
Abstract
Study Design:
Retrospective review of private neuromonitoring databases.
Objectives:
To review neuromonitoring alerts in a large series of patients undergoing lateral lumbar interbody fusion (LLIF) and determine whether alerts occurred more frequently when more lumbar levels were accessed or more frequently at particular lumbar levels.
Methods:
Intraoperative neuromonitoring (IONM) databases were reviewed and patients were identified undergoing LLIF between L1 and L5. All cases in which at least one IONM modality was used (motor evoked potentials (MEP), somatosensory evoked potentials (SSEP), evoked electromyography (EMG)) were included in this study. The type of IONM used and incidence of alerts were collected from each IONM report and analyzed. The incidence of alerts for each IONM modality based on number of levels at which at LLIF was performed and the specific level an LLIF was performed were compared.
Results:
A total of 628 patients undergoing LLIF across 934 levels were reviewed. EMG was used in 611 (97%) cases, SSEP in 561 (89%), MEP in 144 (23%). The frequency of IONM alerts for EMG, SSEP and MEPs did not significantly increase as the number of LLIF levels accessed increased. No EMG, SSEP, or MEP alerts occurred at L1-L2. EMG alerts occurred in 2-5% of patients at L2-L3, L3-L4, and L4-L5 and did not significantly vary by level (P = .34). SSEP and MEP alerts occurred more frequently at L4-L5 versus L2-L3 and L3-L4 (P < .03).
Conclusions:
IONM may provide the greatest utility at L4-L5, particularly MEPs, and may not be necessary for more cephalad LLIF procedures such as at L1-L2.
Keywords
Introduction
Lateral lumbar trans-psoas interbody fusion (LLIF) is a minimally invasive technique that can improve patient reported outcomes, while possibly reducing the risks associated with anterior, oblique-lateral, or posterior interbody approaches to the spinal column.1,2 Compared to approaches for anterior or oblique-lateral interbody fusion, LLIF may allow for decreased risk of vascular injuries as the LLIF working corridor is further away from the major abdominal vessels.1,3-6 Compared to posterior approaches for interbody fusions, LLIF does not require entry into the spinal canal or foramina, therefore thecal sac and nerve root retraction are avoided. Additionally, compared to posterior approaches, a larger interbody graft can be placed with the LLIF technique which may provide for greater improvement in sagittal alignment and foraminal height, and a more favorable biomechanical and biologic environment for arthrodesis.7,8
Although minimally invasive, this procedure requires traversing of the psoas muscles, which is avoided in anterior and oblique-lateral approaches, and therefore carries the potential risk of neurological injury to the lumbar plexus and its associated nerve branches. The incidence of lumbar plexus injuries varies from 6% to 33% in some studies.4,9 The clinical manifestation of intraoperative nerve root injury can range from transient paresthesia or weakness to devastating persistent long-term pain or femoral nerve palsy.10,11 Given the proximity of the lumbar plexus with the trans-psoas retroperitoneal approach, it is the only approach marketed to require neurophysiologic monitoring to establish a safe zone within the psoas muscle. Most LLIF systems utilize surgeon-directed free-run and evoked electromyography (EMG); however, studies have questioned the accuracy of EMG during LLIF as patients have developed postoperative nerve deficits in the setting of normal EMG readings.10-13
Therefore studies have been designed to investigate the utility of multimodal intraoperative neuromonitoring (IONM) techniques to decrease the incidence of postoperative neurologic complications and some of these studies have demonstrated additive benefit of utilizing somatosensory evoked potentials (SSEP) or motor evoked potentials (MEP) during LLIF surgery.14-17 However, other studies question the utility of IONM during LLIF approaches, and have demonstrated comparable complication rates without utilizing any form of IONM. 18 The purpose of this study was to review neuromonitoring alerts in a large series of patients undergoing LLIF and determine whether alerts occurred more frequently when more lumbar levels were accessed and if alerts occurred more frequently at particular lumbar levels. The results may help guide surgeons who selectively use IONM during LLIF. We hypothesized that IONM alerts would be less common at the upper lumbar levels compared to L4-L5 where the “safe zone” is known to be smaller. 19
Methods
This study was approved by the Hospital for Special Surgery Institutional Review Board (2018-0543).
This was a retrospective database review examining IONM data collected by Accurate Monitoring LLC (Fairfield, New Jersey, USA) and U.S. Monitoring Inc. (USMON) (North Oakes, Minnesota, USA). These are private databases that are maintained internally by the company and contain demographic and procedural information from all spine surgery cases in which at least one IONM modality (EMG, SSEP, or MEP) was utilized. In addition, an accompanying IONM report is available for each case which contains monitoring strategies, baseline/intraoperative responses, and conclusions of any critical changes. The databases do not contain information regarding patient comorbidities, preoperative clinical data, complications, or postoperative outcomes.
