
Abstract
Objective
To assess the effect of pelvic floor muscle exercise in patients with chronic low back pain.
Methods
Adults (aged ≥18 years) with chronic low back pain (with or without radiculopathy) were randomized to undergo either routine treatment (ultrasonography, short wave diathermy and lumbar strengthening exercises; control group) or routine treatment with pelvic floor exercises (intervention group) for 24 weeks. Pain, disability (Oswestry Disability Index [ODI] score) and trunk muscle function were assessed at baseline and after completion of treatment.
Results
The study included 47 patients (control group n = 24; intervention group n = 23). Pain severity and ODI scores were significantly lower in the intervention group than in the control group after 24 weeks. There were no significant between-group differences in trunk muscle function.
Conclusion
Pelvic floor exercise in combination with routine treatment provides significant benefits in terms of pain relief and disability over routine treatment alone.
Introduction
Low back pain is common worldwide, with 60–80% of people affected at some time in their lives.1–3 It has a major impact on health and health-related quality of life, diminishing the capacity for standing, walking and sitting.4,5
Exercise is commonly used in the management of chronic low back pain, in particular the training of core stabilizing muscles including pelvic floor muscle.6–8 Pelvic floor muscle dysfunction is associated with the development of low back pain.9,10 The pelvic floor is a hammock of muscles that connect the pubis to the tailbone and ischial tuberosities. 11 Pelvic floor muscle insufficiency can occur as a result of pain, poor movement patterns, trauma, surgery or childbirth. 9 These muscle imbalances do not recover spontaneously, and can lead to low back, pelvis and/or hip pain. 10
The pelvic floor is an important component of the core stabilizing muscles, but many physical therapists and patients with low back pain neglect to train pelvic floor muscles. 12 In addition, there is little evidence that combined routine treatment (ultrasonography, short wave diathermy and lumbar strengthening exercises) and pelvic floor muscle exercise offers any advantage over routine treatment alone. The present study assessed the effects of routine treatment with or without pelvic floor muscle exercise in patients with chronic low back pain. The effects of both treatments on self-reported pain levels and trunk muscle strength were evaluated.
Patients and methods
Study Population
This double-blind, randomized, controlled trial enrolled patients aged 18–60 years, with chronic, nonspecific low back pain for ≥3 months, with or without radiculopathy. Patients were recruited from the Department of Rehabilitation Medicine, Pudong New District Gongli Hospital, Shanghai, China, between August 2010 and May 2012. Exclusion criteria were: (i) continuous pain >8 on a visual analogue scale (VAS; where 0 represented no pain and 10 represented the worst pain possible); 13 (ii) previous attendance at any structured pelvic floor muscle training programme; (iii) previous spinal or pelvic surgery; (iv) progressive neurological deficit, structural anomaly, acute infection, ongoing back pain treatment by other health care providers, severe instability, severe osteoporosis, and severe cardiovascular or metabolic disease.
All participants completed a questionnaire including demographic data, medical history, Oswestry Disability Index (ODI) score 14 and back pain. Patients were randomized to the intervention or control group by an independent collaborator within 2 days after enrolment, using opaque closed envelopes.
The study was approved by the Ethics Committee of Pudong New District Gongli Hospital, and all patients provided written informed consent prior to enrolment.
Treatment
All patients followed a 24-week treatment plan of routine treatment, with (intervention group) or without (control group) additional pelvic floor exercises. Both treatment programmes were led by registered physical therapists.
Routine treatment comprised ultrasonography (1 MHz continuous at 1.2 W/cm2 for 5 min), short-wave diathermy (continuous mode for 15 min) and lumbar strengthening exercises (10 repetitions each of prone leg elevation, prone chest elevation and supine bridging). 15 Routine treatment was performed three times per week for 24 weeks.
The pelvic floor muscle exercise programme was based on contraction of the pelvic floor muscles for 6 s followed by rest for 6 s, resulting in 5 contraction cycles/min. The number of contraction cycles was increased over the 24-week treatment period: week 1, 25 cycles/day (5 min total); week 2, 50 cycles/day (10 min total); week 3, 75 cycles/day (15 min total); weeks 4–24, 100 cycles/day (20 min total). 16
Outcome Measures
Outcome measures were assessed at baseline and after the 24-week treatment period. All assessments were performed by three independent, experienced physical therapists who were not employed at the participating rehabilitation centre, had no contact with patients during the treatment period and were blinded to treatment allocations. All assessments took place at Department of Rehabilitation Medicine, Pudong New District Gongli Hospital, Shanghai, China.
