
Abstract
Study Design:
This is a retrospective cohort study using a nationally representative administrative database.
Objective:
To identify the impact of obesity on postoperative outcomes in patients undergoing thoracolumbar adult spinal deformity (ASD) surgery.
Background:
The obesity rate in the United States remains staggering, with approximately one-third of all Americans being overweight or obese. However, the impact of elevated body mass index on spine surgery outcomes remains unclear.
Methods:
We queried the MarketScan database to identify patients who were diagnosed with a spinal deformity and underwent ASD surgery from 2007 to 2016. Patients were then stratified by whether or not they were diagnosed as obese at index surgical admission. Propensity score matching (PSM) was then utilized to mitigate intergroup differences between obese and nonobese patients. Patients <18 years and those with any prior history of trauma or tumor were excluded from this study. Baseline demographics and comorbidities, postoperative complication rates, and short- and long-term reoperation rates were determined.
Results:
A total of 7423 patients met the inclusion criteria of this study, of whom 597 (8.0%) were obese. Initially, patients with obesity had a higher 90-day postoperative complication rate than nonobese patients (46.1% vs 40.8%, P < .05); however, this difference did not remain after PSM. Revision surgery rates after 2 years were similar across the 2 groups following primary surgery (obese, 21.4%, vs nonobese, 22.0%; P = .7588). Health care use occurred at a higher rate among obese patients through 2 years of long-term follow-up (obese, $152 930, vs nonobese, $140 550; P < .05).
Conclusion:
Patients diagnosed with obesity who underwent ASD surgery did not demonstrate increased rates of complications, reoperations, or readmissions. However, overall health care use through 2 years of follow-up after index surgery was higher in the obesity cohort.
Introduction
Adult spinal deformity (ASD) is a common pathology, especially among individuals aged 65 years and older, where its prevalence is as high as 65% in some reports. 1 -3 ASD includes a broad range of degenerative pathologies that, in the presence of sagittal imbalance, can have significant impact on quality of life and overall health outcomes. 4 -6 Historically, the treatment of ASD included few surgical options because of the high-risk nature of the procedure, though in recent decades improvements in surgical technique, anesthesia, and critical care have led to an increase in these operations. 7 These surgical interventions have been successful in lessening the significant burden of pain and disability faced by these patients 8 ; However, ASD surgery remains complex, with rates of complications ranging from 34% to 75%. 4,9 -14
Obesity is an epidemic in the United States, with the Centers for Disease Control estimating the prevalence of obesity to be 39.8% in 2016. 15 Within spinal surgery, the impact of obesity on outcomes is controversial. Some studies have shown a correlation between obesity and longer operation times, higher rates of surgical site infection, higher rates of blood loss, increased venous thromboembolism risk, and postoperative complications. 16,17 Other authors report no differences between obese patients and their control counterparts in terms of postoperative complications or morbidity. 18 -20 Finally, one study did find an increase in postoperative complications but, nonetheless, came to the conclusion that the ultimate benefits of surgery for these patients outweigh the increased risk because of an overall increase in health-related quality of life. 5 Most studies analyzing outcomes between obese and control patients have been within select pathologies. 21 Here, we investigate complications and health care costs associated with obese and control patients undergoing thoracolumbar spinal deformity surgery.
The aim of this study is to utilize a large data set to compare complications and costs following thoracolumbar spinal deformity surgery in obese patients and a control group.
Methods
Data Source
This study obtained a sample of the MarketScan Commercial Claims and Encounters database (Truven Health Analytics, Ann Arbor, MI) from January 1, 2007, to December 31, 2016. This database is a collection of commercial inpatient, outpatient, and pharmaceutical claims of more than 75 million employees, retirees, and dependents representing a substantial portion of the US population covered by employer-sponsored insurance. MarketScan contains 53 million inpatient records, 40 million with employer-sponsored insurance, 3.7 million with Medicare Part B, and 6.8 million on Medicaid, for a total of more than 28 billion patient records. Truven Health Analytics MarketScan data sets are publicly available to researchers for a fee per year of data. The MarketScan database contains International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and 10th Revision, Clinical Modification (ICD-10-CM), Current Procedural Terminology (CPT), and Diagnosis Related Group (DRG) codes as well as National Drug Codes (NDC).
