
Abstract
Study Design:
Retrospective matched-pair analysis.
Objectives:
Lumbosacral transitional vertebrae (LSTV) have a reported prevalence of 4-36% in the population. The safe zones for screw placement for spinopelvic fusion in adult spinal deformity surgery for patients with LSTV have not been described in the literature. Our study aimed to assess the safety of S1-pedicle screw (S1PS), S2-alar screw (S2AS), S2-alar-iliac screw (S2AIS), and iliac screw (IS) placement in patients with LSTV.
Methods:
Out of the 819 examined patients, 49 patients with LSTV were included in our retrospective analysis with a matched pair control group. We used the 3-dimensional planning tool mediCAD for screw placement of S1PS, S2AS, S2AIS, IS with different angles, length and diameters.
Results:
We evaluated a total of 10 192 screw trajectories. No serious complications occurred due to the trajectories used for S1PS. LSTV increased the risk of vessel injury for S2AS trajectories (P = .001) but not for S2AIS (P = .526). Besides the presence of an LSTV, the screw trajectory had a major influence on the frequency of serious complications.
Conclusions:
Sacral anchoring of long spinal constructions using S1PS, S2AS, S2AIS and IS is also possible in the presence of LSTV. For S2AS the trajectory with 30° lateral and caudal angulation of 10° showed the least vascular injuries and the least sacro-iliac-joint violations in patients with LSTV. S2AIS trajectories with 40° lateral and 0° sagittal angulation reduced the risk of serious complications in our patients collective with LSTV.
Keywords
Introduction
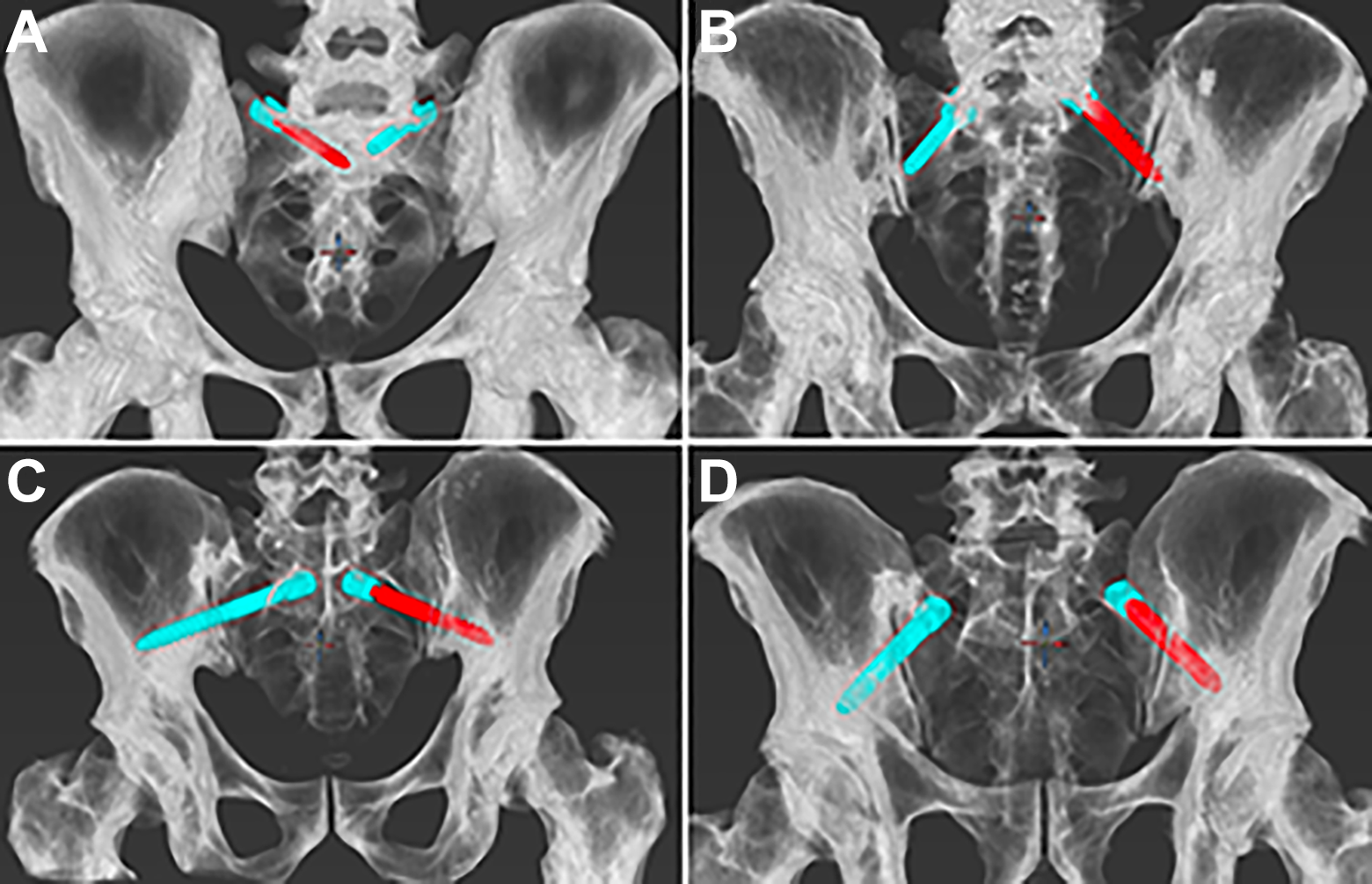
With a reported prevalence of 4-36% in the general population, lumbosacral transitional vertebrae (LSTV) are one of the most common congenital anomalies of the spine. LSTV is defined as either a sacralization of the lowest lumbar segment or a lumbarization of the superior sacral segment.1,2 In 1984, a radiographic classification system was introduced by Castellvi et al, defining 4 different types of LSTVs as shown in Figure 1. 3
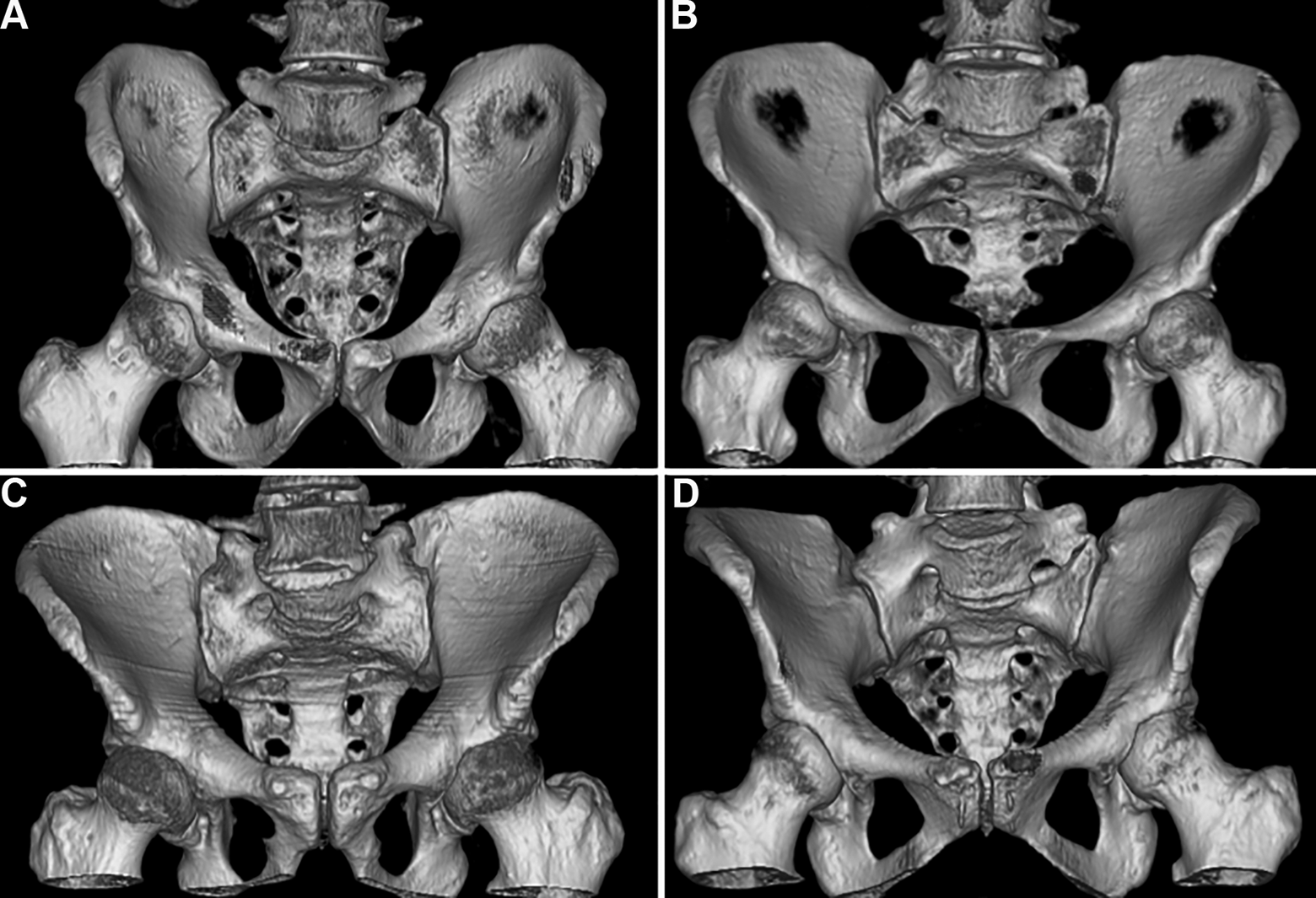