Outcome measures included: (i) average pain intensity over the previous week, assessed via VAS; 13 (ii) disability, assessed via ODI scoring; 14 (iii) static muscle endurance (length of time the patient was able to maintain an unsupported upper body in the prone [extension] and supine positions [flexion]); (iv) dynamic muscle endurance (number of sit-ups [flexions] and prone trunk extensions performed in 1 min). 17
Statistical Analyses
Data were expressed as mean ± SD. Differences between groups at baseline were analysed using independent samples t-test and the χ2-test. The effect of treatment was assessed via two-way analysis of variance (group × time). Statistical analyses were performed with SPSS® software, version 17.0 (SPSS Inc, Chicago, IL, USA) for Windows® and Microsoft® Excel 2003 (Microsoft, Redmond, WA, USA). A P-value <0.05 was considered statistically significant.
Results
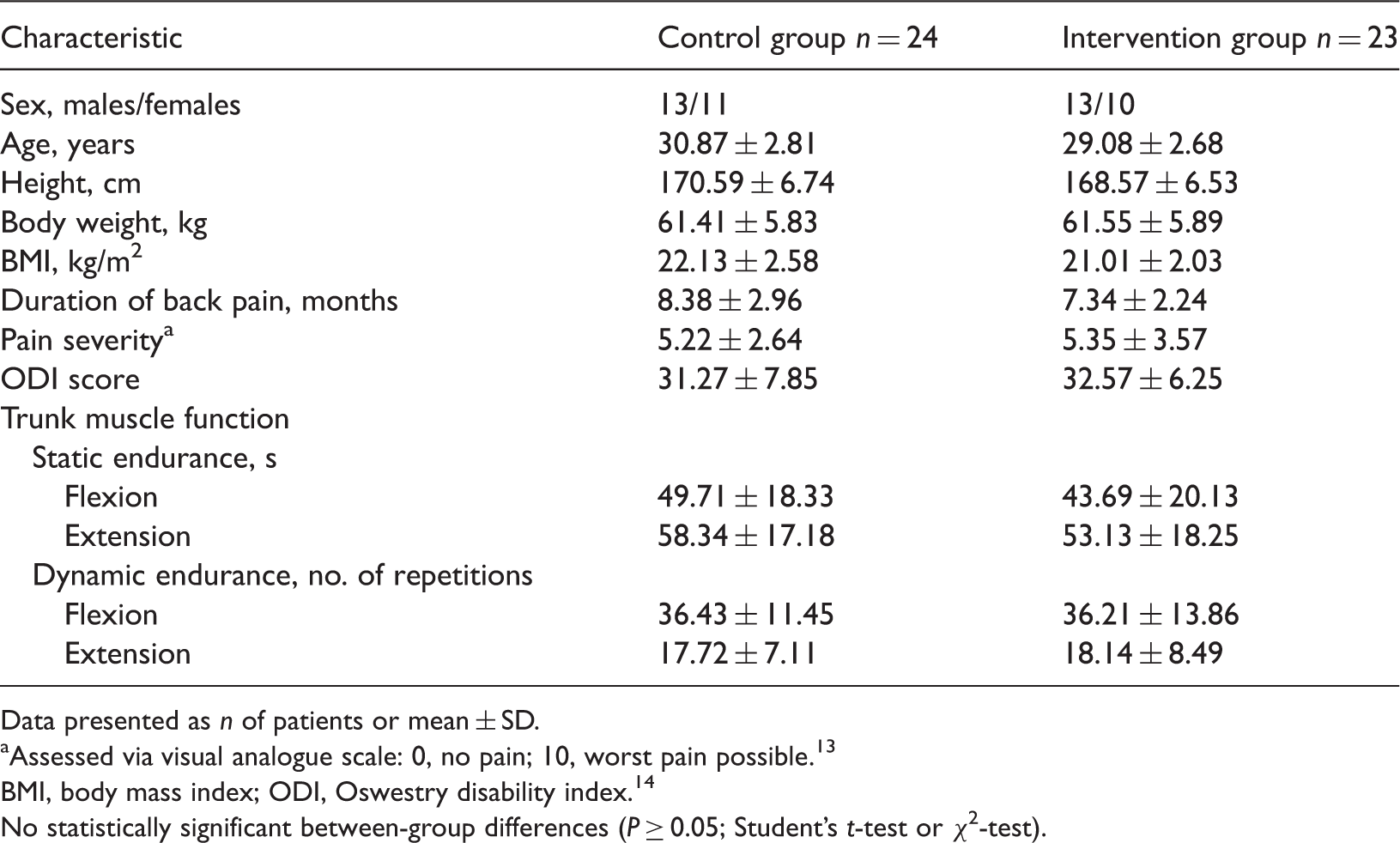
In total, 50 patients were randomized (n = 25 per group). A flow chart indicating the recruitment and treatment allocations of the patients is shown in Figure 1. At the end of the 24-week treatment period, outcome data were available for 23/25 patients in the intervention group and 24/25 in the control group. Baseline demographic and clinical characteristics of the patients are shown in Table 1. There were no statistically significant between-group differences in any characteristic at baseline.
