
Abstract
Study Design:
Systematic literature review.
Objectives:
To comprehensively review the S2-alar iliac (S2-AI) screw technique for pelvic fixation in pediatric neuromuscular scoliosis.
Methods:
Articles identified from the PubMed and EMBASE databases were reviewed for relevance and applicability, and the studies were summarized.
Results:
Eight articles met the inclusion criteria. A total of 277 pediatric patients underwent spinopelvic fixation using S2-AI fixation for neuromuscular scoliosis; the mean follow-up was 3 years (range = 0.75-6 years). Six articles had level III evidence (5 retrospective cohort studies, 1 observational study), and 2 articles had level IV evidence (case series). Wound complications occurred in 34 (12.2%) patients. Instrumentation complications occurred in 36 patients (13.0%), including lucency around the screw (6.5%), screw fracture (3.6%), disengaging of the set/screw or rod from the tulip head (2.8%), and screw displacement (0.7%). Three patients (1.1%) required reoperation for instrumentation failures. The overall reoperation rate—including 3 hardware replacements and 3 cases of L5-S1 pseudarthrosis—was 2.1%. The mean Cobb angle correction was 51.4°, and the mean pelvic obliquity correction was 14.8°; deformity correction was maintained at 3- and 5-year follow-ups. There were 10 (3.6%) cases of implant prominence/implant-related pain, 1 case of sacroiliac joint pain (resolved with longer screw placement), and no major neurological or vascular complications secondary to S2-AI screw placement.
Conclusions:
This review suggests that the use of S2-AI screws in pediatric neuromuscular scoliosis is efficacious with a reasonable safety profile and provides a useful technique for pelvic fixation in children with scoliosis.
Keywords
Introduction
Pelvic obliquity is caused by the extension of the scoliotic curve into the pelvis 1 ; the resultant coronal and sagittal imbalance requires spinopelvic fixation for deformity correction. 2 Historically, the Galveston technique, 3 which involves complicated 3-dimensional contouring of rods, 4 -6 was used; however, iliac screws or S2-alar iliac (S2-AI) screws can provide better pull-out strength and the ease of modular components to incorporate with the remainder of the fusion construct. The addition of iliac fixation to the caudal end of constructs can decrease stress on S1 and improve fusion outcomes.
First described in 2007 by Sponseller, 7 the S2-AI screw technique is a method of pelvic fixation with screws placed through the sacral ala that cross the sacroiliac joint and are directed into the ilium (“low-profile pelvic fixation”). 8 -11 The pull-out forces of iliac and S2-AI screws are similar, 12,13 but iliac screws frequently require offset connectors and extensive soft tissue dissection at the posterior superior iliac spine, which may lead to prominent instrumentation and related complications. 14 In contrast, one of the main advantages of S2-AI screws is decreased implant prominence because of a more midline entry point that places the screw head into a thicker soft tissue envelope that aligns with rostral instrumentation without the need for offset connectors. Thus, S2-AI screws can be placed without exposing the iliac crest and potentially devascularizing the overlying soft tissues, which may decrease complications caused by implant prominence.
Limited data exist regarding the long-term sequelae of the use of S2-AI screws in pediatric patients, specifically for spinopelvic fixation in neuromuscular scoliosis. 3 These patients benefit from the low-profile technique because they commonly have a smaller body habitus with less soft tissue available to cover their instrumentation, they are frequently sitting and may be more susceptible to discomfort from prominent screws, and they have higher risks of wound-related complications. The varying definitions of complications in previous reports regarding spinopelvic fixation have made comparing techniques difficult. 1 In this systematic review, we aim to describe the current body of literature on the use of S2-AI screws for spinopelvic fixation in pediatric neuromuscular scoliosis. We hypothesize that the use of S2-AI screws for spinopelvic fixation in neuromuscular scoliosis has low clinical, neurological, and instrumentation-related complication rates and acceptable outcomes when compared with traditional iliac screw fixation or other pelvic fixation techniques.
Methods
Literature Search
A literature search was performed using PubMed and EMBASE in January 2019; the aim of our search was to identify English-language studies with large sample size (>15 patients). Medical subject heading (MeSH) and title/abstract keywords were included to maximize the inclusion of any article that related to the utility of S2-AI screws for pelvic fixation in pediatric neuromuscular scoliosis. The PubMed Search was “(‘s2 alar’ OR (s2 AND (alar/exp OR alar))) AND (pediatric/exp OR pediatric),” and the EMBASE search was “(‘s2 alar’ OR (s2 AND (‘alar’/exp OR alar))) AND (‘pediatric’/exp OR pediatric).”