Inclusion Criteria
This study identified and included 7423 patients who underwent thoracolumbar deformity surgery (CPT codes 22 800, 22 802, 22 804, 22 808, 22 810, 22 812, 22 818, 22 819, 22 843, 22 844, 22 846, 22 846, or 22 847) and who had a concurrent ICD-9 diagnosis code of spinal deformity (737.xx) between 2007 and 2016. Obesity at the time of index surgery was identified by the presence of ICD-9 diagnosis codes (278.xx). Patients <18 years old or those who had ICD-9-CM codes consistent with prior of history of tumor or trauma were excluded.
Outcomes and Variables
The primary outcome of this study was an overall composite complication rate. Specific complications, length of stay, 90-day readmissions, revision rates, and costs were assessed as well. Given that ASD surgery can occur in a staged manner during a single admission, revisions were defined as the presence of an ASD surgery procedure code after discharge from initial admission. Patient-level variables, including age at diagnosis, sex, geographic region, and quality and cost metrics, were taken directly from the claims data. Complications were assessed using ICD-9-CM codes. A subgroup analysis of osteotomy type was also included.
Analyses and Patient Involvement
The data set was queried to identify patients who underwent primary ASD surgery. Patients were then grouped according to history of obesity diagnosis, and these cohorts were mutually exclusive. To minimize the effect of potential confounding on the direct comparison of patients undergoing ASD surgery with and without obesity, a propensity score match (PSM) was utilized. A greedy nearest-neighbor algorithm was used to match patient cohorts with a 5:1 (nonobese:obese) ratio. A caliper of 0.01 was utilized in the match, and replacement of patients in the algorithm was not allowed. Baseline demographics such as age and sex, and surgical approach were input into the algorithm, leading to the matched covariates having no statistically significant differences. Student t tests and χ2 tests were utilized to assess significant differences in demographic data, baseline comorbidities, postoperative complications, quality outcomes, and payments among the groups. P values were interpreted as significant if less than .05.
Patient Involvement
Because this study includes only analysis of secondary deidentified data, it was not considered human subject research and received exemption from the institutional review board approval at our institution.
Results
Patient Cohort
A total of 7423 patients met the inclusion criteria of this study, of whom 597 (8.0%) were obese. Obese patients were older (51.4 vs 45.5, P < .05) and had a significantly higher comorbidity burden that nonobese patients. Patients with obesity had higher rates of congestive heart failure (CHF), hypertension, diabetes, and previous cardiac arrythmias (P < .05). Obese patients were also more frequently tobacco users (13.9% vs 9.2%, P < .05). Posterior surgical approach was preferred in both cohorts; however, obese patients were less likely to be operated on anteriorly (P < .05). Osteotomy use was consistent between cohorts. After PSM, there were no longer any statistically significant differences in mean age or sex ratios. Approach type was also similar between the control and obesity cohorts (Table 1).
Baseline Characteristics of Patients Undergoing Primary ASD surgery.
