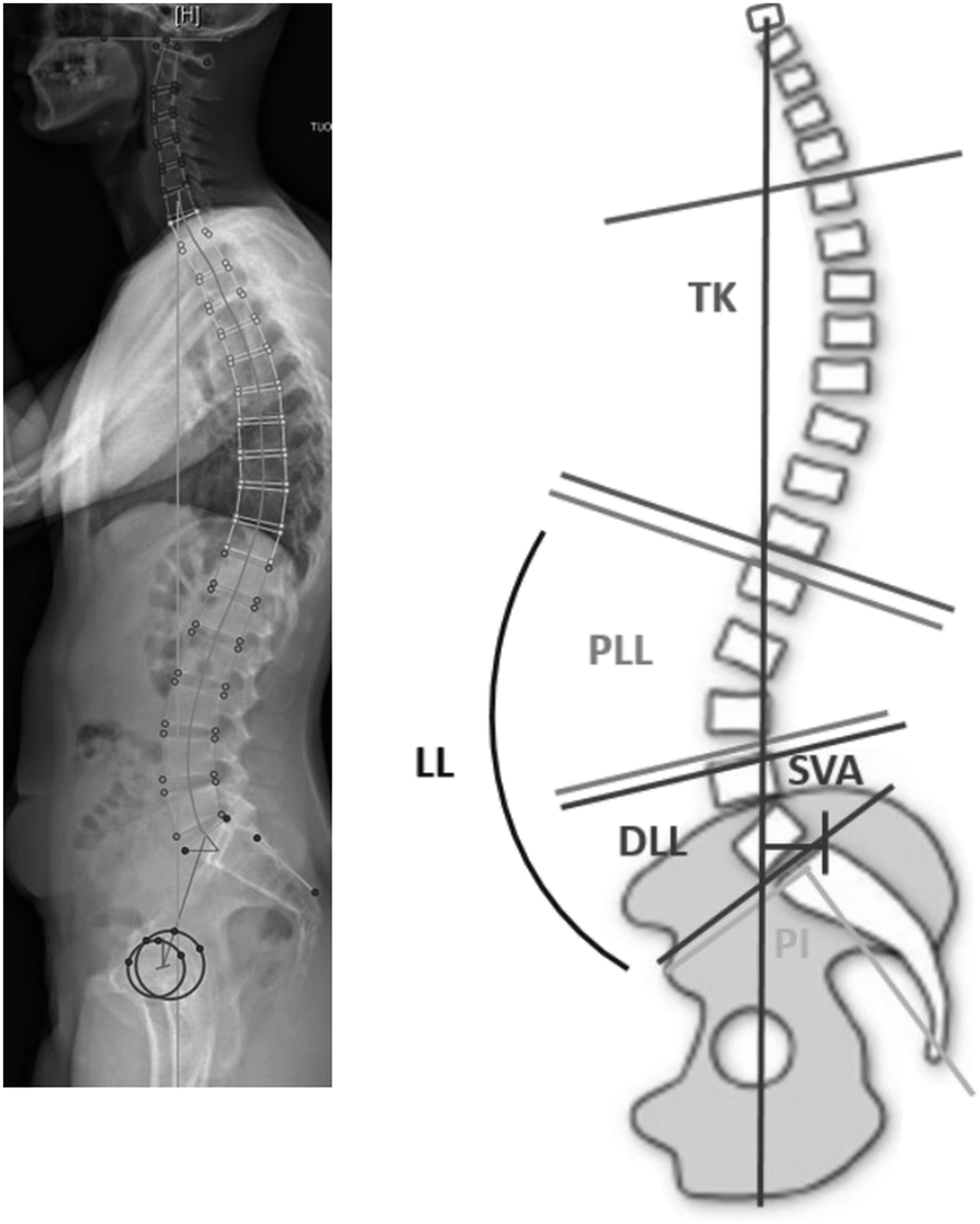
Demographic Parameters
The age and gender of each subject were recorded and blinded to reviewers. Subjects were stratified into groups according to age: 20–34-year-old (Y.O.) 35–49 Y.O., 50–64 Y.O., and over 65 Y.O. The study population was further stratified by PI: low PI < 45°, intermediate PI 45°–60°, high PI > 60°. 7
Radiographic Parameters
The radiographic analysis determined global LL between the thoracolumbar inflection point and the S1 endplate, proximal lumbar lordosis (PLL) between thoracolumbar inflection point and the lumbar apex (defined as the vertebra furthest from the tangent passing through the postero-inferior edge of the last LL vertebra and the postero-superior corner of the first LL vertebra), distal lumbar lordosis (DLL) between the lumbar apex and the S1 endplate, global TK between cervicothoracic and thoracolumbar inflection points. Kyphosis and lordosis were expressed as positive values. PI, sacral slope, pelvic tilt (PT) and the C7 Sagittal Vertical Axis (SVA) were measured.
Statistical Analysis
Statistical evaluation was performed with R Software Version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). A Bayesian inference using the Markov chain Monte Carlo techniques with low informative priors was used. To infer the mean of indices and correlation coefficients between 2 indices, point estimates correspond to the median of posterior distributions and credibility intervals to their 2.5 and 97.5 percentiles. Spinopelvic parameters were compared by gender, PI (low PI < 45°, medium PI 45°–60°, high PI > 60°) and age groups. Significance tests were based on the probability of superiority for the difference between 2 means and for correlation coefficients (strong if ρ < −.5 or ρ > .5). For PI, the medium group and for ages the group 20–34 years were considered as references. The significance level was set at a .95 probability of superiority.
Results
Study Population
Radiographic analysis was performed on 1540 patients (845 females and 695 males). The mean age was 53.5 years (range 20 to 93). The mean PI of the global cohort was 53.3° (range 18.9°–98.0°).
Population stratification by age and pelvic incidence (n).