Two authors screened the titles and abstracts of the resulting articles. Throughout the abstract and full-text review process, the reviewers evaluated articles separately. To ensure selection accuracy and to avoid misrepresentation of populations and pathologies, a subset of articles was jointly reviewed as a form of an interrater reliability test. Full-text papers were acquired, and data was extracted. Articles were only included if they contained the search terms and appropriate study population of interest. Each study was individually assessed for bias and independently graded for level of evidence. 15,16
Variables of Interest
We examined clinical and radiographic variables reported in each of the identified articles. These included number of patients, complication rates and types, length of follow-up, and overall conclusions. Surgical variables included wound/infectious complications (ie, dehiscence, superficial infection, deep infection), implant problems/failure (eg, screw fractures), other screw problems, screw lucency >2 mm, lateral screw protrusion, and symptomatic complications (eg, implant prominence, pain, pseudarthrosis). Radiographic variables included Cobb angle correction, pelvic obliquity correction (defined as the angle between the horizontal and the intercristal line 10 ), sacroiliac joint dysfunction, and L5-S1 pseudarthrosis.
A pooled analysis was performed for the primary and secondary outcomes. The primary outcome was the frequency of postoperative complications from S2-AI screw placement. Secondary outcome measures included mean degree of correction, pelvic obliquity correction, and sacroiliac joint degeneration and morbidity attributable to S2-AI screws.
Statistical Analysis
Data was summarized in a descriptive manner using means and standard deviations.
Results
The results of the systematic review can be found in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) diagram in Figure 1. The PubMed and EMBASE searches yielded a total of 8 articles that met the inclusion criteria and were used for review and analysis (Table 1). All articles were published within the last 10 years: 1 from 2010, 1 from 2015, 1 from 2016, 3 from 2017, and 1 each from 2018 and 2019. Six of the articles were level III evidence (5 retrospective cohort studies, 1 observational study), and 2 articles were level IV (case series). Four of the studies were cohort studies with comparison groups. All studies examined the use of S2-AI screws in neuromuscular scoliosis in patients requiring spinopelvic fixation.
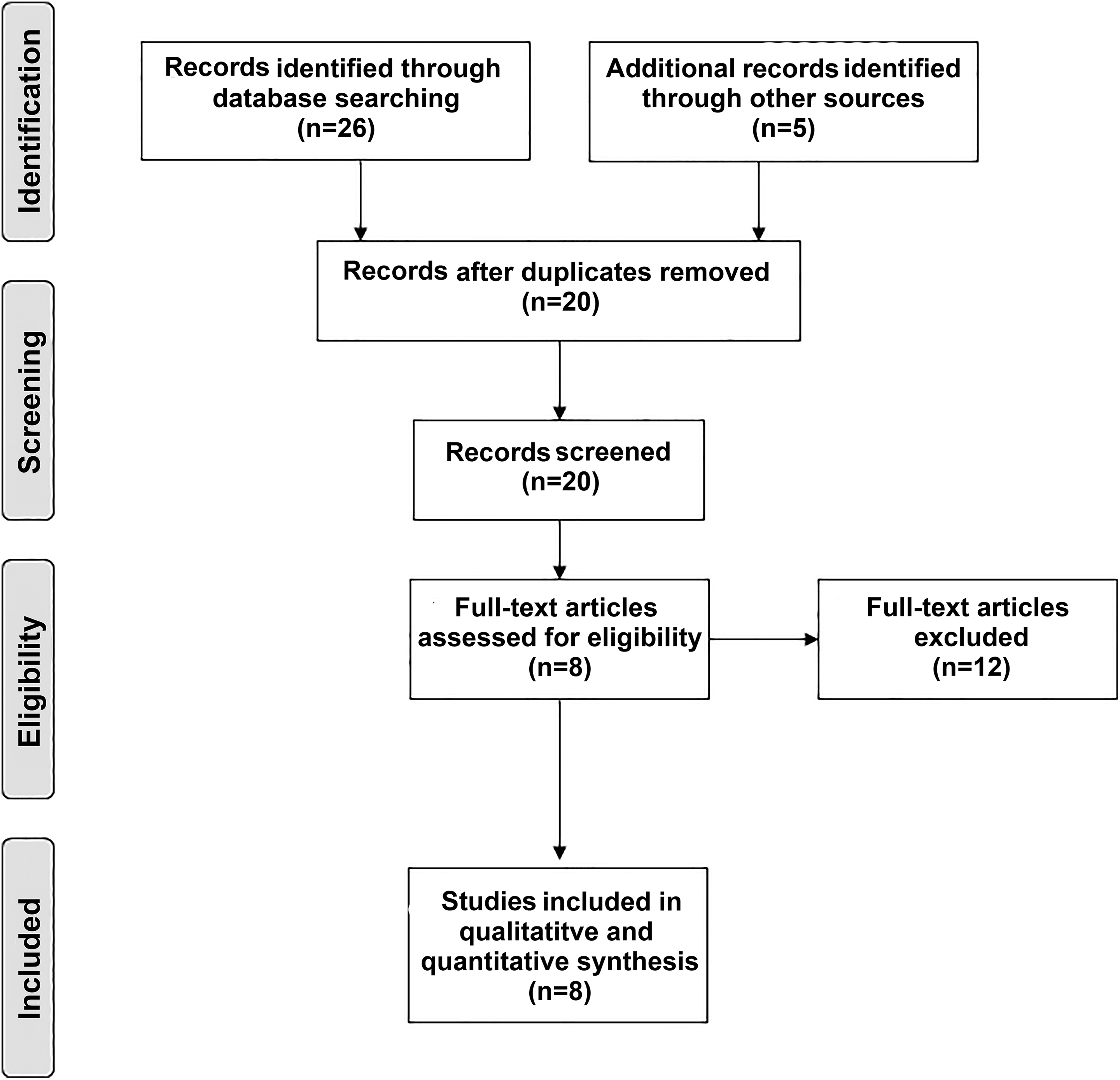
PRISMA flowchart. PubMed and EMBASE literature search on S2-AI screws in pediatric neuromuscular scoliosis.
