
Abstract
Study Design
Retrospective case-control study.
Objective
This study aimed to identify the underlying pathologies of non-rheumatic retro-odontoid pseudotumors (NRPs), which would help establish an appropriate surgical strategy for myelopathy caused by NRP.
Methods
We identified 35 patients with myelopathy caused by NRP who underwent surgery between 2006 and 2017. An age- and sex-matched control group of 70 subjects was selected from patients with degenerative cervical myelopathy. Radiographic risk factors for NRP were compared between cases and controls. We also assessed surgical outcomes following occipital-cervical (O-C) fusion, atlantoaxial (C1-2) fusion, or C1 laminectomy.
Results
Patients with NRP had significantly lower C1 sagittal inner diameter, C2-7 range of motion (ROM), C2-7 Cobb angle, and C7 tilt, as well as significantly higher C1-2 ROM, atlantodental interval (ADI), and C1-2 to O-C7 ROM ratio. Multivariate regression analysis revealed that ADI, C2-7 ROM, and C7 tilt were independent risk factors for NRP. Neurological recovery and pseudotumor size reduction were comparable among surgical procedures, whereas post-operative cervical spine function was significantly lower in the O-C fusion group than in the other groups.
Conclusion
Non-rheumatic retro-odontoid pseudotumor was associated with an increase in ADI, suggesting that spinal arthrodesis surgery is a reasonable strategy for NRP. C1-2 fusion is preferable over O-C fusion because of the high prevalence of ankylosis in the subaxial cervical spine. Given that 29% of patients with NRP have C1 hypoplasia, such cases can be treated by posterior decompression alone. Our study highlights the need to select appropriate surgical procedures based on the underlying pathology in each case.
Keywords
Introduction
Although a non-rheumatic retro-odontoid pseudotumor (NRP) is a relatively rare non-neoplastic lesion, it is increasingly recognized as a cause of cervical myelopathy in the elderly.1-3 Several surgical strategies such as resection of the pseudotumor via the anterior transoral, or far-lateral or posterior extradural or transdural approach;2,4-8 C1 laminectomy without fusion (posterior indirect decompression);9-11 occiput-cervical (O-C) fusion;12-15 and atlantoaxial (C1-2) arthrodesis surgery 15-22 have been reported for NRP. However, to date, there is no consensus regarding surgical strategies.
The most probable reason for the lack of an established surgical treatment for NRP is the challenge in directly removing a pseudotumor because of the difficulty in accessing the lesion due to its anatomical location. Another reason is that diverse underlying conditions, including congenital and degenerative factors, are associated with the development of NRP. From a pathological perspective, any condition that causes minor chronic damage to the transverse ligament can produce reactive fibrocartilaginous tissue behind the odontoid process. In this regard, posterior O-C or C1-2 arthrodesis surgery has been considered as an appropriate strategy for NRP. Spontaneous mass regression after posterior fusion surgery, even in cases without atlantoaxial instability, supports this idea. A recent study reported a favorable neurological recovery after C1 laminectomy alone and hence proposed C1 laminectomy as an alternative treatment strategy for NRP.9,11 This finding suggests that a suitable surgical strategy may differ according to the underlying conditions of each patient with NRP. Therefore, a comprehensive understanding of the underlying conditions for NRP is needed to establish a suitable surgical strategy for NRP.
In this study, we aimed to identify the underlying conditions of NRP using a matched case-control study and compare the surgical outcomes of O-C or C1-2 arthrodesis surgery and C1 laminectomy for NRP exhibiting myelopathy, the knowledge of which would help determine appropriate surgical strategies for each pathology.
Materials and Methods
Patients
The inclusion criteria were adult patients (aged >18 y) who developed myelopathy because of NRP and who underwent surgery for NRP at one university hospital and 6 branch hospitals between 2006 and 2017. In this study, a retro-odontoid pseudotumor was defined as a mass lesion with an anteroposterior diameter ≥5 mm on sagittal T1-weighted magnetic resonance imaging (MRI). Retro-odontoid pseudotumors with rheumatoid arthritis, hemodialysis, os odontoideum, or odontoid fractures were excluded. During the specified period, 35 patients were identified to have cervical myelopathy caused by NRP. Among them, 31 patients were followed up for more than 2 y (mean ± standard deviation, 29.2 ± 10.9 months; range, 24–48 months).
An age- and sex-matched control group of 70 subjects without NRP (a 2:1 ratio of control group patients to NRP group patients) was selected from the patients who underwent laminoplasty for degenerative cervical myelopathy (DCM) in the database of our hospitals. One reason we chose patients with DCM who underwent surgery as a control group was that their medical records contained information necessary for this study, including radiographs, computed tomography (CT), and MRI of the cervical spine. The exclusion criteria for the control group were rheumatoid arthritis, hemodialysis, congenital cervical disorders, or cervical fractures.
This study was approved by our institutional review board (approval number: 014-0383) and was conducted per the guidelines of the Declaration of Helsinki. The study was based on data obtained from medical records and imaging findings of 35 patients with NRP and 70 control patients with DCM, and the need for patient-informed consent was waived owing to the retrospective nature of the study and the deidentified data used.
Outcomes
The medical records of 35 patients with NRP were reviewed to assess demographic data, neurologic impairments, radiographs, and surgical outcomes. Degenerative changes or anatomical variations that we considered as possible radiographic risk factors for pseudotumor formation were atlantoaxial instability, degeneration of atlantoaxial joints, hypoplasia of the atlas, ankylosis of the occipito-atlantal joint, and ankylosis of the subaxial spine.
Atlantoaxial instability was defined as an atlantodental interval (ADI) >4 mm or positional change in ADI >4 mm. Degeneration of the anterior atlantodens and atlantoaxial facet joints was quantified according to the grading system described by Betsch et al.23,24 Patients with grade 2 (moderate) and grade 3 (severe) degeneration were considered to have osteoarthritis (OA), whereas those with grade 1 (none or mild) degeneration were considered to have no OA. Hypoplasia of the atlas was determined based on a C1 sagittal inner diameter ≤29 mm.19,25,26 Since there was no case with congenital agenesis of the posterior arch of the C1 in this case series, C1 hypoplasia was defined as a congenital small atlas ring in this study. Ankylosis of the cervical spine was assessed by measuring the range of motion (ROM) of O-C1, C1-2, and C2-7 on preoperative flexion-extension radiographs and based on their appearance on CT reconstruction images. Ankylosis of the subaxial cervical spine was defined as a C2-7 flexion/extension ROM of <20°, referring to the values of ROM in asymptomatic Japanese individuals aged 70–79 y 27 Spondylosis with bridging spur formation or the presence of syndesmosis or ossification of the longitudinal ligaments in the subaxial cervical spine was also investigated in cases of ankylosis of the subaxial cervical spine. Ankylosis of the occipito-atlantal joint was determined based on O-C1 ROM and CT reconstruction images of the occipito-atlantal joint. To estimate the relative stress concentration to the C1-2 segment, we calculated the C1-2 to O-C7 ROM ratio (%).
