
Abstract
Study design
Systematic Review
Objective
To evaluate the efficacy of available treatment options for patients with persistent coccydynia through a systematic review.
Methods
Original peer-reviewed publications on treatment for coccydynia were identified using Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines by performing a literature search of relevant databases, from their inception to January 17, 2020, combined with other sources. Data on extracted treatment outcome was pooled based on treatment categories to allow for meta-analysis. All outcomes relevant to the treatment efficacy of coccydynia were extracted. No single measure of outcome was consistently present among the included studies. Numeric Rating Scale, (NRS, 0–10) for pain was used as the primary outcome measure. Studies with treatment outcome on adult patients with chronic primary coccydynia were considered eligible.
Results
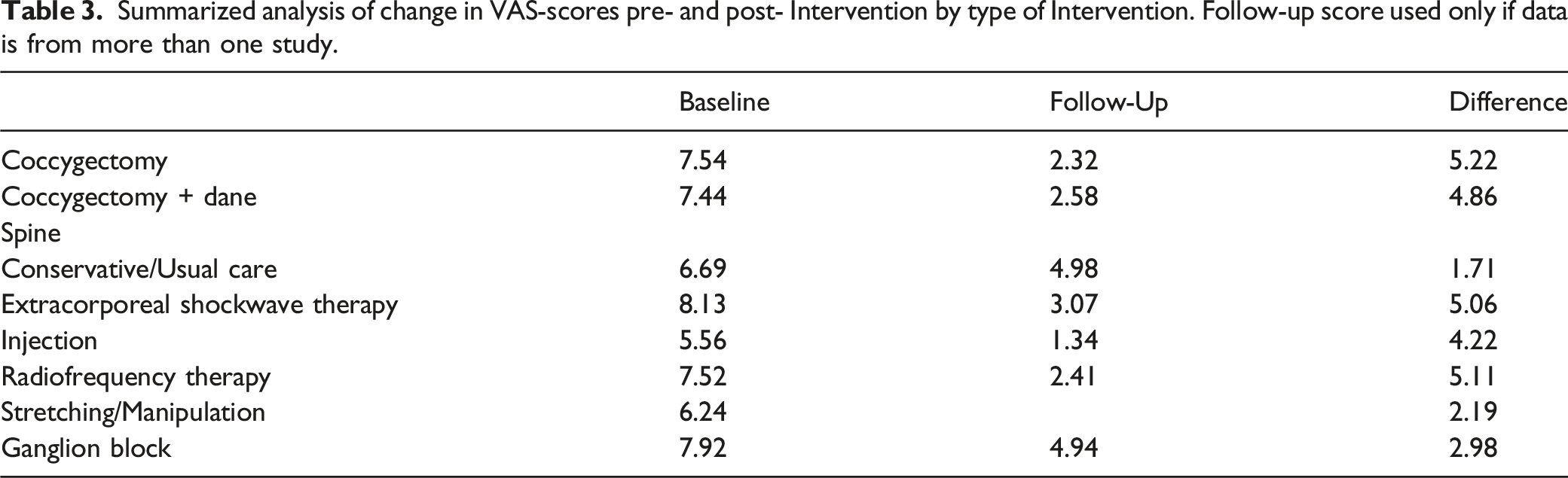
A total of 1980 patients across 64 studies were identified: five randomized controlled trials, one experimental study, one quasi-experimental study, 11 prospective observational studies, 45 retrospective studies and unpublished data from the DaneSpine registry. The greatest improvement in pain was achieved by patients who underwent radiofrequency therapy (RFT, mean Visual Analog Scale (VAS) decreased by 5.11 cm). A similar mean improvement was achieved from Extracorporeal Shockwave Therapy (ESWT, 5.06), Coccygectomy (4.86) and Injection (4.22). Although improved, the mean change was less for those who received Ganglion block (2.98), Stretching/Manipulation (2.19) and Conservative/Usual Care (1.69).
Conclusion
This study highlights the progressive nature of treatment for coccydynia, starting with noninvasive methods before considering coccygectomy. Non-surgical management provides pain relief for many patients. Coccygectomy is by far the most thoroughly investigated treatment option and may be beneficial for refractory cases. Future randomized controlled trials should be conducted with an aim to compare the efficacy of interventional therapies amongst each other and to coccygectomy.
