
Abstract
Study Design:
A prospective cohort study in a high-flow spine center in Germany.
Objectives:
This study aimed to evaluate clinical outcomes and complications of the trans-tubular translaminar microscopic-assisted percutaneous nucleotomy in cases of cranially migrated lumbar disc herniations (LDH).
Methods:
Between January 2013 and January 2018, 66 consecutive patients with cranio-laterally migrated LDH were operated upon. The following outcome measures were evaluated: (1) Visual Analog Scale (VAS) for leg and back pain; (2) Oswestry Disability Index (ODI) and Macnab´s criteria. All patients were operated upon with trans-tubular Translaminar Microscopic-assisted Percutaneous Nucleotomy (TL-MAPN). Perioperative radiographic and clinical evaluations were reported. The mean follow-up period was 32 months.
Results:
The mean age was 59 years. L4/L5 was the commonest affected level (27 patients). The mean preoperative VAS for leg pain was 6.44 (±2.06), improved to 0,35 (±0.59) postoperatively. Dural injury occurred in 1 patient, treated with dural patch. Improved neurological function was reported in 41/44 Patients (neurological improvement rate of 93%) at the final follow up. There was a significant improvement in the mean ODI values, from 50.19 ± 4.92 preoperatively to 10.14 ± 2.22 postoperatively (P < 0.001). Sixty four out of 66 patients (96%) showed an excellent or good functional outcome according to Macnab´s criteria. No recurrent herniations were observed.
Conclusion:
The translaminar approach is a viable minimal invasive technique for cranially migrated LDH. The preservation of the flavum ligament is one of the main advantages of this technique. It is an effective, safe and reproducible minimally invasive surgical alternative in treatment of cranially migrated LDHs.
Keywords
Introduction
In approximately 10% of patients presenting with extruded LDH, the fragment is migrated cranially at the level of the posterior aspect of the vertebral body.1-3 This zone of migration is called the hidden zone and was described in 1971 by Macnab. 4 Migration of the LDH in the hidden zone may result in symptoms related to both the exiting and the traversing nerve roots. In cases of extruded LDH, exposure of the intervertebral disc may not be required. Removal of the extruded fragment alone without discectomy is sufficient to improve patient´s symptoms.5 The approach for lumbar cranially sequestrated disc herniation is controversial. The standard surgical treatment usually consists of an interlaminar approach as described by Caspar et al, 6 which is performed either with laminotomy or inter-laminectomy and, when required, with a facetectomy. In some cases, this surgical approach may produce iatrogenic spinal instability depending on the extent of boney resections, 7 For this reason, in 1998, Di Lorenzo et al 8 described an approach targeting exposure of Macnab’s hidden zone. The approach was based on unroofing the posterior wall of the hidden zone through fenestration of the pars interarticularis. This approach is called a translaminar (TL) approach and allows removal of the extruded fragment without extensive bone removal.
To reduce the surgical trauma and to prevent postoperative instability, Greiner-Perth et al described the muscle-splitting approach through a tubular working canal in 2003. 9
The aim of this study is to evaluate clinical and functional outcomes as well as complications of trans-tubular translaminar microscopic assisted percutaneous nucleotomy (TL-MAPN). The study compares these outcomes to the published alternatives and also highlights the technical steps and difficulties of this procedure.