Each database was queried for patients who underwent lateral lumbar interbody fusion between 2008 and 2018, and all cases in which at least one IONM modality was used (MMEP, SSEP, EMG) were included in this study. We included all patients that underwent isolated lateral interbody fusion between L1 and L5. We excluded patients that underwent concurrent anterior, transforaminal or posterior interbody fusion. We also excluded patients that received concurrent corpectomy, kyphoplasty, osteotomy, and cases where the level of the LLIF was unclear. The data of patients that met the inclusion and exclusion criteria contained with the Accurate Monitoring and USMON databases were merged and analyzed.
Patient demographics, procedure, lumbar level, and number of levels at which the LLIF was performed were reviewed. In addition, type of IONM used and incidence of alerts were collected from each IONM report and analyzed. Data was assessed for normality and univariate analysis was performed comparing the incidence of alerts for each IONM modality based on number of levels at which at LLIF was performed and the specific level an LLIF was performed. When analyzing the specific level of an alert, we only analyzed patients that underwent LLIF at one level because we were unable to decipher at which level an alert occurred in patients who underwent multilevel LLIF. A P-value <.05 was considered statistically significant.
Results
A total of 628 patients were included in the final analysis. The average age of the cohort was 62 ± 11 years-old and 58% were female. Single level LLIF was performed in 403 (64%) patients, 2-level in 159 (25%), 3-level in 51 (8%), and 4-level in 15 (2%). A total of 934 levels were treated with the following number of LLIFs placed at a given lumbar level: L1-L2 70 (7%), L2-L3 234 (25%), L3-L4 403 (43%), and L4-L5 227 (24%). EMG was used in 611 (97%) cases, SSEP in 561 (89%), MEP in 144 (23%).