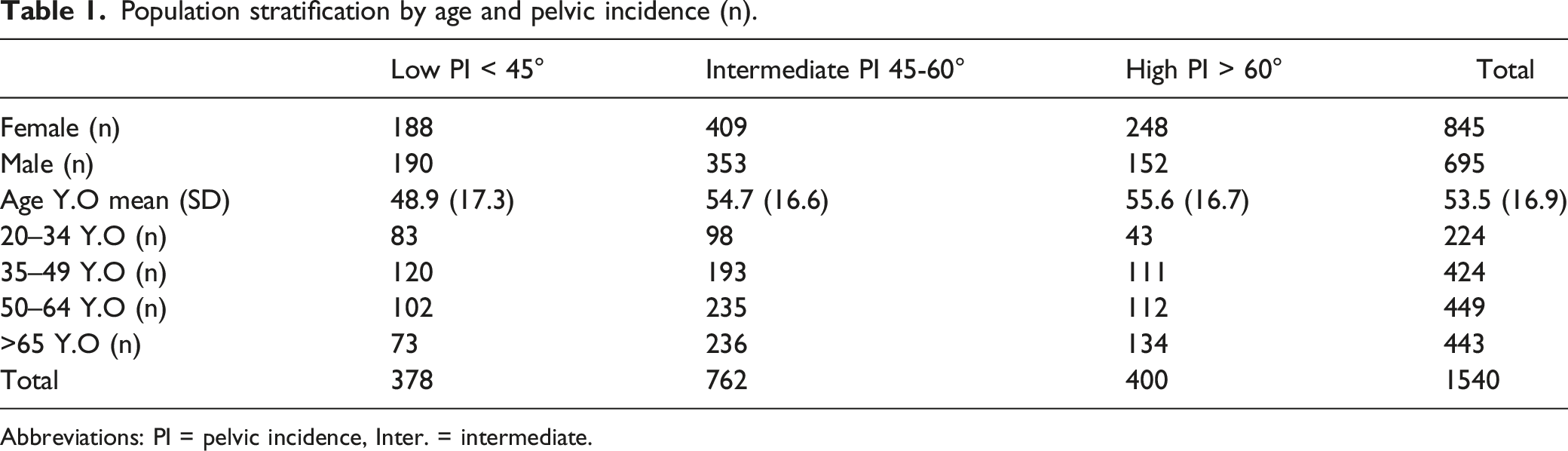
Abbreviations: PI = pelvic incidence, Inter. = intermediate.
Comparison of pelvic and spinal parameters Male/Female.
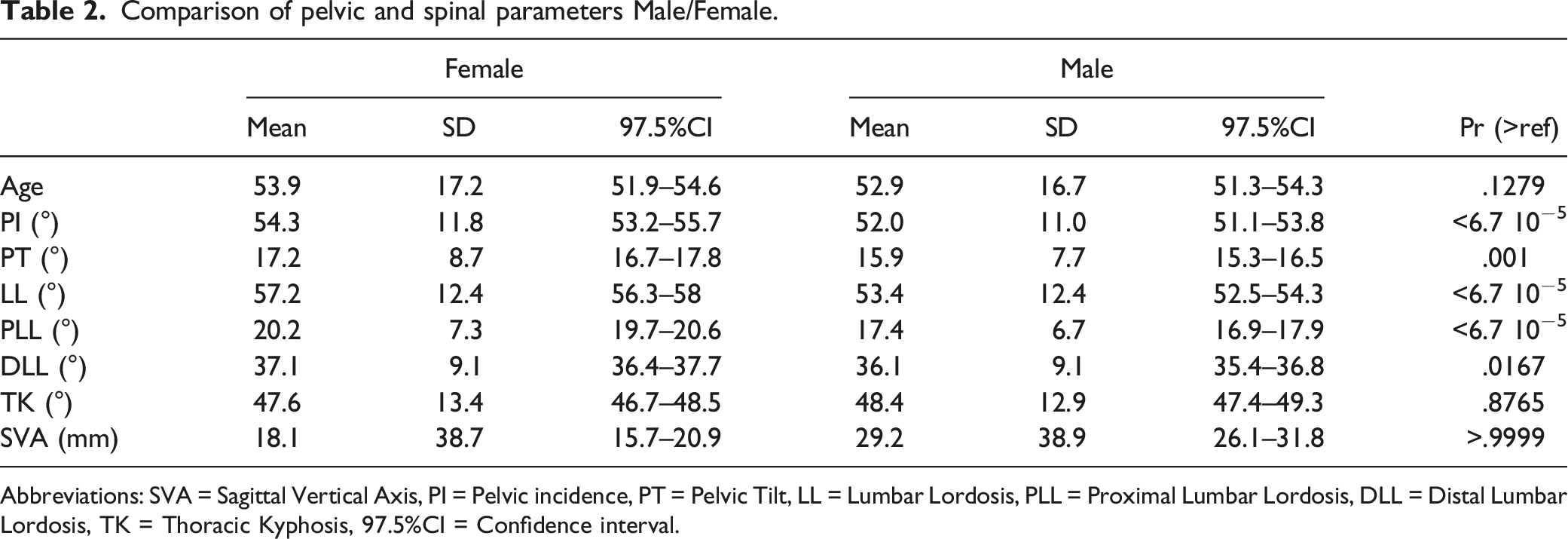
Abbreviations: SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis, 97.5%CI = Confidence interval.