Patients and Methods
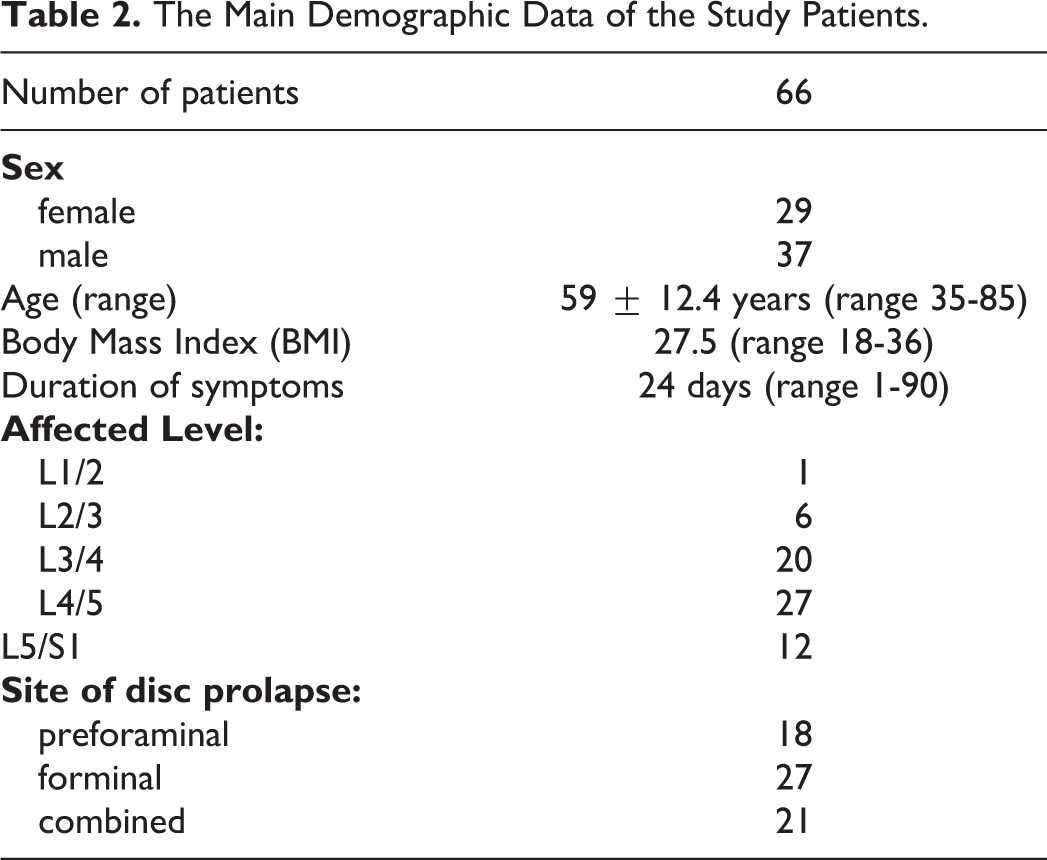
This is a retrospective analysis of prospectively collected data in a single institution. Between January 2013 and January 2018, a total of 66 patients (37 men and 29 women, with a mean age of 59 ± 12.40 years) were operated upon for cranially migrated LDH in the pre-foraminal and foraminal zones using the TL-MAPN technique as the standard of treatment in our institution. The total number of trans-tubular MAPN procedures—for various indications—done in that period was 1155.
Inclusion Criteria
Failure of conservative treatment with persistent (> 6 weeks) or intractable leg pain despite adequate analgesia and/or Significant or progressive neurologic deficit due to compressive radiculopathy, and Corresponding MRI findings of LDH in the hidden zone from L1 to S1.
Exclusion Criteria
Associated extraforaminal pathology or canal stenosis caused by hypertrophied facet or osteophytes, and/or
Associated instability of the affected segment.
All patients demonstrated signs of nerve root compression with radicular pain and hypoesthesia. Motor weakness at least 1 grade (mostly affecting the exiting nerve root) was found in 44 patients (67%) confirmed by neurologist preoperatively.
The most commonly affected level was L4/5 in 27 patients (41%), L3/4 in 20, L5/S1 in 12, L2/3 in 6 and 1 case with L1/2. All patients underwent magnetic resonance imaging (MRI) (Figure 1) of the lumbar spine demonstrating pre-foraminal LDH in 18 cases, foraminal in 27 and both in 21 patients. Two patients were already operated via interlaminar approach at the same level for posterolateral disc herniations. Patients were assessed pre-, postoperatively, and at final follow-up using the German validated Oswestry Disability Index (ODI) and the Visual Analog Scale (VAS) for leg and back pain. In addition, Macnab´s criteria 4 have been used to evaluate patients’ satisfaction in 4 grades: excellent, good, fair, and poor (Table 1).