The frequency of IONM alerts for EMG, SSEP and MEPs did not significantly increase as the number of LLIF levels increased (Figure 1). EMG alerts occurred in 2-5% of patients undergoing 1-3 level surgery, and in 13% of patients undergoing 4 level surgery (P = .21). SSEP alerts occurred in 5% of patients undergoing 1-level surgery and 8-9% of patients undergoing 2-4 level surgery (P = .60). MEP alerts only occurred in 4% of patients undergoing 1-level surgery and no alerts occurred in patients undergoing 2-4 level surgery (P = .64).
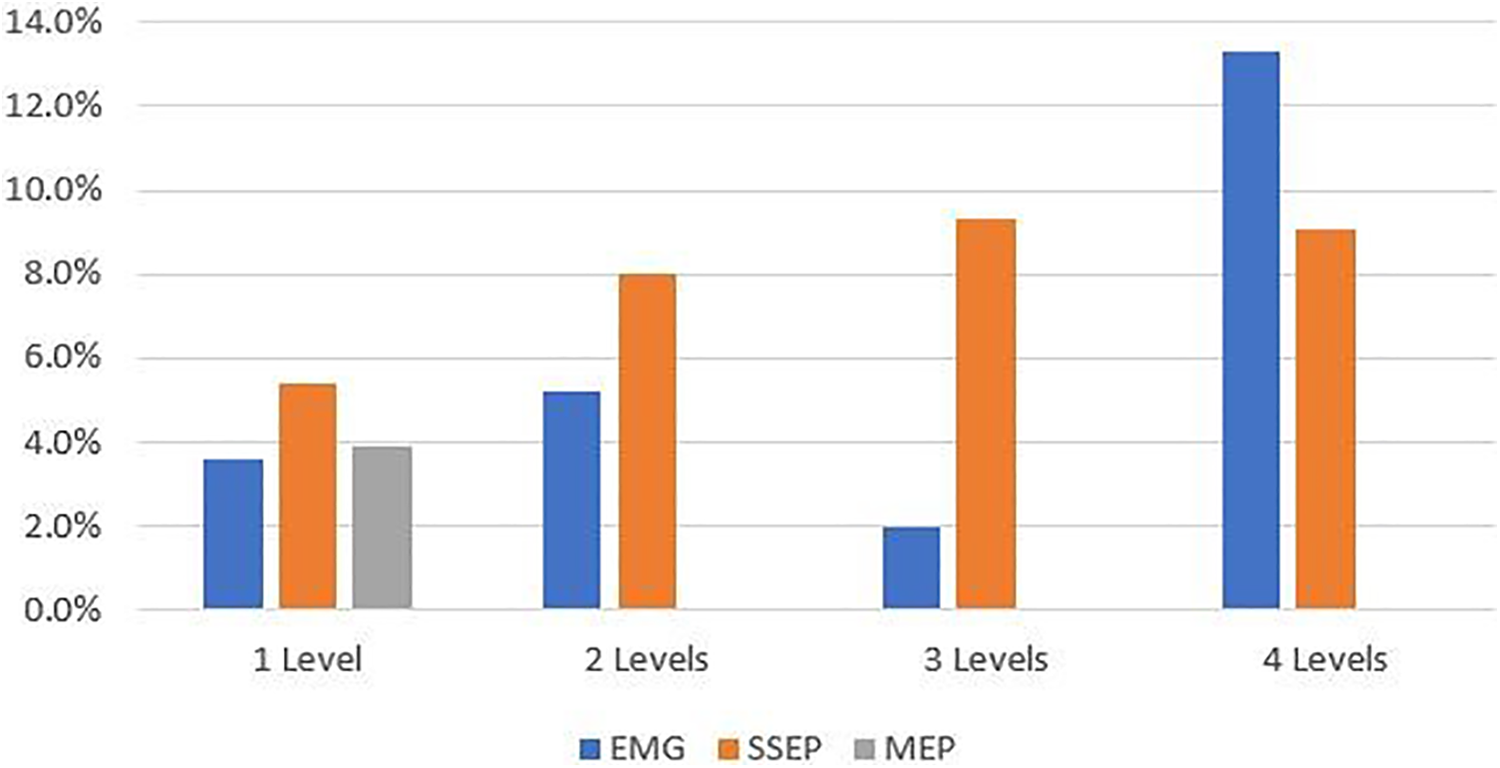
IONM alerts based on the number of lumbar levels treated.
In the 70 patients who underwent single level LLIF at L1-L2, there were no EMG, SSEP, or MEP alerts (Figure 2). EMG alerts occurred in 2-5% of patients at L2-L3, L3-L4, and L4-L5 and did not significantly vary by level (P = .34). SSEP alerts significantly varied by level and occurred in 3-5% of patients at L2-L3 and L3-L4, and 12% of patients at L4-L5 (P = .02). MEP alerts also significantly varied by level, occurring in 0% of patients at L2-L3 and L3-L4 and 17% of patients at L4-L5 (P = .03). SSEP and EMG were used in greater than 90% of patients undergoing single-level surgery. MEP was used in 29% of patients. There was no significant association between MEP use and total number of levels treated (P = .105). MEP was used more frequently at L1-L2 (45%) compared to L2-L3 (24%), L3-L4 (25%), and L4-L5 (23%), but this was not statistically significant (P = .125).
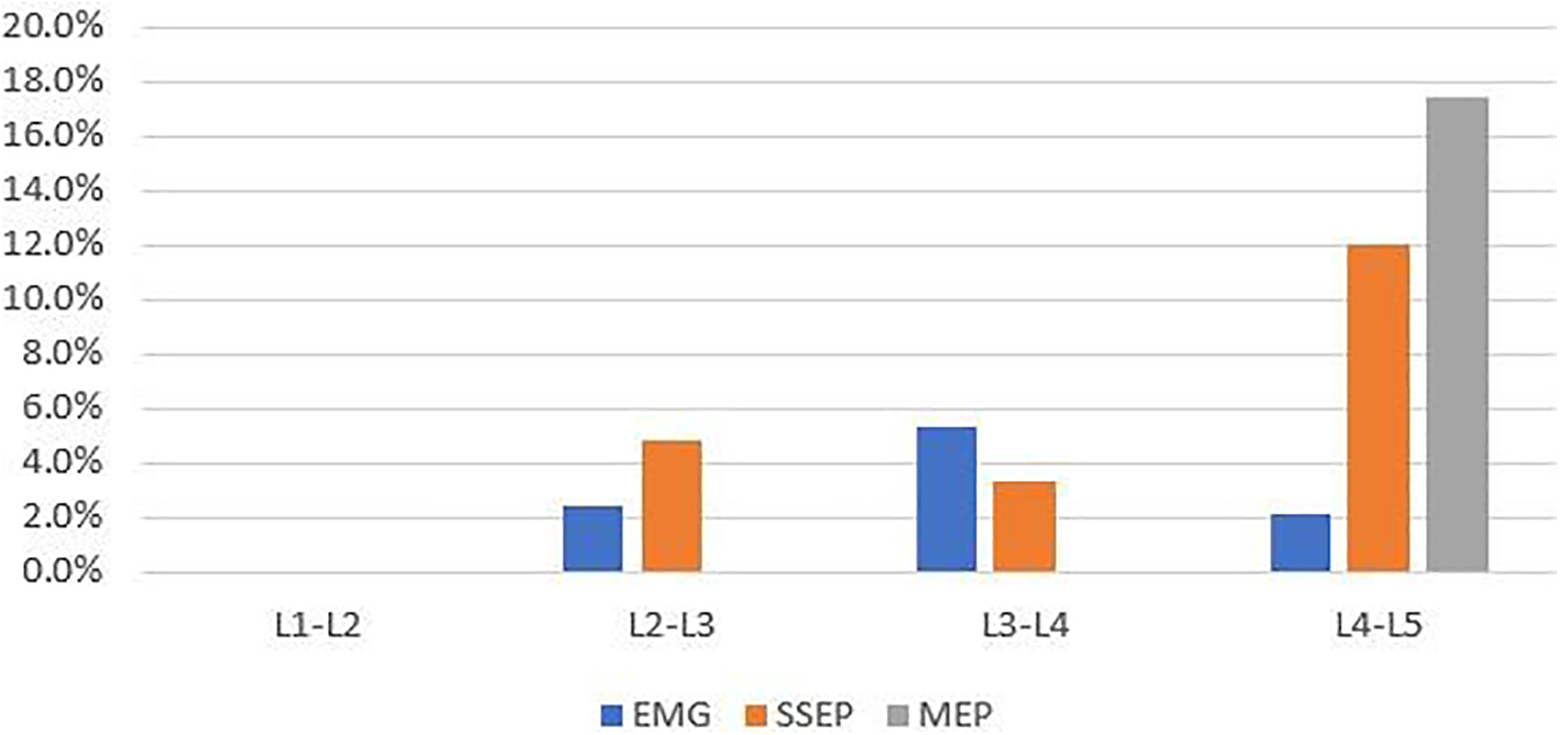
IONM alerts based on the specific level treated in patients undergoing single-level surgery.
Discussion
The use of the LLIF technique has gained popularity over the past 2 decades and studies have demonstrated improved clinical and radiographic outcomes in patients undergoing LLIF for degenerative pathology;2,20-23 however, this technique has resulted in a new set of approach-related nerve complications involving the lumbar plexus which courses through the psoas muscle.3,4,9,11,24 In an attempt to mitigate these complications, the use of IONM has been investigated.
