
Abstract
Study Design
Systematic review and meta-analysis
Objectives
The present review aimed to summarize the evidence regarding differences in proprioception between children with and without adolescent idiopathic scoliosis (AIS).
Methods
Seven electronic databases were searched from their inception to April 10, 2021. Articles were included if they involved: (1) AIS patients aged between 10 and 18 years, (2) measurements of proprioceptive abilities, and (3) comparisons with non-AIS controls. Animal studies, case reports, commentaries, conference proceedings, research protocols, and reviews were excluded. Two reviewers independently conducted literature screening, data extraction, risks of bias assessments, and quality of evidence evaluations. Relevant information was pooled for meta-analyses.
Results
From 432 identified citations, 11 case-control studies comprising 1121 participants were included. The meta-analyses showed that AIS participants displayed proprioceptive deficits as compared to non-AIS controls. Moderate evidence supported that AIS participants showed significantly larger repositioning errors than healthy controls (pooled mean difference = 1.27 degrees, P < .01). Low evidence substantiated that AIS participants had significantly greater motion detection threshold (pooled mean difference = 1.60 degrees, P < .01) and abnormal somatosensory evoked potentials (pooled mean difference = .36 milliseconds, P = .01) than non-AIS counterparts.
Conclusions
Consistent findings revealed that proprioceptive deficits occurred in AIS patients. Further investigations on the causal relationship between AIS and proprioception, and the identification of the subgroup of AIS patients with proprioceptive deficit are needed.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) is the most common three-dimensional spinal deformity among schoolchildren. Adolescent idiopathic scoliosis is defined as a lateral curvature of the spine (i.e., Cobb angle ≥10°) in adolescents aged between 10 and 18 years with unknown causes. 1 The global prevalence of AIS was 1.34% (pooled data from a meta-regression among 17 countries between 1977 and 2005). 2 Although AIS patients may not display curve progression during puberty, those untreated may develop severe curves, resulting in breathing difficulty, 3 spinal pain, 4 as well as cosmetic concerns. 5 To minimize the risk of developing severe curvatures, AIS patients with signs of curve progression are treated conservatively or surgically. 2 Although bracing may slow down the spinal curve progression, 6 some individuals with brace may perceive poorer body images and quality of life than untreated and surgically treated counterparts. 7 Although the innovative surgical management (e.g., vertebral body tethering 8 ) have been developed to treat AIS, surgery still involve some degree of risks. Therefore, it is critically important to accurately identify AIS patients at risk of curve progression so that timely interventions can be provided.
To date, the etiopathogenesis of AIS is unclear but the causes are thought to be multifactorial. Of various causes, some have suggested that functional abnormalities in the central nervous system (e.g., proprioceptive deficit 9 ) may be related to the pathomechanisms of AIS. 10 In order to maintain a correct spinal alignment and balance in various postures, the brain relies on proprioceptive signals from various body parts to inform the relative positions and movements of body segments.11,12 Abnormal proprioception (i.e., absence or disruption of proprioceptive afferent) can adversely affect an individual’s ability to reposition body parts and/or refine motions during functional tasks. 13 This hypothesis substantiated by the evidence that some AIS patients displayed proprioceptive deficits.14-16
The potential relationship between AIS and proprioceptive deficit is also indirectly substantiated by recent animal models. The runt-related transcription factor 3 (Runx3) knockout mice that developed severe scoliosis were characterized by a lack of tropomyosin receptor kinase C (TrkC) neurons, which connect peripheral proprioceptive mechanoreceptors with the spinal cord. 17 Similarly, the early growth response 3 knockout mice that had TrkC neurons but no muscle spindles displayed less severe spinal curves. 17 These findings together suggest that proprioceptive deficit may play an important role in the development of AIS.
Therefore, this review aimed to identify the proprioceptive deficits in AIS patients so as to inform future research.
Methods
The present review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 18 The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (Identity: CRD42020207647).
Search Strategy and Selection Criteria
The research question of the present review was based on the Patient, Intervention/exposure, Comparison, and Outcome (PICO) framework, 19 that is, “Are AIS patients comorbid with impaired proprioception comparing to healthy adolescents?” Primary studies were included in the present review if they involved: (1) participants aged between 10 to 18 years, (2) a patient group diagnosed with AIS, (3) a control group with non-AIS children, and (4) evaluations of proprioceptive ability. Animal studies, human cadaver studies, case reports, commentaries, conference proceedings, protocol registries, reviews, and non-English articles were excluded.
Systematic searches were conducted on seven online databases, including Academic Search Complete, Allied and Complementary Medicine Database (AMED), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials, Excerpta Medica Database (CENTRAL), Medical Literature Analysis and Retrieval System Online (MEDLINE), and Web of Science. The search period was from the inception of databases to April 10, 2021. The search strings for this review consisted of three aspects: adolescents, idiopathic scoliosis, and proprioception. Forward citation search via Scopus and hand-searching of the reference lists of all included studies were conducted to retrieve additional relevant studies. The details of the search are presented in Supplementary Appendix 1.