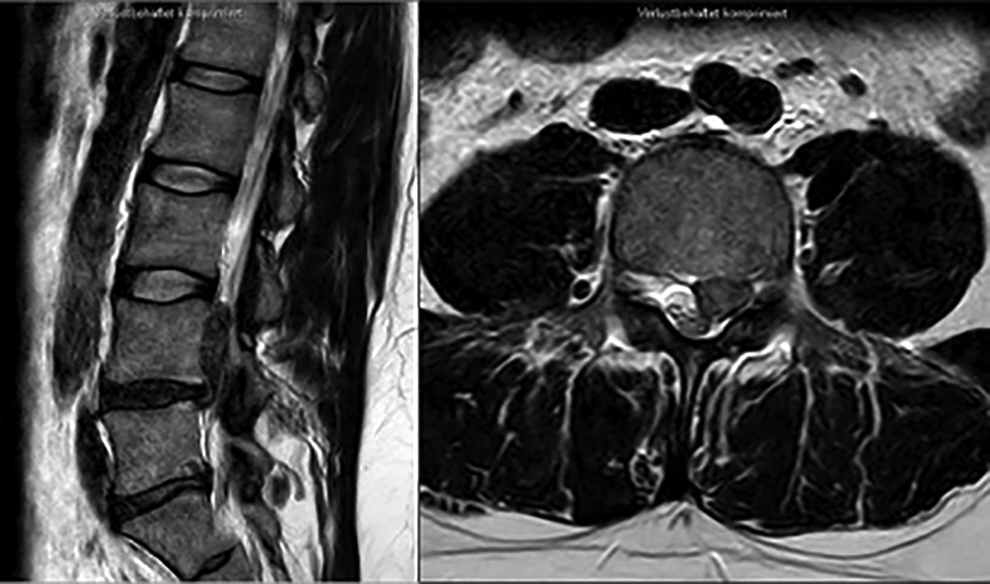
Preoperative MRI of a 45 year-old man, showing cranially migrated sequestration L4/5 on the left side.
Distribution of Patients’ Functional Outcome According to Macnab´s Criteria (N = Number of Patients).
Preoperative diagnostic workup included standing plain radiographs of the lumbar spine anteroposterior, lateral, and dynamic views, and MRI. The mean follow-up period was 32 months (12 -51 months). All patients were counseled about treatment options and possible complications.
Surgical Technique
All operations were performed by 3 senior surgeons (HA, BK, and ASA) with more than 10 years’ experience performing this technique.
All operations were performed under general anesthesia in the prone position. The level of interest was identified using an image intensifier (antero-posterior view). A 1.5 cm paramedian stab incision was performed, followed by sequential trans-muscular dilatation of the paravertebral muscles. The docking site is the lamina cranial to the target disc space. The 16 mm working tube was docked on the lamina that covers the disc herniation and fixed by a flexible-arm retractor. After removing the remaining soft tissue from the bony surface, the lateral border of the lamina was visualized.
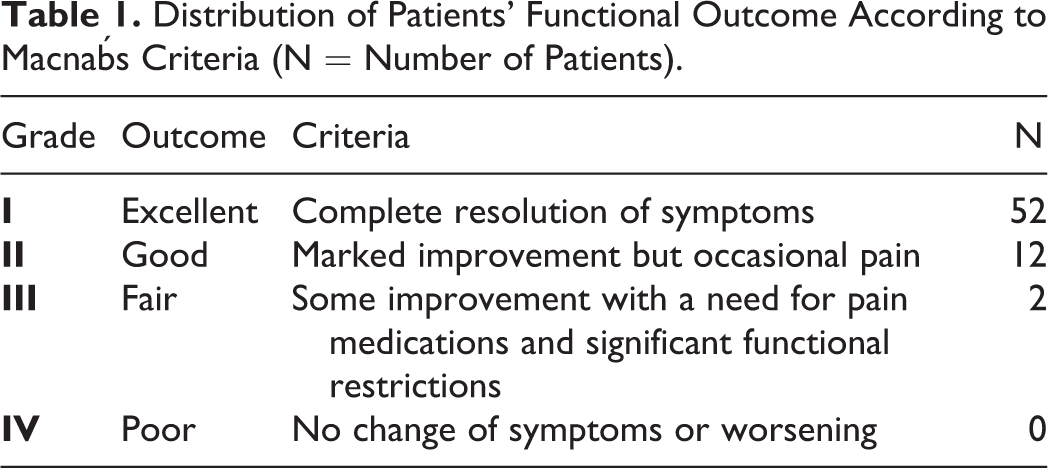
A high-speed 1.8 mm diamond burr was used to identify the optimal position to drill the bony window (Figure 2). The final position was verified again by the image intensifier AP und lateral. Then, the surgical microscope was used. Proper positioning of the hole depends on 2 factors; level of the lamina, site of the disc herniation and diameter of the pars interarticularis. 