Literature Review With Large Studies Examining S2-AI Screws in Pediatric Patients.
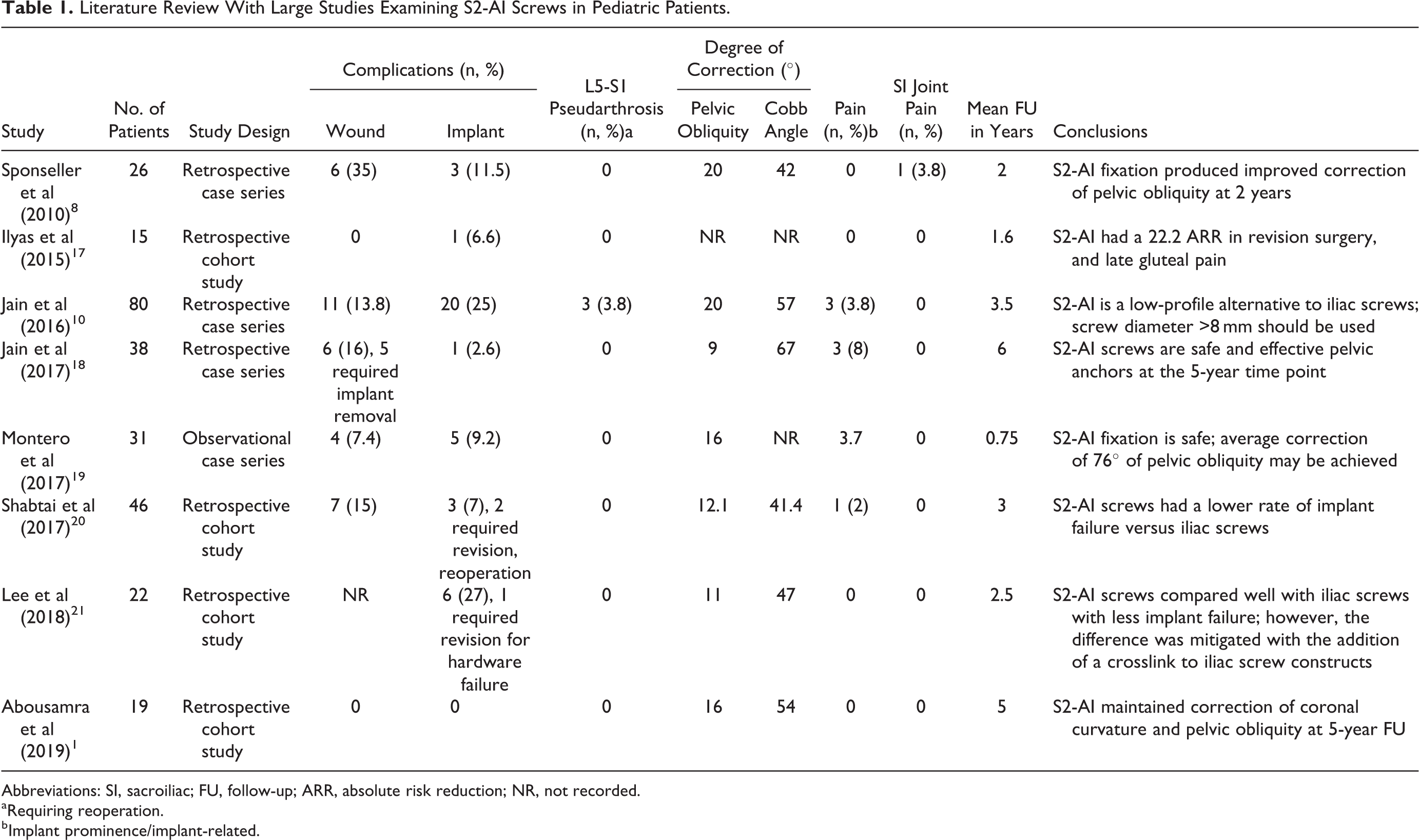
Abbreviations: SI, sacroiliac; FU, follow-up; ARR, absolute risk reduction; NR, not recorded.
a Requiring reoperation.
b Implant prominence/implant-related.