Study Selection
Two independent reviewers (K.K.L.L. and K.K.P.L.) conducted the two-stage screening of literature. After removing duplicates, the title-abstract screening was conducted. Studies considered to be eligible by both reviewers were included for the full-text screening. Discrepancies between the two reviewers were resolved by discussion and consensus. Further disagreement was arbitrated by the third reviewer (A.Y.L.W.). The selection agreement between the reviewers was assessed by Cohen’s kappa statistics.
Data Extraction
The two reviewers (K.K.L.L. and K.K.P.L.) independently extracted the data. A standardized spreadsheet form was used to extract relevant information from the included studies. Information related to the authors, years of publication, methodology (i.e., study country, research design, and sample size), participants (i.e., age, sex, and Cobb angle), and proprioception tests (i.e., measurement methods, tested body part, and findings) was extracted. Statistical data (i.e., mean and standard deviation) related to the proprioception tests was also documented.
Qualitative Synthesis
The risk of bias of the included studies was assessed independently by the two reviewers (K.K.L.L. and K.K.P.L.). Any disagreements were resolved by discussion between the reviewers. Depending on the study design, different risks of bias appraisal tools were used. Notably, randomized controlled trials and cohort/case-control studies were evaluated by the physiotherapy evidence database scale, 20 and Newcastle–Ottawa scale (NOS), 21 respectively. Further, all proprioceptive outcome measures were evaluated by the grading of recommendations, assessment, development, and evaluations (GRADE) approach to assess the quality of evidence. 22 GRADE has four levels of evidence: very low, low, moderate, and high. The certainty in the evidence was modified based on the risk of bias, imprecision, inconsistency, indirectness, and publication bias. 22 The details of relevant risk of bias assessment tools and the GRADE analysis are listed in Supplementary Appendix 2.