10 A 4 mm diamond burr was used to cut an ovoid window into the hemi-lamina cranio-medially to the facet joint. The epidural space is often reached directly as the ligamentum flavum is deficient under the upper half of the lamina. A 3 mm rim of bone in all directions should be preserved to prevent iatrogenic fractures of the pars interarticularis. The epidural exploration begins at the lateral border of the dural sac. Bayoneted instruments were preferably used. Further careful dissection is directed toward the herniated disc fragment. Finally, the fragment is removed with small hooks and rongeurs. After hemostasis and careful control on epidural bleeding, the working channel is removed, and 1 or 2 subcutaneous sutures are performed. The skin closure is done by strips (Figures 3 and 4). Postoperatively, patients were allowed to ambulate from the first day without spinal orthosis. (Figure 5)
Intraoperative images on the image intensifier showing localization of the level in antero-posterior and lateral view using a 1.5 mm high speed burr just penetrating the outer cortex of the lamina and then the 90-degree hook introduced through the fully prepared laminotomy hole. The hook is placed lateral to the dural sac and behind the vertebral body cranial to the disc space.

Intraoperative images showing the tube system used fixed to the operative table. The incision after closure and the fragment removed are also shown.
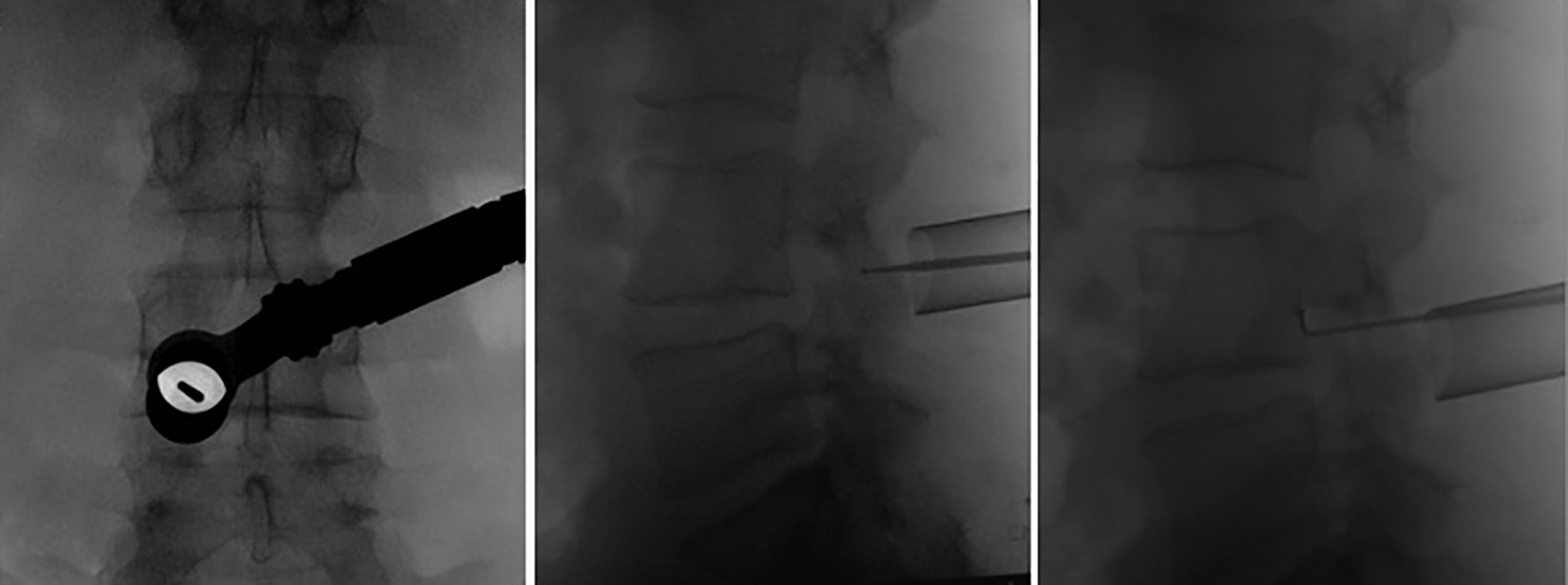
A) The operative field under microscope with the yellow circle encircles the laminotomy hole, while the ligamentum flavum is still in place. B) The dural sac is seen after removal of the ligamentum flavum. C) Part of the sequestrated fragment can be seen after medial retraction of the dural sac and hemostasis using a cottonoid patty laterally. D) The removed sequestrated fragments.