Among the 8 studies, there were 277 patients; these were pooled together for analysis. Wound complications occurred in 34 (12.2%) patients. Of the 34 total wound-related complications, 11 were reported as wound dehiscence, 3 as superficial wound infections, 16 as deep infections (7 requiring hardware removal, 9 requiring irrigation and debridement), and 4 as surgical site infection with no description of treatment or hardware management.
Instrumentation complications secondary to the S2-AI screws occurred in 36 patients (13.0%). Three cases of L5-S1 pseudarthrosis thought to be secondary to S2-AI hardware failure were reported, all in one study. 10 The mean Cobb angle correction magnitude was 51.4°, and the mean pelvic obliquity correction magnitude was 14.8°. Ten cases (3.6%) of implant prominence/implant-related pain were recorded. There was one case of sacroiliac joint pain, which resolved after longer screws were placed. No major neurological or vascular complications were experienced secondary to S2-AI screw placement. The mean follow-up time for the studies was 3 years (range = 0.75-6 years).
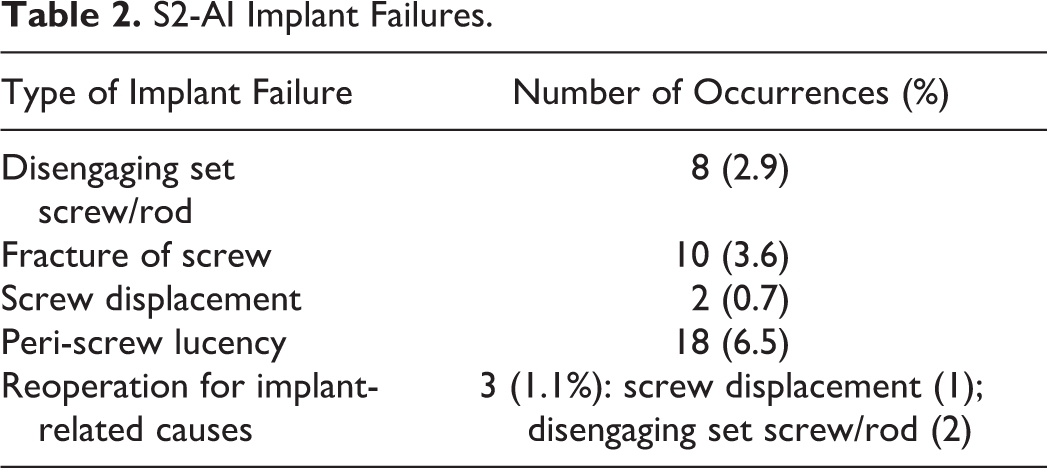
Table 2 summarizes the implant failures that occurred. The most common occurrence was lucency around the screw, which occurred in 6.5% of cases. The next most common event was screw fracture (3.6%), followed by disengaging of the set/screw or rod from the tulip head (2.8%) and screw displacement (0.7%). It is notable that only 3 patients required reoperation for S2-AI hardware failures, which yielded a frequency of 1.1%. The overall reoperation rate from all 277 patients—including 3 hardware failures requiring revision and 3 cases of lumbar pseudarthrosis—was 2.1%.
S2-AI Implant Failures.
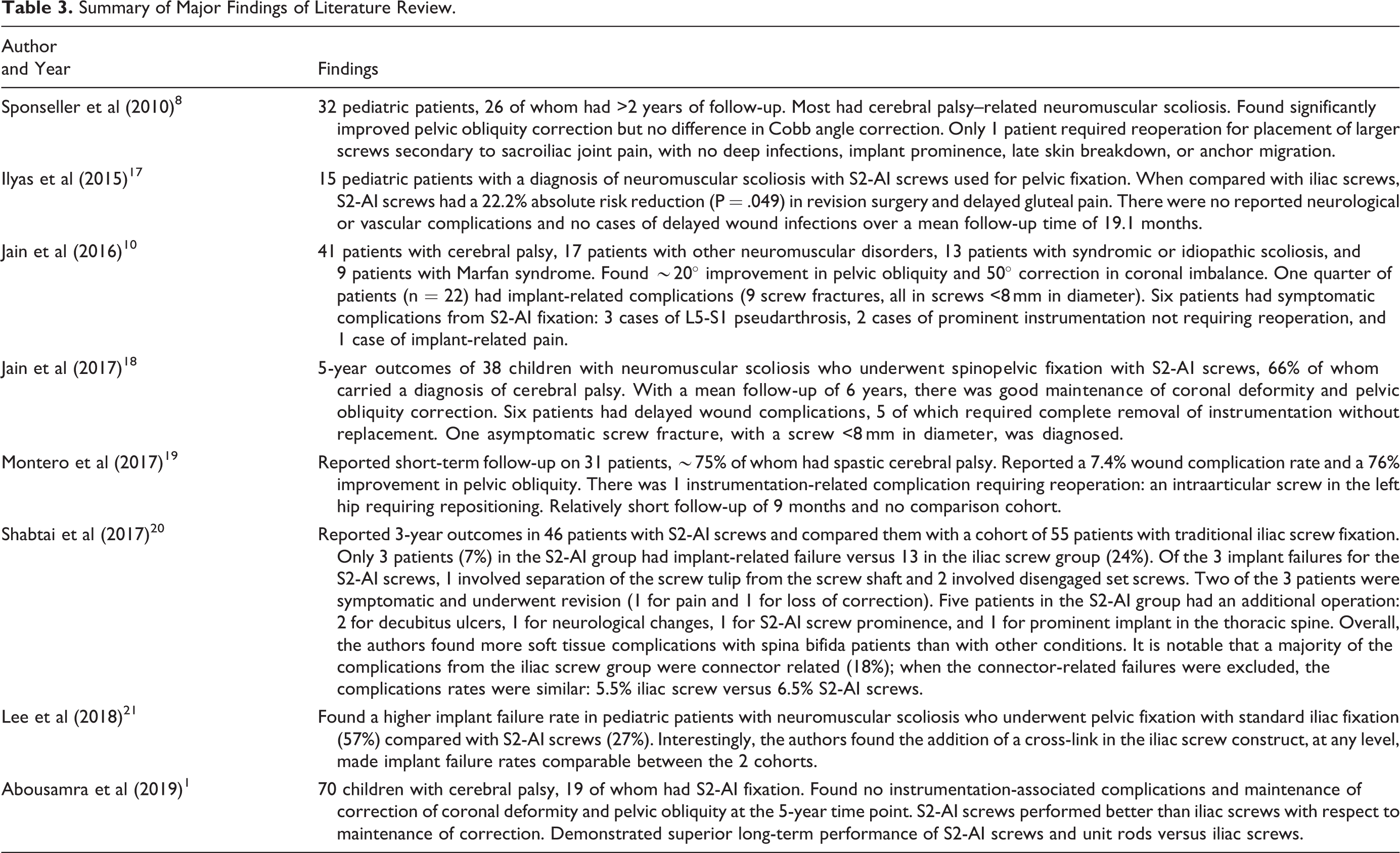
A summary of the major findings of each study can be found in Table 3.
Summary of Major Findings of Literature Review.
Discussion
In this review, we found an increasing use of S2-AI screws for spinopelvic fixation in neuromuscular scoliosis over the past 10 years. Overall, the complication profile related to the use of S2-AI screws is favorable. The frequency of superficial or deep wound infections was 12.2%, and the rate of overall instrumentation complications was 13.0%. The overall reoperation rate was 2.1%.