Surgical procedures were identified from the medical records. The severity of myelopathy was evaluated before and after the operation using the Japanese Orthopedic Association scoring system (JOA score). The surgical outcome was rated using Hirabayashi’s recovery rate [100 × (post-operative JOA score—preoperative JOA score)/(17—preoperative JOA score)]. Post-operative cervical spine function was assessed using the Japanese Orthopedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ) from the latest follow-up. Changes in pseudotumor size before and after surgery were evaluated by measuring the anteroposterior diameter of the pseudotumor on MRI.
Statistical Analyses
JMP Pro version 15 (SAS Institute Inc, Cary, NC, USA) was used for the statistical analyses. The differences in the measured variables between the two groups were analyzed using the Student’s t-test or Fisher’s exact test, as appropriate. Multivariate logistic regression analysis was performed to identify risk factors for the occurrence of NRP. The selection of a priori variables was based on previous literature and their clinical importance. Linear regression was used to calculate correlations between ADI and other variables using Pearson’s product-moment correlation coefficient. The difference in the JOA score, neurological recovery rate, post-operative cervical spine function, and pseudotumor size reduction ratio between surgical procedures was analyzed using the Kruskal–Wallis test. Statistical significance was set at P values < .05.
Results
Comparison of Radiographic Features of Patients With NRP and Age- and Sex-Matched Patients in the Control Group.
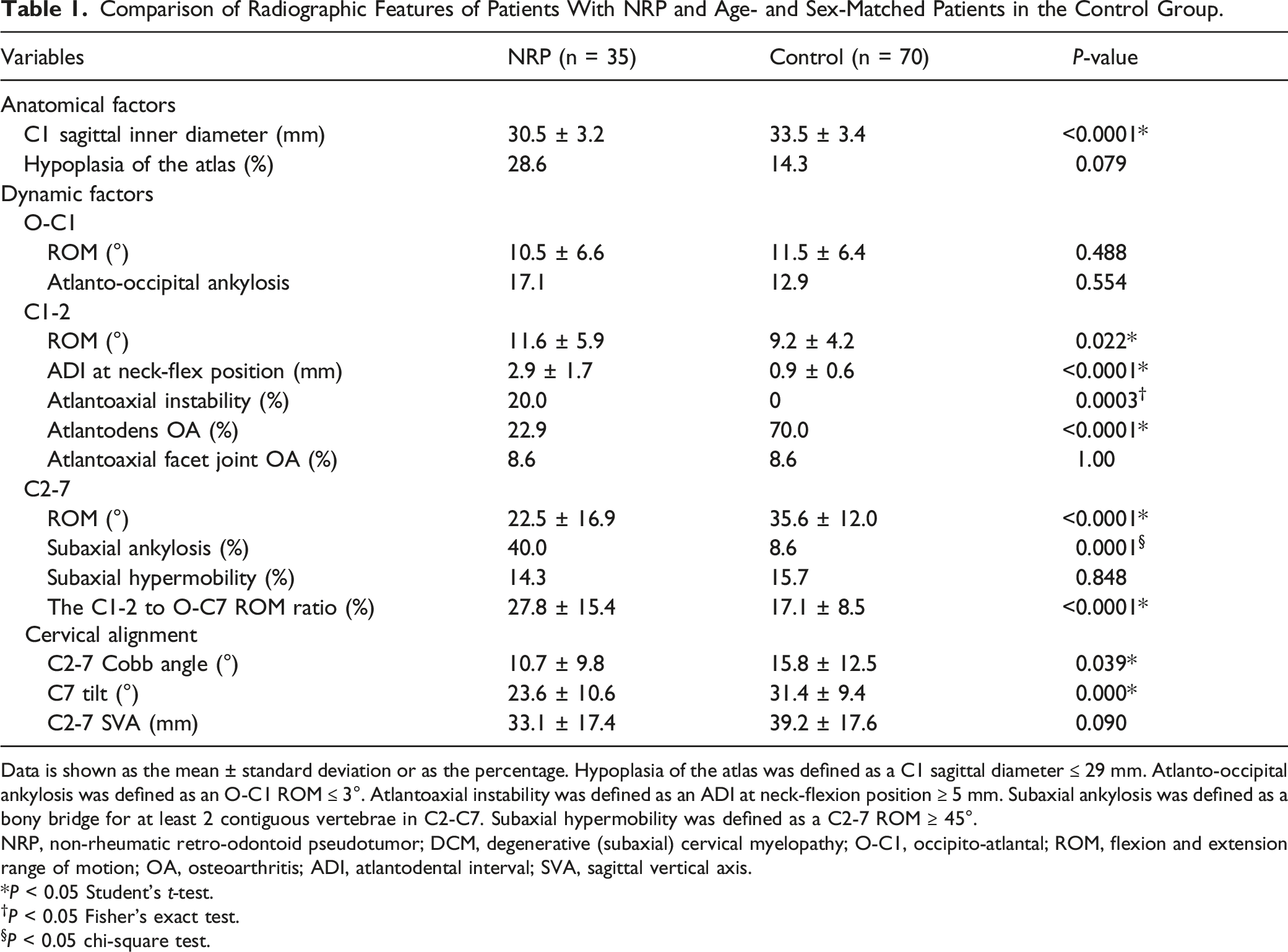
Data is shown as the mean ± standard deviation or as the percentage. Hypoplasia of the atlas was defined as a C1 sagittal diameter ≤ 29 mm. Atlanto-occipital ankylosis was defined as an O-C1 ROM ≤ 3°. Atlantoaxial instability was defined as an ADI at neck-flexion position ≥ 5 mm. Subaxial ankylosis was defined as a bony bridge for at least 2 contiguous vertebrae in C2-C7. Subaxial hypermobility was defined as a C2-7 ROM ≥ 45°.
NRP, non-rheumatic retro-odontoid pseudotumor; DCM, degenerative (subaxial) cervical myelopathy; O-C1, occipito-atlantal; ROM, flexion and extension range of motion; OA, osteoarthritis; ADI, atlantodental interval; SVA, sagittal vertical axis.
