
Abstract
Study Design:
Retrospective cohort study.
Objectives:
We hypothesized that spine surgery patients with a history of bariatric surgery do not differ in expectations of surgery, perceived benefit of surgical intervention, or physician determined outcome of surgery from patients with no history of bariatric surgery.
Methods:
Patients seen in our spine clinic between January 1, 2 009 and December 30, 2 010 were reviewed. Included patients had a history of bariatric surgery and were 18 to 89 years old. We compared their expectations for recovery, self-perceived clinical outcome (Oswestry Disability Index [ODI] or Neck Disability Index [NDI] and visual analog scale [VAS]), satisfaction with surgery, and physician-perceived clinical outcome (Odom’s criteria) to a matched cohort with no such history. Patients were matched by type of surgery (approach, levels, and procedure), diagnosis, sex, body mass index (BMI), weight category, age, and smoking status.
Results:
Of 210 included patients, 89 underwent spine surgery. One bariatric patient could not be matched. Seventeen received cervical spine surgery; 71 received lumbar spine surgery. The 2 cohorts had similar expectations and satisfaction. Patients with no history of bariatric surgery tended to be more satisfied than the bariatric surgery patients, but not significantly so. ODI/NDI and VAS scores were statistically worse for the bariatric cohort. Differences were attributed to differences among lumbar spine surgery patients; neck surgery patients were not different. Odom’s scores were not different between the two.
Conclusions:
Postoperative expectations and satisfaction of bariatric patients are similar to those of nonbariatric patients. Bariatric patients receiving lumbar spine surgery experienced inferior clinical outcomes compared with nonbariatric patients. Cervical spine surgery bariatric patients have similar clinical outcomes as nonbariatric patients.
Introduction
The psychological effects of bariatric surgery on a patient are being investigated and evidence is mixed as to whether or not the patient’s quality of life is improved by the procedure. 1,2 Indeed, suicidal risk has been shown to increase after bariatric surgery. 3 This may be troubling for the spine surgeon, who may elect to operate upon a patient with a history of bariatric surgery, because the impact of patient-perceived outcome of elective surgical intervention in the spine among those who previously sought elective surgery for treatment of their obesity has not been documented. Because of immediate and significant weight loss frequently following bariatric surgery, a patient may have elevated expectations of pain relief or increased function following orthopedic surgery.
When expectations are not met, a patient can express decreased satisfaction, though not always. There is no consensus on the role of patient expectations prior to surgery in surgical success. Positive preoperative expectations are sometimes associated with better postoperative satisfaction, but Toyone found that even if expectations are met, some patients will still be dissatisfied. 4 –6 Some have found that higher preoperative expectations are related to lower postoperative satisfaction. 7,8 On the other hand, McGregor et al 9 found that patients’ preoperative expectations are not correlated to postoperative satisfaction. (McGregor et al’s patients’ preoperative expectations typically exceeded their postoperative achievements. The disparity was greater among patients who attached great importance to achieving good functional outcomes.)
In this retrospective cohort study, we identified those with a history of bariatric surgery who also had spine surgery in a population of patients receiving care at a busy spine center. We assessed their expectations for recovery, their self-perceived clinical outcome (Oswestry Disability Index [ODI] or Neck Disability Index [NDI] and visual analog scale [VAS]), their satisfaction with their surgery, and their physician-perceived clinical outcome (Odom’s criteria) in contrast to a matched cohort with no history of weight-loss surgery. We hypothesized that patients receiving surgical care for spine conditions who also have a history of bariatric surgery have no differences in expectations of surgery, perceived benefit of surgical intervention, or physician determined outcome of surgery, as compared to those with no history of a bariatric procedure.
Methods
Study Design and Approval
This was a retrospective matched cohort study. Patients seen at our private practice, spine specialty center with initial visits between January 1, 2009 and December 30, 2010 were included. Approval was obtained from the local review board prior to study initiation (Allina Health IRB Reference Number 667 783-9) and study patients gave written consent to the investigators to use their medical records for research purposes.
Study Participants
Factors that disqualified patients included refusal of research, age outside of the acceptable range (ages <18 or >89 years), and unavailable records. Patients who met the inclusion criteria were separated into those with and those without bariatric surgery. Those who reported “yes” to having had bariatric surgery in their initial evaluation or on their self-intake form comprised the bariatric surgery group. The kind of bariatric procedure received was not recorded.
Bariatric surgery patients with spine surgery were matched against spine surgery patients who had not had weight-loss surgery. The primary matching criteria was the type of surgery including surgical approach, number of levels (1-2, >2), and diagnosis (International Classification of Diseases, Ninth Revision [ICD-9] code). Secondary match criteria were then used if possible, including the number of diagnoses relevant to the surgery, sex, body mass index [BMI] weight category, 10 age, and smoking status.
Variables
Patient demographics included age, sex, height, weight, BMI, BMI weight category, and smoking status. Health history included the onset of condition, diagnoses, and comorbidities. Comorbidities were not weighed or aggregated. Surgical details included type of spine surgery, surgical approach, and number of operated levels. Self-evaluated outcomes included expectations, satisfaction, ODI or NDI, and back and leg pain or neck and arm pain (VAS). For preoperative scores, the investigators used responses with dates closest to the date of surgery; for postoperative scores, responses dating closest to a 1-year follow-up were used.
Our primary postoperative outcome was the patient’s perceived benefit of surgical intervention. We assessed this through 6 quality-of-life and function questions and 1 satisfaction question. The quality-of-life and function questions targeted their expectations of complete pain relief, moderate pain relief, the ability to do more activities, the ability to sleep more comfortably, the ability to go back to work, and the ability to do more sports after surgery. A 5-point scale (1 being “not likely” and 5 being “extremely likely”) was used. The patient’s satisfaction with his or her quality of life was recorded pre- and postoperatively with the question, “If you had to spend the rest of your life with your back (or neck) condition as it is NOW, how would you feel?” A 7-point Likert-type scale was used with 1 being “extremely dissatisfied” and 7 being “extremely satisfied.”