Evolution of Surgical Technique
The use of pelvic fixation in pediatric spinal deformity accomplishes 2 goals in neuromuscular scoliosis: (1) allowing improved correction of the deformity, including pelvic obliquity, specifically if the apex of the curvature is in the lumbar spine, and (2) stabilizing the lumbosacral junction, as this can be a point of nonunion. 22
The methods for pelvic fixation have evolved over the past 20 to 30 years as modifications to address load distribution, stability, lucency, and migration were made. Because of continued concerns about instrumentation prominence, especially in patients with neuromuscular scoliosis, 8 Chang et al 11 introduced the technique of “low-profile pelvic fixation,” which involves a sacral starting point immediately caudal to the starting point of an S1 screw at the top of the S2-ala; with an angle 40° lateral and caudal, the screw captures the widest part of the sacral ala and into the thickest portion of the ilium just above the sciatic notch (Figure 2). There is a palpable change in density as the sacroiliac joint is crossed, 23 and inclusion of this joint provides tricortical bone fixation for all S2-AI screws. 14 Image guidance or fluoroscopy can be used to visualize the sciatic notch in anteroposterior and lateral views and the ilium via an oblique view. 8,11,14,24 The oblique angle of the screw allows for the screw head to be recessed 1.5 cm deeper beneath the skin, prevents dorsal back-out of the screws, and places the screw head in line with the remainder of the construct, so no offset connector is needed (Figure 3). Iliac bolts can also be placed in a low-profile fashion with the entry point at the iliac crest just lateral to the S2 foramen rather than at the traditional site at the posterior superior iliac spine. This alternative entry point can facilitate alignment of screws with the rostral instrumentation without the use of offset connectors and its deep location may obviate the need for extensive soft tissue dissection.