Introduction
Coccydynia is pain located in the coccygeal bone or the surrounding tissues. 1 Coccydynia is a relatively rare condition, occurring more frequently in females and in all ages.1-3 The anatomy of the os coccygis varies. It consists of a number of rudimentary vertebrae ranging from 3 to 5 and varies in regard to the incidence of segmental fusion. The positioning of the coccyx has been described and classified into 4 types by Postacchini and Massobrio. 4 Coccydynia is most frequently associated with single-axis traumatic injury, childbirth, obesity, and rapid weight-loss related to gastric by-pass surgery.5,6 There are several etiologies to the occurrence of secondary coccydynia, such as cancer pain, infection, or iatrogenic. 7 Previous surgery in the area can lead to inflammation, formation of granulation tissue, adhesions, and possibly a change in elasticity of the tissue surrounding the os coccygis, which, over the course of time, can lead to secondary coccydynia. Extracoccygeal disorders may also manifest as coccydynia. Examples of such are pilonidal cysts, perianal abscesses, hemorrhoids, and diseases of the pelvic organs as well as disorders of the lumbosacral spine, sacroiliac joints, piriformis muscle, and the sacrum.8,9
Coccydynia presents most frequently in an acute form with mild symptoms, typically resolving with no treatment within weeks to months. 5 When pain does not resolve, treatment is primarily expectant and aimed at symptom management, as pain spontaneously improves in up to 90% of patients receiving conservative treatment. 10 However, for some patients the pain persists and remains refractory to initial conservative treatment. 5 Chronic coccydynia is a condition for which there is limited understanding of the pathology and the effectiveness of different treatments. Patients may experience a marked loss in quality of life and difficulty in performing everyday activities. 5 Sitting is often conspicuously painful in patients with coccydynia, but can be exaggerated with sexual intercourse, with some patients also having difficulty defecating. 3
There are various treatment options available for symptom relief, including conservative, pharmacological, and surgical treatment. Patients are advised to sit on a U-shaped cushion or a modified wedge-shaped cushion.10,11 Other options are nonsteroidal anti-inflammatory drugs (NSAIDs), massage, stretching, physical therapy,11,12,13 or interventional treatment, such as steroid injections, radiofrequency treatments (RFT), extracorporeal shockwave therapy (ESWT), and ganglion blocks.14-19 Surgical intervention, including both partial and complete resection of the coccyx, is typically an option for patients with coccygeal pain refractory to other therapeutic options.20-23
Currently there are no official clinical guidelines regarding the treatment of coccydynia. With this systematic review the authors aim to contribute to the development of clinical guidelines for the treatment of coccydynia.
The study objective is to evaluate the efficacy of current available treatments for coccydynia in adults, by systematically reviewing existing original peer-reviewed publications according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.
Materials and Methods
Protocol and Registration
This systematic review was generated following the PRISMA guidelines. A completed copy of the PRISMA checklist is provided (Supplementary Data Content 1, SDC 1).
Search, Information Sources, Eligibility Criteria, and Study Selection
A systematic literature search was conducted on January 17, 2020, in EMBASE.com, PubMed.com, Scopus, and Web of Science bibliographic databases from their inception to the search date. The search was conducted using index-words related to the coccyx and coccydynia. Index-words together with the full search strategy are attached (SDC 2). An experienced librarian, affiliated with the Faculty of Health at Aarhus University, was consulted for guidance in designing the search. A search for published studies and Epubs ahead of print in journals with relevance to spine surgery was also conducted. Finally, reference lists and citations of the included studies were screened in order to identify other relevant papers, and a cohort of non-published data from DaneSpine was included in the review. 24 The inclusion and exclusion criteria were created based on eligibility (SDC 3).
Inclusion Criteria Were
(1) Publications of original peer-reviewed randomized controlled trials, cohort studies, or case-series, available in full text. (2) Papers in English, Danish, Norwegian, Swedish, Serbian, Croatian, Bosnian, and Spanish. (3) Studies addressing treatment of patients with coccydynia with any available treatment option.