Our secondary postoperative outcome was the surgeon’s assessment of postsurgical success. Patients were scored according to Odom’s criteria, 11 which has 4 outcome classifications: excellent (no complaints and able to carry on daily occupations without impairment), good (occasional discomfort that does not significantly interfere with work), fair or satisfactory (subjective improvement but significantly limited physical activities), and poor (no improvement or worse as compared with presurgery). To accurately award these scores, the primary investigator and the co-investigators assessed each patient’s chart notes from various follow-ups and reviewed indicators from patient notes, physician assessments, and physician observations. ODI or NDI scores were not available to the investigators at the time of their review to ensure that the Odom’s scores were independent.
Subanalyses were also performed on cervical spine surgery patients and lumbar spine surgery patients separately.
Data Source
Data was extracted from the patients’ electronic health records within our local hospital system. For preoperative ODI or NDI, VAS, and expectation scores, the investigators used responses closest to the dates of surgery; for postoperative scores, responses closest to a 1-year follow-up were used.
Statistics
Statistical tests used for this analysis included the paired t-test to compare numeric data that was continuous, the Wicoxon signed rank test to compare number of comorbidities (because of its limited range), McNemar for dichotomous binary data, and marginal homogeneity for ordinal data. Statistical tests are named in the tables (given in the Results section). Analyses were performed using SPSS 13.0 for Windows (SPSS Inc, Chicago, IL).
One bariatric surgery patient could not be matched and was therefore excluded.
Results
Of 12 681 total patients, 8136 were eligible for the present study. (The large majority of ineligible patients were ones who had declined to participate in research.) Of the eligible patients, 210 were found to have had bariatric surgery. Eighty-nine of the 210 bariatric patients also had spine surgery. One of these patients was unable to be matched, and was therefore excluded, leaving a total of 88 cases. The workflow is shown in Figure 1.
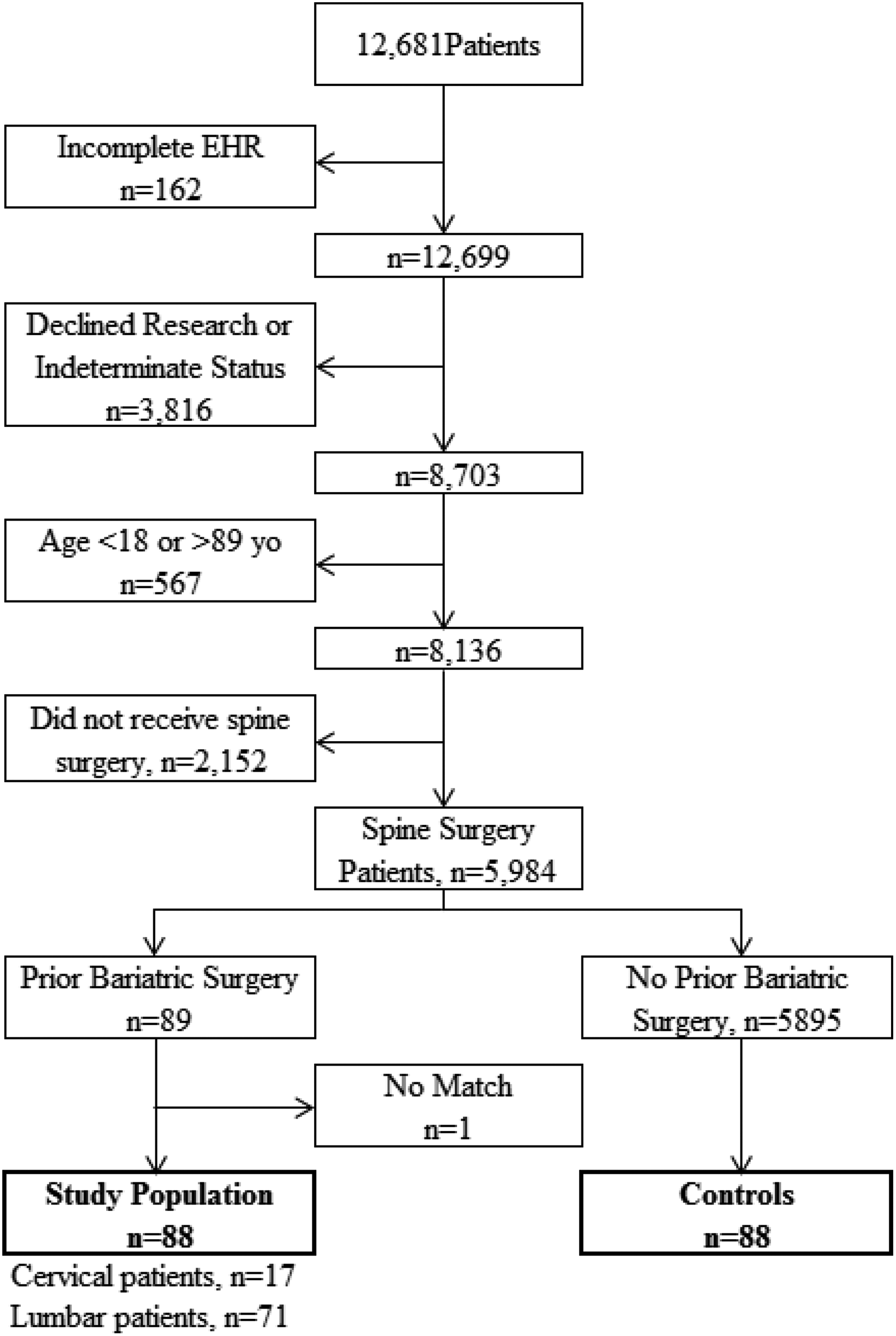
Inclusion and exclusion flowchart.