The Castelllvi classification allows the grouping in transitional vertebrae. Transitional vertebrae with an enlargement of the transverse process to at least 19.0 mm are classified as unilateral (Ia) or bilateral (Ib) (A). Pseudarticulation of the transversal process with the sacral bone is classified as IIa in unilateral occurrence and IIb (B) in bilateral occurrence. The fusion of the transversal process with the sacral bone is classified as IIIa in the case of unilateral occurrence and as IIIb (C) in the case of bilateral occurrence. Unilateral fusion and contralateral pseudarticulation of the transversal process with the sacral bone are classified as Castellvi IV (D). 3
Long spinal fusions are an increasingly common procedure in the surgical correction of adult spine deformity. 4 However, due to a high degree of mobility of the lumbosacral unit and intense stress on the sacrum, lumbosacral fusions show a high rate of pseudarthrosis and revision is indicated in about 25% of patients. 5 In order to prevent implant failure of fusions ending at S1, extension of the instrumentation to the pelvis has become increasingly common. However, spinopelvic fixation remains surgically challenging. Even though iliac screws provide biomechanically strong constructs, they may lead to wound dehiscence over screw heads or postoperative pain due to screw prominence, which is why S2-alar (S2AS) and S2-alar-iliac screws (S2AIS) were introduced.6,7 In contrast to iliac screws (IS), S2AIS require a deeper insertion point which is in line with that of S1-pedicle screws (S1PS) and thus offset use is not required. 8 A recent meta-analysis of 11 studies showed that S2AIS fixation has an improved fusion rate as well as fewer postoperative complications and reoperation rate compared with IS fixation. 9
Placement of S2AS, S2AIS or IS remain potentially problematic with complications ranging from decreased fixation strength to injury of major vessels which is why safe insertion of these screws is crucial. However, to our knowledge, a larger analysis of safe spinopelvic screw insertion in patients with LSTVs has not been investigated yet. Our study’s aim therefore was to assess the feasibility and safety regarding screw length, diameter and angles as well as complications of S1PS, S2AS, S2AIS and IS insertion in patients with LSTV compared to a matched control group.