Flow chart indicating recruitment, randomization and follow-up of patients with chronic low back pain included in a study to compare the effects of 24 weeks of routine treatment (ultrasonography, short wave diathermy and lumbar strengthening exercises; control group) or combination routine treatment and pelvic floor muscle exercise (intervention group) on back pain, disability and function. Baseline demographic and clinical characteristics of patients with chronic low back pain included in a study to compare the effects of 24 weeks of routine treatment (ultrasonography, short wave diathermy and lumbar strengthening exercises; control group) or combination routine treatment and pelvic floor muscle exercise (intervention group) on back pain, disability and function. Data presented as n of patients or mean ± SD. Assessed via visual analogue scale: 0, no pain; 10, worst pain possible.
13
BMI, body mass index; ODI, Oswestry disability index.
14
No statistically significant between-group differences (P ≥ 0.05; Student’s t-test or χ2-test).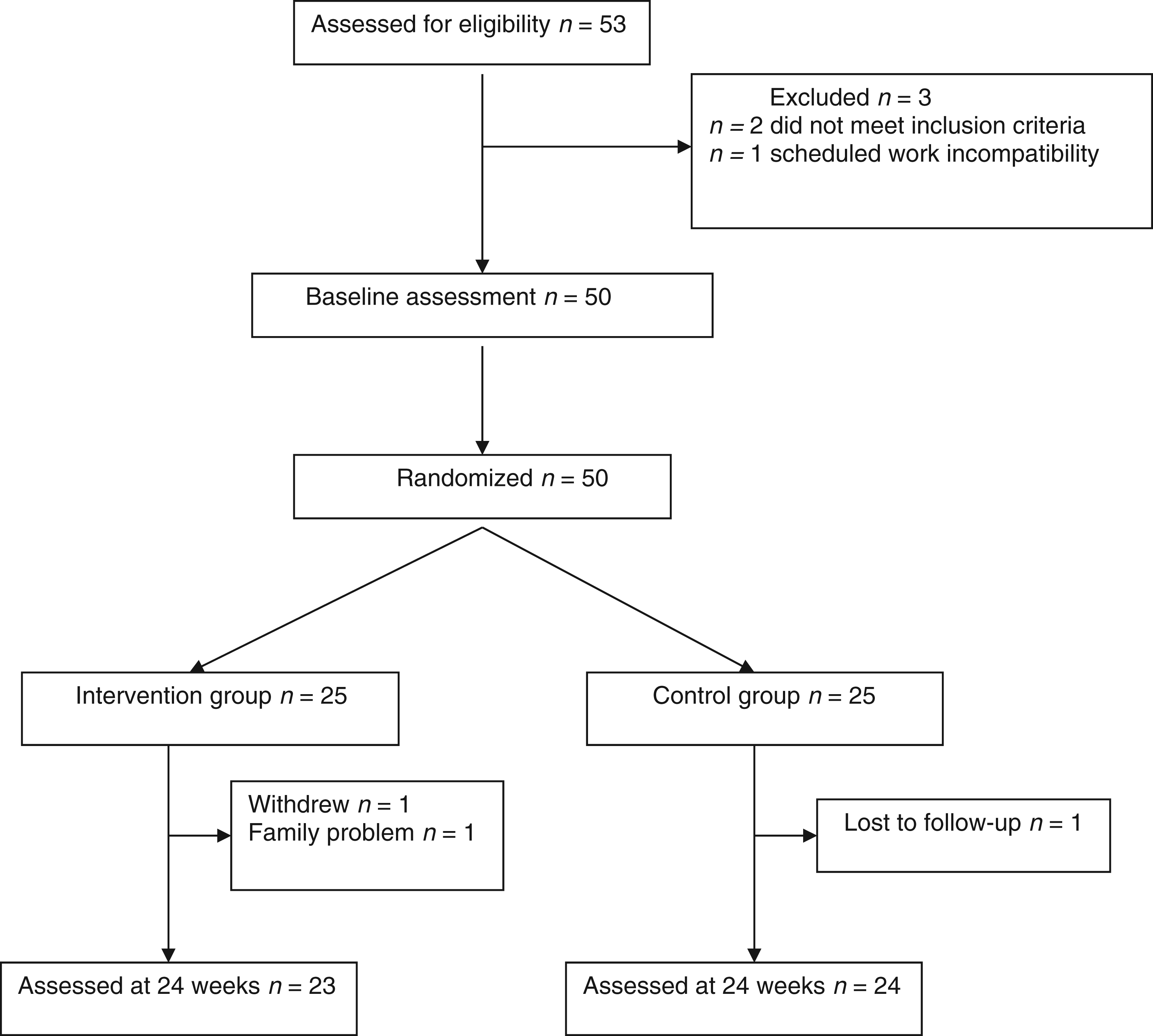
Back pain, disability and functional parameters in patients with chronic low back pain after completion of a 24-week treatment programme, comprising routine treatment (ultrasonography, short wave diathermy and lumbar strengthening exercises; control group) or combination routine treatment and pelvic floor muscle exercise (intervention group).

Data presented as mean ± SD.
ODI, Oswestry disability index; 14 NS, not statistically significant (P ≥ 0.05).
Two-way analysis of variance.
Assessed via visual analogue scale: 0, no pain; 10, worst pain possible. 13
Discussion
Pelvic floor muscles make up a large part of the body's core, 18 which is the foundation for all movement, balance, stability and flexibility. 