Data Analysis
The principal measure was the mean difference (MD) in the proprioceptive measure between participants with and without AIS. Outcome measures that only investigated by a single study were reported descriptively, while a meta-analysis was conducted for each proprioceptive measure reported by at least two included studies. The pooled estimates were calculated by random effects models and the inverse variance method. The level of significance was set at .05. The homogeneity among comparisons was calculated by the I-square statistics (i.e., the proportion of total variation in study estimates attributed to heterogeneity). 23 The I-square value was classified as having “low” (I2 ≤ 25%), “moderate” (I2 between 26 and 74%), or “high” (I2 ≥ 75%) heterogeneity. 24 Publication bias was examined by a funnel plot if the meta-analysis of a given outcome included ≥ 10 studies. 25 Review Manager version 5.4 (Cochrane Collaboration, UK) was used for the meta-analyses.
Results
The literature search retrieved 651 references. After the removal of duplicates, 432 records remained. Following the title-abstract screening, 329 citations were excluded. Of 32 screened full-text papers, 21 articles were excluded because they were unrelated to proprioception (n = 13) or did not report proprioceptive measures (n = 8). Eleven studies with 1121 participants were included in the present review.26-36 The inter-rater agreement between the two reviewers in screening articles were “almost perfect” (Cohen’s k = .96). The flow diagram of the study selection is shown in Figure 1. Flow diagram of study selection.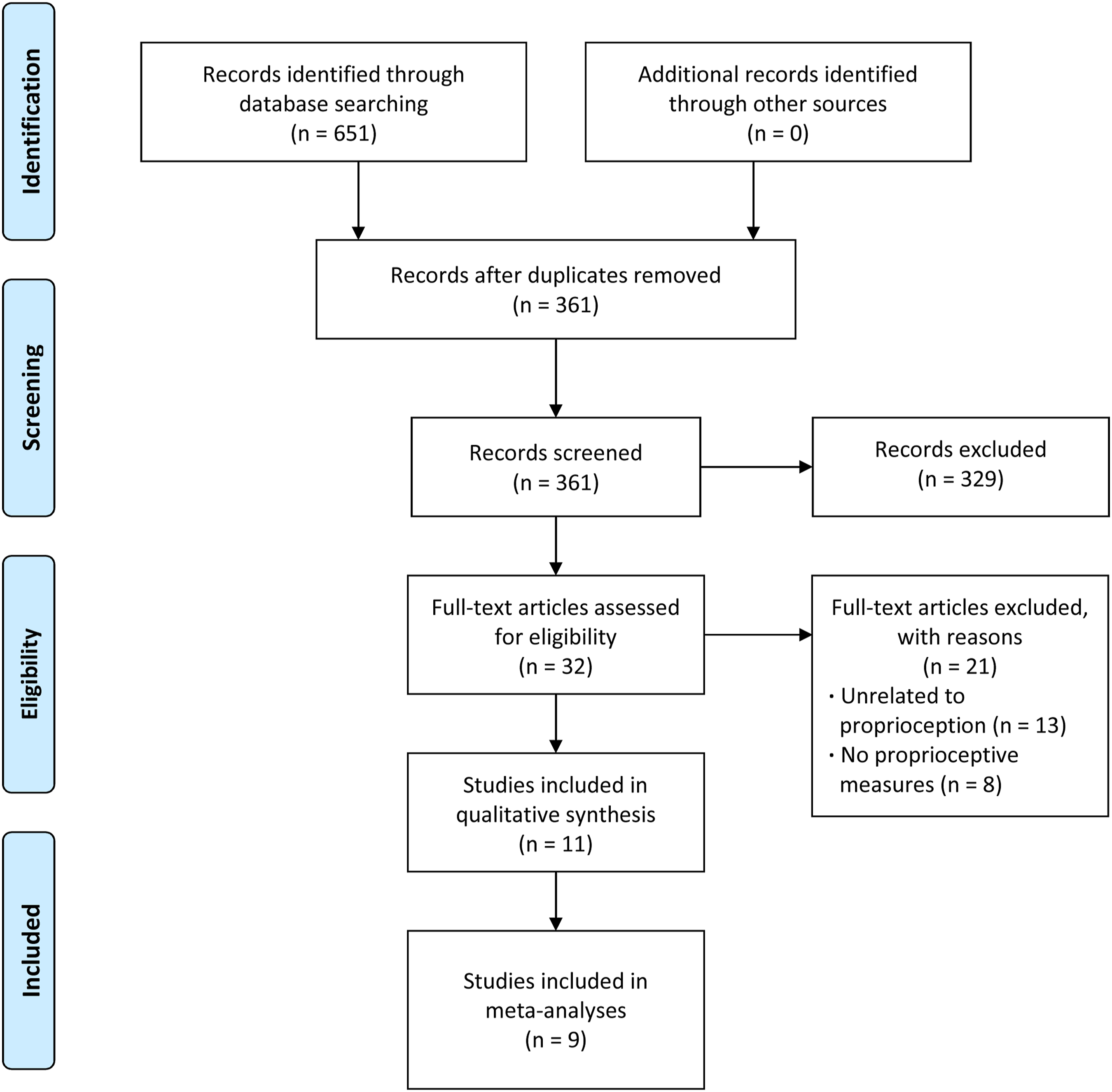
Study Characteristics
Study Characteristics.
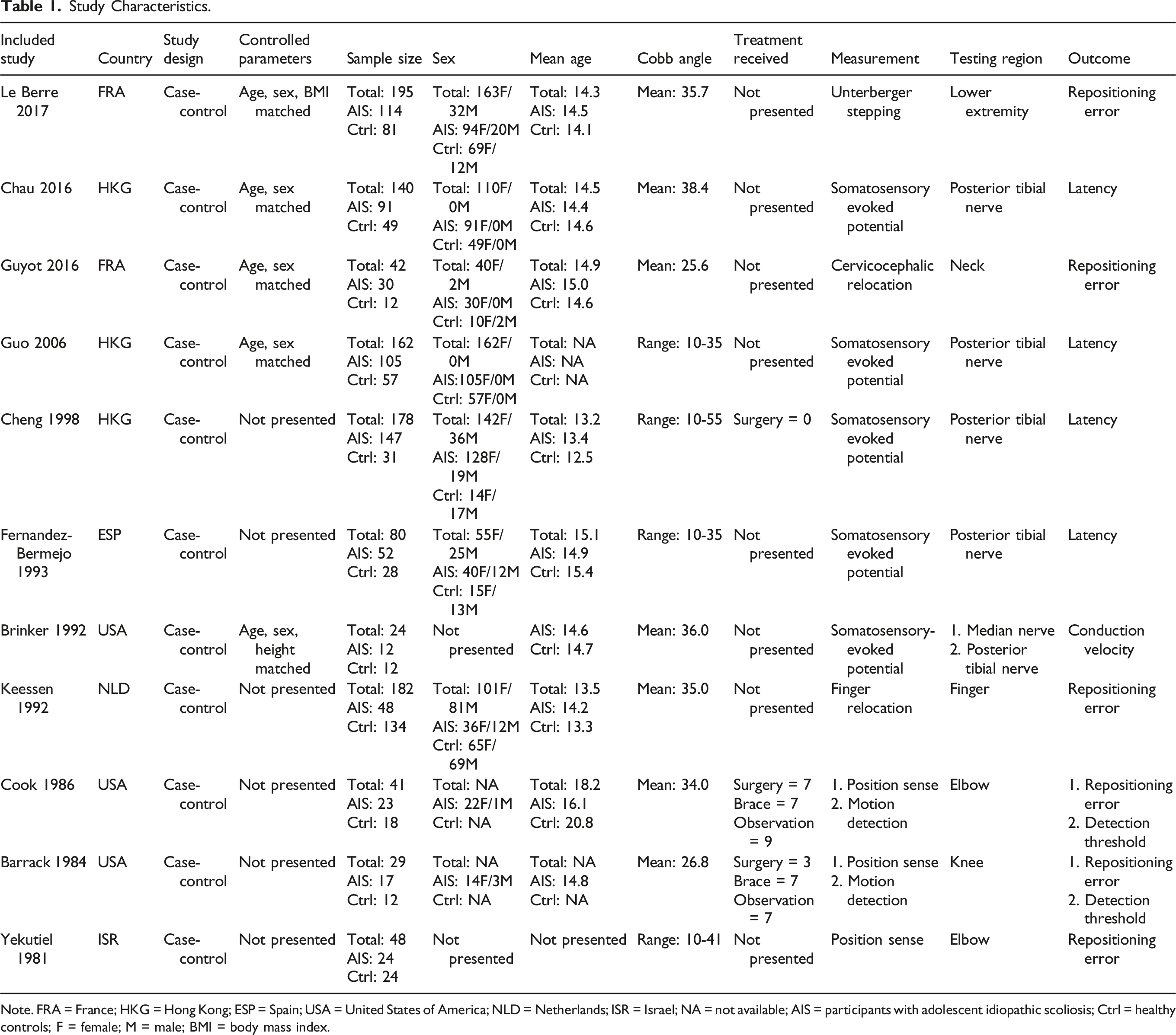
Note. FRA = France; HKG = Hong Kong; ESP = Spain; USA = United States of America; NLD = Netherlands; ISR = Israel; NA = not available; AIS = participants with adolescent idiopathic scoliosis; Ctrl = healthy controls; F = female; M = male; BMI = body mass index.