Low PI Group
In the low PI group, there were 188 females and 190 males. The distributions of thoracolumbar inflection and lumbar apex were more distal in subjects over 65 Y.O. when compared to younger subjects (Figure 2). Distribution of thoracolumbar inflection point and lumbar apex.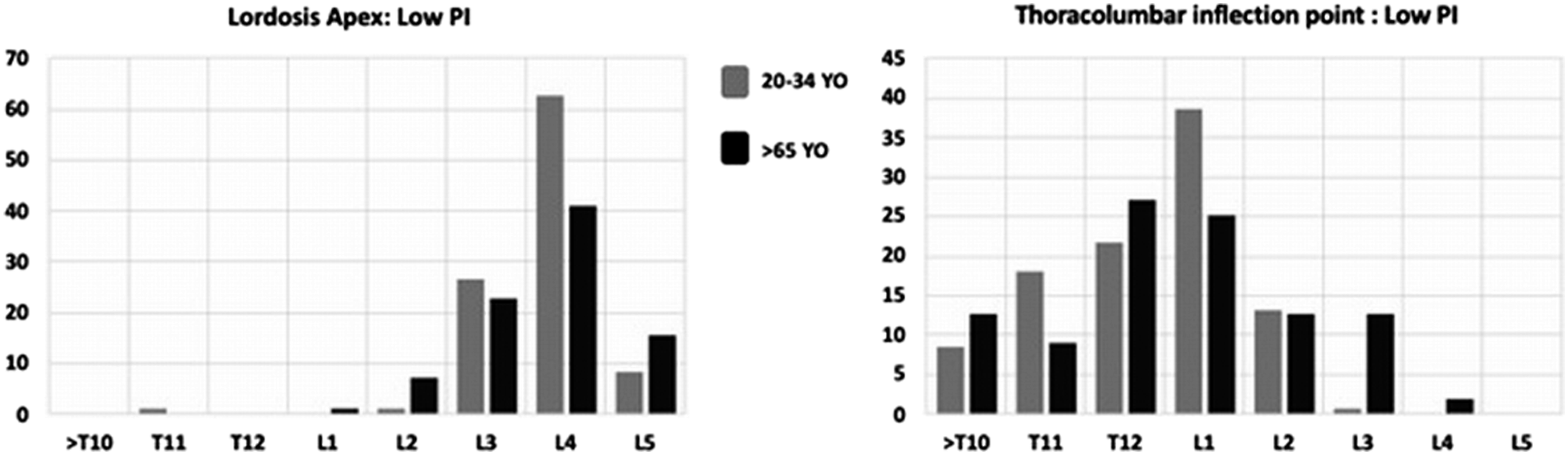
Global LL decreased with age in PLL and DLL segments (Figure 3). Thoracic kyphosis was stable in age groups from 20 to 64 Y.O. and then increased significantly (Pr = .999) after 65 Y.O. The SVA increased after 49 Y.O., whereas pelvic retroversion occurred as early as 35 Y.O., concomitantly to lordosis decrease. Pelvic and spinal parameters of subjects with low pelvic incidence by age category. (SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis).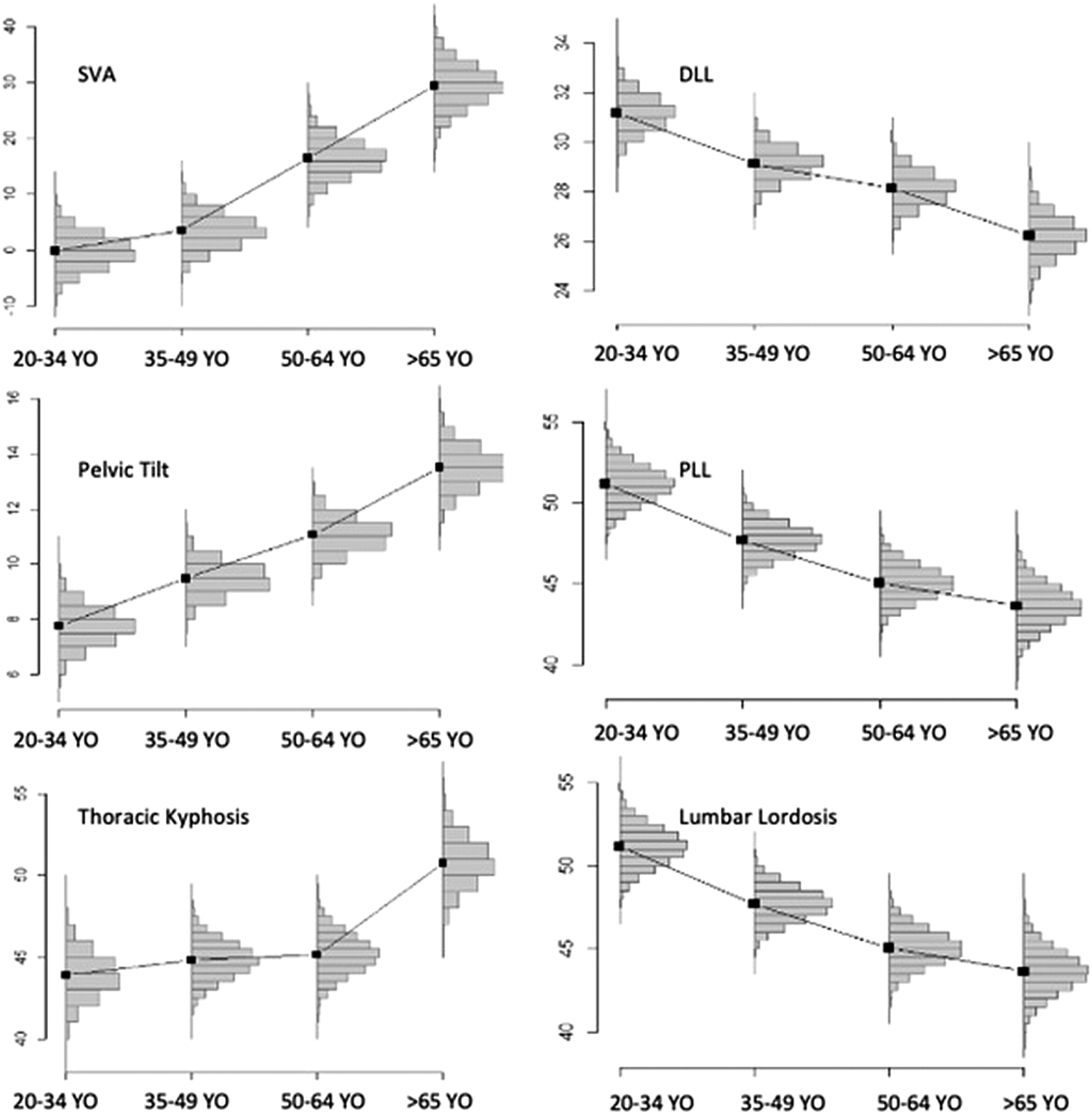
Pelvic and spinal parameters of subjects with low pelvic incidence by age category.