Material and Methods
Patients
The study protocol was approved by the local institutional ethics board (ethics proposal number EA1/300/19). We retrospectively included patients in which abdominal-pelvic computed tomographies (CTs) from at least level L1 to the greater trochanter of the femur had been performed in our department of radiology from 2016 to 2019 due to tumor staging or exclusion of visceral bleeding. Exclusion criteria were metastatic and primary malignancy of the musculoskeletal system and previous spinal or pelvic fusion surgery. A total of 819 patients were identified, of which 52 showed anatomical changes in the lumbosacral transition. Three were excluded because of inadequate image quality for software evaluation. The remaining 49 patients were matched with control patients from the cohort described above, using propensity score matching with a tolerance of 0.01, matching for age and gender. The data was collected and analyzed completely anonymized, patients informed consent was not required by the local ethics committee.
Radiographic Measurements
CT images were reconstructed with the Food and Drug Administration certified hybrid planning spine 3D reconstruction software (mediCAD Hectec GmbH, Germany). The screw trajectories were placed by one of the authors (B.L.), a spinal surgeon trained by a spinal attending surgeon (author; M.P.). Screw malplacement was assessed in a consensus reading approach in order to minimize the risk of systematic bias.
LSTVs were detected by 2 independent experienced radiologists. The vertebral body S1 was defined as the first vertebral body below an at least rudimentary vertebral disc. To normalize the screw trajectory angles and reduce bias opportunities, the oblique lying position of the patients on CT table was evaluated and reflected in the placement of the screw trajectories. For this purpose, a line tangentially intersecting both spinae iliacae posteriores superiores was defined in the axial plane. An orthogonal line to this line was defined as 0° axial angulation. The sagittal screw angulation was determined in the sagittal plane. The line that was perpendicular to the displayed CT table in the sagittal plane was defined as 0° sagittal angulation as shown in Figure 2.