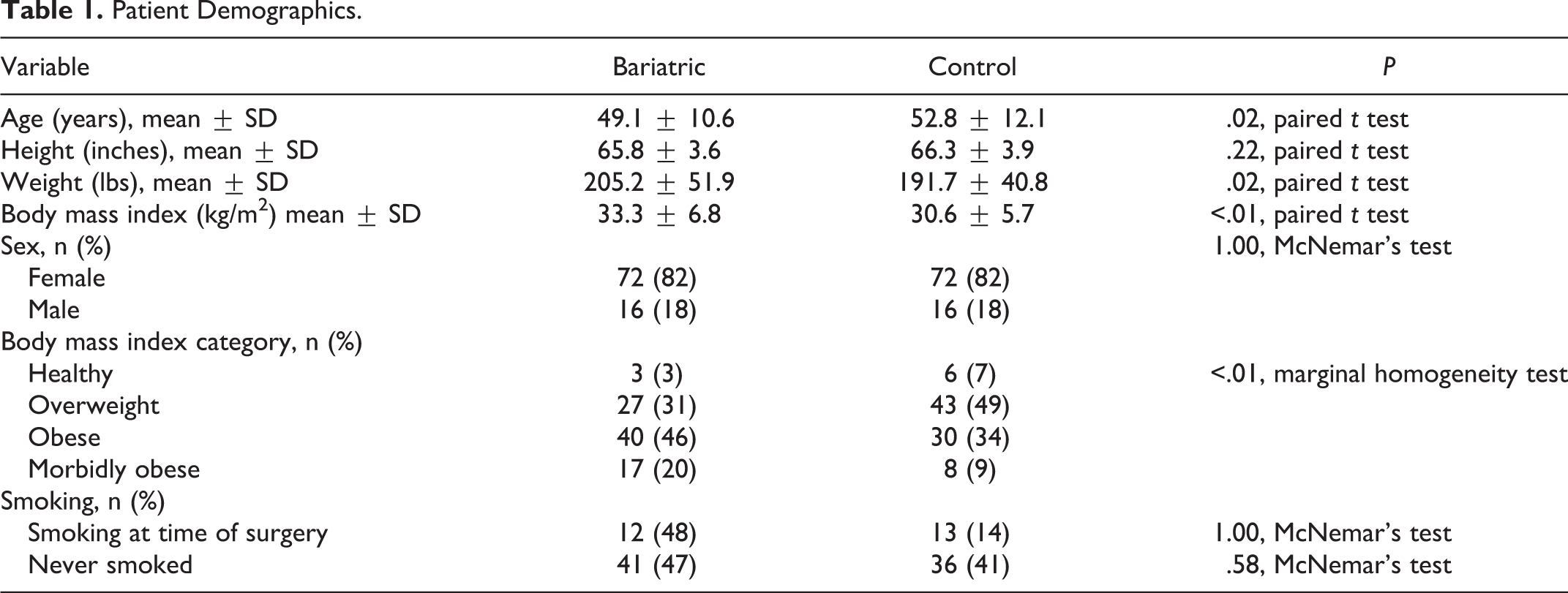
The bariatric surgery patients were not different from the control cohort on height and sex but were younger by about 4 years (Table 1). The weight and BMI of bariatric surgery patients were greater than those of control patients. Control patients were more often in the healthy or overweight categories compared to bariatric surgery patients, who were more often in the obese or morbidly obese categories. Smoking status was not different between the 2 cohorts.
Patient Demographics.
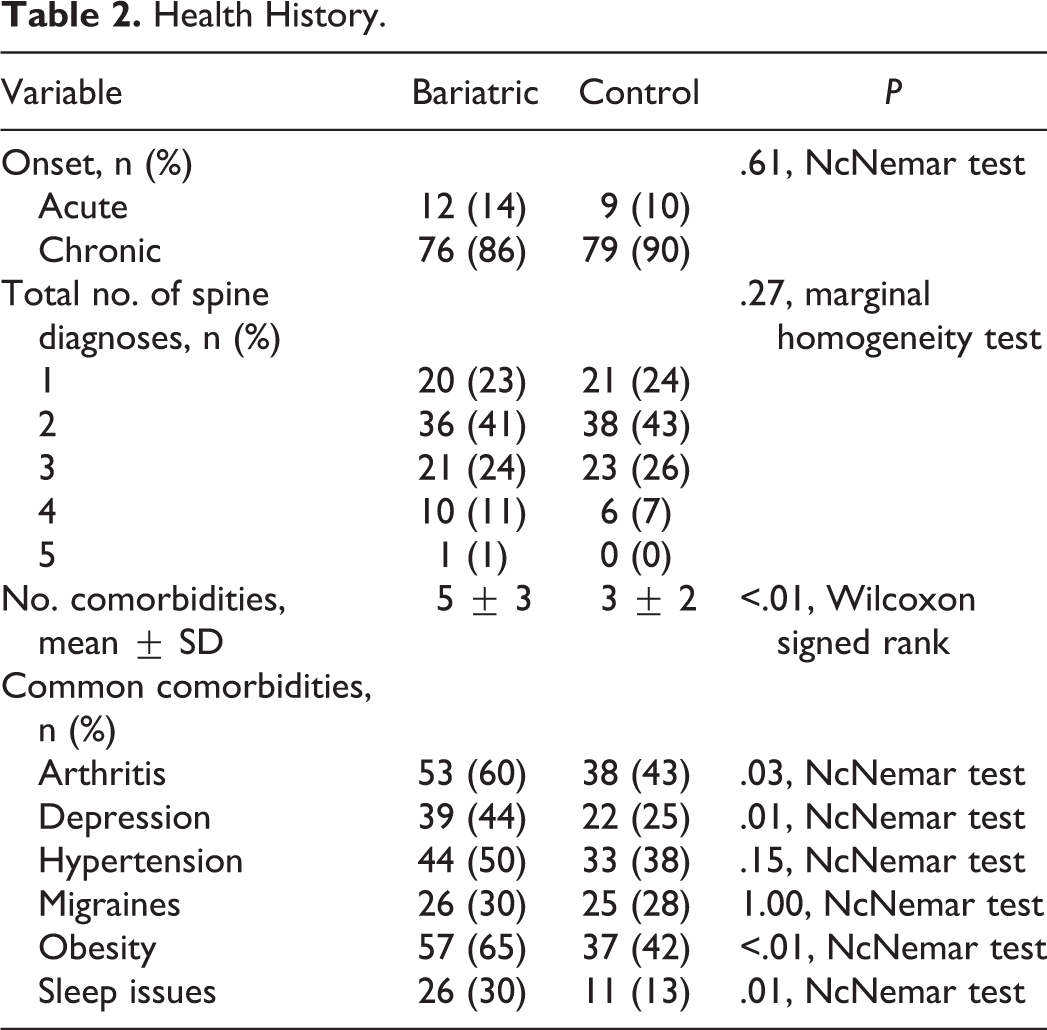
Onset of symptoms was not different between the 2 groups (Table 2). The total number of spine diagnoses likewise was not different between bariatric surgery patients and the control cohort. Bariatric surgery patients suffered from a greater number of comorbidities compared to patients with no history of bariatric surgery. Among the most common comorbidities, bariatric surgery patients exhibited more instances of arthritis, depression, obesity, and sleep issues than control patients.