Exclusion Criteria Were
(1) Animal studies and studies addressing evaluation of technical equipment. (2) Studies including patients less than 16 years of age. (3) Studies without treatment outcome (e.g., studies of etiology). (4) Acute coccydynia or patients with coccydynia with a duration less than 2 months. (5) Studies solely concerning secondary coccydynia as a complication of another condition (e.g., cancer-derived pain and infectious-derived pain). (6) Systematic reviews, meta-analyses, opinions, commentaries, and studies involving less than six cases.
Identified articles were screened for duplicates, using both EndNote and Covidence. The screening was done by two authors independently using Covidence, involving a third author in case of disagreement. Articles were initially screened based on title and abstract, followed by a full text screening. In cases where initial screening could not be performed due to a missing abstract, the full text article was obtained.
Risk of Bias in Individual Studies
To assess article quality and bias, two authors independently evaluated all included articles, followed by an attainment of consensus. Cochrane Risk of Bias Tool was used to assess the presence and extent of bias in Randomized Controlled Trials (RCTs). 25 Included observational studies were scored using Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist. 26
Data Collection Process and Data Items
Data extraction was performed independently in duplicate and compared when completed. During the process of data extraction, all suitable measures of treatment effect were initially extracted due to the largely heterogeneous sample of included studies. The primary outcome measure for evaluating the efficacy of the different treatments was the Visual Analog Scale (VAS) pain scores at last follow-up compared to baseline. Secondary outcome measures consistent throughout the included studies were complications and qualitative measures of outcome, that is, “improved,” “no change,” “worse.” The authors recorded the proportions of these qualitative measures by consensus, considering that some studies used a different terminology, that is, “better,” “unchanged,” “worse.” It was decided to compile the different qualitative measures of outcome into “successful, moderate, or poor outcome” as this was deemed the most representative. In addition, two continuous measures of pain before and after treatment were established as pre- and post-Numeric Rating Scale ranging from 0 to 10. It was decided to interpret several different measures of pain scores, such as Visual Analog Scale (VAS), Pain Analogue Scale (PAS), and Numeric Pain Score (NPS) to the Numeric Rating Scale (NRS). Studies that reported pain using the VAS ranging from 0 to 100 were rescored to a 0 to 10 scale.
Data Analysis