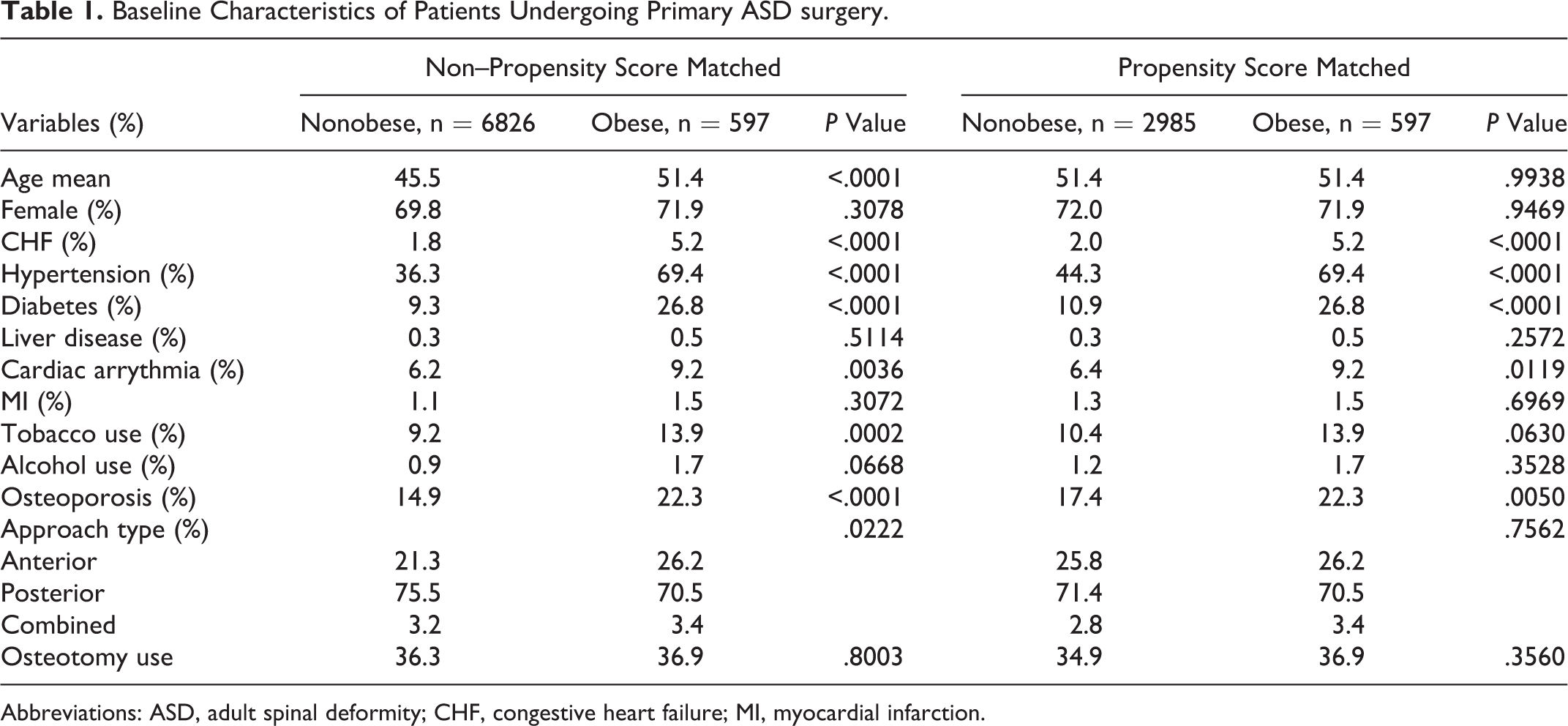
Abbreviations: ASD, adult spinal deformity; CHF, congestive heart failure; MI, myocardial infarction.
90-Day Complication Rates Between Obese and Nonobese Patients
Patients with obesity had a higher 90-day postoperative complication rate than nonobese patients (46.1% vs 40.8%, P < .05). This was primarily driven by elevated rates of posthemorrhagic anemia (32.8% vs 27.3%, P < .05). Acute kidney injury, sepsis, central nervous system (CNS)-related complications, wound complications, and hematoma rates were also higher in obese patients.
After PSM, the overall 90-day complication rate was similar between obese and nonobese patients. The complication rate was 42.4% in the control cohort and 46.1% in the obese cohort. Only wound complications (3.5% vs 2.1%, P < .05) and acute kidney injury rates (4.4% vs 1.7%, P < .05) remained significantly higher in obese patients (Table 2).
Postoperative Complications Within 90 Days.