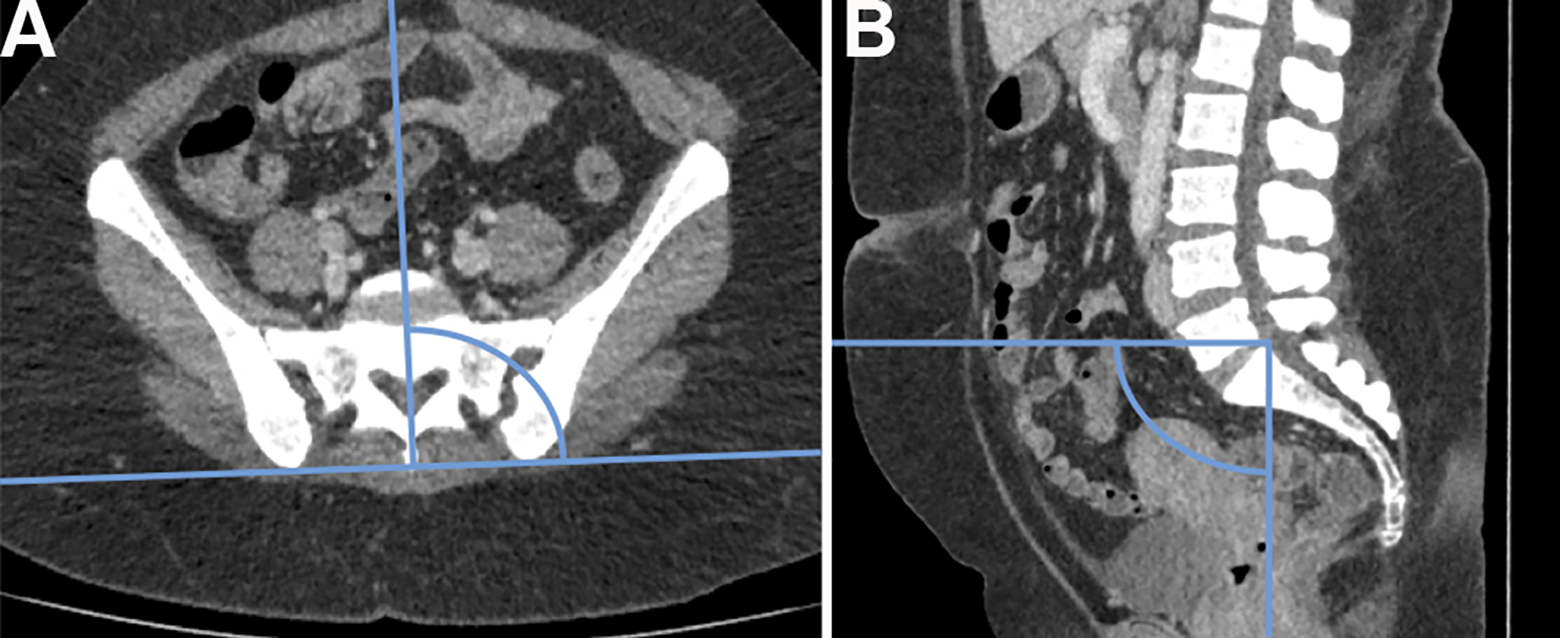
In (A) an axial CT image is shown, in which the line connecting the 2 spinae iliacae posteriores superiores and the orthogonal line defining 0° axial angulation are highlighted. In (B) a sagittal CT image is shown. A line parallel to the CT table and a line orthogonal to it defining 0° sagittal angulation are depicted. The intersection of the 2 lines was placed on each predefined screw entry point for screw placement.
All screw trajectories were examined for penetrating the cortical bone apart from the entry point, which was classified as a cortical breach. Entry points were defined as mentioned in Figure 3.
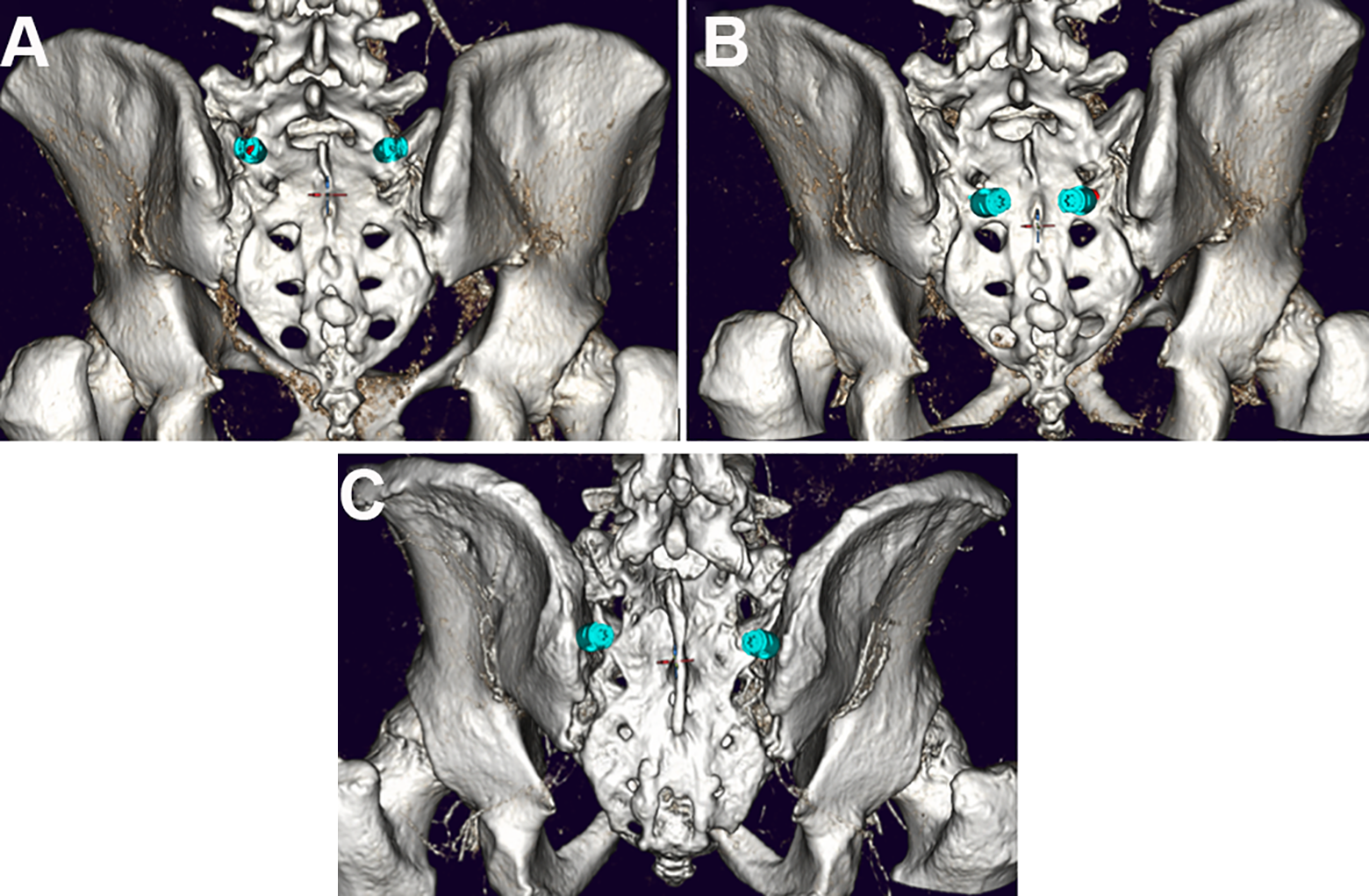
For the S1PS trajectory (A) the intersection between a transverse line at the level of the inferior tip of the inferior articular process of L5 and a longitudinal line along the ridge of the superior articular process