P < 0.05 Student’s t-test.
†P < 0.05 Fisher’s exact test.
P < 0.05 chi-square test.
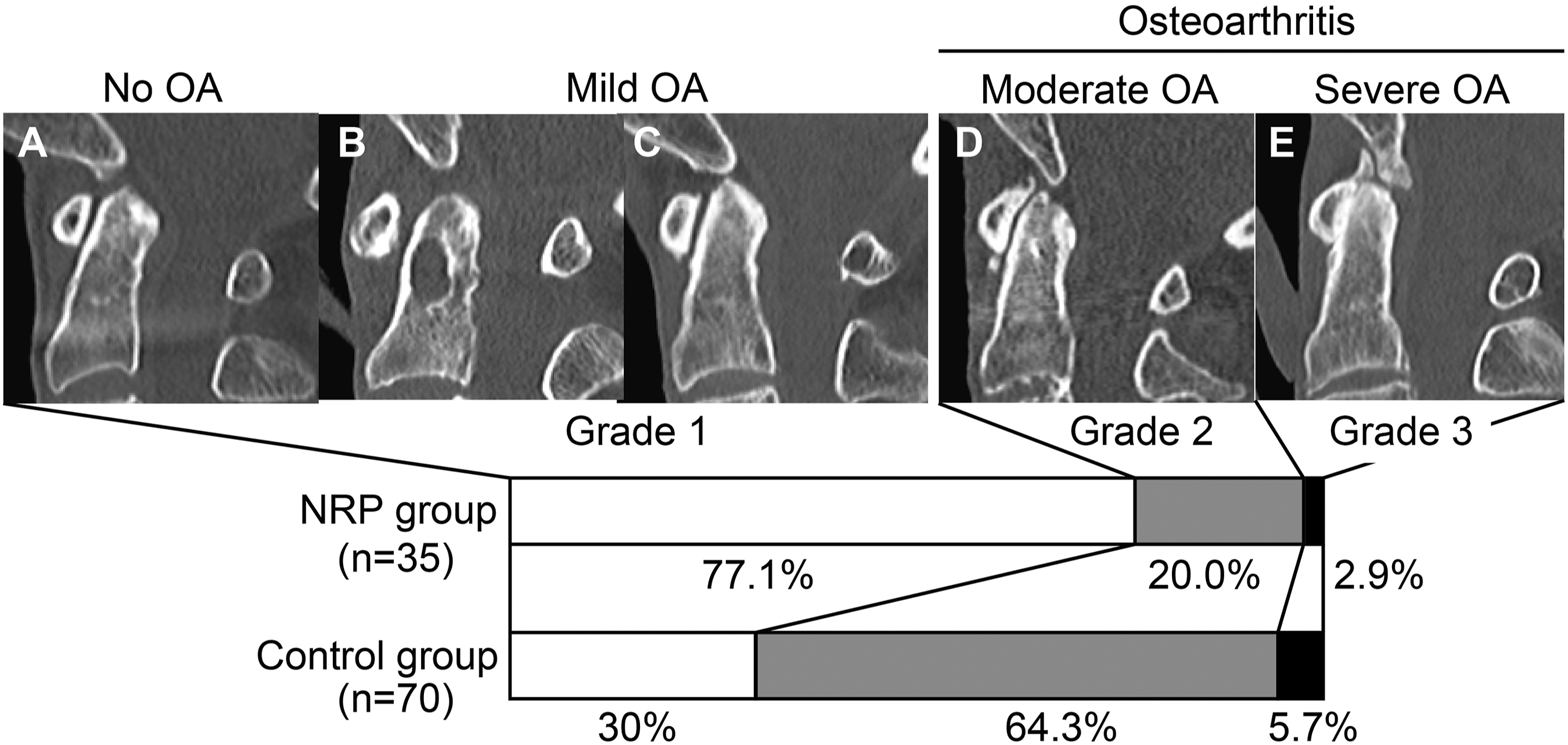
Comparison of ADI degeneration between patients with NRP and age- and sex-matched patients in the control group. Representative sagittal computed tomography reconstruction images of all grades of osteoarthritis of the atlantodense interval. (A) No osteoarthritis (OA), (B) mild without narrowing ADI (frequently observed in the NRP group), (C) mild OA with narrowing ADI, (D) moderate OA, and (E) severe OA. Bar graphs showing the prevalence of each grade in the NRP and control groups, respectively. NRP, non-rheumatic retro-odontoid pseudotumors; ADI, atlantodental interval; OA, osteoarthritis.
Multiple Regression Analysis for Radiographic Factors Associated With the NRP.