Proprioception Measurements
The proprioceptive outcome measurement in the included studies could be classified into clinical and subclinical tests (see Table 1). Six included studies used reposition tests (measuring the active repositioning error),26,28,33-36 and two studies34,35 used a motion detection test (measuring the threshold for detecting passive motions) as clinical proprioception tests. The tested body regions included neck, fingers, elbows, knees, and lower extremities. Additionally, five included studies measured the latency and conduction velocity of somatosensory evoked potentials (SSEP) of median and posterior tibial nerves as the subclinical proprioception test.27,29-32
A typical reposition test involved placing a person’s limb in a specific position (joint angle), and then asking the person to actively reproduce the same position. 13 Le Berre et al 26 and Guyot et al 28 used a stepping test and cervicocephalic relocation test, respectively, to compare the deviations between the starting position and the ending position of the feet or head. Keessen et al 33 measured the difference between the destinated left/right finger position and the self-reproduced finger position in another limb. Yekutiel et al 36 evaluated the difference between an examiner-positioned elbow joint angle and the participant reproduced angle. In Barrack et al 35 and Cook et al 34 studies, an examiner passively moved a participant’s body part and asking the participant to memorize the position before reproducing the target position. A motion detection test is the detection of the threshold for a motion required to be recognized. 13 Barrack et al 35 and Cook et al 34 used a low speed motor (0.4°/second) to move a participant’s body part and then stopped the motor immediately when the participant detected a movement or a change in position. The joint angle at the stopped point was recorded as the threshold. To conduct a SSEP test, electrical stimulation was given to either the median nerve at the wrist or the posterior tibial nerve at the ankle, while the corresponding electrical signals were recorded on the scalp (near the sensory cortex). 37
Risk of Bias Assessments
Since all included articles were case-control studies, the NOS for case-control studies was used to evaluate the methodological quality (see Supplementary Appendix 2). Three studies were classified as having “not serious,” five as having “serious,” and three as having “very serious” risk of bias. The mean NOS score was 4.9 out of 9 points. The most common risk of bias was the recruitment of healthy controls from hospitals rather than from the community. Another common problem was no clear description or statistical analysis to compare the baseline demographic data between patient and control groups. The risk of bias assessment results is presented in Supplementary Appendix 3.