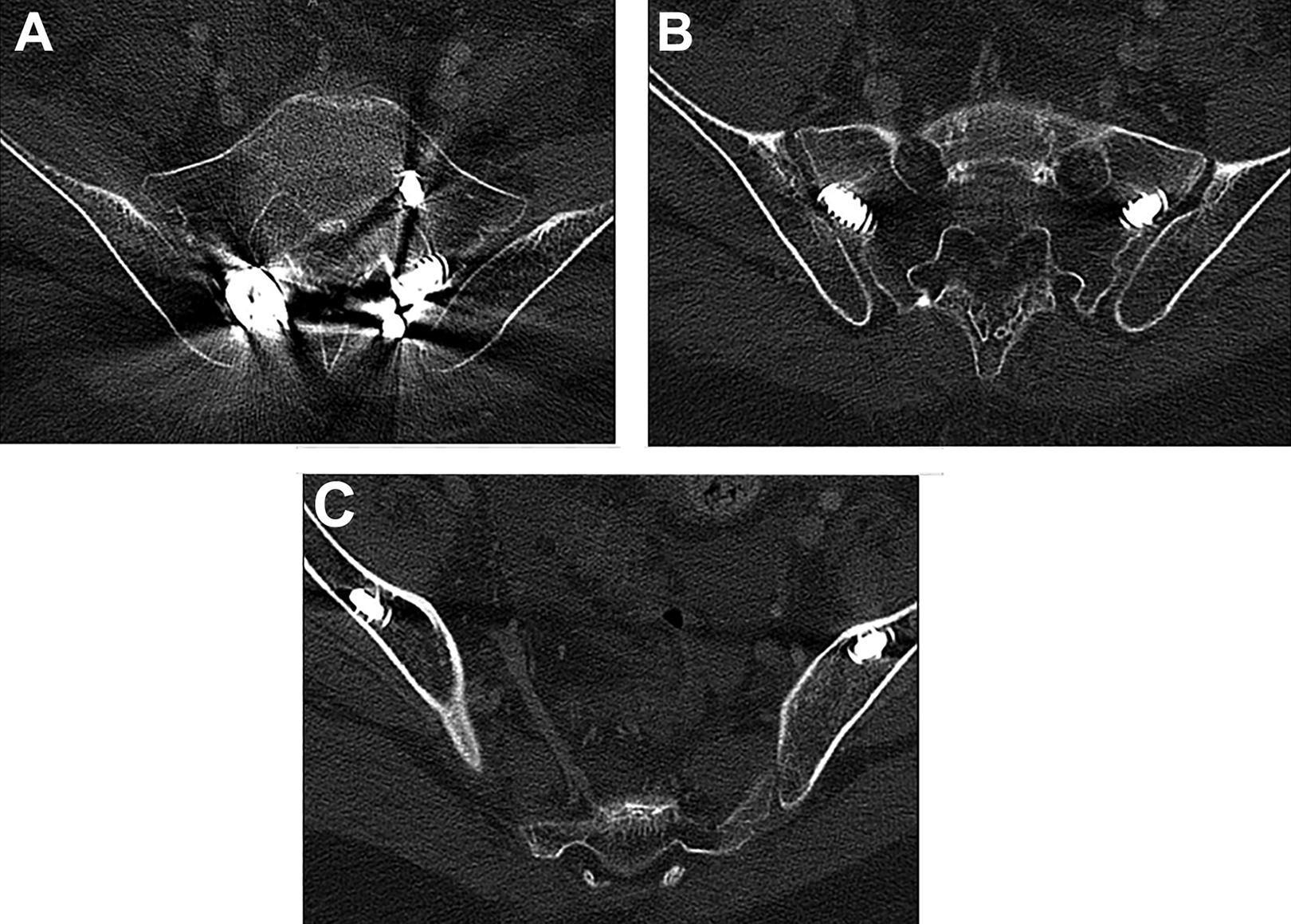
Axial computed tomography images demonstrating the entry point (A) on the second sacral vertebra is 25 mm caudal to the superior endplate of S1 and 22 mm lateral to the midline, angled 40° laterally and 40° caudally. Image guidance or anterior/posterior lateral fluoroscopy can be used to identify and visualize the sciatic notch and the ilium via an oblique view. The screw trajectory is 40° to 50° from horizontal and 20° to 30° caudal aimed toward the greater trochanter, rostral to the sciatic notch; the ideal trajectory is one that allows the screw to interface with dense bone above the sciatic notch for better pullout strength. (B) There is a palpable change in density once the sacroiliac joint is crossed; inclusion of the sacroiliac joint provides tricortical bone fixation for all S2-AI screws. 14 (C) The tip of the screw lies in the deep cancellous bone of the ilium.