of S1 was selected as the screw entry point.5,10 For S2AS and S2AIS trajectories (B) the intersection between a vertical line through the S1 and S2 dorsal foramina and midway between these dorsal foraminae was selected as the screw entry point.5,10 For the IS (C) trajectory the entry point was selected 1 cm medial to the iliac crest and inferior to the spina iliaca posterior superior. 11
For all screw trajectories the interference of the screw trajectory with iliac or gluteal vessels was assessed as presented in Figure 4. In case of even partial interference, this was evaluated as vascular injury.
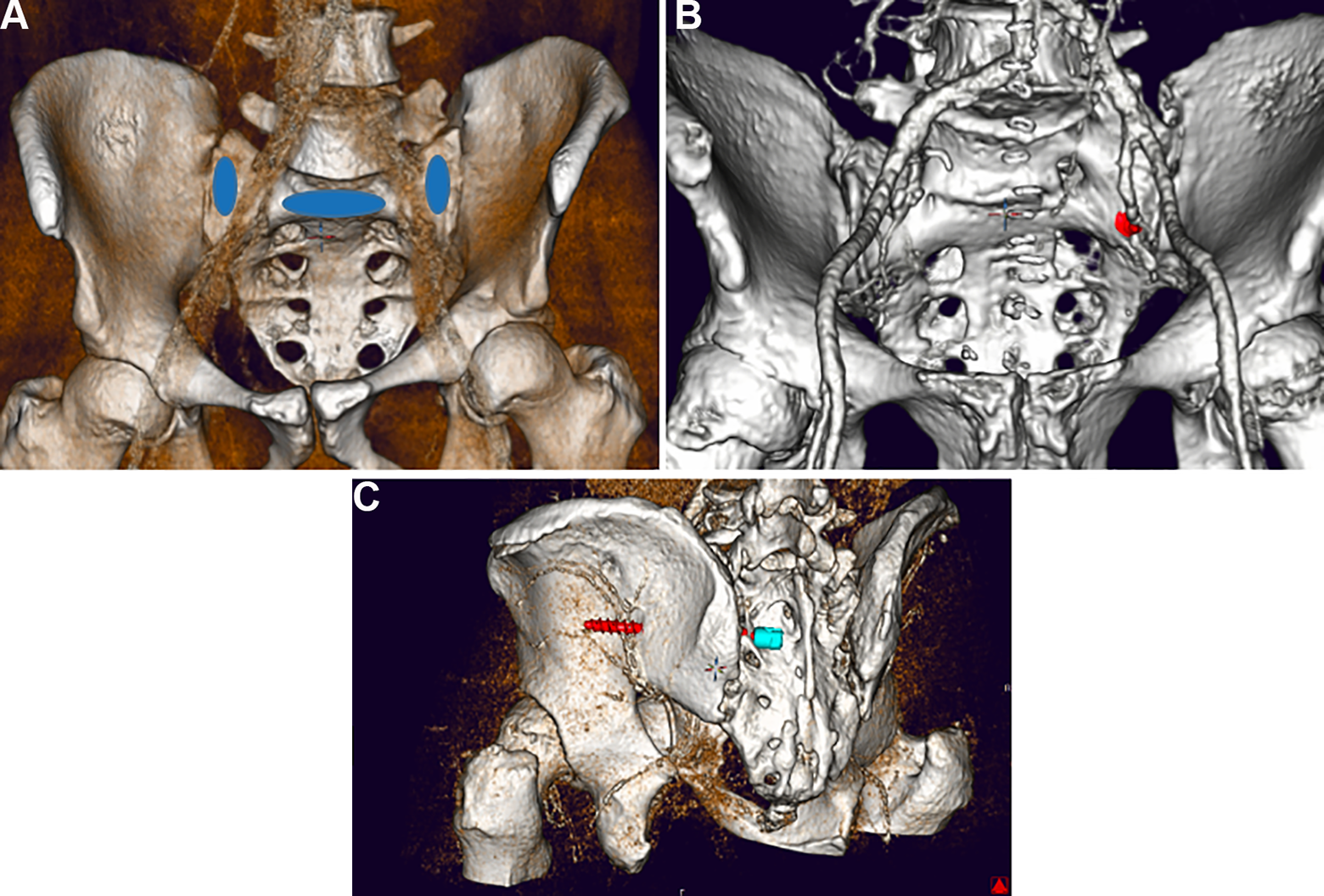
A, Anterior vessel interference in a patient with LSTV due to an S2AS with 30° lateral and 25° sagittal angulation, 8.5 mm diameter and 50 mm length. B, Posterior vessel injury due to an S2AIS with 60° lateral and 10° sagittal angulation, 9.5 mm diameter and 95 mm length.