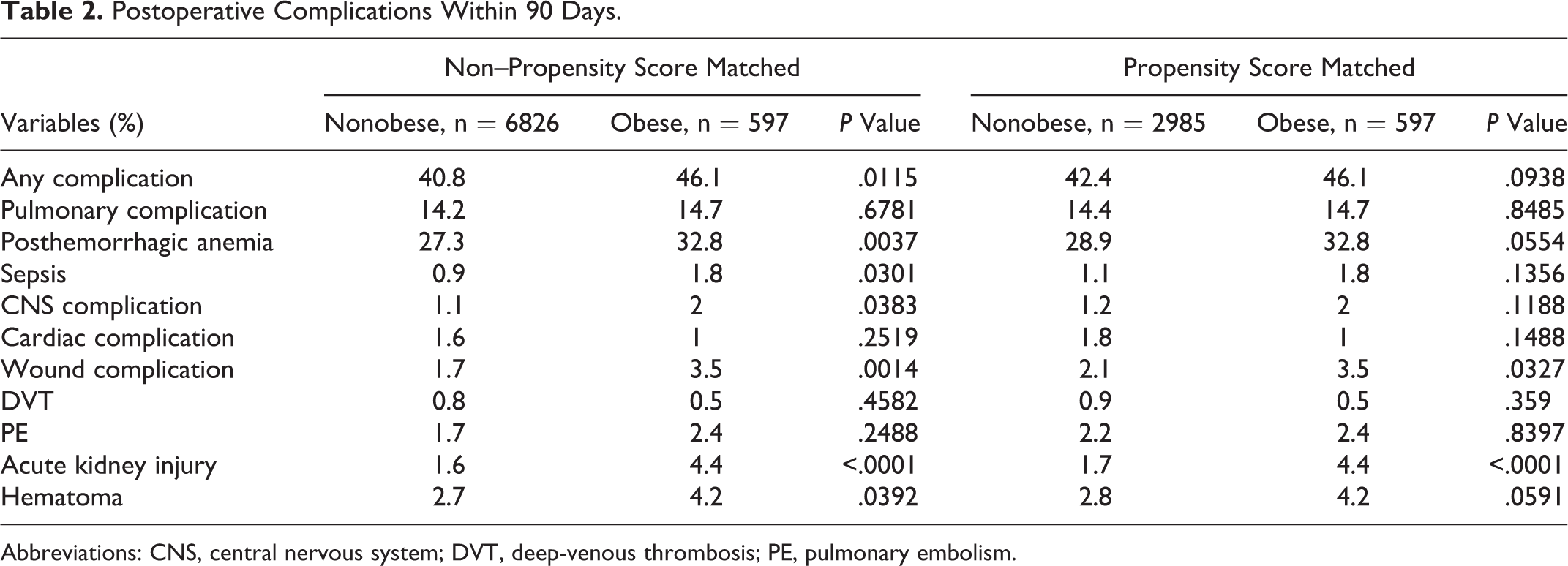
Abbreviations: CNS, central nervous system; DVT, deep-venous thrombosis; PE, pulmonary embolism.
Quality and Health Care Use Outcomes
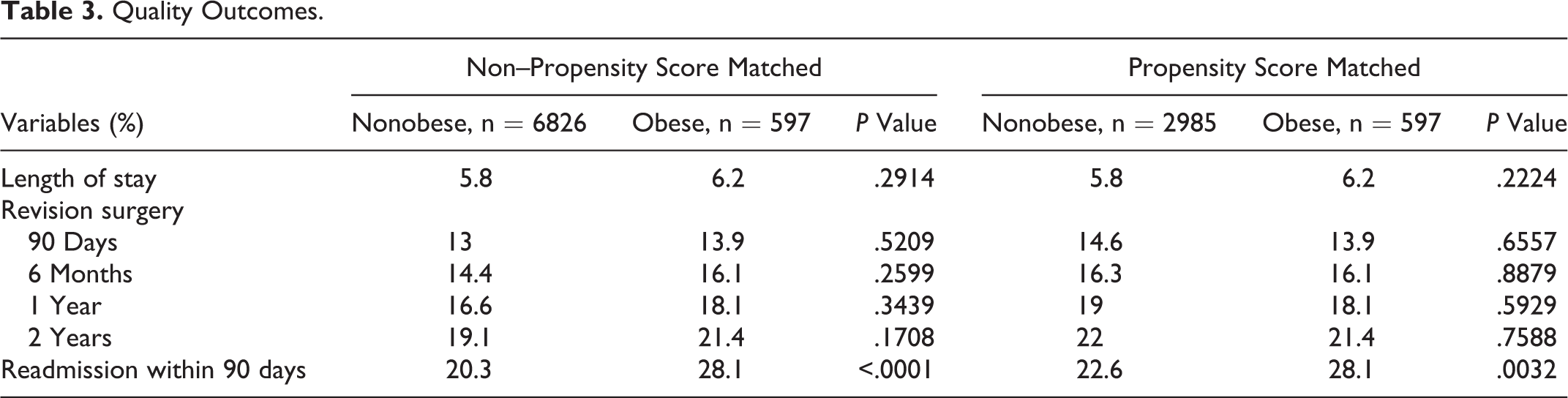
Lengths of stay were similar between obese and nonobese patients (6.2 vs 5.8 days). Revision surgery occurred at a higher rate in the obese cohort. However, the difference in rates at 90 days (13.9% vs 13.0%), 6 months (16.1% vs 14.4%), 1 year (18.1% vs 16.6%), and 2 years (21.4% vs 19.1%) following primary surgery failed to achieve statistical significance. Rates of readmission were higher in patients with obesity (28.1% vs 20.3%, P < .05; Table 3). After PSM, length of stay and revision surgery rate remained similar between cohorts. Readmission rates remained significantly higher in the obese cohort (P < .05).