Quality of Evidence
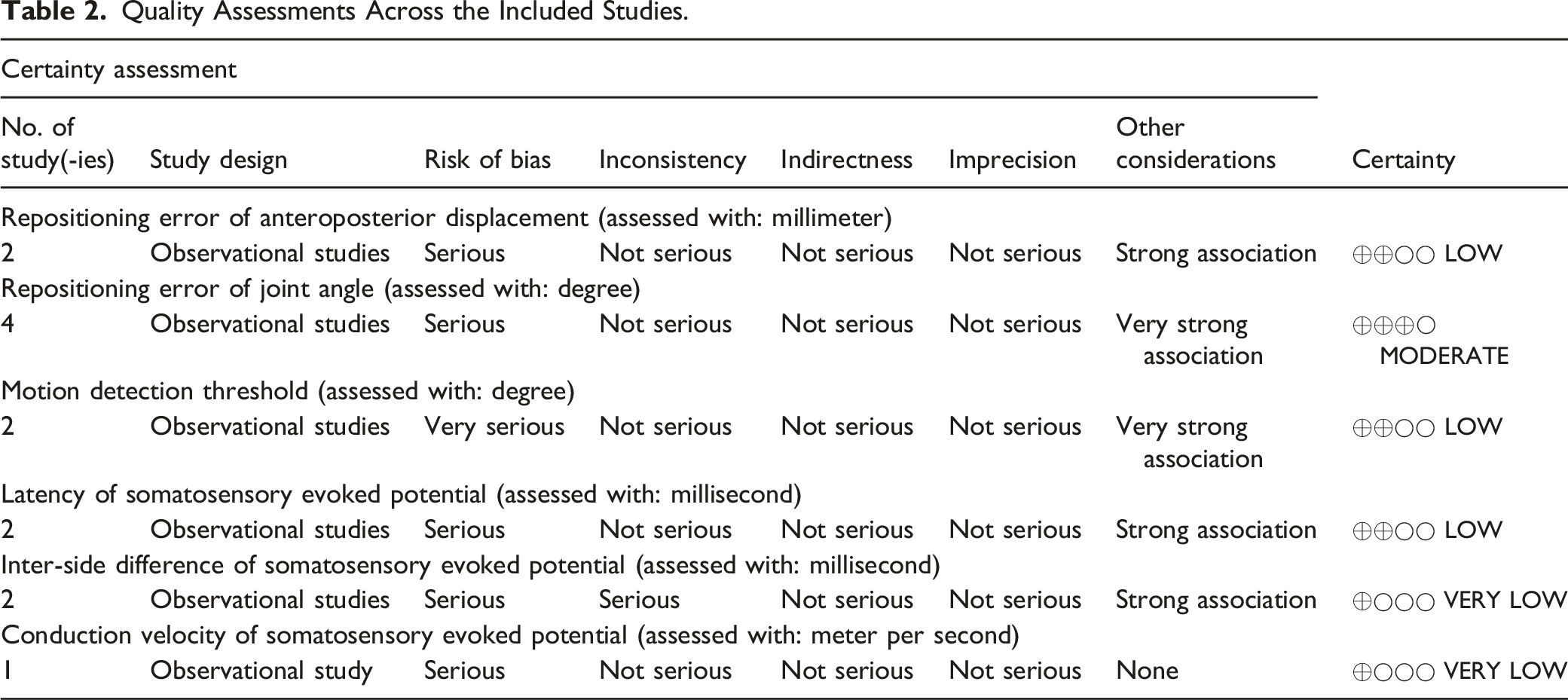
Quality Assessments Across the Included Studies.
Descriptive Statistics
The conduction velocity of SSEP was the only proprioceptive measure that could not be pooled for meta-analysis. There were no significant differences in this measure between children with and without AIS. The GRADE analysis showed “very low” level of evidence. All descriptive statistics of the clinical and subclinical measures are presented in Supplementary Appendixes 4 and 5.
Meta-Analyses of Clinical Measures
The meta-analyses of clinical proprioceptive measures are displayed in Figure 2. Pooled data from the repositioning errors of neck, elbow, and knee joint angles showed moderate evidence that AIS participants had significantly larger joint repositioning errors than healthy counterparts (3 studies; pooled MD = 1.27°; 95% CI = .57 to 1.97; P = .0004; I2 = 31%). Similarly, a meta-analysis of another two included studies revealed a low level of evidence to support that AIS participants had significantly greater repositioning errors of anteroposterior displacement in bilateral upper and lower extremities than non-AIS controls (pool MD = 10.82 mm; 95% CI = 2.03 to 19.62; P = .02; I2 = 51%). The results implied that AIS participants demonstrated greater repositioning errors. In addition, AIS participants had a larger sensitive motion detection threshold of elbow and knee joints as compared to healthy controls (2 studies; pooled MD = 1.60°; 95% CI = 1.05 to 2.15; P < .00001; I2 = 0%), yet the level of evidence was low. This indicated that AIS participants had poorer ability to detect a joint motion than their non-AIS counterparts. Forest plots of clinical proprioceptive measures.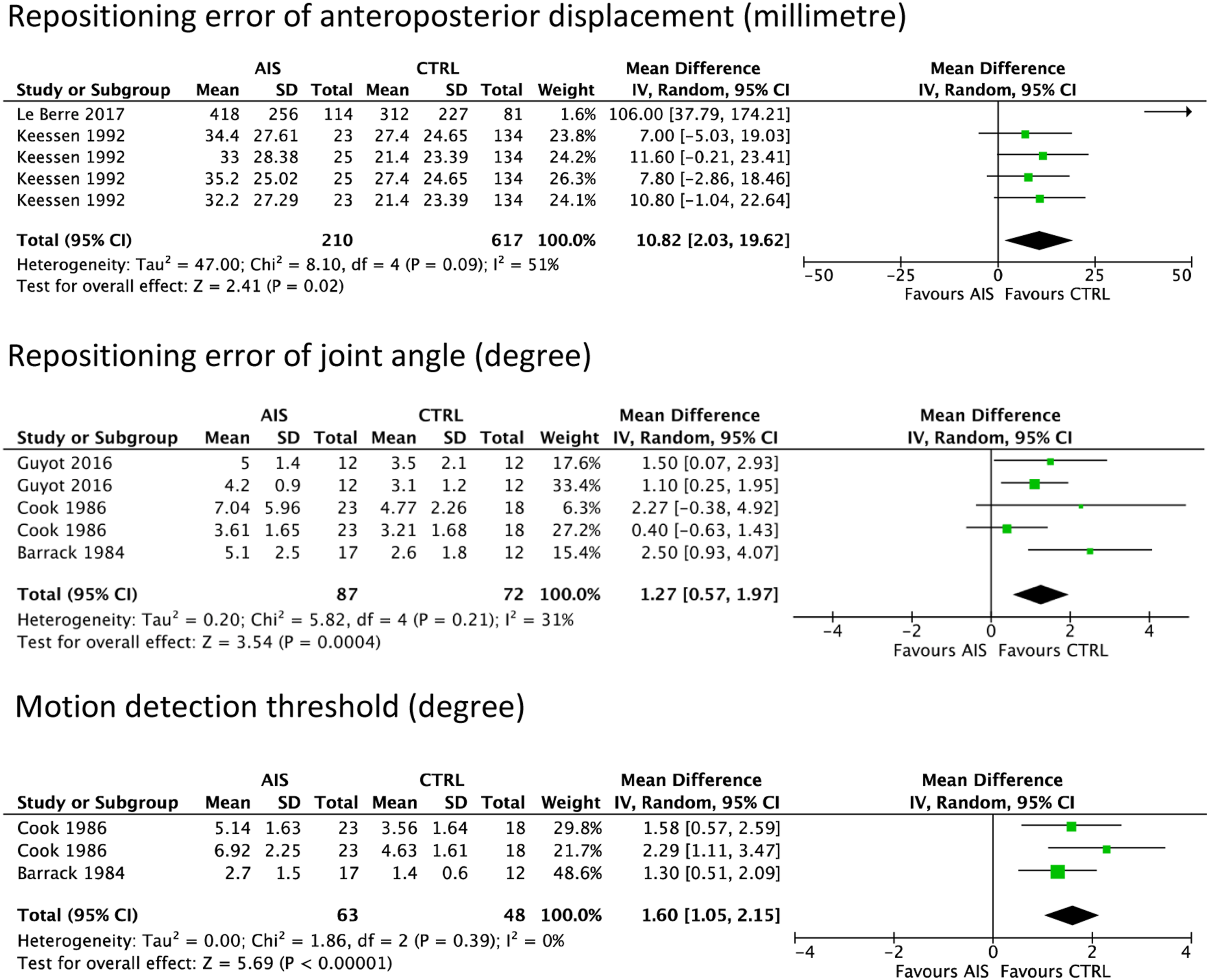
Meta-Analyses of Subclinical Measures