We subgrouped each patient side according to the extent of the transition to 1 of the 4 groups: No transition, enlarged transverse processes, pseudarthrosis, osseous fusion. For S1PS trajectories accuracy of the pedicle screw position regarding the medial pedicle breach was evaluated using the Rampersaud classification. 12 For S2AS trajectories position in relation to the sacroiliac joint (SIJ) was additionally classified (0 = no SIJ infiltration, 1 = infiltration of the os sacrum cortex (belonging to the SIJ), 2 = in the SIJ gap, 3 = infiltration os ilium). In all patients, all the screw trajectories options listed in Table 1 were placed on both sides of the os sacrum/ilium. Examples of screw trajectories are presented in Figure 5.

Abbreviation: Ang., angulation.
Examples of screw positioning of S1PS (A) with 30° medial and 25° sagittal angulation on the right sacral side and 20° medial and 10° sagittal angulation on the left sacral side, each 6.5 mm in diameter and 45 mm length. S2AS (B) right with 30° lateral and 10° sagittal angulation, left with SIJ violation with 45° lateral and 25° caudal angulation each with a screw diameter of 8.5 mm and a screw length of 50 mm. S2AIS (C) right with 40° lateral and 0° caudal angulation, left with dorsal screw breach at 60° lateral and 10° caudal angulation with a screw diameter of 9.5 mm and a screw length of 95 mm. IS (D) right with 20° lateral and 30° caudal angulation and left with 35° lateral and 45° caudal angulation.
Statistical Analysis
All statistical analyzes were performed using IBM SPSS Statistics 27 software (IBM, Armonk, USA). The chi-square test was used for nominal scaled variables and for metrical data Wilcoxon signed-rank test. The association between the degree of fusion (none, enlarged transverse process, pseudoarticulation, fusion) and breach frequencies was investigated using Spearman’s correlation coefficients. We tested the data for statistically significant frequency distributions of screw breaches, vascular injuries and SIJ violations depending on the screw trajectory of the defined groups against each other. A P-value < .05 was considered statistically significant.
Results
Patients
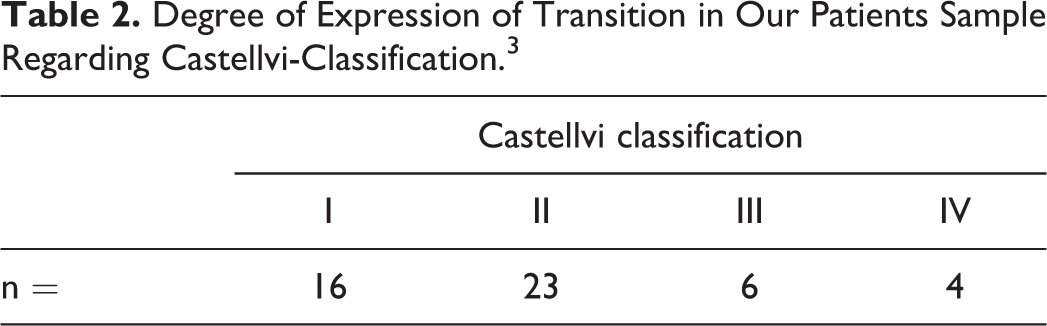
Based on the study design there were no significant differences in age (mean 52.0 years, range 16-81/19-86 years (LSTV/control) P = .893) and gender (24/49 female and 25/49 male in LSTV and control group). Transitional vertebrae had a prevalence of 6.3% in our patient’s population. Castellvi types in our population are given in Table 2.
Degree of Expression of Transition in Our Patients Sample Regarding Castellvi-Classification. 3
S1-Pedicle Screw
None of the 784 S1PS trajectories showed neither a violation of the spinal canal nor vascular injury. Patients with LSTV were significantly more likely to have a ventral screw breach with selected screw trajectories (P < .001; LSTV 98/392, control 43/392). Castellvi type of LSTV significantly correlated with the frequency of a ventral breach of the screw tip (P = .009, r = 0.132).