Health History.
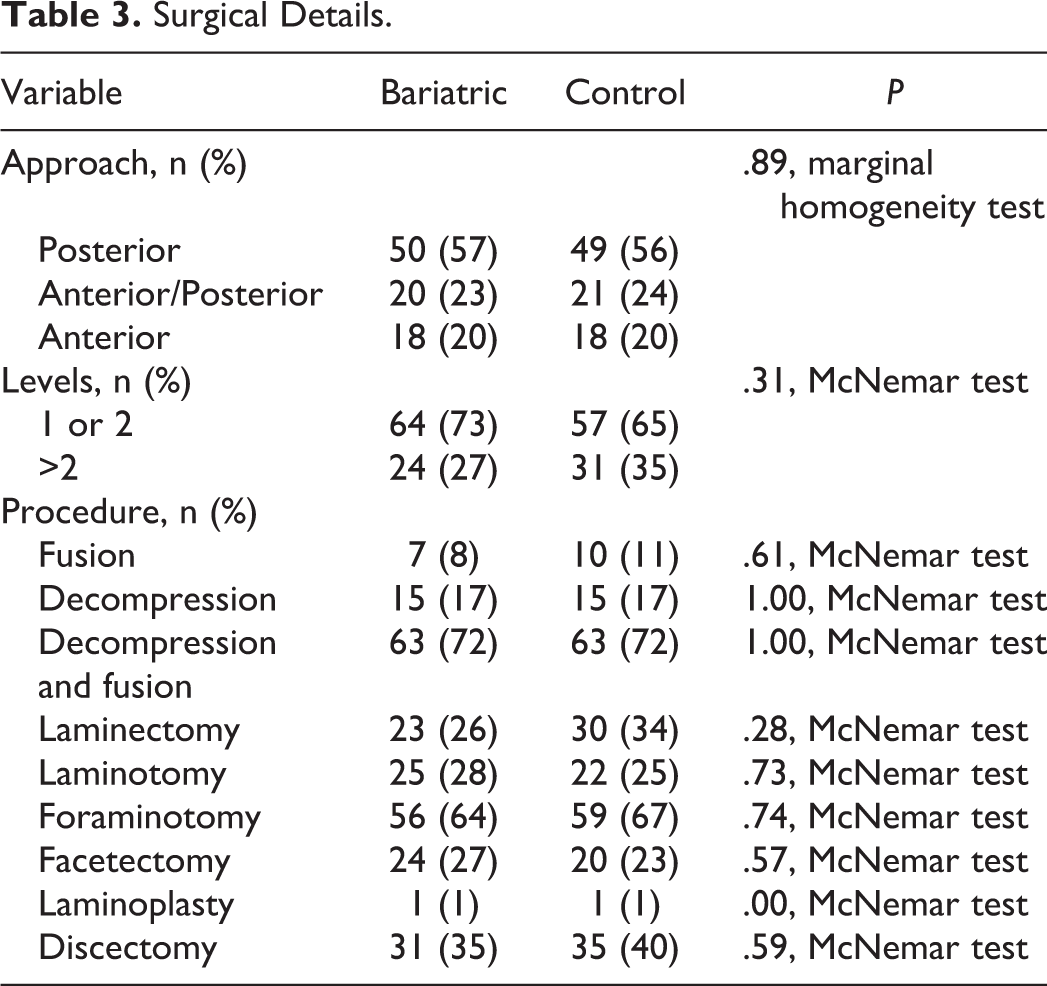
There were no differences between the 2 groups in surgical details (Table 3). The approach (anterior, posterior, or anterior/posterior), the number of operated levels (1-2 or >2) and the kinds of surgical procedures performed were the same for both.
Surgical Details.
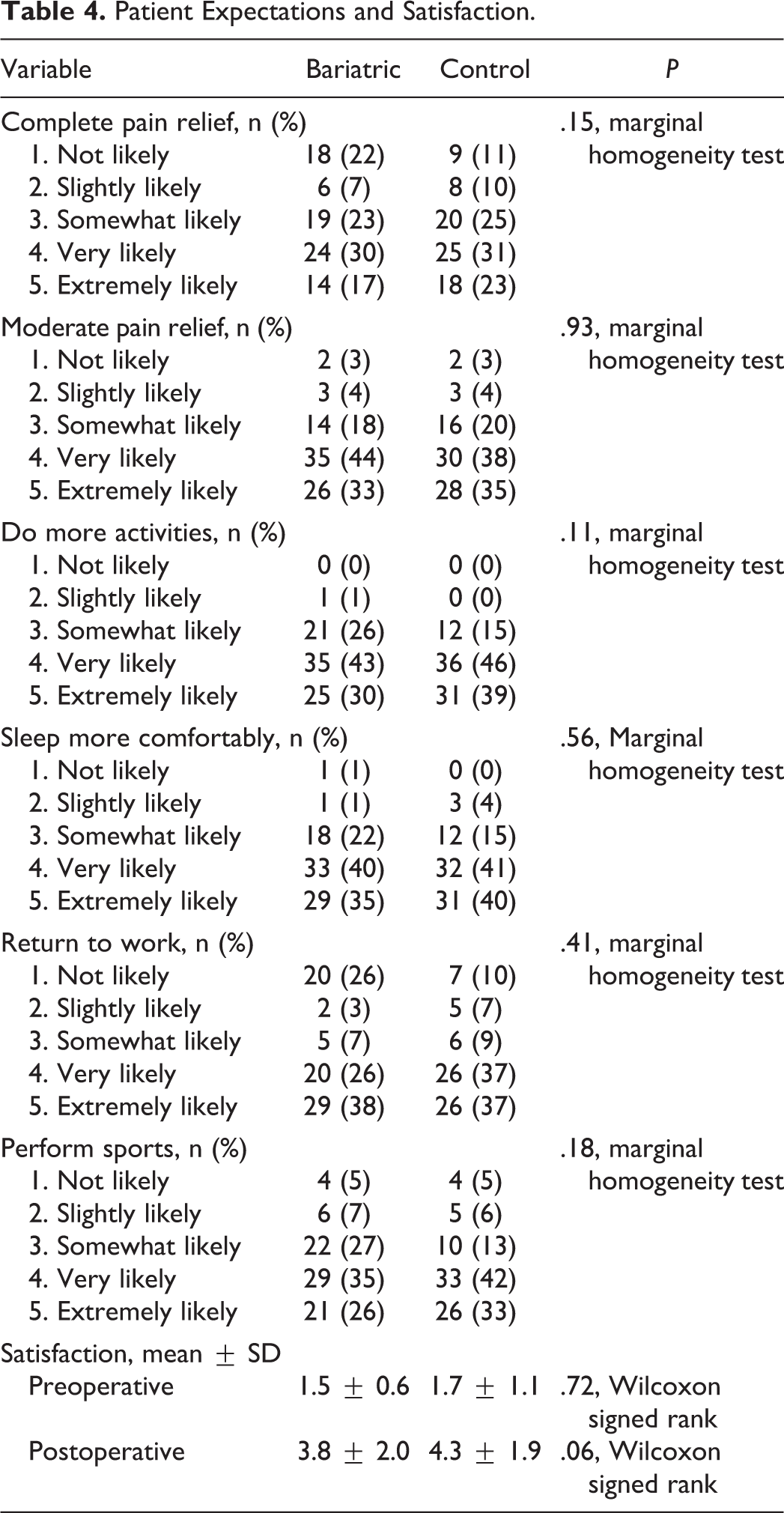
There were no differences between the bariatric surgery cohort and the control cohort in postoperative expectations (Table 4). Patients with no history of bariatric surgery tended to be more satisfied than the bariatric surgery patients, but not significantly so (P = .06).