19 The pelvic floor muscle exercise protocol used in the present study was designed to coactivate superficial and deep core muscles, and resulted in significantly better improvements in pain and ODI score compared with routine treatment alone. Back function parameters were improved over baseline in both treatment groups, with no significant between-group differences. These results are consistent with the findings of others, who demonstrated the superiority of a core strengthening programme to simple strengthening exercises for chronic low back pain. 7 Others have suggested, however, that core stability exercises do not provide any benefit over conventional physiotherapy exercises in terms of pain or disability reduction. 20 A pelvic floor muscle exercise programme comprising 6 contraction cycles/day for 12 weeks was found to provide no additional improvement in pain or ODI score compared with routine treatment. 21 The more intense training and longer treatment period (a minimum of 25 contraction cycles/day for 24 weeks) may explain the significant improvements in pain and disability seen in the present study. Improving the biomechanical characteristics of muscles in patients with low back pain may require long-term pelvic floor muscle training. Studies have shown that a training period of ≥20 weeks is required for patients with persistent pelvic girdle pain. 22
The current study had several limitations. First, this was a single-centre study and the sample size was too small to draw any firm conclusions. Secondly, some patients did not perform the pelvic floor muscle exercises correctly. Finally, as the study population included patients with nonspecific low back pain, it is not possible to generalize these findings to those with low back pain of specific cause.
In conclusion, pelvic floor exercises in combination with routine treatment provide significant benefits in terms of pain relief and disability over routine treatment alone. Further, larger-scale studies with long-term follow-up are required before these findings can be applied to a wider patient cohort.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This research was supported by grants from the Science and Technology Development Fund of Shanghai Pudong (PKJ2008-Y39), the Program of Shanghai Pudong Subject Chief Scientist (PWRd2010-06) and the Science and Technology Development Fund of Shanghai Pudong (PKJ2011-Y05).