The included studies were divided into groups based on treatment strategies. All analyses were performed using SPSS V26.0 (IBM, Armonk, New York). Data was analyzed using weighted pooled averages. Mean difference in pain scores from baseline to last follow-up were used as measure of an intervention’s efficacy.
The current review was conducted in accordance with the protocol and is registered in PROSPERO (PROSPERO ID: CRD42020166379).
Results
2149 references were identified by applying our search string (SDC 2). After removal of duplicates, a total of 930 references were added to title/abstract screening. Sixty three studies were included for data extraction.1,9-13,15-21,23,27-75 No articles were included through the search in relevant journals, nor through reference and citation screening (see flowchart of literature screening, Figure 1). Prisma Flowchart.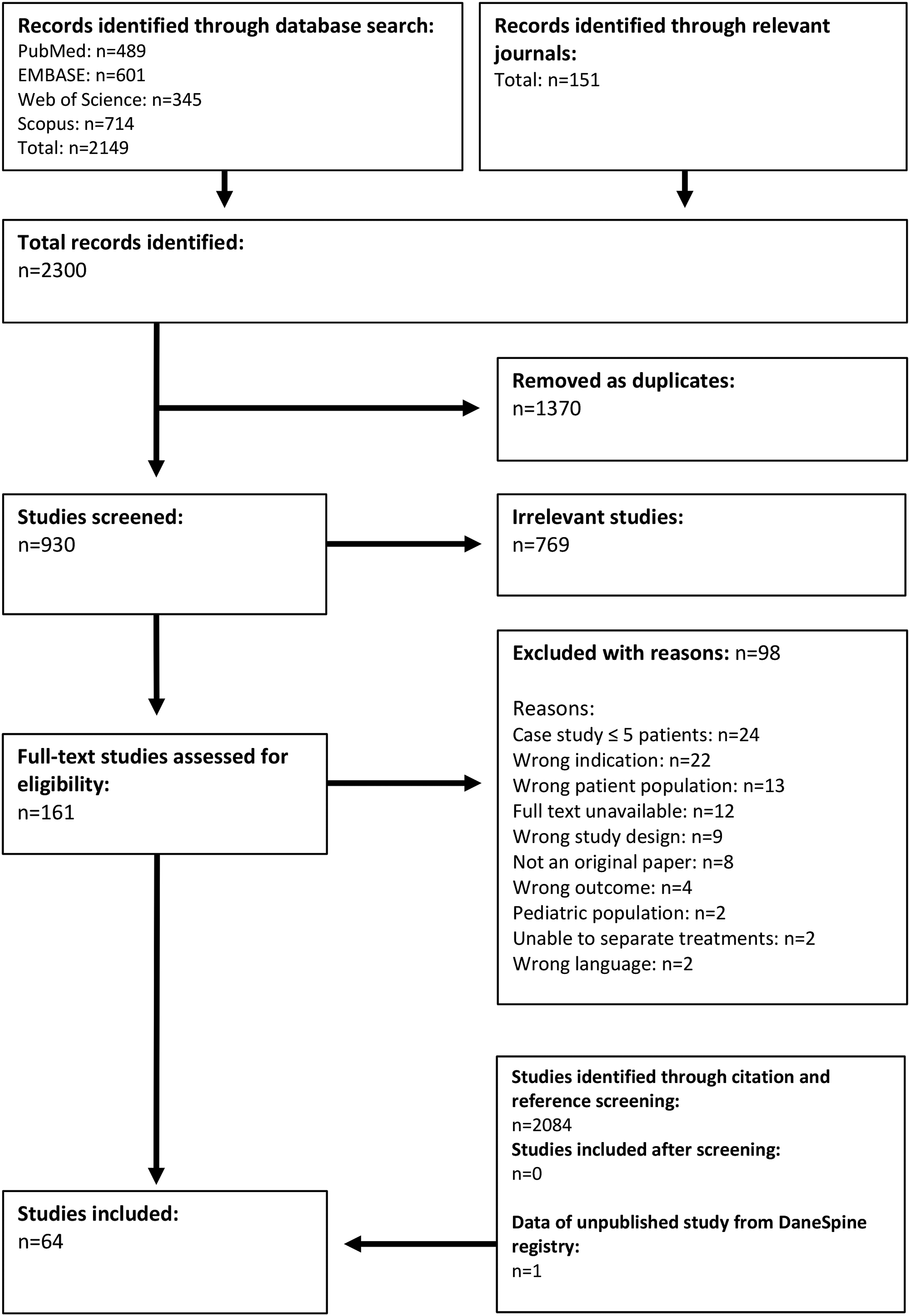
Studies Included for Analysis in Systematic Review.
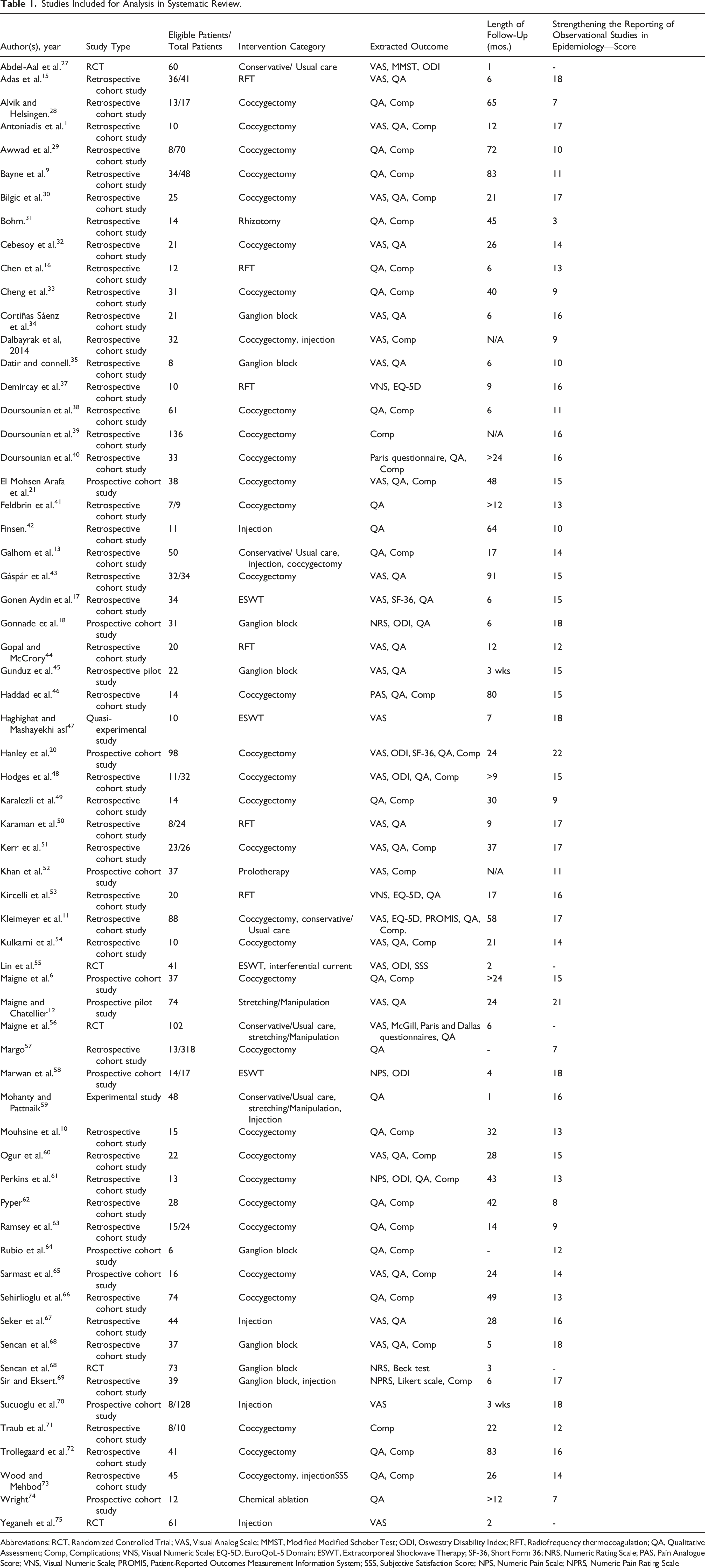
Abbreviations: RCT, Randomized Controlled Trial; VAS, Visual Analog Scale; MMST, Modified Modified Schober Test; ODI, Oswestry Disability Index; RFT, Radiofrequency thermocoagulation; QA, Qualitative Assessment; Comp, Complications; VNS, Visual Numeric Scale; EQ-5D, EuroQoL-5 Domain; ESWT, Extracorporeal Shockwave Therapy; SF-36, Short Form 36; NRS, Numeric Rating Scale; PAS, Pain Analogue Score; VNS, Visual Numeric Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; SSS, Subjective Satisfaction Score; NPS, Numeric Pain Scale; NPRS, Numeric Pain Rating Scale.