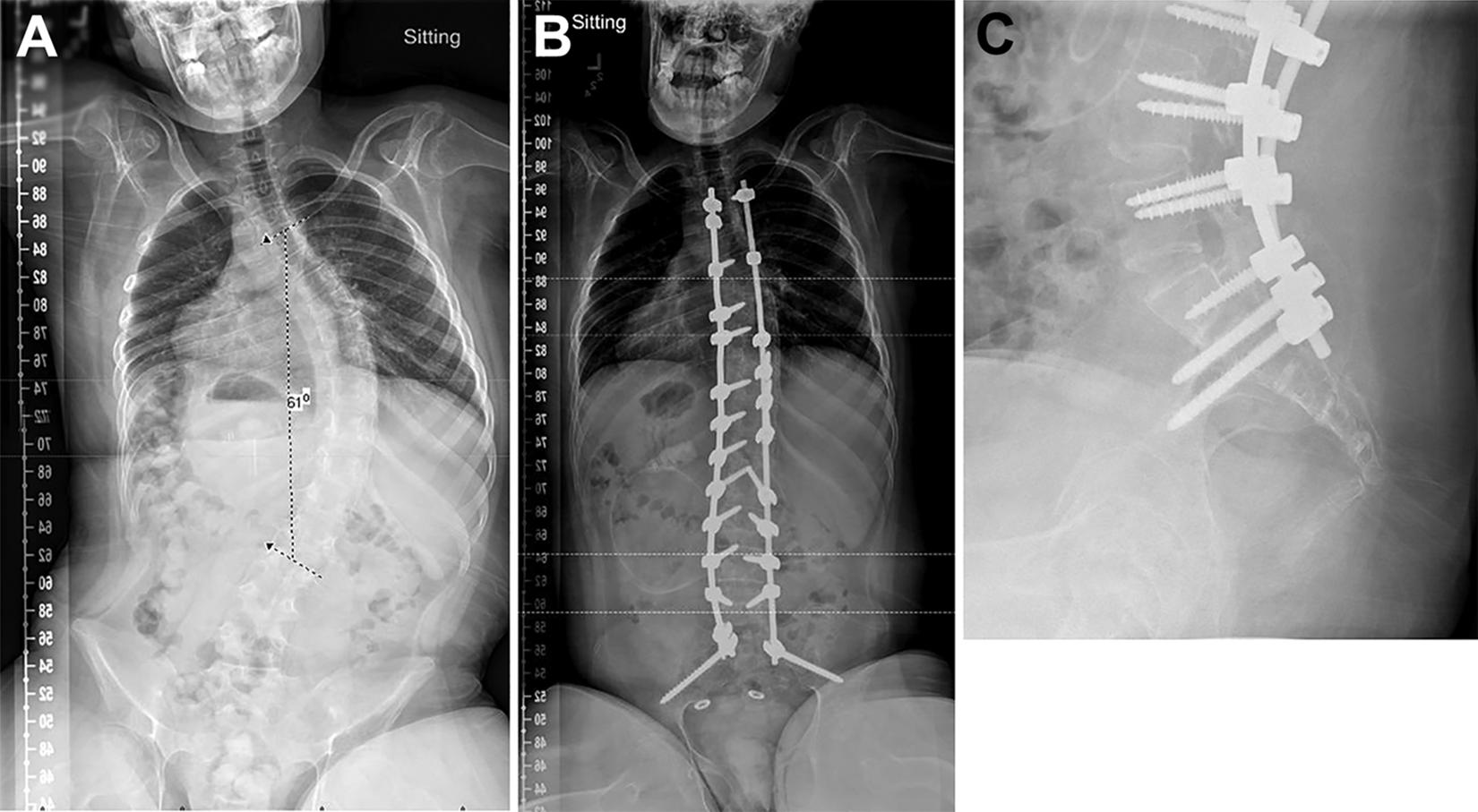
Preoperative anterior/posterior (A) and postoperative anterior/posterior (B) and lateral (C) radiographs demonstrating the S2-AI screws with no need for an offset connector (A) with the tulip heads in line with one another and the screws recessed deep in the pelvis allowing for more skin coverage versus traditional iliac screws (B).
With respect to deformity correction, the S2-AI technique may allow up to 105 mm of distance to achieve sacropelvic purchase. 11 Screw diameter and length may vary in children with neuromuscular scoliosis so screw sizes should be chosen based on anatomic parameters on preoperative films to maximize bone purchase and minimize potential neurological and vascular complications. Placement of iliac screws requires significant dissection of paraspinal muscles and adjacent skin. In children with neuromuscular scoliosis, the distal portion of the wound is most at risk for breakdown. Prominent instrumentation accompanied with extensive subfascial dissection to expose the iliac crest both contribute to wound-related issues. Screws inserted close to the posterior superior iliac spine may also contribute to pain as their prominence may cause discomfort to patients when sitting. In addition, if iliac bone graft harvest is necessary, this could also compromise the integrity of the ilium as a sole site for screw placement. 25
Pooled Results
Patients with neuromuscular disorders often have weak, osteoporotic bone, which may be weak in the sacral ala portion; thus, larger screws with cortical fixation to the ilium can be beneficial in providing a strong caudal fixation point. In addition, in accordance with the findings of Sponseller et al, 8 the S2-AI technique provides better improvement in pelvic obliquity because it allows for direct, rigid control of the pelvis for distraction or compression. 10 The studies examined in our review reported degrees of correction from 9° to 20° (Table 2).