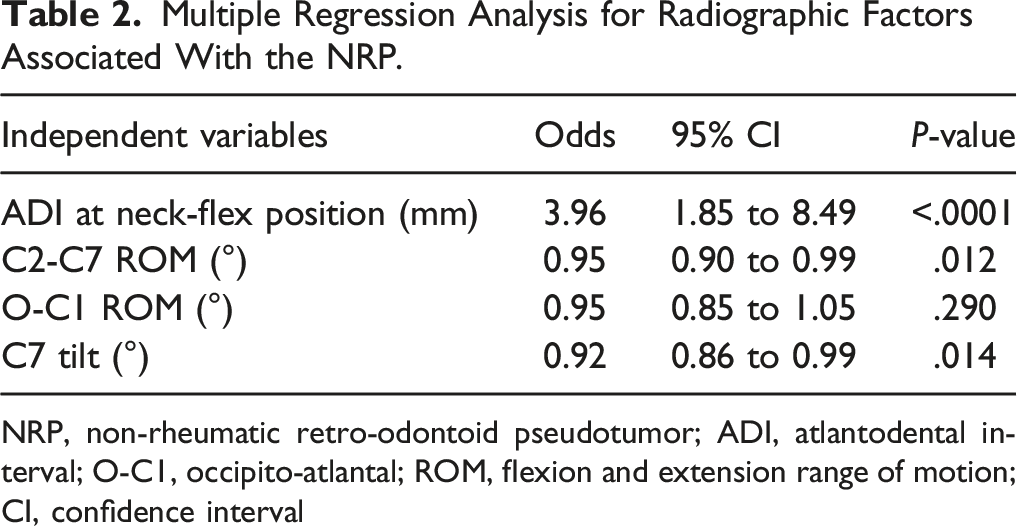
NRP, non-rheumatic retro-odontoid pseudotumor; ADI, atlantodental interval; O-C1, occipito-atlantal; ROM, flexion and extension range of motion; CI, confidence interval
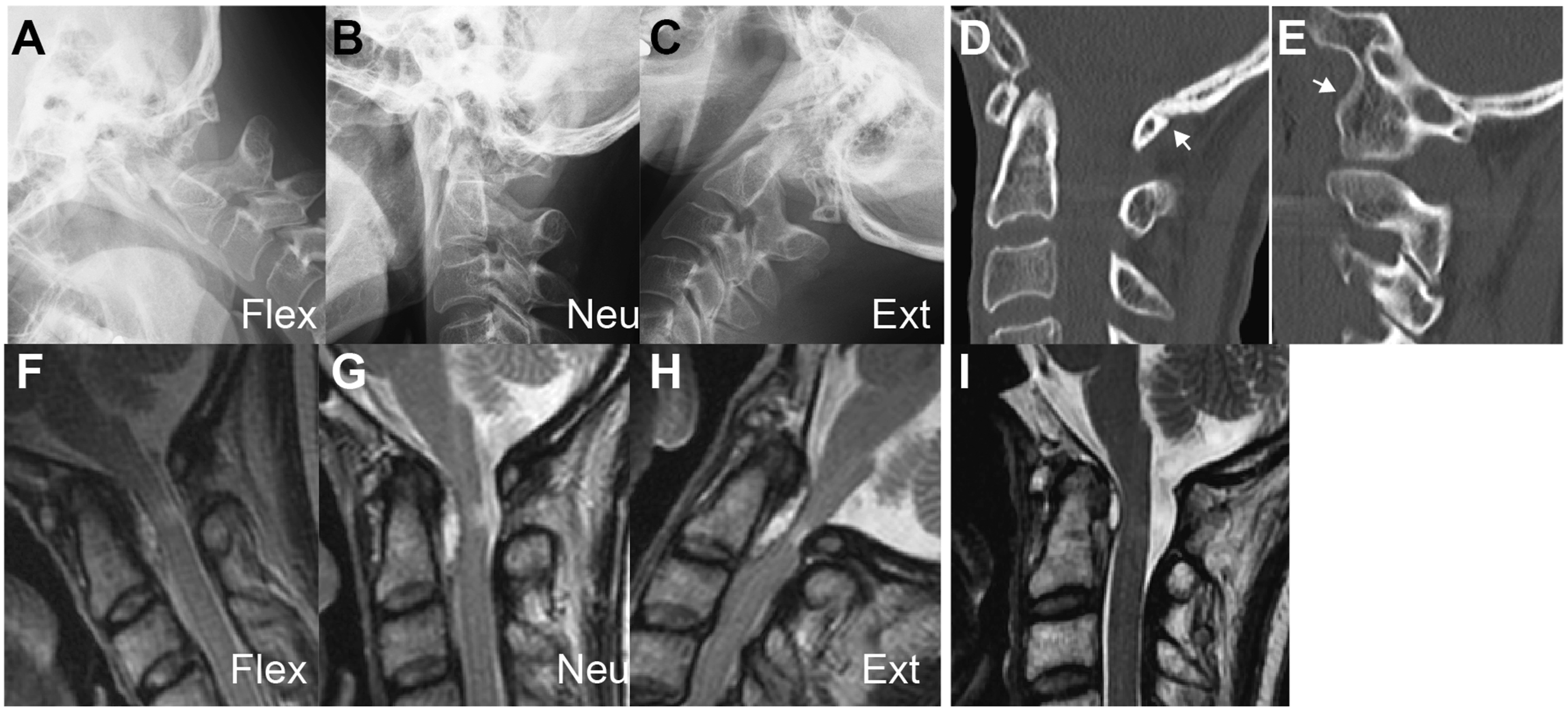
There was a gender difference in the prevalence of some radiographic risk factors (Figure 2). Female patients in the NRP group were likely to have ankylosis in the occipito-atlantal joint with less O-C1 ROM compared to female patients in the control group (Figure 3), whereas this trend was not observed among male patients. Ankylosis in the occipito-atlantal joint included both congenital atlanto-occipital assimilation and osteoarthritic changes of the atlanto-occipital joint. In contrast, male patients in the NRP group had significantly lower C7 tilt than male patients in the control group, but no significant between-group differences were observed among female patients. Comparison of radiographic risk factors for NRP between the NRP and control groups with respect to sex. *P < .05 vs control; **P < .01 vs control. Representative case of a 56-year-old woman with NRP who had atlanto-occipital assimilation as a background pathology. (A-C) Preoperative plain lateral radiograms in flexion, neutral, and extension showing 19° angular motion at the C1-2 segment. Preoperative CT reconstruction images of the midsagittal (D) and parasagittal (E) section showing atlanto-occipital assimilation (white arrows). Preoperative T2-weighted sagittal MRI images in neck