The meta-analyses of subclinical proprioceptive measures are presented in Figure 3. Two included studies showed that AIS participants had significantly prolonged latency of SSEP from the posterior tibial nerves than non-AIS counterparts (overall pooled MD = .36 ms; 95% CI = .07 to .65; P = .01; I2 = 0%), and the level of evidence was graded as low. The subgroup analyses revealed that data from the cortical P37 potential (pooled MD = .39 ms; 95% CI = −.02 to .79; P = .06) and that from the cortical N45 potential (pooled MD = .36 ms; 95% CI = −.09 to .75; P = .12) showed a similar trend although they were not statistically significant. Likewise, a meta-analysis of the two studies showed that AIS participants had a significantly greater inter-side difference in the latency of SSEP originated from the posterior tibial nerves than non-AIS controls (pooled MD = .40 ms; 95% CI = .08 to .71; P = .01; I2 = 76%). Specifically, AIS participants had a longer latency of SSEP on the concave side than the convex side as compared to healthy adolescents. However, the level of evidence for this measure was very low. Forest plots of subclinical proprioceptive measures.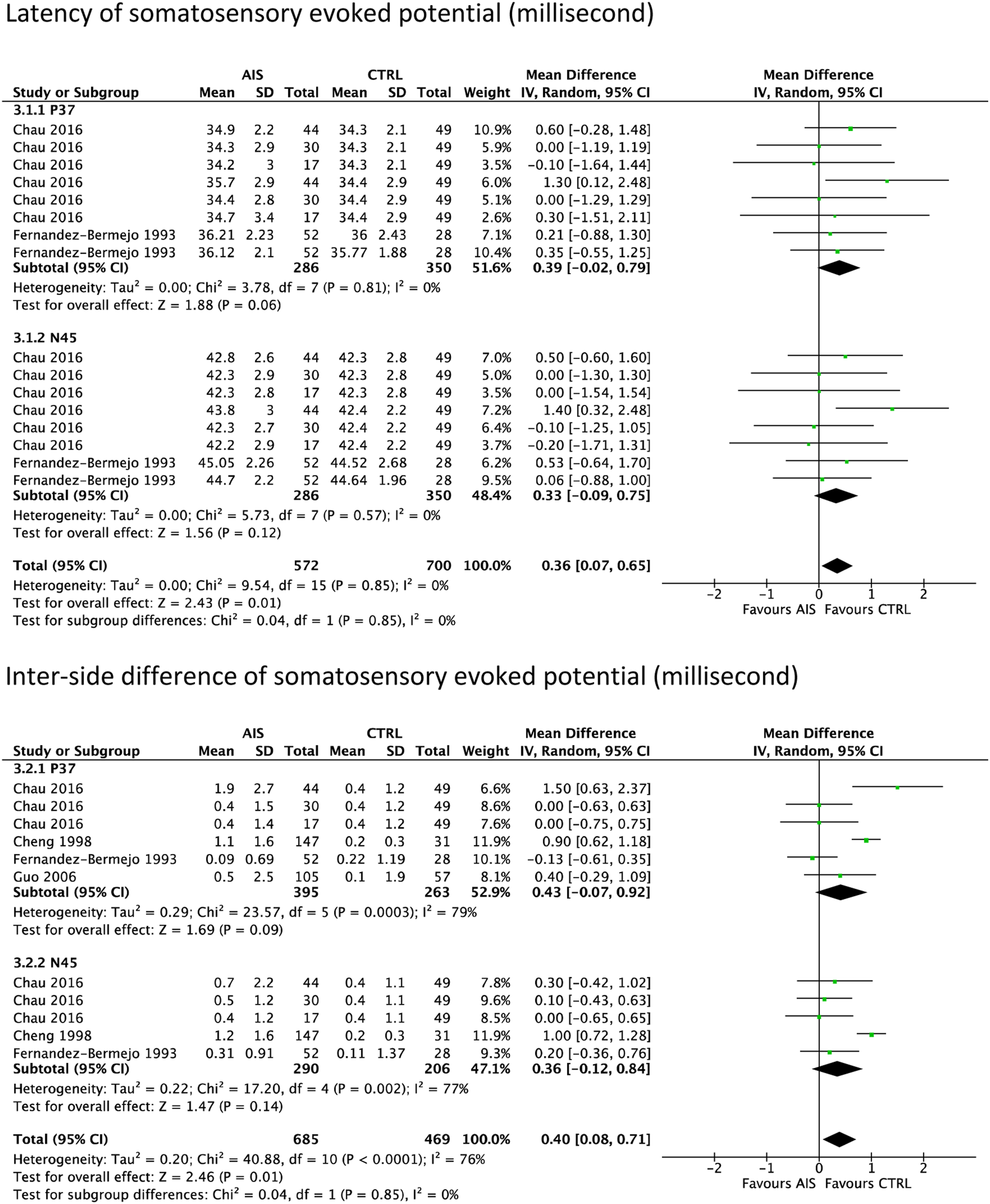
Discussion
The present review consistently showed that AIS patients displayed proprioceptive deficits (i.e., larger repositioning errors, higher motion detection threshold, and abnormal SSEP) as compared to non-AIS controls. These findings may indicate underlying changes in the central and/or peripheral nervous system(s) of AIS patients.
Several research teams have separately hypothesized that the proprioceptive defect is the cause rather than the consequence of AIS. It is thought that if proprioceptive deficit is the triggering factor for AIS initiation, the severity of proprioception dysfunction might be unrelated to the subsequent curve severity. Conversely, if proprioceptive deficits are secondary to AIS, larger Cobb angles and the curve progression rate of children with AIS may be associated with poorer proprioceptive functions. Cheng et al noted that AIS patients with abnormal SSEP have a diverse curve patterns and curve severity, 30 which implied that there was no relationship between the severity of AIS and the extent of proprioceptive deficits. Le Berre et al 26 also revealed no significant relationship between the magnitude of the