Electromyography is commonly used during LLIF in part due to historical precedent. 1 Although studies have demonstrated the efficacy of EMG use during LLIF, it has low specificity, may not detect nerve compression, and it cannot reliably monitor sensory-specific nerves.13,24-28 The use of MEPs in LLIF may have promise because MEPs may be able to accurately monitor fully formed peripherals nerves of the lumbar plexus which innervate the quadriceps muscle.15,29 However, MEP use has its own set of limitations including necessitating avoidance of inhalational anesthesia and long-acting paralytics, and the interpretation of MEP data requires extensive training, is highly subject to variability, and is dependent on establishing accurate and reproducible baseline MEP responses. Lastly, the use of SSEPs as an IONM strategy was previously limited as traditional SSEP techniques only track the lower lumbosacral plexus (L4-S2) by monitoring the posterior tibial or peroneal nerves. SSEP monitoring of the saphenous nerve may can monitor the upper lumbar plexus, 16 but similar to MEPs, its interpretation is dependent on establishing reliable baseline signals and can vary based on thresholds for alerts. Currently the use, or combined use, of EMG, MEP and SSEP during LLIF remains without consensus in part because of the above-mentioned limitations and because some studies have demonstrated no correlation between intraoperative neuromonitoring alerts and neurological function postoperatively.10-12,14,26
Through the utilization of 2 neuromonitoring databases, we were able to review 628 patients undergoing LLIF across 934 levels, resulting in the largest study, excluding systematic reviews, analyzing IONM during LLIF in the literature. Our analysis demonstrated that in all patients that had an LLIF performed with IONM there was heterogeneity in IONM strategies. EMG was utilized in 98% of cases, SSEP in 89% and MEP is 23%. We further demonstrated that the frequency of IONM alerts does not increase when the number of levels accessed increases, and at L1-L2 there were no EMG, SSEP or MEP alerts in any patient. EMG alerts did not vary by level, SSEP alerts occurred significantly more frequently at L4-5 compared to other lumbar levels, and MEP alerts only occurred at L4-L5.