Patient Expectations and Satisfaction.
Bariatric surgery patients were significantly different (worse) from the control cohort in pre- and postoperative ODI or NDI score and in postoperative pain (VAS) (Table 5). The 2 groups were not different according to the investigators’ assessment of their functional outcome (Odom’s criteria).
Outcomes Results.
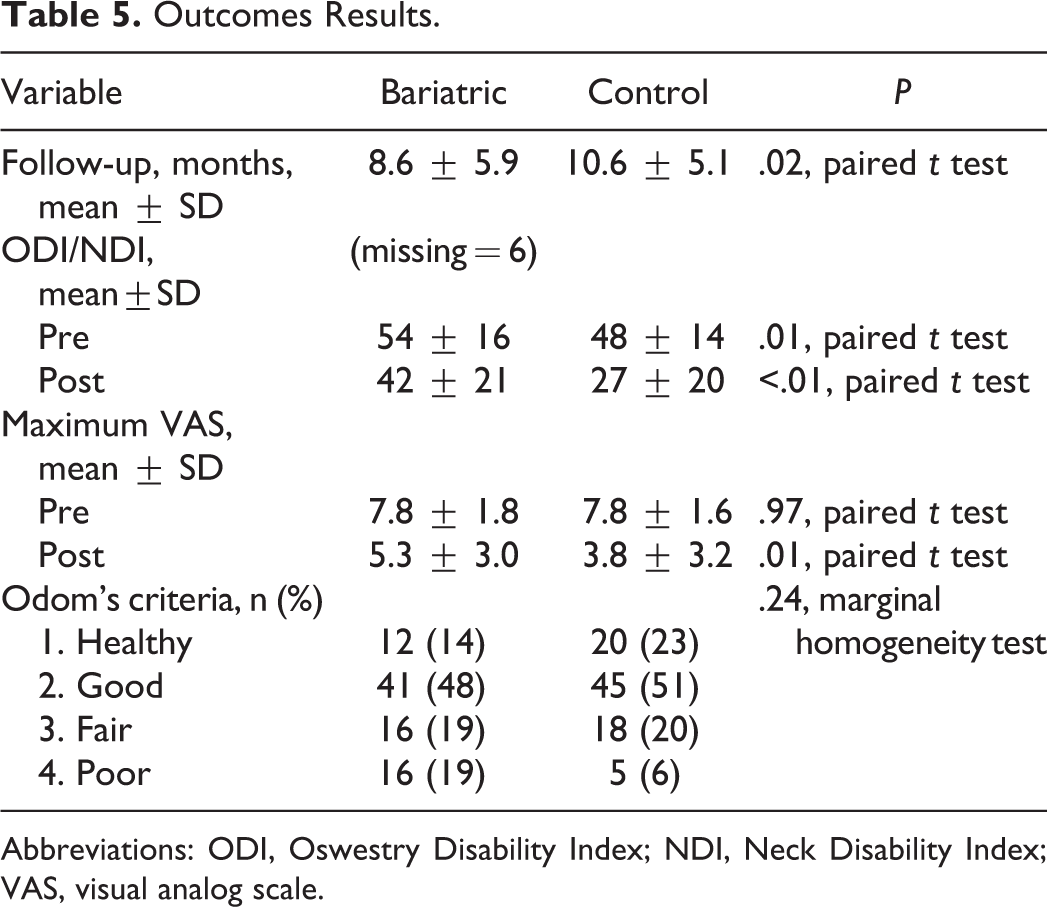
Abbreviations: ODI, Oswestry Disability Index; NDI, Neck Disability Index; VAS, visual analog scale.