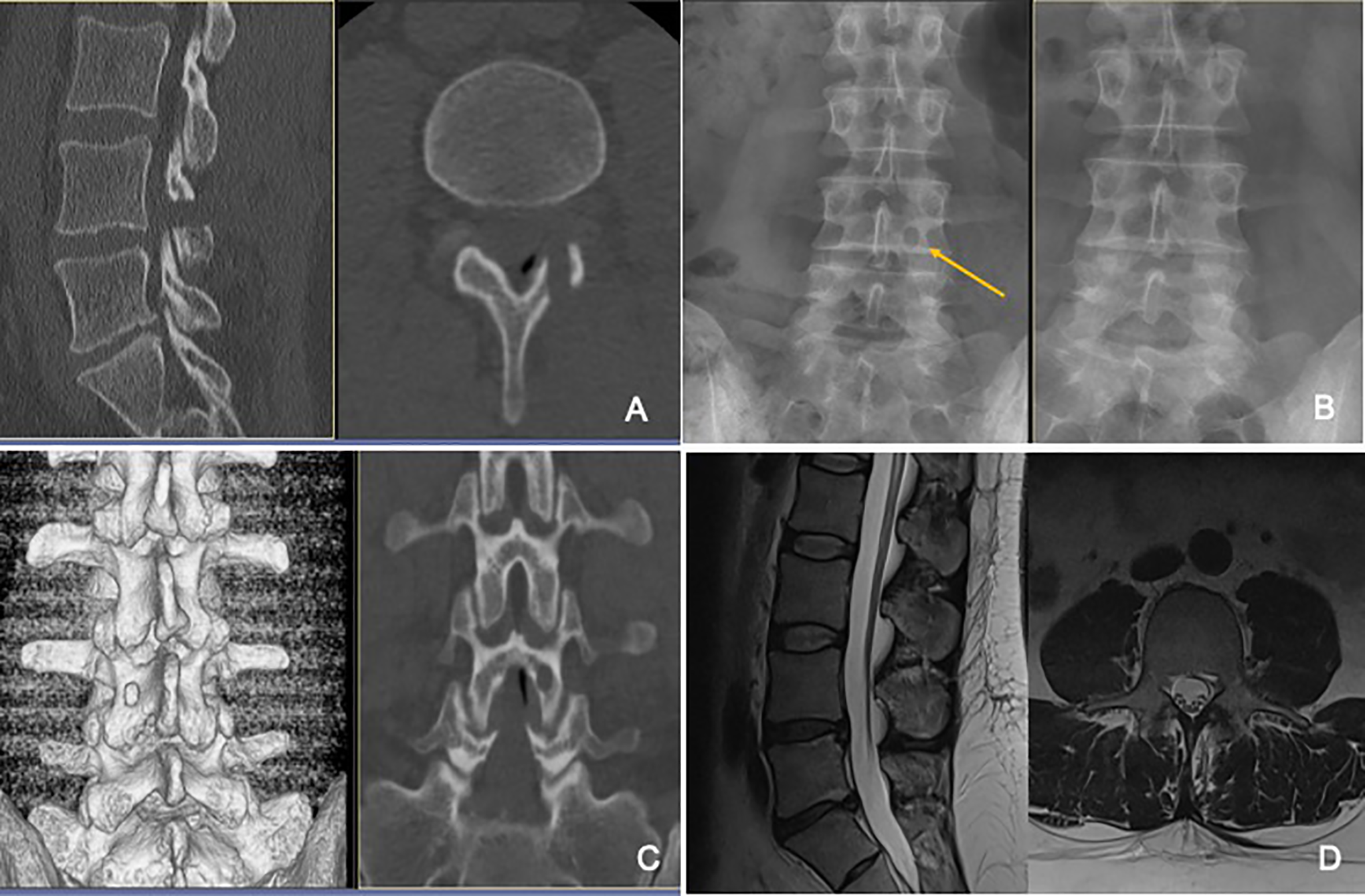
A) Postoperative CT sagittal and axial reconstructions showing the drilled hole in the laminaof L4. B) The pre- and postoperative plain x-ray showing the hole in the lamina on the left image. C) The 3D and coronal reconstruction of the postoperative CT showing clearly the perserved upper and lower border of the lamina and the intact pars interarticularis. D) Postoperative MRI shows the complete removal of the sequestrated disc and the minimal muscle trauma.