flexion (F), neutral (G), and extension (H) showing spinal cord impingement by NRP and C1 lamina in neck extension. Post-operative (I) T2-weighted sagittal MRI image showing spinal cord decompression and reduction of pseudotumor size. NRP, non-rheumatic retro-odontoid pseudotumors; CT, computed tomography; MRI, magnetic resonance imaging.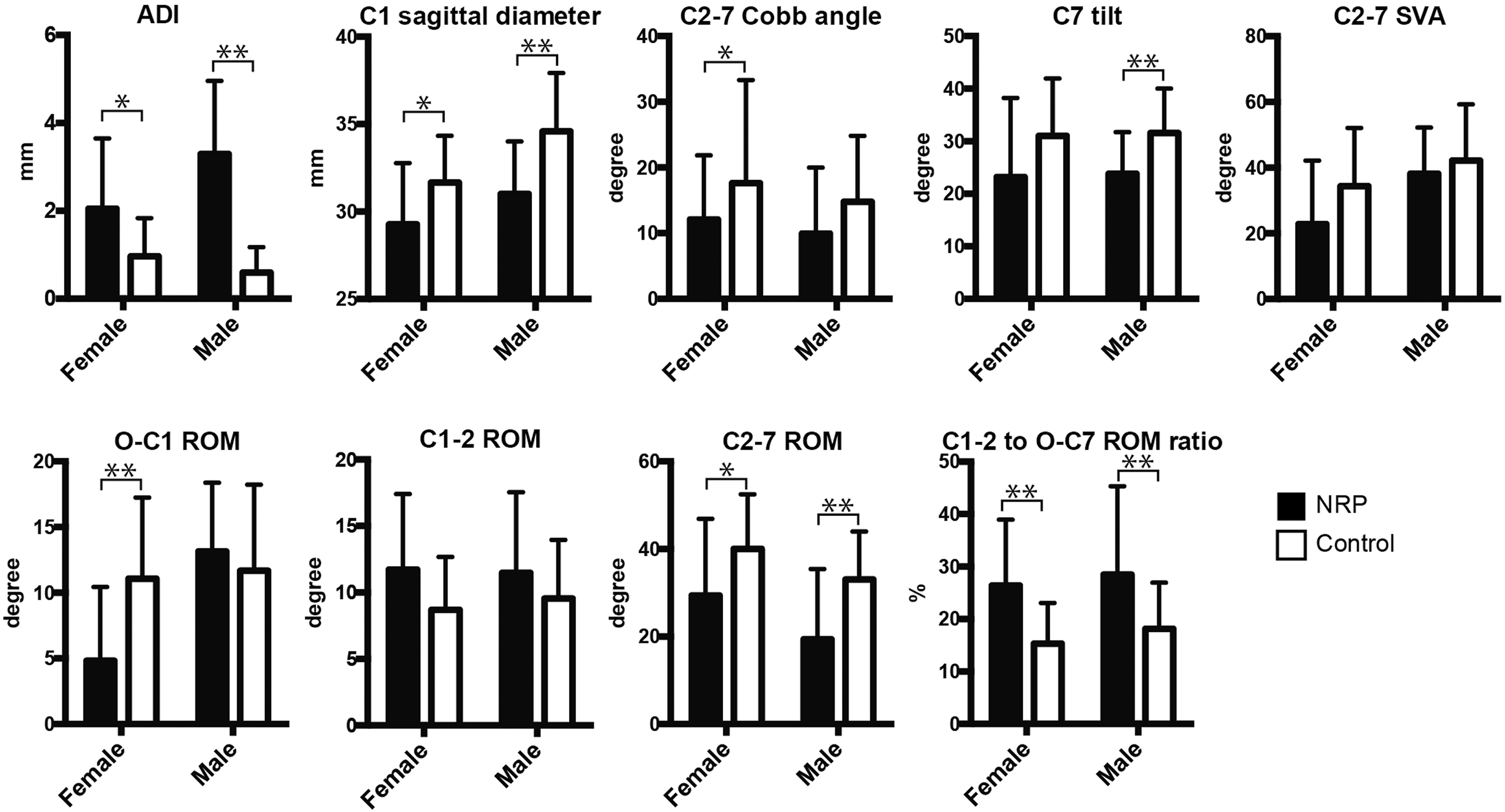
Given that ADI is the most important risk factor for the development of NRP, we investigated the relationship between ADI and other radiographic factors to clarify the factors that influence ADI. Pearson’s correlation analysis showed that C2-7 ROM, C2-7 Cobb angle, and C7 tilt were negatively correlated with ADI (Figure 4). In contrast, O-C1 ROM, C1-2 ROM, and C2-7 SVA showed no significant correlation with ADI. Pseudotumor size was positively correlated with the ADI. Correlation between ADI and other radiographic variables (A-G). Scatter plot showing a negative linear correlation between ADI and C2-7 ROM, C2-7 Cobb angle, and C7 tilt, as well as a positive linear correlation between ADI and pseudotumor size. Solid black circles and black circles indicate NRP cases and controls, respectively. Solid red line indicates the regression line, and the red areas are 95% confidence intervals. NRP, non-rheumatic retro-odontoid pseudotumors; ADI, atlantodental interval; ROM, range of motion.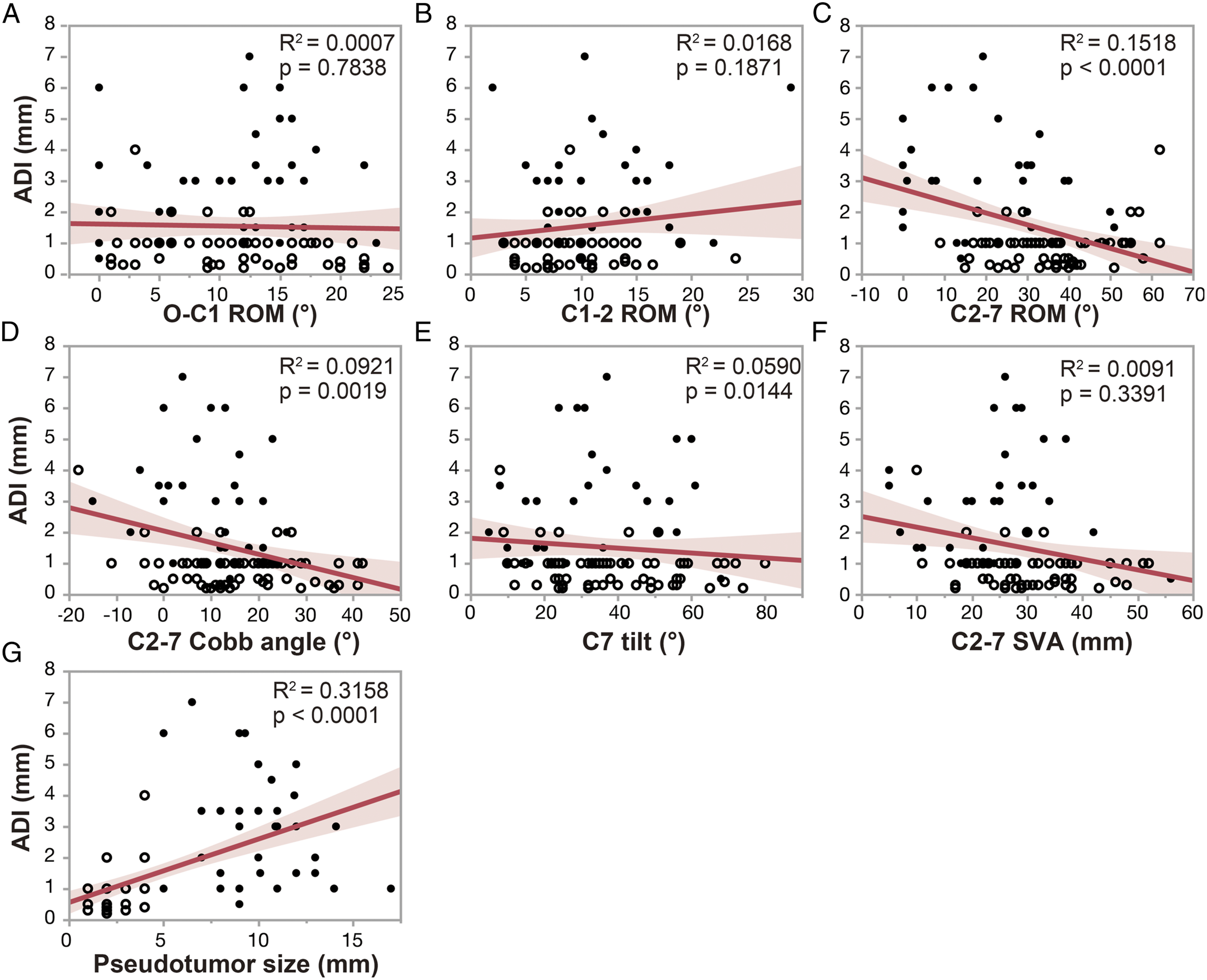
Comparison of Surgical Outcomes in Patients With NRP Receiving C1 Laminectomy With and Without Fusion.