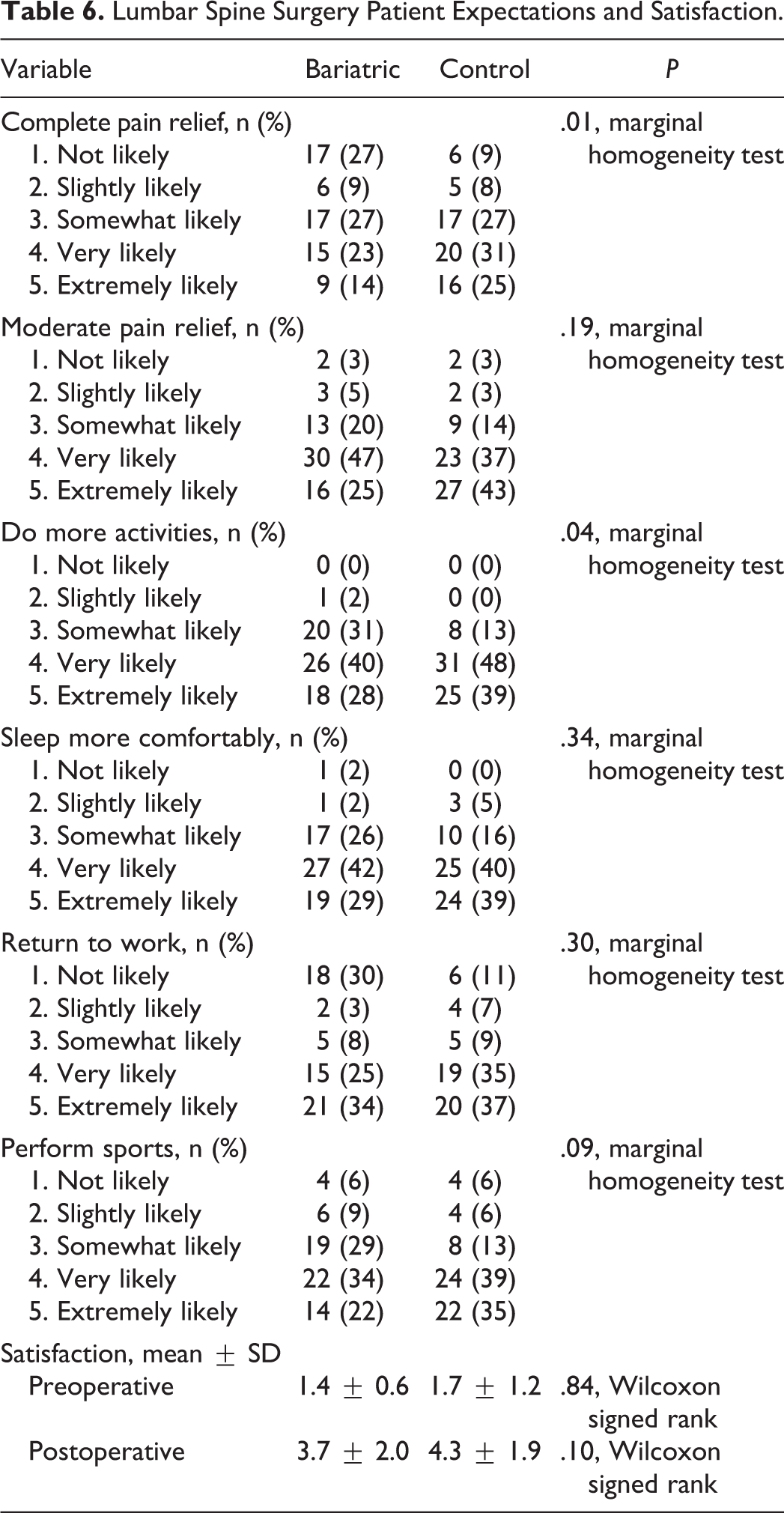
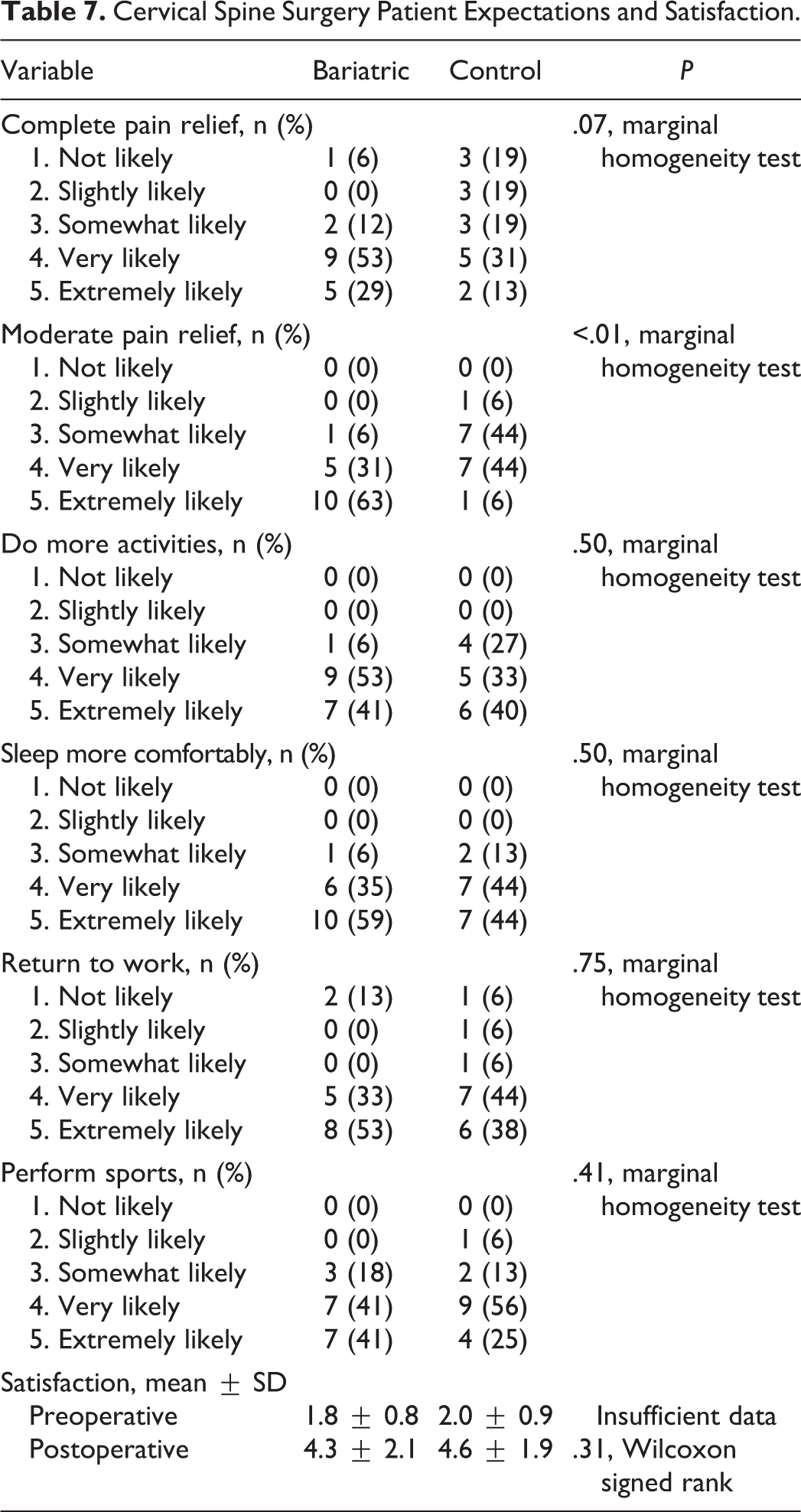
Seventeen patients had cervical spine surgery, and 71 patients had lumbar spine surgery. Among lumbar spine surgery patients, the bariatric cohort had lower expectations for complete recovery and lower expectations to do more activities than the control cohort (Table 6); satisfaction was not different between the 2 groups. Among cervical spine surgery patients, the bariatric cohort had higher expectations for moderate recovery than the control cohort (Table 7). Among lumbar spine surgery patients, the bariatric surgery patients were significantly different from the control cohort in pre- and postoperative ODI score and in postoperative pain (back and leg VAS) (Table 8). The bariatric surgery patients tended to have better functional outcomes based on the investigators’ assessment, but the difference was not statistically significant (P = .06). Among cervical spine surgery patients, the bariatric surgery patients were not different from the control cohort in pre- and postoperative NDI score and in pre- and postoperative pain (neck and arm VAS) (Table 9). The 2 groups were not different according to the investigators’ assessment of their functional outcome.