Statistical Analysis
The statistical analysis was performed using SPSS version 22.0 (SPSS Inc, IBM Corp, Armonk, NY). A P-value of < 0.05 indicated statistical significance. For the descriptive presentation of results, the absolute and percentage frequency were calculated for categorial variables, while the median, mean, minimum and maximum were calculated for ordinal and quantitative variables. The data showed normal distribution and the paired samples T-test was used to compare means before and after the intervention.
Results
The mean body mass index was 27.5 (range 18–36). The mean duration of symptoms was 24 days (range 1–90 days
The Main Demographic Data of the Study Patients.
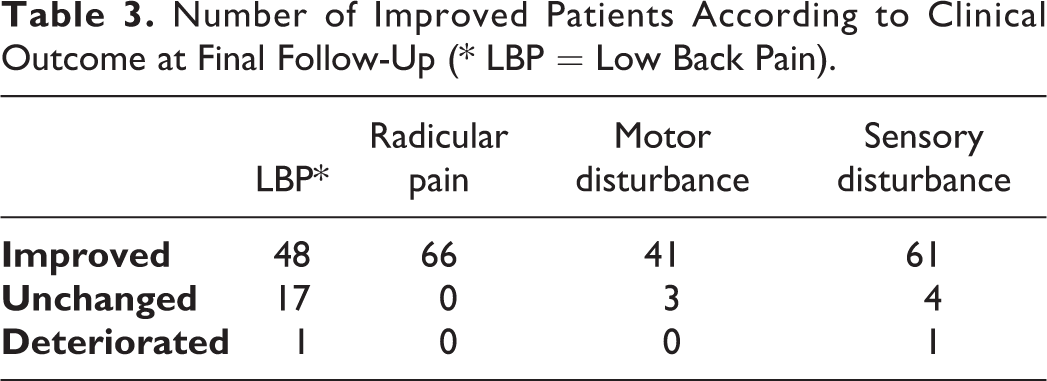
Patients had an average VAS score of 6.44 ± 2.06 (range 2–9) for radicular pain and 3.8 ± 2.19 (range 0–8) for low-back pain before surgery. At the day of discharge from the hospital, the VAS score had decreased to 0.35 ± 0.59 (range 0–2) for radicular pain and 1.29 ± 0.87 (range 0–3) for low-back pain. The improvements in radicular and low-back pain were statistically significant (both P < 0.001). Regarding the patients’ functional status, there was a significant improvement in the mean ODI values, from 50.19 ± 4.92 preoperatively to 10.14 ± 2.22 at the final follow-up (FU) (P < .001). At the final FU, this improvement was maintained, with a mean VAS of 0.12 ± 0.47 (0–3) of leg pain and 1 ± 0.80 (0–4) of back pain. Compared with immediate postoperative values, the change was not statistically significant. The preoperative motor weakness improved at least 1 grade in 41/44 patients (neurological improvement rate (NIR) of 93%) (Table 3). One patient had persistent dysesthesia that improved during the first postoperative 3 months. Another patient had instability above the level of herniation and had to be fused 14 months later and showed a fair outcome. No recurrent herniations were observed.
Number of Improved Patients According to Clinical Outcome at Final Follow-Up (* LBP = Low Back Pain).