The location of the lumbar plexus as it pertains to the LLIF approach has been described in previous anatomic studies.19,30-33 At L1-L2, the lumbar plexus nerve roots are located in the posterior one-fourth to one-fifth of the disc space, and therefore the safe zone at this level is relatively large and resultant nerve root injury is less likely.19,30,32 This safe zone becomes progressively smaller at more caudal lumbar levels and at L4-L5, the safe zone may be less than 50% the width of the disc, significantly increasing the risk for nerve injury.19,32 Given this anatomic relationship, the results of our study are not surprising—there were zero EMG, SSEP or MEP alerts at L1-L2, significantly more SSEP alerts at L4-L5, and MEP alerts only occurred at L4-L5. Although this is not the first study to demonstrate a higher level of alerts at L4-L5,14,34 it is the first to demonstrate no EMG, SSEP or MEP alerts at L1-L2 in patients undergoing single-level surgery.
With regard to the number of levels approached, previous studies have demonstrated that increasing the number of operative levels may be associated with a higher likelihood of neurologic complications likely secondary to disrupting a large amount of psoas muscle volume thereby increasing the change of lumbar plexus injury.3,35 In the present study, EMG, SSEP, and MEP alerts did not vary by the number of levels accessed during LLIF surgery. It is likely that the level being accessed is a more important factor in deciding whether to use IONM as compared to the number of levels being treated.
Based on the results of this study, the authors recommend the use of EMG during LLIF based both due to historical precedent and that the frequency of EMG specific alerts did not vary based on level accessed in the analyzed data. However, SSEP and MEP may only have added utility at lower lumbar levels as there were zero alerts in either modality at L1-L2. MEPs were most frequently monitored at L1-L2, but all MEP alerts occurred at L4-L5. Further consideration should be given to selective utilization of MEPs when performing LLIF at the L4-L5 level. The nonselective utilization of multimodal IONM including SSEP and MEP for all LLIF procedures may be unnecessary and is not without significant cost. Using multimodal IONM at all lumbar levels as a standard practice may result in increased intraoperative time, unnecessary changes to anesthesia technique, and ultimately increased cost which will be passed on to the patient and payer.36,37
The results of this study demonstrate some significant findings, but they must be interpreted within the limitations of the study design. First, the study utilized 2 private IONM databases in which patients undergoing LLIF were identified but no control group of patients without IONM were available for comparison. Second, the database did not contain postoperative data, so whether the alerts prevented or missed postoperative neurologic complications is unknown. Lastly, in patients undergoing multilevel LLIF, we could not identify at which level the alert occurred and therefore our analysis of IONM alerts based on lumbar level is limited to patients undergoing single-level LLIF.
In conclusion, the results of this study have implications for future studies that attempt to clearly define which surgeries utilizing LLIF techniques require multimodal IONM. Currently, the limitations of each modality and the lack of clinical evidence have led to a wide range of IONM combinations utilized for the same LLIF approach regardless of specific lumbar level of total number of levels treated. It may be that IONM provides the greatest utility at L4-L5, particularly MEPs, and may not be necessary for more cephalad procedures such as at L1-L2. Future studies should investigate the selective use of IONM during LLIF with the hypothesis that SSEPs and MEPs have low utility at upper lumbar segments and added utility at lower lumbar segments.
Footnotes
Acknowledgments
Authors would like to thank Accurate Monitoring, LLC for the use of their data for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Sheeraz A Qureshi: Consulting: Paradigm Spine, Globus Medical Inc., Stryker K2 M; Royalties: Globus Medical, Inc., Stryker K2 M; Ownership interest: Avaz Surgical, Vital 5 (past relationship); Scientific Advisory Board/Other Office: Association of Bone and Joint Surgeons, Cervical Spine Research, Contemporary Spine Surgery, Healthgrades, International Society for the Advancement of Spine Surgery, ![]() Inc., Minimally Invasive Spine Surgery Group, Minimally Invasive Spine Study Group, North American Spine Society, Simplify Medical, Inc., Society of Minimally Invasive Spine Surgery, Spinal Simplicity, LLC; Editorial Board: Annals of Translational Medicine, Global Spine Journal, Journal of American Academy of Orthopaedic Surgeons, Spine, The Spine Journal; Honoraria: AMOpportunities, RTI Surgical Inc.; Speakers fees: Globus Medical Inc.
Inc., Minimally Invasive Spine Surgery Group, Minimally Invasive Spine Study Group, North American Spine Society, Simplify Medical, Inc., Society of Minimally Invasive Spine Surgery, Spinal Simplicity, LLC; Editorial Board: Annals of Translational Medicine, Global Spine Journal, Journal of American Academy of Orthopaedic Surgeons, Spine, The Spine Journal; Honoraria: AMOpportunities, RTI Surgical Inc.; Speakers fees: Globus Medical Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.