Lumbar Spine Surgery Patient Expectations and Satisfaction.
Cervical Spine Surgery Patient Expectations and Satisfaction.
Lumbar Spine Surgery Patient Outcomes Results.
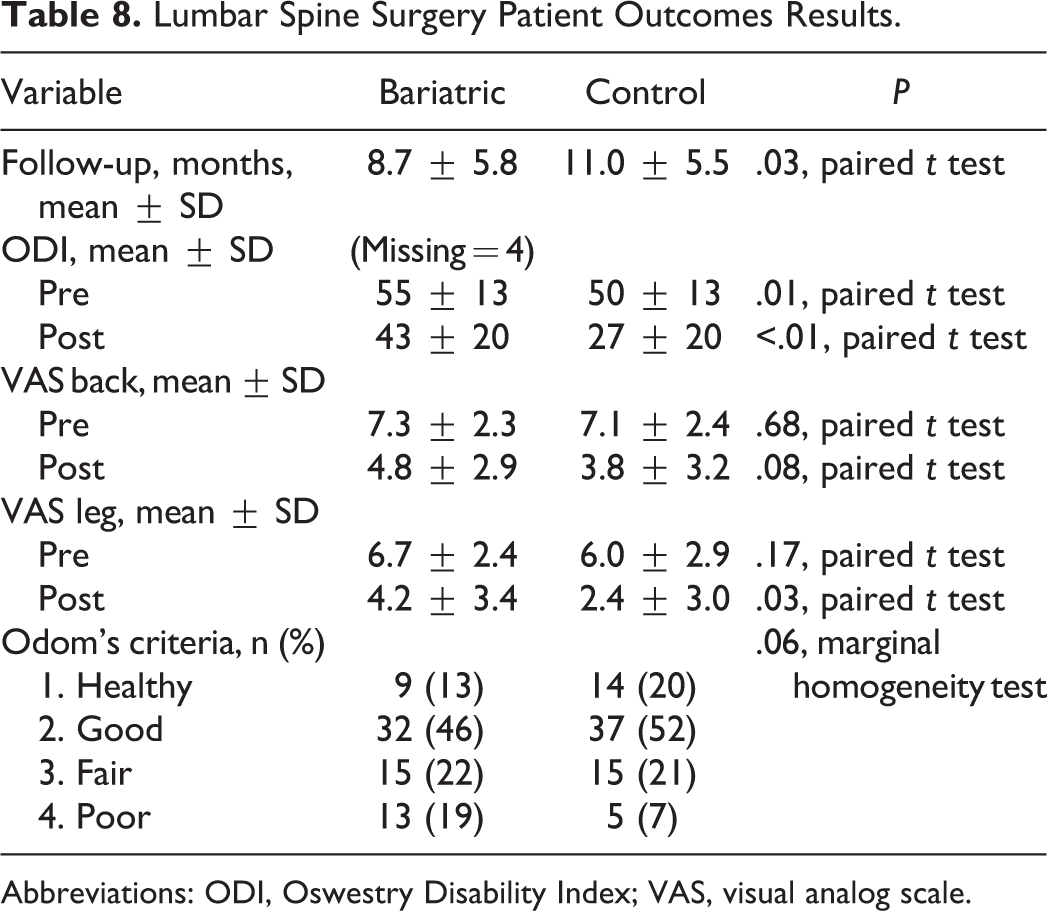
Abbreviations: ODI, Oswestry Disability Index; VAS, visual analog scale.
Cervical Spine Surgery Patient Outcomes Results.