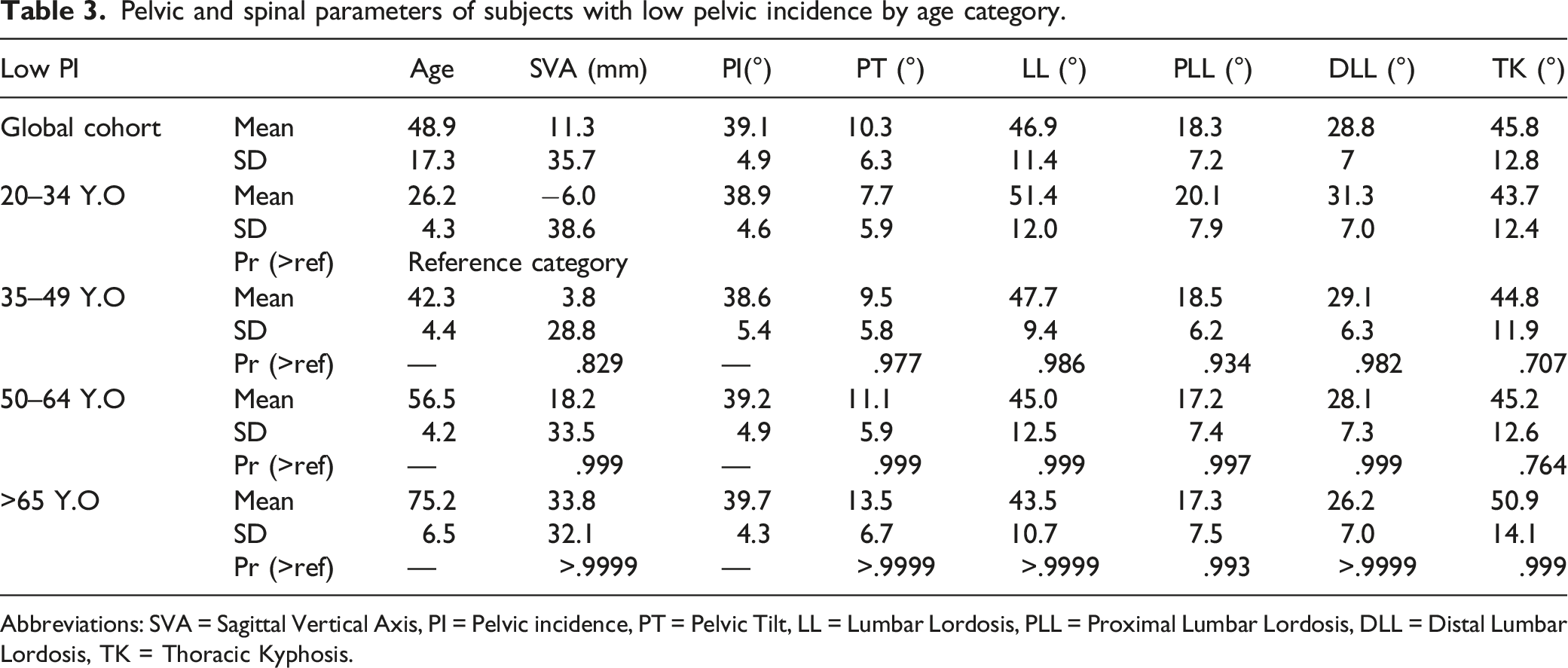
Abbreviations: SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis.
Intermediate PI Group
In the intermediate PI population, there were 409 females and 353 males. The thoracolumbar inflection point was more distal in subjects over 65 Y.O., while the lumbar apex remained stable throughout age groups (Figure 4). Distribution of thoracolumbar inflection point and lumbar apex.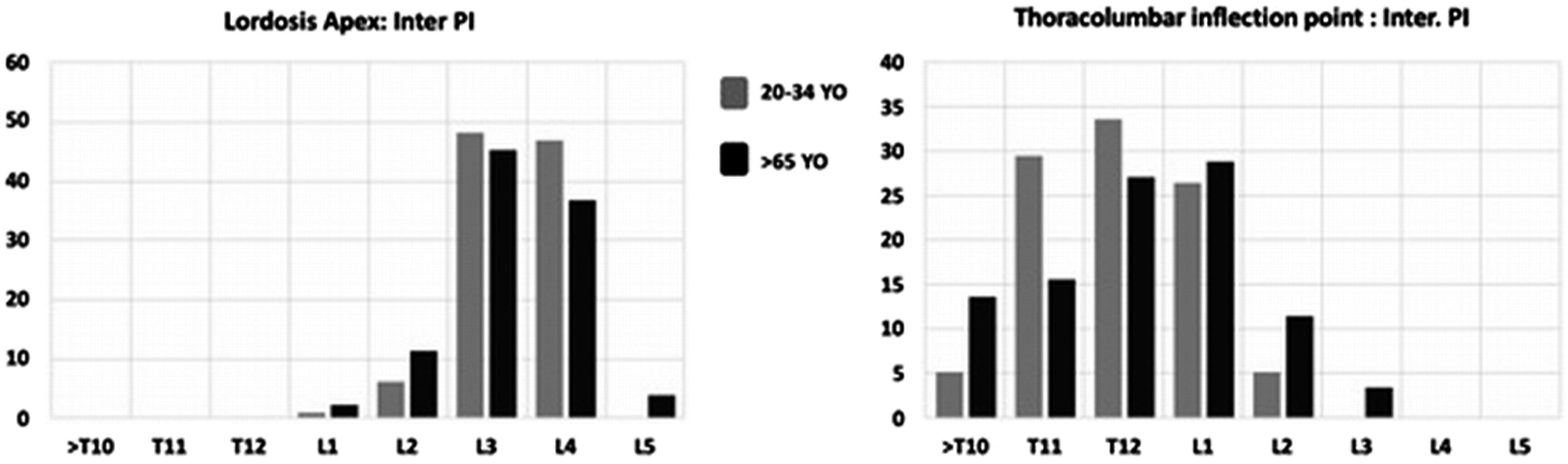
The global LL decrease was 7.5° with a constant decrease across age categories: 59.3° at 20–34 Y.O. vs 51.6° after 65 Y.O.
Pelvic and spinal parameters of subjects with intermediate pelvic incidence by age category.