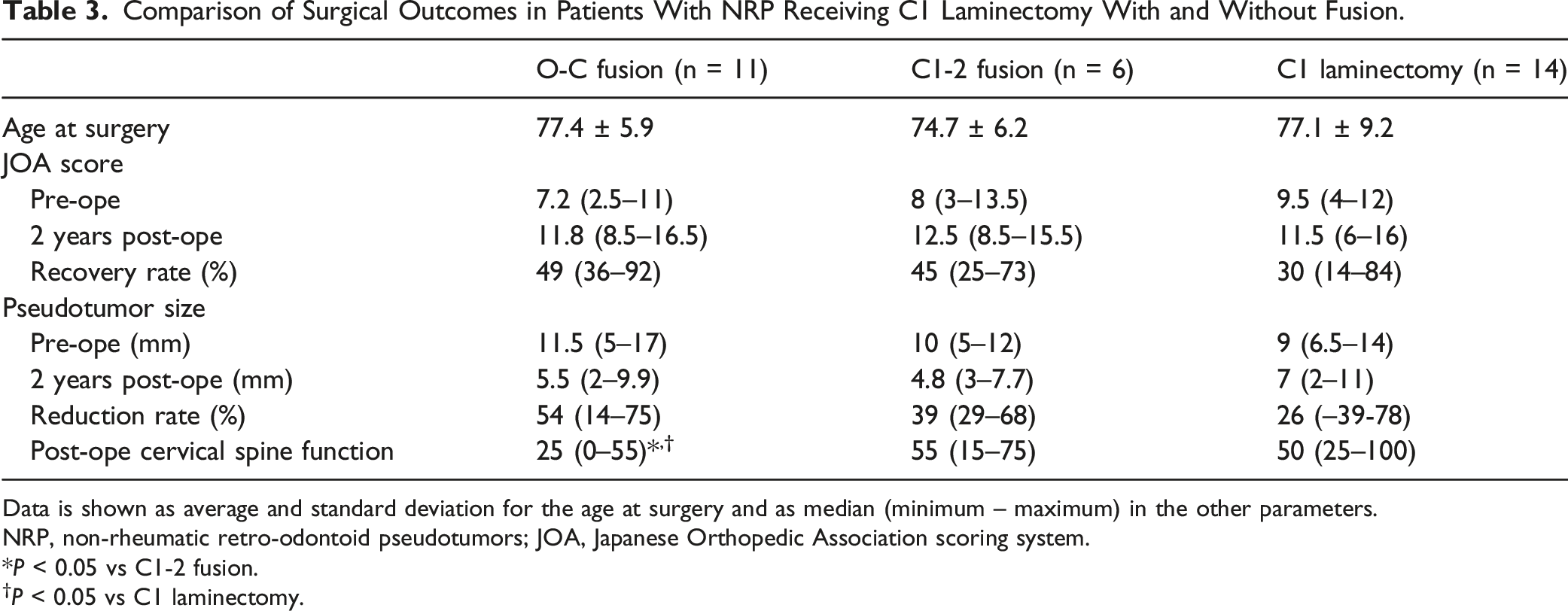
Data is shown as average and standard deviation for the age at surgery and as median (minimum – maximum) in the other parameters.
NRP, non-rheumatic retro-odontoid pseudotumors; JOA, Japanese Orthopedic Association scoring system.
P < 0.05 vs C1-2 fusion.
†P < 0.05 vs C1 laminectomy.
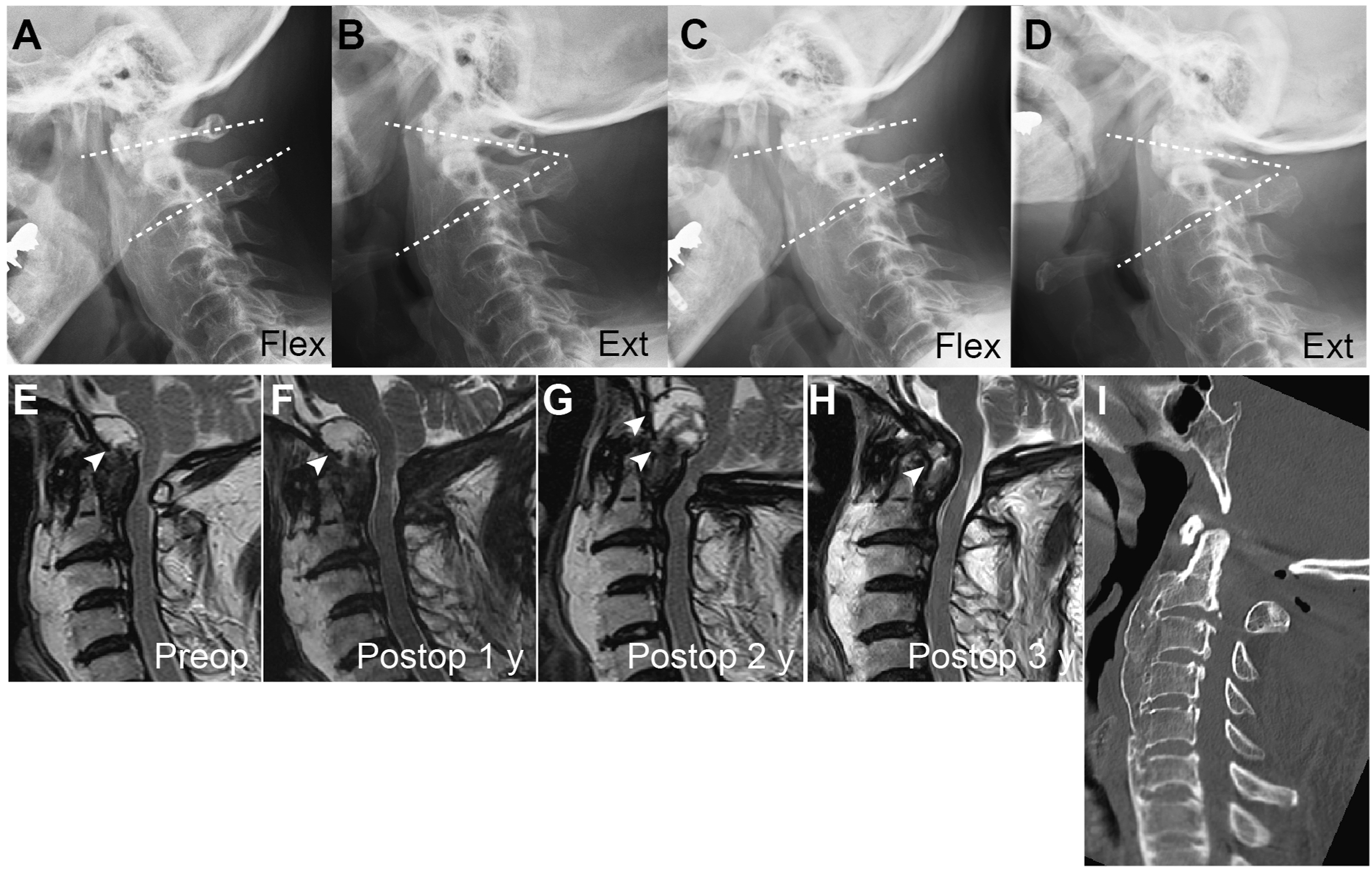
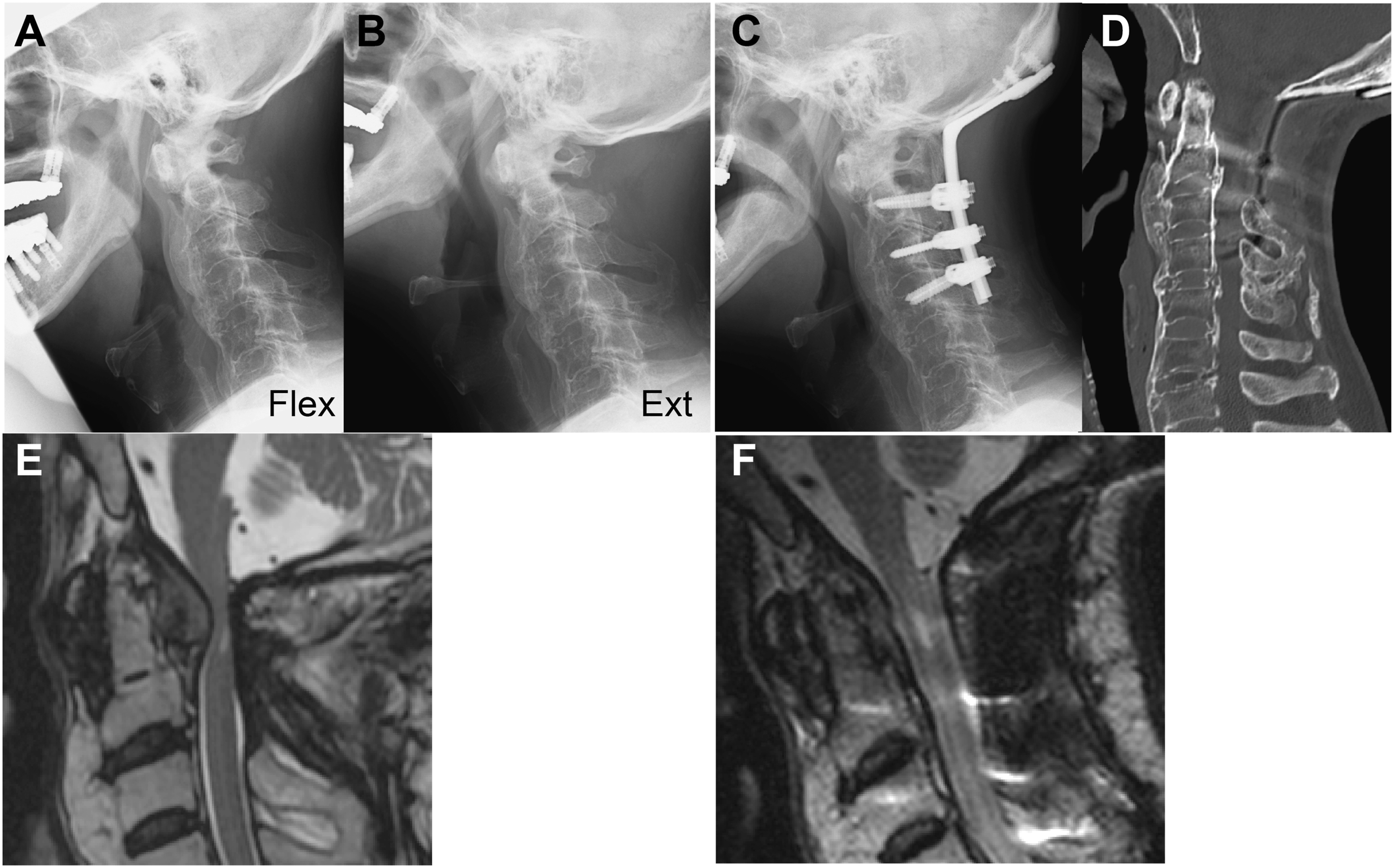
Representative case of a 77-year-old man with NRP that developed most probably from ankylosis of the subaxial cervical spine. (A, B) Preoperative flexion-extension lateral plain radiographs showing that only the O-C1 and C1-2 segments were mobile, but the C2-7 was spontaneously fused. (C, D) Post-operative lateral plain radiograph showing that O-C1 and C1-2 segments were still mobile after C1 laminectomy. T2-weighted sagittal MRI images before operation (E), and 1 year (F), 2 y (G), and 3 y (H) post-operative showing a temporal increase in the pseudotumor size (white arrowheads) during the post-operative course. (I) Sagittal CT reconstruction image showing ossification of the anterior longitudinal ligament at C2-T1 levels. NRP, non-rheumatic retro-odontoid pseudotumors; MR, magnetic resonance.