Sixty four out of 66 patients (96%) showed an excellent or good outcome and fair outcome in 2 Cases with respect to the functional grade according to Macnab (Table 1
Discussion
The frequency of cranio-laterally extruded disc fragments as reported by Ebleling and Reulen was 7%. 11 In our own patient population, 5.7% of all disc herniations were operated on by the trans-tubular TL-MAPN, which clearly indicates the familiarity with the technique. Removal of the fragment without disc excision is supported by several publications. Some authors even found it superior to conventional disc removal because of the lower rate of postoperative spinal instability and lower rate of re-herniations.5,12-14 Many studies1,8,15,16 reported similar trans-laminar approaches, however, through a normal open approach. The possibility of using a tubular retractor system in combination to minimize approach-related trauma was also reported.3,17,18 The standard interlaminar exposures with upward 2 or downward laminotomy 19 for the foraminal LDH in the hidden zone were also described.
Placement of the bony fenestration should be planed depending on the localization of the herniation. 20 Crossover translaminar approach was recently described by Reinshagen et al. 21 The entry point was through the medial portion of the contralateral lamina, just at the base of the spinous process. This approach was recommended for recurrent LDH to avoid operating directly through scar tissue.
Vanni et al 22 stressed on the possibility to spare the flavum ligament as one of the main advantages of trans-laminar technique. They used the technique for LDH in the pre-foraminal zones, for the levels above L2–L3, and in the pre-foraminal and foraminal zones, for the levels below L3–L4. Recently, percutaneous translaminar endoscopic approach was described for down-migrated LDH under local anesthesia without any dural or neural injuries. 23 For the treatment of purely foraminal LDH, De Bonis et al 24 reported on 47 patients using trans-pars microscopic approach with drilling the lateral border of the pars interarticularis. There were no cases of spinal instability and no recurrence at the follow-up. Compared to interlaminar approach, trans-laminar approach provided more relief from back pain and improved quality of life better than the conventional interlaminar approach. 25 Comparing interlaminar, translaminar and endoscopic transforaminal surgical approaches in the treatment of LDH in the hidden zone. It was found that all 3 surgical approaches led to a significant reduction of preoperative pain. The interlaminar and translaminar techniques were the safest and fastest ways of gaining access to cranially migrated disc material and also proved to be the most effective approaches over a period of 6 weeks and the most successful in relieving pain. The endoscopic transforaminal approach was relatively unsuitable for the removal of cranially displaced disc fragments. By contrast, endoscopic translaminar and endoscopic interlaminar approaches may lead to better results in the future. 26 To reduce the surgical trauma, we combined the TL approach with the use of a working tube
(trans-tubular) that is inserted after blunt dilatation of the paraspinal muscles, followed by use of surgical microscope. This technique has been described by several authors for use in lumbar discectomy and decompression procedures.27,28 It preserves as many normal muscular and ligamentous attachments to the spine as possible and accordingly, beneficial for the long-term maintenance of spinal stability and alignment. 29 This becomes more relevant as the cranial sequestration is strongly correlated with increased age. 30 The mean age in our study was 59 years. Such patients are more likely to suffer from osteoporosis and degenerative spinal disorders such as facet joint hypertrophy, which may manifest segmental instability.
Radicular motor weakness is commonly encountered is this group of patients. It may be due location of the herniation with less space available for nerve root and also because of the vulnerability of neural elements in elderly patients.
The use of microscope is easy and familiar to most spine surgeons. In contrast to endoscopy, it offers the benefits of a 3-dimensional perspective. The use of endoscopy is a valuable alternative; however, it is difficult to reach these cranially migrated fragments and it entails a long learning curve.