spinal curve and the repositioning errors of lower limbs in AIS patients. These studies showed that AIS patients were characterized by proprioceptive deficits, but their curve magnitudes were unrelated to the severity of proprioceptive deficits. However, the case-control study design of these studies prevented the determination of causal relations.
The presence of AIS patients that displays proprioceptive deficits is substantiated by recent genetic studies. Researchers have identified an association between human patients with scoliosis and proprioception-related gene mutation, namely piezo type mechanosenstive ion channel component 2 (PIEZO2). Two AIS patients from Canada and the United States with the poor proprioceptive ability (i.e., less sensitive to the direction of arm and leg movements as well as less accurate finger-to-nose repositioning) demonstrated autosomal recessively inherited loss-of-function variants in the PIEZO2 gene. 38 Comparably, two French twin sisters with the mutated PIEZO2 gene developed severe scoliosis and showed abnormal SSEP. 39 Several case series have also reported similar results, which attested to the relationship between scoliosis and proprioceptive deficits.40-42 Importantly, a recent case-control study found that the expression of PIEZO2 gene was related to the proprioceptive deficits in AIS patients who received spinal fusion. 43 The authors used the Unterberger stepping test 26 to classify AIS patients into impaired (n = 18) and unimpaired (n = 16) proprioception groups and took their paraspinal muscle biopsy during surgery. The impaired group demonstrated significantly less expression of PIEZO2 gene and a significantly smaller number of muscle spindle as compared to the unimpaired group. A significant positive relationship was also noted between PIEZO2 gene expression level and the average number of muscle fibers in the muscle spindle. These findings imply that the suboptimal expression of PIEZO2 gene may be related to the defective proprioception in AIS patients, which could be associated with the etiology of AIS.