Lee et al 21 found comparable performance between S2-AI and iliac screws, with improved rates of radiographic implant failure in the S2-AI screw group compared with the iliac screw group, but the rates became equivalent when a cross-link was added to a structural interbody support construct. In the adult population, S2-AI screws were independently associated with fewer unplanned reoperations for wound-related complications and instrumentation failures than the use of iliac bolts. 26
Implant-related failure, as reported by Jain et al, 10 can be as high as 25%, but the findings in this comprehensive review that demonstrate a mean instrumentation failure rate of 13% suggest the rate is generally consistent with previous findings in the pediatric deformity literature with respect to pelvic fixation. 27 -29
Lumbar pseudarthrosis occurred in 3 of the 277 cases: one in a patient who received shorter screws (7 ×50 mm), one in a patient with Loeys-Dietz syndrome, and one in a patient with an acquired iliac deformity.
Among the main disadvantages to the S2-AI screw technique is the risk of injury anterior in the pelvis and to the sacroiliac joint 30 ; however, in this pooled analysis, there were no reported neurological or vascular injuries related to screw placement and only one case of sacroiliac joint pain, which resolved with placement of longer screws. Additionally, crossing the sacroiliac joint could theoretically increase sacroiliac pain, but S2-AI screws are associated with less postoperative sacroiliac pain. 31
Only 3 patients required reoperation for the instrumentation failures—which yielded a frequency of 1.1%. In the report by Jain et al, 10 all 9 screw fractures experienced in that study were in patients that received screw with diameters ≤8 mm; thus, these authors recommended placing larger-diameter screws for improved purchase and reduced fracture/failure rates. The overall reoperation rate from the 277 patients total was quite low at 2.1%.
S2-AI fixation has lower rates of implant failure (4% to 7% vs 7% to 24%), fewer revisions for implant failure (4% vs 7% to 11.6%), fewer complications for screw prominence (2% vs 11%), and lower rates of wound infection requiring reoperation (15% vs 22%) than traditional iliac fixation in neuromuscular scoliosis. 17,20 The lower rates of hardware failure are likely a result of eliminating the need for a screw-to-rod connector. A recent meta-analysis by De la Garza Ramos et al 32 demonstrated a 14.2% revision surgery rate due to mechanical failure or wound complications in adults who underwent S2-AI instrumentation and a 2.6% infection rate, with a 1.8% rate of screw prominence/pain. In our analysis of patients with neuromuscular scoliosis, we found a wound complication rate of 12.2% but a 5.7% wound complication rate requiring reoperation and an overall revision surgery rate of 1.1% for hardware-related problems, which is much lower than in a healthy, adult population. Thus, the use of S2-AI screws in pediatric neuromuscular scoliosis holds up well.
Limitations
Although this was a comprehensive, systematic review of the literature, there are shortcomings based on the quality of the evidence available for review. All of the studies are level III or IV evidence; thus, recall bias may be inherent to each of them. In addition, many of the studies come from centers that developed the technique; thus, selection bias may be a factor. Additionally, not all of the variables of interest were available from each of the reviewed publications.
In many of the publications there was no comparison group, and there were varying lengths of follow-up time. Surgical technique and use of intraoperative computed tomography imaging or fluoroscopy may vary from center to center as well; this limitation may conversely improve the generalizability of the findings. Although the main comparison is drawn between S2-AI screws and iliac screws, the goal of this study was not to compare the 2 techniques but rather to highlight the published characteristics of S2-AI screw fixation in this population.
We have purposefully not included demographic data including age at the time of surgery, sex, or Gross Motor Function Classification System and ambulatory/nonambulatory status. The purpose of the investigation was to assess the efficacy of S2-AI screws in pediatric neuromuscular patients undergoing deformity correction utilizing spinopelvic fixation. This is treating the pooled cohort as a homogenous entity in order to maximize the data output and potential conclusions. Further study of patient-level factors leading to S2-AI-related morbidity is necessary.
Conclusions
In this report, we have outlined the current literature reporting the use of S2-AI screws in pediatric spinal deformity correction. We found the evidence supporting the use of S2-AI because of the relatively favorable complication profile and good correction of coronal deformity and pelvic obliquity. The reoperation rate in the pooled analysis was 2.1%.
Ultimately, a prospective collection of data with meticulous complication profiles is needed, but on the basis of the data in this study, we believe the use of S2-AI screws is safe and durable for spinopelvic fixation in pediatric neuromuscular scoliosis. Although the results of the use of S2-AI screws were superior to those of iliac screws, modifications of surgical technique, protocol, and patient care may be needed to improve the overall outcomes and limit morbidity in patients with neuromuscular scoliosis. Further long-term studies are necessary to describe the behavior of S2-AI screws in the neuromuscular population along the sacroiliac joint and potential long-term complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Alexander Ropper is a consultant for Globus and Stryker. Dr Darrell Hanson is a consultant with Medtronic, Dupuy Synthes, and Alphatec and receives royalties from Depuy Synthes. Dr Benny Dahl serves on the K2M advisory board. The other authors have no disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.