Representative case of a 72-year-old man with NRP who underwent O-C fusion. (A, B) Preoperative flexion-extension lateral plain radiographs showing that only the O-C1 and C1-2 segments were mobile. (C) Post-operative plain lateral radiograph. (D) Post-operative sagittal CT reconstruction image showing ankylosis of the subaxial cervical spine. (E, F) Preoperative and 1-year post-operative T2-weighted sagittal MRI reconstruction images showing size reduction of NRP and decompression of the spinal cord after the surgery. NRP, non-rheumatic retro-odontoid pseudotumors; MRI, magnetic resonance imaging.
Discussion
This study shows that the expansion of the atlantodens joint is a significant risk factor for NRP, even though the average ADI of NRP patients was 3 mm, which was slightly higher than that of age-sex-matched patients with degenerative cervical myelopathy. Given that the ADI narrows linearly with age and generally becomes 1 mm or less after the age of 70, 23 an ADI of 3 mm is a supraphysiological value considering the age of NRP patients, typically 75 y or older. However, it should be noted that it is unclear whether the expansion of the atlantodens joint is the cause or the result of NRP. A positive correlation between pseudotumor size and ADI indicates that the atlantodens joint is expanded because of the outgrowth of fibrocartilaginous tissue or synovium around the dens. Nevertheless, C1-2 stabilization is considered a reasonable strategy for the treatment of NRP based on its proven effectiveness in reducing pseudotumor size and relieving myelopathy.12,17,21,22,28,29
This study also showed that NRP is associated with a relative increase in the contribution of the C1-2 segment to the total cervical angular mobility resulting from ankylosis of the subaxial cervical spine. Although multiple regression analysis showed that C1-2 ROM was not a significant risk factor for NRP, low C2-7 ROM was identified as an independent risk factor for NRP. The proportion of patients with ankylosis of the subaxial cervical spine was significantly higher in the NRP group than in the control group. These findings have important implications in selecting surgical procedures because O-C arthrodesis surgery could lead to impaired neck mobility, resulting in a significantly negative impact on quality of life, such as impaired swallowing function in elderly patients with ankylosis in the subaxial cervical spine.
Our data also showed a possible association between hypolordosis of the cervical spine and NRP. The C2-7 Cobb angle and C7 tilt were negatively correlated with ADI, and these were significantly lower in the NRP group than in the control group. Miyazaki et al. 30 reported that when the cervical alignment shifted with age from normal to less lordotic, the segmental motion tended to decrease at all levels. The contribution of the upper cervical spine segments to the total angular mobility also increases. Therefore, it is assumed that hypolordosis of the cervical spine increases the risk of NRP by increasing supraphysiological stress to the C1-2 segment.
Our data suggests that patients with NRP without gross atlantoaxial instability can be treated with C1 laminectomy alone. Given that 29% of patients with NRP have C1 hypoplasia, C1 laminectomy is presumed to expand the spinal canal sufficiently to decompress the spinal cord in many patients with NRP. The selection of C1 laminectomy is also justified because the pseudotumor size reduction can be expected following C1 laminectomy, as previously reported.9,11,26 Although the mechanism of pseudotumor size reduction following C1 laminectomy remains unclear, we speculated that the resection of the interspinous muscles and the rectus capitis posterior minor muscles, which arise from the tubercle on the dorsal arch of the atlas, led to a decrease in C1-2 ROM, resulting in the reduction of mechanical stress to the transverse ligament. However, it should be noted that spinal arthrodesis surgery is superior to C1 laminectomy in terms of reducing pseudotumor size. Furthermore, there is a risk of enlarging the pseudotumor after C1 laminectomy. 31 Nevertheless, given that most patients with NRP are elderly patients aged ≥70 y and therefore prefer minimally invasive surgery, C1 laminectomy alone is a recommended treatment for patients without gross atlantoaxial instability.
It may be worth mentioning that C1 hypoplasia might be a risk factor for the development of NRP or at least NRP-induced cervical myelopathy despite the fact that we failed to detect a significant difference in the prevalence of C1 hypoplasia between the NRP and control groups. We defined a C1 sagittal inner diameter ≤29 mm as C1 hypoplasia based on the study by Kelly et al. 19 Considering that Kelly et al. 19 defined a threshold of 29 mm as representing the lowest 2.5% of the general population, the prevalence of 28.6% in patients with NRP is quite high. The most probable reason for why we failed to detect C1 hypoplasia as a risk factor for NRP in this study is that the control group was not from the general population but rather was patients with DCM who are likely to have a developmentally narrow spinal canal; 32 this is a limitation of our study.
Interestingly, congenital assimilation or degenerative ankylosis of the occipito-atlantal joints was observed in 46% of women with NRP. This suggests that NRP could develop because of any factor causing repetitive and excessive stress on the atlantoaxial ligaments. In case of assimilation or ankylosis of the occipito-atlantal joints, O-C2 fusion could be an appropriate treatment option; however, 2 of 6 patients with O-C1 ankylosis in this case series underwent C1 laminectomy and successfully recovered.
This study had several limitations. First, the number of patients in this study was small because of the rarity of NRP. Second, this study was a retrospective analysis of existing data from various hospitals, and the treatment strategy was not controlled. The operating surgeons selected the surgical procedure according to their experience and the patient’s condition. Third, we proposed a surgical strategy based on the underlying pathology of NRP; however, this surgical strategy should be validated in a future prospective clinical study to reach a consensus. Fourth, we compared post-operative cervical spine function between surgical procedures, but could not evaluate preoperative function due to the lack of data. Therefore, we could not determine how different surgical procedures affect cervical spine function based on the results of this study alone. Fifth, a 2-year follow-up was not long enough to judge whether the recurrence rate was comparable among surgical procedures. However, it should be noted that many elderly patients, especially those who could not visit the hospital by themselves, did not prefer regular visits to the hospital after 2 y post-operatively.
In conclusion, our data suggests that NRP can be induced by supraphysiological stress on the atlantodens joint resulting from ankylosis and hypolordosis of the subaxial cervical spine. Therefore, arthrodesis surgery is an effective surgical strategy for myelopathy caused by NRP; however, the indication of O-C fusion should be carefully determined for patients with ankylosis of the subaxial cervical spine because it results in a remarkable loss of cervical motion function. The development of myelopathy is attributable to C1 hypoplasia in 31% of our cases, indicating that such patients could be treated by posterior decompression alone. Thus, our study suggests that C1-2 arthrodesis surgery or C1 laminectomy alone would be a reasonable surgical strategy to treat myelopathy caused by NRP in the elderly.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.