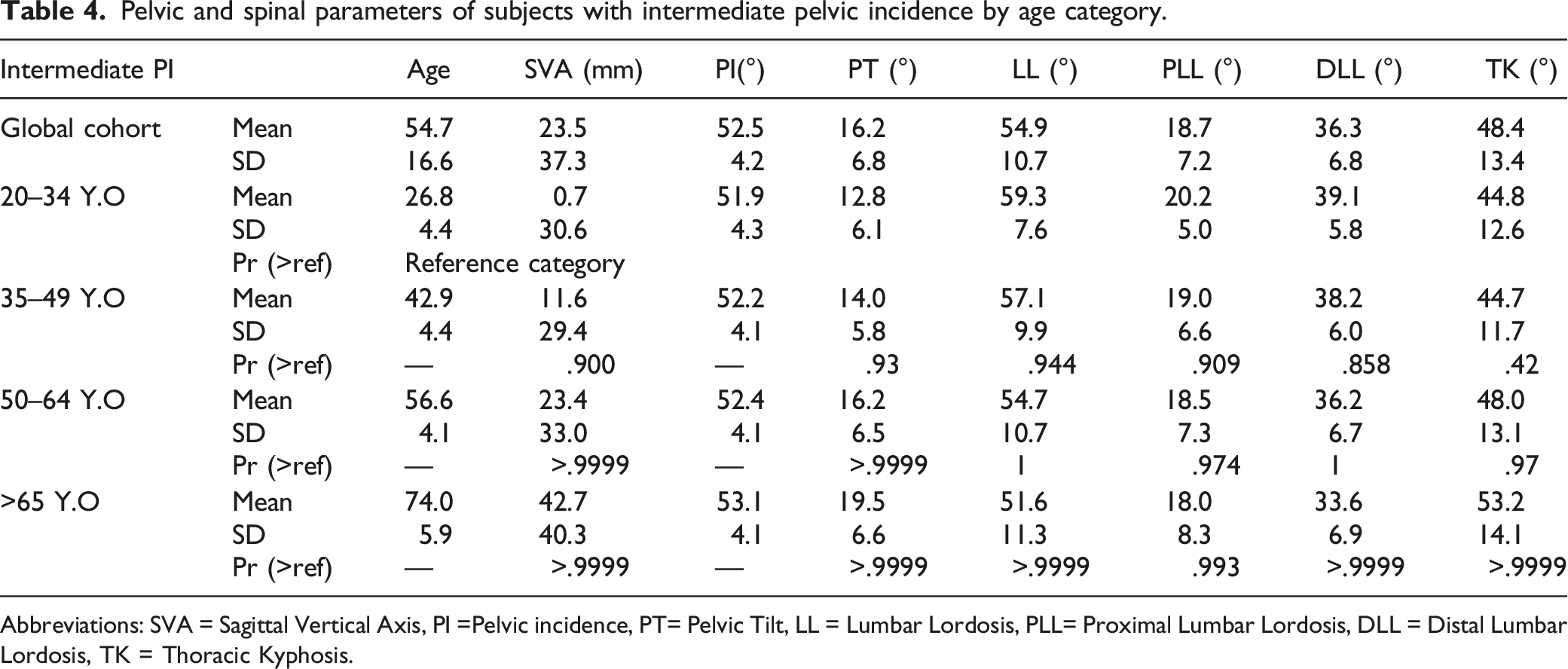
Abbreviations: SVA = Sagittal Vertical Axis, PI =Pelvic incidence, PT= Pelvic Tilt, LL = Lumbar Lordosis, PLL= Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis.
Pelvic and spinal parameters of subjects with intermediate pelvic incidence by age category. (SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis).
High PI Group
In the high PI population, there were 248 females and 152 males. The thoracolumbar inflection point was more distal in elderly subjects while the LL apex remained unchanged across age groups (Figure 6). Distribution of thoracolumbar inflection point and lumbar apex.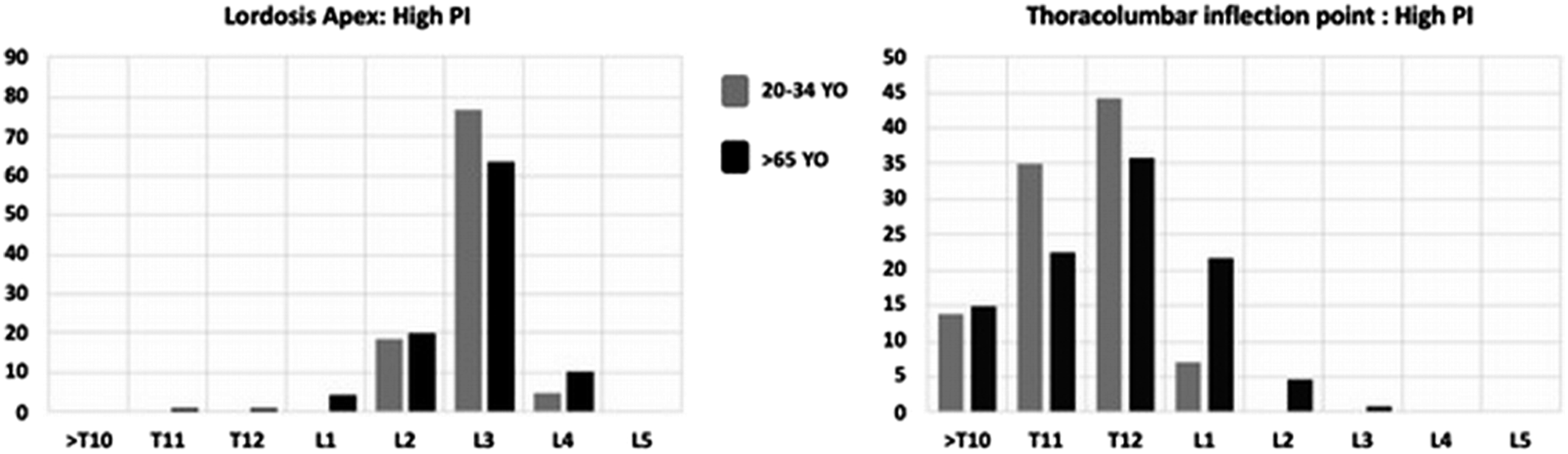
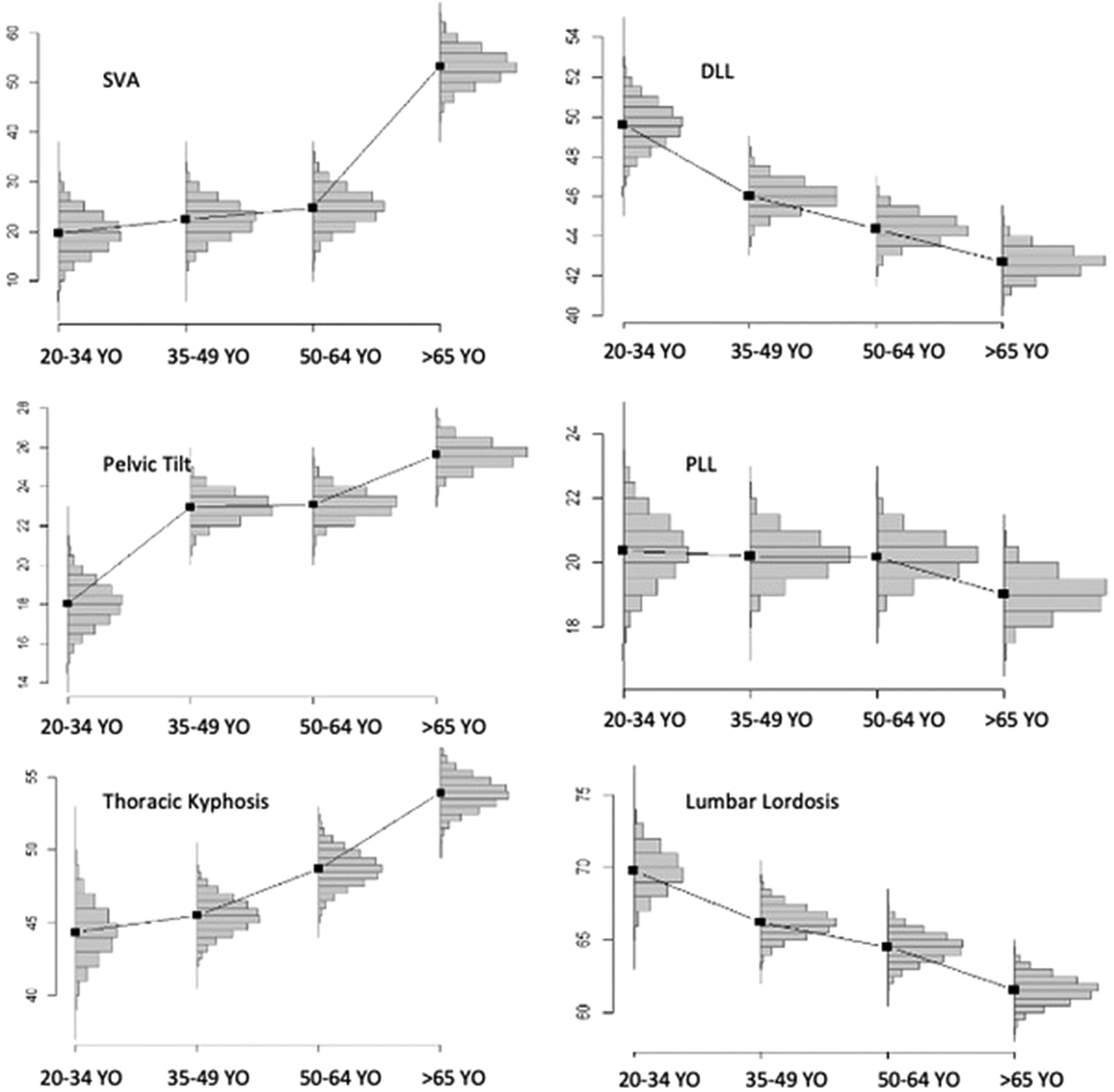