Summary of Pooled Data Available for Extraction from Included Studies by Type of Intervention.
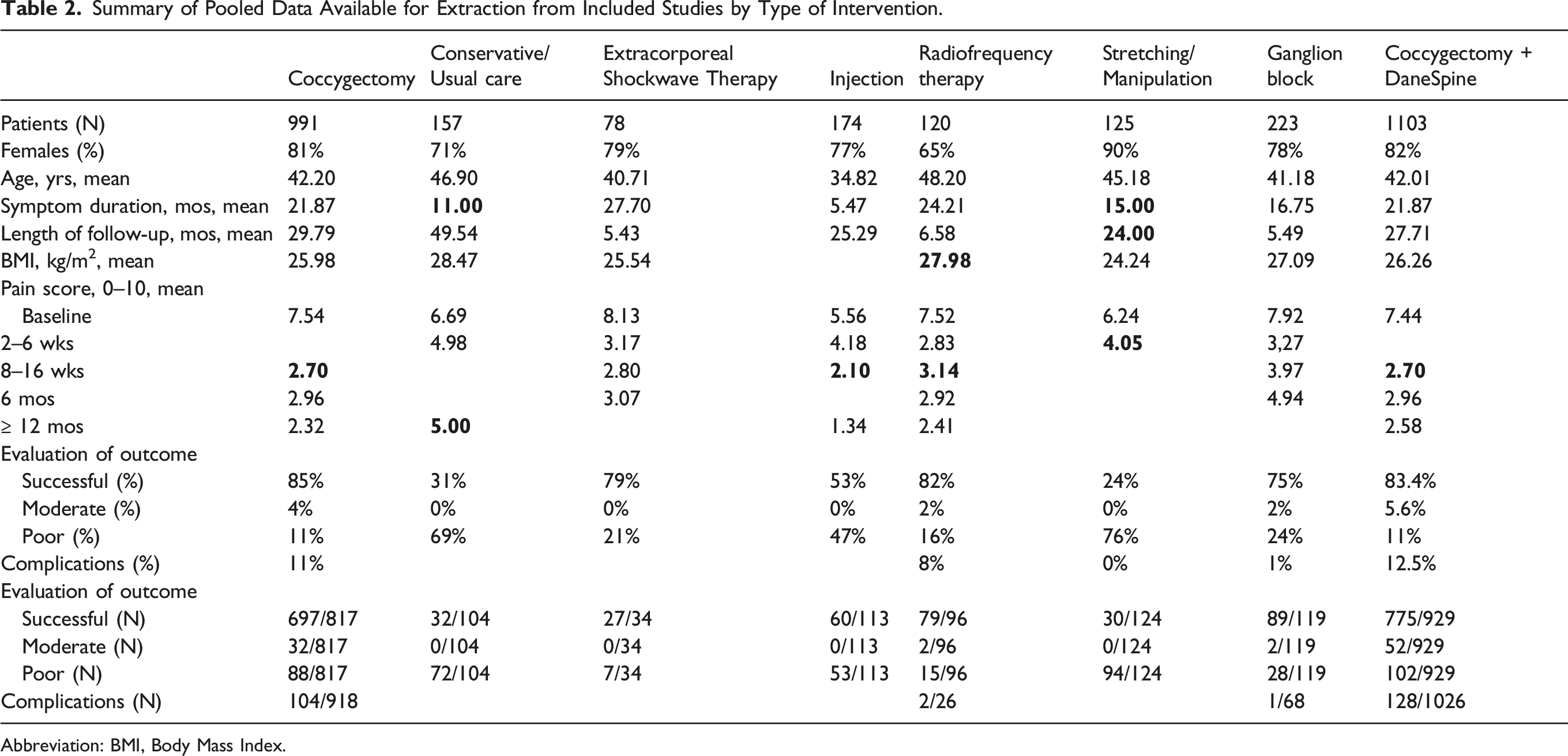
Abbreviation: BMI, Body Mass Index.
Summarized analysis of change in VAS-scores pre- and post- Intervention by type of Intervention. Follow-up score used only if data is from more than one study.
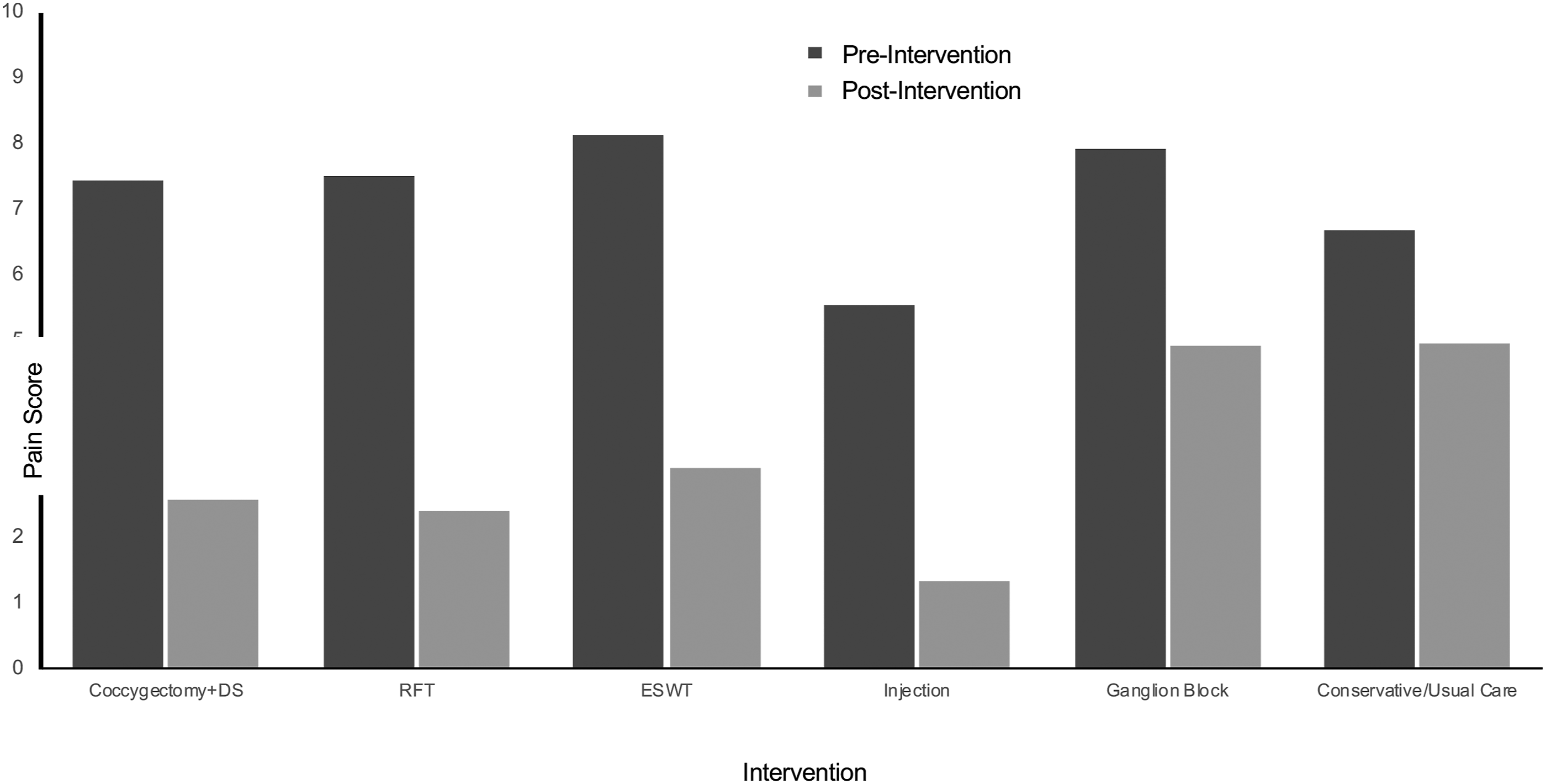
Change in NRS-scores Pre- and Post-Intervention by Type of intervention. Abbreviations: RFT, Radiofrequency thermocoagulation; ESWT, Extracorporeal Shock Wave Therapy.
Discussion
This is the most wide-ranging systematic review on treatment modalities for coccydynia and the first systematic review on the topic.
Our main findings suggested overall good outcomes in most of the treatment modalities investigated. The largest patient-reported pain reductions were observed in ESWT, RFT, and coccygectomy. Usual care and stretching/manipulation showed the least reduction in pain. Ganglion blocks showed a modest effect for a shorter period. Coccygectomy, RFT, and ESWT likewise presented with the highest success-rates, respectively. Coccygectomy is by far the most widely represented treatment-modality in terms of eligible studies and patients included for analysis. In terms of complication rates, all treatment modalities showed very little or no complications, except for coccygectomy which showed an overall high complication-rate. Complications were almost exclusively infections, due to the anatomical area of the surgical site, and could be treated with additional antibiotics.
The main limitation to this systematic review is the lack of high-quality studies, specifically randomized clinical trials with adequate sample size on the subject. The validity of any analysis is dependent on the quantity and quality of included evidence, which varies widely between the included studies. The limited number of randomized controlled trials, the small sample sizes within the studies and differences in the type of treatments being compared for studies conducted in this field of research proved inadequate for inclusion in the main analysis as no treatment strategies could be pooled. Since the majority of included studies are observational there is inherent bias. Potential bias as a consequence of loss to follow-up and patient selection is present in each study and will inevitably impact the present results. The STROBE score will guide the reader to evaluate the quality of the articles included and the degree of impact this will have on the results. As the investigated interventions were of immense heterogeneity, we considered it too excessive to weight the results of individual studies by their STROBE score. All non-randomized studies of intervention (NRSI) were assessed using STROBE for consistency because of the differences in study design.