Quality Outcomes.
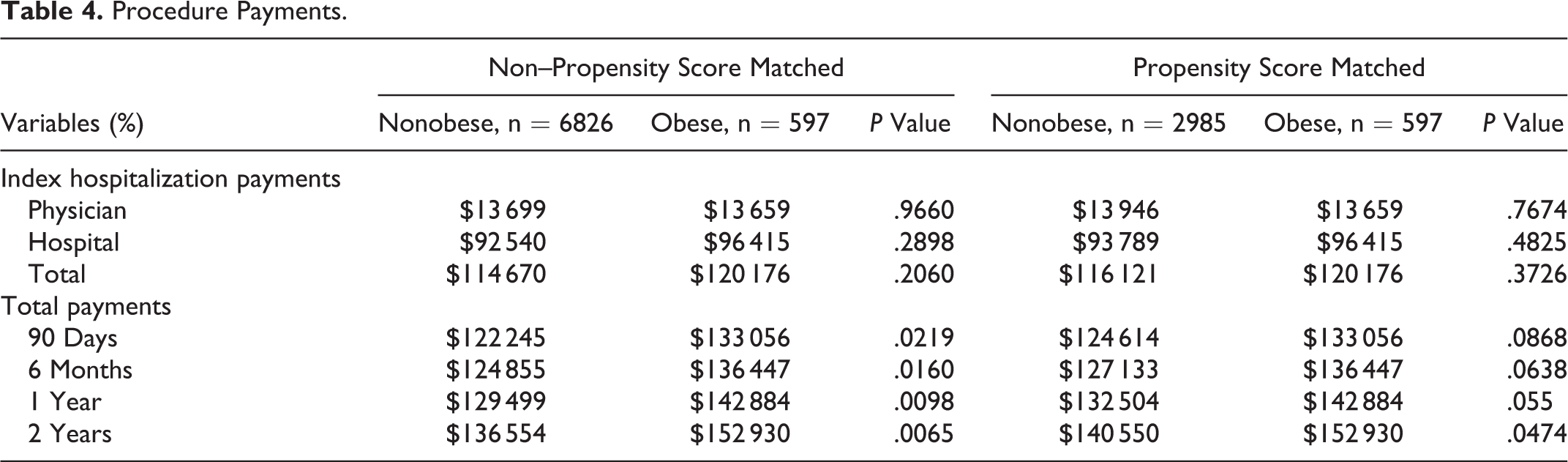
In the non-PSM data, there were no apparent differences in immediate health care use during index hospitalization (control, $114 670, vs obese, $120 176; P = .3978). However, obese patients were associated with higher payments at all time points during follow-up through 2 years (P < .05). After PSM, the only difference in health care use occurred at long-term follow-up of 2 years (obese, $152 930, vs nonobese, $140 550, P < .05; Table 4).
Procedure Payments.
Discussion
Obesity and Postoperative Outcomes
Several prior studies have reported on the relationship between obesity and long-term outcomes and complications following ASD surgery; however, there is no clear consensus as to its impact. Studies with a positive finding include the work of Pull ter Gunne et al, 22 who found an increased incidence of wound infection for obese patients, postulating that the larger amount of subcutaneous fat needed to be retracted led to more cell necrosis and, thus, higher rates of infection. Also, Soroceanu et al 8 found that obese patients had a higher rate of major complications and wound infections, but this did not influence the number of minor complications or the need for revision surgery.