Upper end plate infiltration did not differ significantly between the control group and LSTV (P = .720) nor was it influenced by the Castellvi type (P = .484). Screw trajectories with 20° medial angulation instead of 30° resulted in significantly more ventral breaches in both the control group (P < .001; 20° 27/196, 30° 16/196) and patients with LSTV (P < .001, 20° 62/196, 30° 36/196). Sagittal angulation had a significant effect on the overall frequency of a breach in both the control group (P < .028; 10° 82/196, 25° 41/196) and patients with LSTV (P < .001; 10° 101/196, 25° 73/196). Screw trajectories with 10° sagittal angulation perforated the endplate by 38.27% whereas trajectories with 25° sagittal angulation infiltrated the endplate only by 1.53% (P = .149; 10° sagittal angulation 150/392, 25° 6/392).
S2-Alar Screw
1252 of the 3136 tested S2AS trajectories caused a breach. The frequency of ventral screw breaches of the trajectories did not differ significantly between the control group and patients with LSTV (P = .141; LSTV: 40/1586, control: 28/1586). However, patients with LSTV were significantly more likely to have a violation of the SIJ by S2AS trajectories tested (P < .001; LSTV 784/1586, control 400/1586). The frequency of SIJ injury by S2AS trajectories showed a significant but weak correlation with the degree of expression of a transitional vertebra (P < .001, r = 0.109).
In the group with LSTV, the reported S2AS trajectories led to significantly more vessel injuries (P = .001; LSTV 11/1568 vessel injuries, control 0/1568). The frequency of vascular injuries caused by S2AS trajectories showed no connection with the Castellvi type of LSTV (P = .465). Vascular injuries in patients with LSTV resulted only from screw trajectories with a lateral angulation of 30° and sagittal angulation of 25° (11/392) while none of the other screw trajectories led to vessel injury (0/1176). The use of screw trajectories with a length of 50 mm resulted in significantly more vascular injuries compared to 45 mm screws in the LSTV group (P = .034; 50 mm 9/784, 45 mm 2/784).
S2-Alar-Iliac Screw
Patients with LSTV showed significant more screw breaches than the control group caused by tested S2AIS trajectories (P < .001; LSTV 625/1568 screw breaches, control 590/1568). Ventral breaches of the screw trajectory were significantly more frequent in the control group (P < .001; LSTV 103/1568, control 278/1568), while dorsal exits were significantly more frequent in the group of LSTV patients (P < .001; LSTV 522/1568, control 312/1568).
The frequency of vascular injuries caused by S2AIS trajectories did not differ significantly between LSTV patients and the control group (P = .526; LSTV 6/1568, control 4/1568). However, degree of expression of LSTV correlated significant but poor with vascular injuries (P < .001, r = 0.101). Vessel injuries with the S2AIS trajectories occurred only with a lateral angulation of 60° and sagittal angulation of 10°. Screw trajectories with a length of 65 mm led to a significant reduction in vascular injuries compared with 95 mm screws (P < .001; 65 mm length 2/1568, 95 mm 8/1568). Whereas the screw trajectories diameter (P = 1.00) had no significant influence on the frequency of vascular injuries.
Iliac Screw
234 of the 3136 IS trajectories showed a breach. The anterior (P = .502) and posterior breach frequency (P = .066) did not differ significantly between the control group and patients with LSTV as presented in Table 3.
Overview of the Frequency of Anterior and Posterior Breaches of the Iliac Screws Depending on the Castellvi Classification.

The screw trajectory with a lateral angulation of 20° did not differ significantly in the frequency of breaches compared to the 35° insertion (P = .095; 20° lateral angulation 77/1568, 35° 157/1568). Whereas trajectories with a sagittal angulation of 30° resulted in a significantly higher frequency of overall breaches compared to 45° downward angulation (P < .001; 30° downward angulation 149/1568, 45° 85/1568). A longer trajectory resulted in significantly more frequent breaches (P < .001; 65 mm screw length 25/1569, 95 mm 209/1568). Two screw misalignments occurred into the sciatic notch with a screw trajectory with a lateral angulation of 20° and a sagittal angulation of 45° downward for patients with LSTV. The frequency of vascular lesions for the trajectories of IS of LSTV patients and the control group did not differ significantly (P = .057; LSTV 8/1568, control group 2/1568). Vascular injuries with the IS trajectories occurred only with a lateral angulation of 35° (35° axial angulation 10/1568, 20° axial angulation 0/1568). Sagittal angulation of screw trajectories of 45° compared to 30° significantly increased the risk of vascular injury (P < .001; 30° 4/1568, 45° 6/1568) as well as the use of longer screws trajectories (P < .001; 65 mm 4/1568, 95 mm 6/1568). The screw diameter (P = 1.00) had no significant influence on the frequency of vascular injuries.
Discussion
As a clinical impact this study shows, that sacral anchoring of long spinal constructions using S1PS, S2AS and S2AIS is also possible and a safe option in the presence of LSTV.