The decrease in LL was more significant (Pr = .97) before 49 Y.O.:69.8° in 20–34 Y.O. vs 66.2° in 35–49 Y.O. This decrease in lordosis involved PLL, whereas DLL varied only slightly across ages.
Thoracic kyphosis was stable until 49 Y.O. and then increased from 45.5° in the 35–49 Y.O. age group to 54° in the over 65 Y.O. age group. The SVA was stable until 64 Y.O. and then increased significantly: 25.4 mm between 50 and 64 Y.O. vs 57.1 mm after 65 Y.O.
Pelvic tilt increased mainly after 35 Y.O. and after 64 Y.O.
Pelvic and spinal parameters of subjects with high pelvic incidence by age category.
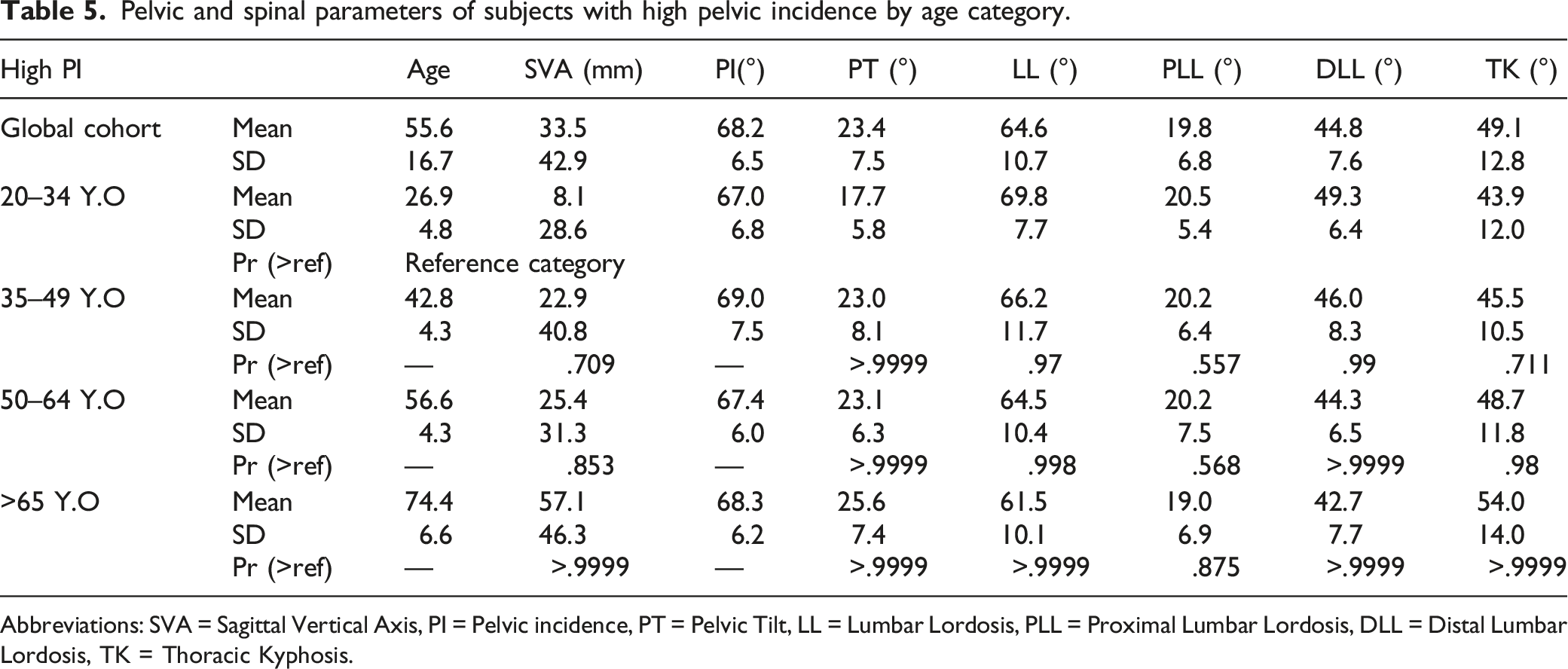
Abbreviations: SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis.