Although the included studies have shown that proprioception is altered in AIS participants, several knowledge gaps remain to be resolved. First, the consistent findings of proprioceptive deficits at different body regions of AIS patients may suggest systemic changes in proprioception rather than a localized effect in a particular body part. However, since prior studies mainly evaluated peripheral proprioception, the extent of spinal proprioceptive deficits in AIS patients remains uncertain. It is possible that spinal proprioception (especially thoracic and lumbar regions) may also be compromised. Second, while the existing studies28,39 seem to indicate that only a subgroup of AIS patients displays proprioceptive deficits, the characteristics of this subgroup remain unclear. Guyot et al 28 found that some AIS participants had difficulty in performing a repositioning task accurately, yet there were no differences in age, sex, and Cobb angles between those with and without proprioceptive deficits. Unfortunately, there is no consensus regarding the gold standard of clinical proprioception test(s) for AIS. Therefore, it is critically important to develop reliable and valid clinical proprioception tests to identify the subgroup of AIS patients who display proprioceptive deficits for further training and follow-ups. Third, the roles of proprioception on the initiation and/or progression of AIS, as well as its relationships with the patterns or severity of the curve are still elusive.
The present review has some limitations. All the included studies adopted a case-control design. They could not reveal the causal relationship between AIS and proprioceptive deficits. Additionally, the overall quality of the evidence was low in the included studies, which might have been limited by confounders. The lack of reporting of demographic data in the patient and control groups could not affirm that the two groups were comparable. Furthermore, most of the reported proprioceptive deficits in the current review were only reported in one or two primary articles, which may underestimate the findings due to insufficient evidence. There was also little information about the validity and reliability of the used proprioception tests, and the respective minimal clinically important difference for determining the proprioceptive abnormality was not reported. These factors may reduce the sensitivity and specificity of the tests in defining the proprioceptive deficits. In addition, since only English articles were included in this review, some non-English studies might have been missed. Although most of the included studies were published before the 21st century, the significance of the reported results might be underpowered.
Collectively, there is consistent evidence supporting that proprioceptive deficits occur in some AIS patients. However, it remains unclear whether there are systemic proprioceptive deficits in both spinal and peripheral regions. Further investigation on the causation between AIS and proprioceptive deficit, as well as the determination of AIS patient subgroup with proprioceptive deficits are necessitated.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211066824 – Supplemental Material for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211066824 for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis by Kenney K. L. Lau, Karlen K. P. Law, Kenny Y. H. Kwan, Jason P. Y. Cheung, Kenneth M. C. Cheung and Arnold Y. L. Wong in Global Spine Journal
Supplemental Material
sj-pdf-2-gsj-10.1177_21925682211066824 – Supplemental Material for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-2-gsj-10.1177_21925682211066824 for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis by Kenney K. L. Lau, Karlen K. P. Law, Kenny Y. H. Kwan, Jason P. Y. Cheung, Kenneth M. C. Cheung and Arnold Y. L. Wong in Global Spine Journal
Supplemental Material
sj-pdf-3-gsj-10.1177_21925682211066824 – Supplemental Material for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-3-gsj-10.1177_21925682211066824 for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis by Kenney K. L. Lau, Karlen K. P. Law, Kenny Y. H. Kwan, Jason P. Y. Cheung, Kenneth M. C. Cheung and Arnold Y. L. Wong in Global Spine Journal
Supplemental Material
sj-pdf-4-gsj-10.1177_21925682211066824 – Supplemental Material for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-4-gsj-10.1177_21925682211066824 for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis by Kenney K. L. Lau, Karlen K. P. Law, Kenny Y. H. Kwan, Jason P. Y. Cheung, Kenneth M. C. Cheung and Arnold Y. L. Wong in Global Spine Journal
Supplemental Material
sj-pdf-5-gsj-10.1177_21925682211066824 – Supplemental Material for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-5-gsj-10.1177_21925682211066824 for Timely Revisit of Proprioceptive Deficits in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis by Kenney K. L. Lau, Karlen K. P. Law, Kenny Y. H. Kwan, Jason P. Y. Cheung, Kenneth M. C. Cheung and Arnold Y. L. Wong in Global Spine Journal
Footnotes
Acknowledgments
We would like to thank Ms Kitty Cheng for helping with the manuscript writing. We also thank Ms Jennifer Ha for assisting with the protocol registration and pilot literature screening.
Author’s Note
Institution at Which the Work Was Performed: The University of Hong Kong
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.