Specifically to thoracolumbar deformities, Yadla et al 20 found no relationship between body mass index (BMI) and the incidence of perioperative minor or major complications. Similarly, Chen et al 23 found that obesity did not affect the outcome of surgical correction for coronal and sagittal scoliotic deformity, which has been affirmed by other authors. 24
Our study found significant differences in postoperative complications between the obese and control cohorts. Specifically, obese patients had a higher rate of overall complications, posthemorrhagic anemia, sepsis, CNS complications, wound infections, acute kidney injury, and hematoma. Obese patients also had a higher rate of readmission than the control cohort. However, obesity is linked with higher rates of many comorbid conditions (hypertension, diabetes, CHF, osteoporosis), which our data similarly demonstrate. 22,23 Thus, many of these findings would largely be a result of not obesity itself but of the sequalae or comorbidities that often present with obesity: CHF, hypertension, and diabetes in this analysis.
Accordingly, our PSM-matched cohort reflected the clinical manifestations of many obese patients, containing a significantly higher percentage of patients with CHF, hypertension, and/or diabetes. Following PSM analysis, the following variables were still significant: increased risk of wound complications, increased risk of acute kidney injury, and increased 2-year payment. Our analysis on wound complication affirms the work by Pull ter Gunne et al 22 : although the effects of obesity and its sequalae on acute kidney injury have not been studied thoroughly, they may be linked to the increased rate of hypertension and arteriolosclerosis in these patients.
In the literature, some studies utilized BMI as a continuous scale, and a gradual increase in back pain and disability with higher BMI could be demonstrated for patients with lumbar degenerative disc disease. 21 Our study and other studies stratified by obese versus nonobese. It is plausible to assume that the longer a patient has been obese, the more comorbidities they may carry, which may not be reflected in a scaled model or in a binary system. Other studies in the literature further stratify obesity into its own categories, 25 which may help elucidate the effects of extreme weight on surgical outcomes. Neither of these characteristics was able to be studied within our population-based data set and warrants further study.
The Effect of Obesity on Cost
The literature on the isolated effects of obesity and cost of thoracolumbar spinal deformity surgery is sparse. Amin et al, 26 in their retrospective review, found that after analyzing 244 ASD patients, class II and III (BMI ≥ 35 kg/m2) obese patients had higher rates of “high episode-of-care costs” (>$80 000). Stephens et al 27 did not find BMI to have a significant impact on cost of adult thoracolumbar spinal deformity surgery in their prospective model of 129 patients. 2 However, this study did not explicitly analyze the difference between an obese cohort and nonobese cohort. In our analysis, we found that obese patients payed more for their care at 90 days, 6 months, 1 year, and 2 years compared with the control cohort. However, after PSM matching, this relationship only remained statistically significant at the 2-year mark, though it approached significance at the 1-year mark. The significant increase in acute kidney disease following the ASD may contribute to this significance. Alternatively, obesity may influence other aspects of long-term management of these patients, such as tolerance to physical rehabilitation. To the authors’ knowledge, our study is the only national database analysis that explores the individual impact of obesity on total cost of adult thoracolumbar ASD surgery.
Limitations
As with all large database studies, interpretations of this study are limited by the retrospective and administrative nature of the data. 28,29 We assumed accuracy of all diagnosis and procedure codes in the database. The MarketScan database aggregates data on commercially insured patients. Because patients, procedures, and clinical outcomes were queried using ICD-9-CM codes, it is not possible to assess the underlying validity of the collected records. A specific concern to this study would be the underdiagnoses and underreporting of obesity, which may have confounded this study’s findings. Although obesity is often recorded in patient’s charts, it is not necessarily billed as a separate code, and for this reason, we may not have been able to capture the full scope of patients with obesity undergoing ASD surgery. There also may have been discrepancies in the degree of deformity between the obese and nonobese cohorts, a factor we were unable to control for. More specific data regarding BMI was also unavailable. However, these data provide novel and useful insight into the tolerability of ASD surgery in obese patients and may aid spine surgeons with patient selection.
Conclusion
In this study, patients with obesity were at no greater risk for postoperative complication and revision surgery; however, obesity may lead to increased health care resource use. The benefits of deformity correction may outweigh the risks, but further prospective research should be conducted to establish the safety of spine surgery in obese patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.