Pelvic and spinal parameters of subjects with high pelvic incidence by age category. (SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis).
Correlation Analysis
Regardless of PI, there was a stable and significant correlation chain across age categories with a strong correlation between the proximal arch of lordosis (PLL) and TK. As the amount of PLL correlated with SVA and TK, the distal arch of lordosis (DLL) correlated with PI and PT.
Correlations per PI group are presented in Figure 8. Correlation between spinopelvic parameters by PI and age. (SVA = Sagittal Vertical Axis, PI = Pelvic incidence, PT = Pelvic Tilt, LL = Lumbar Lordosis, PLL = Proximal Lumbar Lordosis, DLL = Distal Lumbar Lordosis, TK = Thoracic Kyphosis).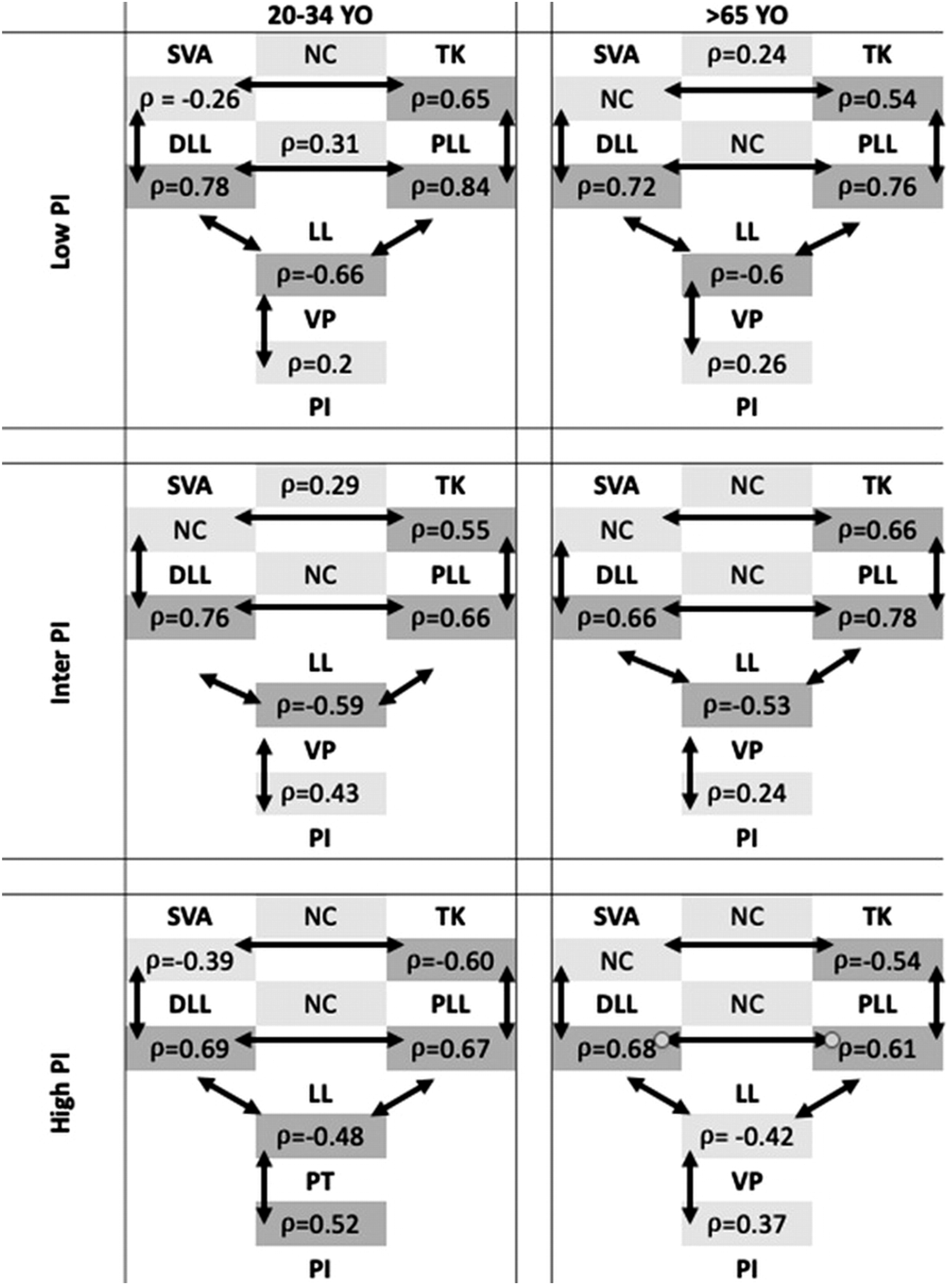
Discussion
Diagnosis and surgical management of multilevel degenerative spinal pathologies requires knowledge of normative values of the different parameters and associated adaptive mechanisms that occur with aging.15,16
Different studies5,6 have reported changes in spinal alignment during aging with a progressive increase in TK, PT, and SVA, concomitantly to a progressive loss of LL. Such results highlighted the importance of age in surgical planning for ASD patients. Lafage et al. 4 defined thresholds for various parameters (PI-LL, SVA, PT) according to age in the setting of ASD correction objectives. This necessity for age-related alignment targets is also important during postoperative course as it was also reported that overcorrected patients were at higher risk of PJK. 12 Recently, Sebaaly et al. 3 described sagittal alignment of the degenerative spine in an attempt to classify patients and to offer treatment algorithm. However, the main limitation is related to the use of sacral slope for classification as this parameter is positional and as a consequence variable. It seems therefore more useful in daily practice to stratify patients according to an anatomical parameter such as PI. The interest of PI was reported by Protopsaltis et al. 13 using age-specific normative SF-36-PCS values to determine alignment targets in different PI groups and recently Zhou et al. 17 reported PI stratified sagittal alignment parameters according to age in a Chinese population.