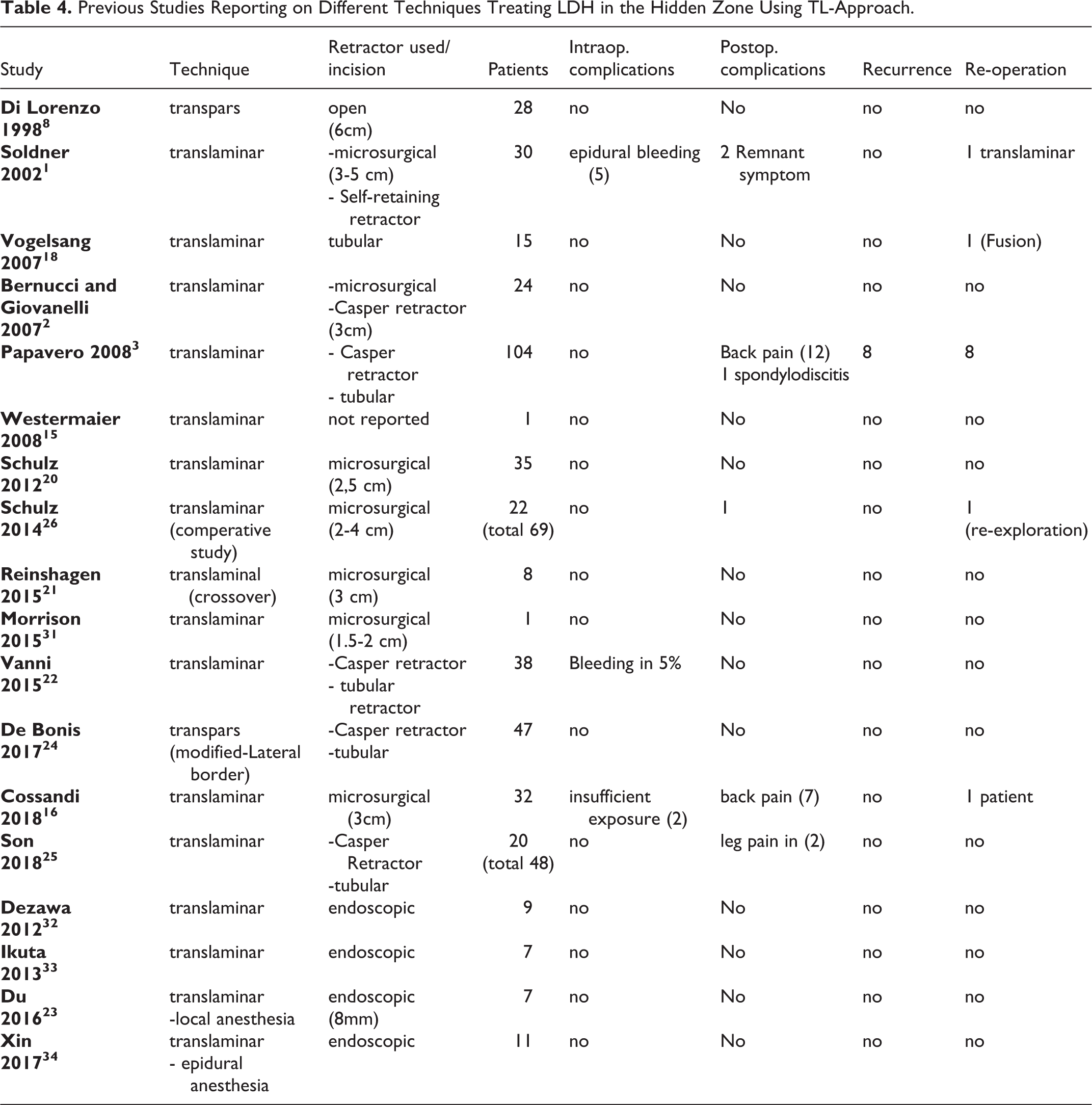
The main strengths of this study are the number of patients, homogenous pathology, and technique. However, the absence of a control group and randomization are the main weaknesses. The authors tried to overcome this comparing our results to the published results using different techniques for such pathology
Previous Studies Reporting on Different Techniques Treating LDH in the Hidden Zone Using TL-Approach.
Conclusion
In conclusion, access to the hidden zone remains surgically challenging. TL-MAPN represents a valuable reproducible alternative in treatment of LDH in this zone. It is a tissue-preserving minimal invasive technique in such cases. The ligamentum flavum, the pars interarticularis and the facet joint are preserved. It is a minimal invasive technique with minimal morbidity. Clinical outcomes, complications, recurrence, and re-operation rate are comparable with other techniques. The approach allows access to the extruded cranial migrated disc fragment and intervertebral disc space comparable to classical approaches.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.