No comparator to the interventions of interest was noted in the eligibility criteria, due to the sequential nature of the treatment options for coccydynia. Steroid blocks are typically not applied without prior unresponsive attempts at conservative treatment, just as surgical intervention is not performed without prior unresponsive attempts of interventional treatment approach. Furthermore, complete post-operative remission from pain may take months or years after initiation of treatment, why the short-dated follow-up period of some grouped therapies compromises comparability in efficacy across treatments. Due to the study design, the analysis of efficacy does not consider subgroups of patients, for example,, traumatic or idiopathic etiology, which could impact treatment outcome.
As our preliminary research suggested that the amount of studies on treatment options to coccydynia was sparse, our search strategy was constructed without restriction to publication year and without restriction to any types of treatment.
Moreover, we lowered the specificity on outcome measures to avoid exclusion of studies assessing less investigated treatment options and studies not using validated score-systems. This weakens the quality of the overall quantitative comparison in efficacy, as a trade-off to be able to report on efficacy in the largest possible number of patients. In order to include as much data as possible, outcome on eligible patients from mixed patient cohorts was extracted, if data was separable from the remaining study sample. This compromised the availability of patient demographics in some instances.
We also included an unpublished set of consecutively sampled data on the efficacy of coccygectomy with relevance to the review. The unpublished data was included due to the quantitative added value, simultaneous acknowledging the lack of peer-review.
Even though RFT, ESWT, and coccygectomy present with very similar results in the analysis, the validity of our findings regarding RFT and ESWT should be considered in relation to the sparse amount of evidence, whereas coccygectomy is the single most investigated treatment option. Although promising treatments, we consider the basis of the current analysis inadequate for comparing the long-term efficacy of RFT and ESWT to that of coccygectomy. Despite presenting with the best validated outcome results, surgical treatment should be reserved to a select subset of patients, unresponsive to all available conservative treatment, and interventional treatment options, due to the potential risk of surgical complications. Future randomized controlled trials should be conducted with an aim to compare the efficacy of interventional therapies amongst each other and to coccygectomy.
Conclusion
The results must be interpreted in the context of the patients included for review, which is why noninvasive treatment despite its modest effect should not be discarded as first-line treatment. A sequential nature of treatment stands out all across the literature, and thus, interventional therapy is preferable to invasive treatment as the former often provides pain relief for many patients, but without the evident risk of complications associated with the latter. Coccygectomy is by far the most thoroughly investigated treatment option and may be beneficial for refractory cases to less invasive procedures. High-quality studies in future may obtain the same or completely different results as seen in this systematic review. Future randomized controlled trials should be conducted with an aim to compare the efficacy of interventional therapies amongst each other and to coccygectomy.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211065389 – Supplemental Material for Coccydynia—The Efficacy of Available Treatment Options: A Systematic Review
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211065389 for Coccydynia—The Efficacy of Available Treatment Options: A Systematic Review by Gustav Ø. Andersen, Stefan Milosevic, Mads M. Jensen, Mikkel Ø. Andersen, Ane Simony, Mikkel M. Rasmussen and Leah Carreon in Global Spine Journal
Supplemental Material
sj-pdf-2-gsj-10.1177_21925682211065389 – Supplemental Material for Coccydynia—The Efficacy of Available Treatment Options: A Systematic Review
Supplemental Material, sj-pdf-2-gsj-10.1177_21925682211065389 for Coccydynia—The Efficacy of Available Treatment Options: A Systematic Review by Gustav Ø. Andersen, Stefan Milosevic, Mads M. Jensen, Mikkel Ø. Andersen, Ane Simony, Mikkel M. Rasmussen and Leah Carreon in Global Spine Journal
Supplemental Material
sj-pdf-3-gsj-10.1177_21925682211065389 – Supplemental Material for Coccydynia—The Efficacy of Available Treatment Options: A Systematic Review
Supplemental Material, sj-pdf-3-gsj-10.1177_21925682211065389 for Coccydynia—The Efficacy of Available Treatment Options: A Systematic Review by Gustav Ø. Andersen, Stefan Milosevic, Mads M. Jensen, Mikkel Ø. Andersen, Ane Simony, Mikkel M. Rasmussen and Leah Carreon in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Data use approval was acquired from the Danish Data Protection Agency ref nr: 16/1586. The study was reviewed and approved by the Research Board of the Center for Spine Surgery and Research at Lillebaelt Hospital.
Informed Consent
Subjects provided consent for use of their data at the time patients completed the questionnaires and were enrolled in DaneSpine.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.