In this study, we analyzed a large cohort in order to provide a reliable baseline of pelvic and spinal parameters with a stratification by age and PI that would facilitate its use in current practice. According to our findings, sagittal spinal aging seems to begin with a loss of LL. The amplitude of this decrease was important between 20–34 Y.O. and 35–49 Y.O., particularly in subjects with low PI (Tables 2–4) while the evolution of the other parameters (PT, TK, SVA) showed later variations after the age of 50 years. These changes are responsible for an anterior malalignment with subsequent development of adaptive mechanisms that aims to bring back the body’s center of gravity behind the femoral heads.18-20 Adaptive mechanisms (i.e., the amount of pelvic retroversion) depended on the subject’s spinopelvic organization as the amount of PT is linked to the amount of PI.21,22
Furthermore, the present study focused on the segmentation of LL into 2 arches allowing a more detailed analysis of the evolution across age groups, according to PI.
In subjects with low PI, the loss of lordosis with aging was distributed almost equally between PLL and DLL. It leads to a caudal shift of the lordosis apex and the thoracolumbar inflection point and an early onset of pelvic retroversion (before 35 Y.O). The increase in SVA and TK occurred later in this population with greater amplitude changes between 50–64 Y.O and > 65Y.O. We also found a correlation between SVA and TK in subjects > 65 Y.O with low PI. This correlation can be explained by a lower pelvic retroversion capacity of these patients, leading to an early imbalance when the TK increases.
In subjects with intermediate PI, loss of lordosis with aging occurred mainly in the PLL and the subjects showed a caudal shift of the thoracolumbar inflection point while the lumbar apex remains stable. The SVA, TK, and PT increased gradually after 49 years of age without any major change in the chain of correlation that links them with age.
In subjects with a high PI, the loss of lordosis was mainly related to the DLL, whereas the PLL remains almost constant across ages.
These differences with aging of the 2 lordosis arches highlight the importance of considering them as 2 distinct entities in clinical practice, using the lordosis apex and the thoracolumbar inflection point to localize them. LL usually described between the endplate of S1 and the upper endplate of L1 should not be considered as a functional unit. The objective of surgical ASD correction can therefore considerer the amplitude of each arc of lordosis and the location of the apex of LL and the thoracolumbar inflection point to restore a physiological lordosis. In our study, there was a strong correlation between LL and PT, whereas the PLL was strongly correlated with TK, regardless of age and PI. These results are consistent with those reported by Pesenti et al. 7 who reported a strong correlation between PLL and PI in asymptomatic subjects while there was no direct correlation between DLL and PI.
When analyzing the correlation chain linking the pelvic and spinal parameters, our results confirmed that when a segment changes because of aging, the other segments adapt to maintain global alignment, which is in line with previous findings of Berthonnaud et al. 23 and Iyer and al. 5 However, our study allowed to identify the specific correlations of each lordosis segment in the lumbar spine, PLL was strongly correlated to TK and acted as an adaptive zone between the DLL and the thorax, especially for subjects with a low PI for whom DLL changed only slightly with aging.
In clinical practice, the results of this study provide normative values of spinopelvic parameters according to age and PI. In a further step, these results might be used to improve surgical planning for ASD patients according to age and PI. The present data could help to establish specific alignment targets more precisely, while taking regional sagittal parameters such as PLL and DLL into account. In other words, knowledge of normative values of PLL and DLL according to age and PI will help to understand in which part of LL (DLL and/or PLL) the loss occurred and which segment needs to be restored during surgery.
This study has limitations. While we reported a stable chain of correlations over time, unlike the studies of Iyer et al. 5 and Hu et al. 6 our study did not include an analysis of the positioning of the lower limbs. Furthermore, clinical scores were not assessed in this cohort of subjects and mostly Caucasian subjects were enrolled and ethnic differences might influence results.
Conclusion
This study provides a detailed repository of sagittal spinopelvic parameters normative values with detailed analysis of segmental kyphosis and lordosis distribution according to age and PI to allow a “patient specific” analysis of spinal aging. In subjects with low PI, the loss of lordosis with aging was distributed almost equally between PLL and DLL leading to a caudal shift of the lordosis apex. In subjects with a high PI, the loss of lordosis was mainly related to the DLL, whereas the PLL remains almost constant across ages. Regardless of PI, there was a stable and significant correlation chain across age categories with a strong correlation between the proximal arc of lordosis (PLL) and TK, the distal arc of lordosis (DLL) correlated with PI and PT.
Footnotes
Acknowledgments
Philippe Roussouly for technical support using the KEOPS online data base.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors Note
Yann Philippe Charles is consultant for Stryker, Clariance, Philips and Ceraver; he received royalties and grants unrelated to this study from Stryker and Clariance. Eloïse Bauduin has no conflict of interest. Sébastien Pesenti has no conflict of interest. Brice Ilharreborde is consultant for Zimmer Biomet, Medtronic and Implanet. Solène Prost has no conflict of interest. Féthi Laouissat is consultant for Spineart and SMAIO. Guillaume Riouallon is consultant for Medtronic, Stryker and NewClip; he received royalties from Euros. Stéphane Wolff has no conflict of interest. Vincent Challier is shareholder of Follow Health SA and consultant for Clariance. Ibrahim Obeid is consultant for Medtronic and Depuy Synthes; he received grants from DePuy Synthes unrelated to this study and royalties from Clariance, Alphatec and Spineart. Louis Boissière is consultant for Neo and Euros; he received grants from DePuy Synthes unrelated to this study. Emmanuelle Ferrero has no conflict of interest. Federico Solla received funding to attend meetings from Medicrea, Medtronic and Euros. Jean-Charles Le Huec is consultant for Medtronic and BD Bard; he received royalties and grants unrelated to this study from Medtronic. Stéphane Bourret has no conflict of interest. Joe Faddoul has no conflict of interest. Georges Naïm Abi Lahoud has no conflict of interest. Vincent Fière is consultant for Clariance; he received royalties Medicrea and Clariance. Michiel Vande Kerckhove has no conflict of interest. Matthieu Campana has no conflict of interest. Jonathan Lebhar has no conflict of interest. Hadrien Giorgi has no conflict of interest. Aymeric Faure is consultant for OSD. Erik André Sauleau has no conflict of interest. Benjamin Blondel is associate editor for OTSR Elsevier-Masson and consultant for Medicrea, Medtronic, Implanet, Vexim Stryker and 3M.
Institutional Review
Institutional review board approval (FC/2019-91). The manuscript does not contain information about devices/drugs.