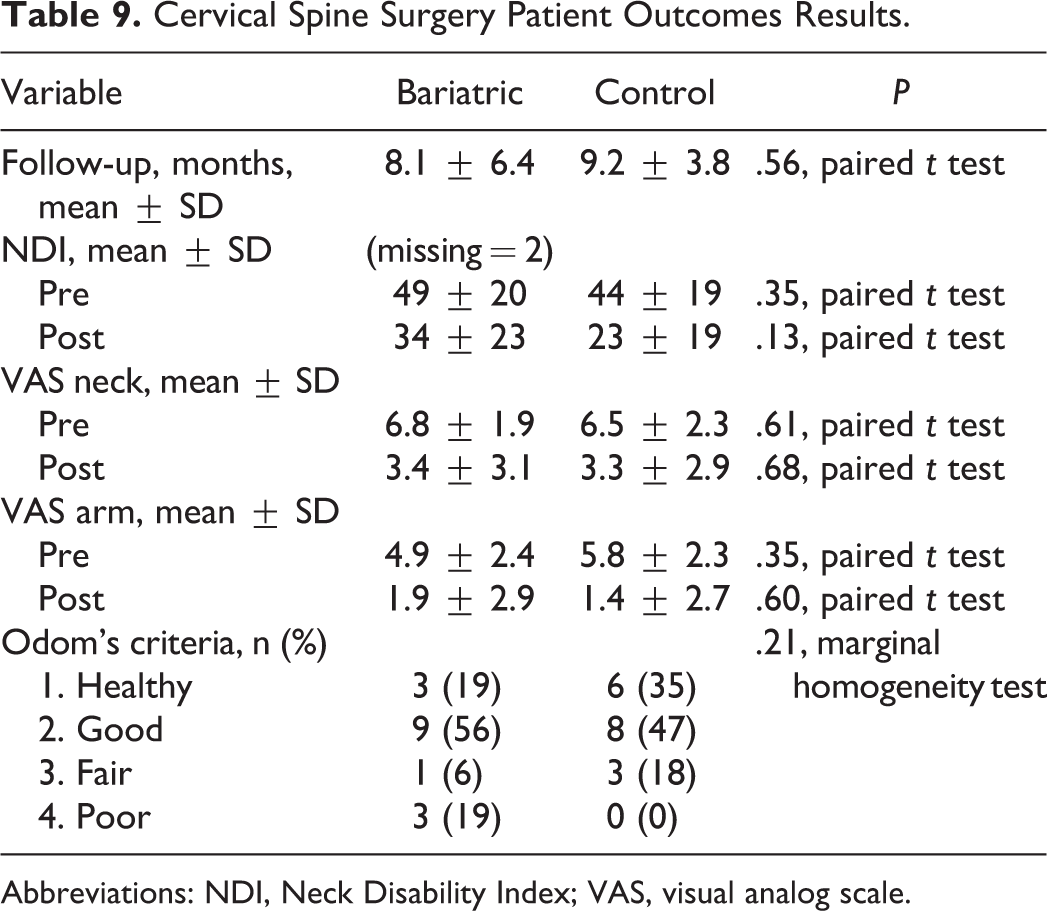
Abbreviations: NDI, Neck Disability Index; VAS, visual analog scale.
Discussion
We hypothesized that patients seeking spine surgery who have a history of bariatric surgery will not differ in expectations after spine surgery from those who have not had bariatric surgery. This hypothesis was supported by the results of this study. Bariatric surgery patients’ expectations for orthopedic spine surgery were not statistically significantly different from the control cohort. This suggests bariatric patients do not have heightened expectations for successful spine surgery in spite of successful weight loss following bariatric surgery. Their expectations for spine surgery are similar to the expectations of others seeking surgical intervention for spine issues.
We hypothesized that the bariatric surgery patients would not be different from the control patients in their perceived benefit of surgical intervention. This hypothesis was not supported by the results of this study. Patients with no history of bariatric surgery tended to be more satisfied than the bariatric surgery patients. Bariatric surgery patients were significantly different (worse) from the control cohort in pre- and postoperative ODI or NDI score and in postoperative pain (VAS).
Hooper et al 12 found that among patients with musculoskeletal pain, 90% of those with neck pain improved after bariatric surgery compared with 83% of patients with low back pain. Wertli et al 13 found that disability and obesity are greater in physical therapy patients presenting with low back pain but not neck pain. Based on these observations, we conducted subanalyses on cervical spine surgery patients and lumbar spine surgery patients separately. Notably, differences between the bariatric surgery cohort and the control cohort were due to differences among the lumbar spine surgery patients and not the cervical spine surgery patients. These results suggest that lumbar spine surgery patients with a history of bariatric surgery may have less chance of achieving as good a functional outcome as patients with no history of bariatric surgery. Among cervical spine surgery patients, there was no difference between those who had had bariatric surgery and those who had not.
Furthermore, we hypothesized that the patients seeking spine surgery who have a history of bariatric surgery will have no difference in physician determined outcome of surgery than those who have not had bariatric surgery. This hypothesis was true: The 2 groups were not different according to the investigators’ assessment of their functional outcome (Odom’s criteria). However, Odom’s scores tended to be higher (better) within the matched cohort compared with the bariatric cohort. As with the ODI and NDI scores, it appears this difference can be attributed to the difference between the lumbar spine surgery patients. Data was insufficient to say whether or not cervical spine surgery patients were statistically different between the 2 types of patients.
Interestingly, the percentage of our patients who had a prior history of bariatric surgery (201 of 12 681, or 1.7%) was more than five times higher than the proportion of bariatric surgery patients as a percentage of the national population (around 0.03%). 14,15 This suggests the incidence of spine issues as a serious side effect of obesity. Khoueir et al 16 showed that weight reduction after bariatric surgery is potentially associated with a lessening of preexisting back pain. Excess weight can put stress on the spine and cause orthopedic health issues, perhaps explaining why a much higher proportion of patients seeking spine care have had bariatric surgery for obesity. The bariatric surgery patients complained of chronic spine problems, possibly stemming from their still elevated BMIs. Indeed, the majority of bariatric surgery patients seeking spine care still had a BMI well within the obese range (65%).
Limitations/Bias
A limitation of this study is the relatively short follow-up period (about 1 year). However, Adogwa et al 17 have recently shown that ODI and VAS scores at 12 months reasonably predict results at 2 years. According to the authors, “…the 12-month measure of treatment effectiveness is sufficient to identify effective versus ineffective patient care.” 17
Another limitation of this study is that the kinds of bariatric surgery procedures that the patients had received were not recorded. It might have been asked of the study participants, but others have shown that patients often forget basic treatment-related facts. 18,19
Because this was a retrospective cohort study, it was not possible to show causality. Another limitation of the study was that the small number of paired cases limited the power to detect differences. Moreover, only existing follow-ups were available for review in this retrospective cohort study.
Conclusion
Overall, the cervical spine surgery patients did better than the lumbar spine surgery patients in both bariatric and matched patients when comparing functional outcome scores, though our small sample size of neck patients limits the statistical power of this observation. Among lumbar spine surgery patients, the bariatric surgery cohort did worse than the control cohort. These trends may help orthopedic surgeons in the future when advising patients with a history of bariatric surgery on the best course of action for treatment of spine issues.
Footnotes
Authors’ Note
This study was reviewed and approved by Abbott Northwestern Hospital IRB by expedited review under 45 CFR 46.110 #(5). Approval was granted on May 12 009.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.