S1-Pedicle Screw
S1PS with a bicortical anchorage have a lower risk of loosening.5,13 Especially the anchorage by the S1 cover plate further increases the pull-out strength.13,14 Considering these results, an S1PS with 10° sagittal angulation may lead to biomechanically superior fixation. While no spinal canal injury was detected independently of medial angulation. Convergence of the screws at 20° is recommended due to more frequent bicortical fixation. Consistent with the results in the literature, which report very low rates of vascular damage, no vascular injury was found regardless of the screw trajectory for control group and LSTV patients. 15
S2-Alar Screw
Bicortical anchoring of S2AS leads to a lower risk of loosening5,16 but increases the risk of injury to presacral neurovascular structures. 17 LSTV have a significant influence on the morphology of the os sacrum and the pelvis. 18 Our results confirm a higher risk of vascular injuries for patients with LSTV (P = .001), especially for longer screws (P = .034) and a trajectory with a steeper caudal angulation of 25° (P = .001). Accordingly, insertion with 10° angulation and utilization of shorter screws could reduce the risk of vascular injury for patients with LSTV. Maximum tested lateral angulation angle for S2AS lead to an increased rate of SIJ injuries in patients with LSTV (P < .001), so a lateral angulation of 30° and 10° caudal angulation should be considered for placement.
S2-Alar-Iliac Screw
S2-alar-iliac screws seems to have clinically lower complication rates compared to iliac screws.9,19,20 According to the findings of Yamada et al, that a low-riding L5 vertebra is supposed to reduce the safety margin for the implantation of a S2-alar-iliac screw 11 we saw a significant (P < .001) accumulation of dorsal breaches in LSTV. The bicortical anchorage in the os ilium does not lead to biomechanical superiority of the screws. 21 A screw trajectory of 40° lateral angulation significantly reduced the breach frequency and lowered the risk for serious complications with injury to the superior gluteal artery (P = .014).
For the treatment of transitional vertebrae, the need for a higher cranial entry point was reported. 22 Screw trajectories with a sagittal angulation of 0° showed no vascular injury, whereas trajectories with a 10° sagittal angulation showed 0.8% vascular injury (P = .014). According to these results, it should be considered to choose the trajectory of S2AIS angulated 40° laterally and 0°.
Longer trajectories had a significantly higher frequency of breaches (P < .001). O’Brien et al showed that S2AIS with a length of 65 mm could be biomechanically equivalent to screws with a length of 80 mm. 21 Recognizing this fact, the need for a longer S2AIS for each specific fusion should be evaluated.
S2AIS, in contrast to the S2AS, did not affect the presacral vessels but, with the trajectories selected, mainly posed a risk of injury to the superior gluteal artery. LSTV did not lead to an increased risk of vascular injury in S2AIS. Therefore S2AIS can be considered as an safe alternative for spinopelvic anchoring in patients with LSTV.
Iliac Screw
The complications of IS did not differ significantly between the control group and patients with LSTV (P = .057). In screw trajectories with 20° lateral angulation, no vascular injury occurred. Sagittal angulation of 45° significantly reduced the breach frequency and therefore should be preferred compared to 30° but did not affect the frequency of vascular lesions.
Limitations
Despite the significant and clinically relevant findings of our study, there are remaining limitations and the results have to be interpreted accordingly. Since each parameter of the screw geometry and angulation has a 3-dimensional influence on possible complications. The clinical implication of this manuscript should not be the ideal screw position, rather illustrate common complications. We evaluated 49 patients with LSTV this might compromise the generalization of the results. Not all of the Castellvi subgroups included the same number of patients, this introduces a bias opportunity. We examined a patient population that did not receive the imaging due to back pain and therefore might differ in the degree of degeneration from a typical patient population for spine surgery. The investigator could see the vessels during screw placement, but the angles for the screw trajectories were applied as described in the methods and the screw trajectories were placed based on this and the defined entry point so that a bias opportunity was reduced as much as possible.
Conclusion
This is, to the knowledge of the authors, the first clinical study to evaluate the safe zones for spinopelvic anchoring of screws in patients with LSTV compared to a matched control group. Due to more frequent screw misalignments in patients with LSTV, sectional imaging may need to be performed more frequently and detailed screw placement planning should be performed. The studied screw trajectories provided a safe insertion of S1PS in LSTV regarding vascular and spinal canal injury. LSTV increased the risk of vessel injury by using S2AS. The S2AS with 30° angulation laterally and a caudal angulation of 10° showed the least vascular injuries and the least SIJ violations in patients with LSTV. No increased risk of vascular injury was found for the S2AIS in patients with LSTV in our patients collective with LSTV. No increased risk of vascular or nerve injury was observed for IS in our patient population with LSTV. Based on our results, in patients with LSTV requiring augmentation of the spino-sacral fixation, the use of S2AIS as well as IS should be considered due to the lower risk of vascular injury evaluated in our collective when compared with S2AS. If fixation with S2AS is necessary in patients with LSTV despite the possible increased risk of vascular injury, a prior detailed radiographic assessment using cross-sectional imaging and preoperative planning of screw trajectories should be performed to account for the altered bone and soft tissue anatomy. Intraoperative navigation could further aid to improve patient safety for S2AS in LSTV patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.