
Abstract
Study Design
Retrospective cohort study.
Objectives
Laminoplasty (LAMP) is one of the effective methods to successfully achieve surgical decompression in patients with degenerative cervical myelopathy (DCM). However, little evidence exists regarding the perioperative complications in LAMP for patients with ossification of the longitudinal ligament (OPLL) compared with cervical spondylotic myelopathy (CSM). We aimed to investigate the perioperative complication rates and medical costs of DCM, including OPLL and CSM patients who underwent LAMP using a large national inpatient database.
Methods
This study identified patients who underwent LAMP for OPLL and CSM from 2010 to 2016 using the Japanese Diagnosis Procedure Combination database. We compared the incidence of perioperative complications (systemic and local), reoperation rates, medical costs during hospitalization, and mortality were between the OPLL and CSM groups after propensity score matching.
Results
This study included 22,714 patients (OPLL: 7485 patients, CSM: 15,229 patients). Consequently, 7169 pairs were matched. More perioperative systemic complications were detected in the OPLL group (one complication: 9.1% vs 7.7%; P = .002), especially for pneumonia (.5% vs .2%; P = .001) and dysphagia (.5% vs .2%; P = .004). The local complication rate was also higher in the OPLL group (paralysis: 1.1% vs .6%, P = .006; spinal fluid leakage: .4% vs .1%, P = .002). The hospitalization costs were approximately $2300 higher ($19,024 vs $16,770; P < .001) in the OPLL group.
Conclusions
More perioperative complications and higher medical costs were noted in patients with OPLL than in patients with CSM who underwent LAMP.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) due to nontraumatic and age-related degeneration is a common spinal cord disorder in middle-aged and older patients. 1 The main diseases are ossification of the posterior longitudinal ligament (OPLL) and cervical spondylotic myelopathy (CSM), although a variety of conditions can cause DCM. 2 OPLL is a disease in which the endochondral ossification of the posterior longitudinal ligament progresses to cause spinal cord compression and myelopathy 3 and is also associated with high body mass index and metabolic diseases, such as diabetes. 4 Moreover, CSM is a condition in which degenerative changes caused by degeneration of the disks, changes in osteophytes, and enlargement of the yellow ligament cause narrowing of the spinal canal, resulting in spinal cord compression and neurological deterioration. 5 Thus, although they commonly cause compressive spinal cord disorders, the characteristics of the disease are different between OPLL and CSM.
Decompression surgeries, including anterior and posterior approaches, are generally used for treating cervical myelopathy. 6 Laminoplasty (LAMP) is one of the eminent procedures for simple posterior decompression of cervical myelopathy. 7 Although LAMP has some limitations, such as postoperative neck pain and stiffness, 8 several studies have reported that it effectively improves neurological disturbance and patient activity levels in individuals with both OPLL and CSM.9-13
Surgeries for cervical OPLL are generally high-risk even in cases treated with posterior only approaches, and the occurrence of surgical complications is not rare. 14 Previous studies have compared neurological improvement after LAMP between patients with OPLL and CSM. However, few studies focused on the difference between OPLL and CSM in terms of surgical complications after LAMP. Thus, this study aimed to examine the details of perioperative complications, including systemic and local LAMP complications for cervical OPLL and CSM using a national inpatient database, and compare the incidence of complications and medical costs between the matched OPLL and CSM patient groups.
Materials and Methods
Informed Consent and Ethics
Informed consent for individual patients has been deemed exempt from requirement because the database in current study was completely anonymized. The application of all data in this study was approved by the ethics committee of the Tokyo Medical and Dental University (M2000-788-22).
Data Extraction
All data in this study was collected from the Diagnosis Procedure Combination (DPC) database, a large national inpatient database in Japan.15,16 Patients who were hospitalized for DCM, OPLL (International Classification of Diseases, Tenth Revision, ICD-10 code: M4882), or CSM (M4712) as a chief diagnosis and who underwent LAMP (Japanese original operation K-code: K142-6) from April 1, 2010 to March 31, 2016 were identified. Furthermore, patients who were diagnosed with cervical disk herniation (M500-502), cervical spondylotic radiculopathy (M4722), cervical spondylotic amyotrophy (G128), and spinal cord injury (S141) were excluded from this study. Patients who underwent laminectomy were also excluded.
The DPC database recorded age, gender, body mass index (BMI), smoking status, admission type (scheduled or unscheduled), emergency transport, hospital type (academic or nonacademic), activities of daily living (ADL) score for admission and discharge, preoperative comorbidities and postoperative complications diagnoses denoted to the ICD-10 codes, surgical procedures, reoperation for postoperative complications, blood transfusions, medical costs, and in-hospital mortality.
Variables and Outcomes
Patients were divided into 2 groups based on whether their preoperative diagnosis was OPLL or CSM. The parameters obtained were age, gender, BMI, smoking status, type of admission, emergency transport, hospital type, ADL score for admission and discharge, preoperative complications, perioperative complications (systemic and local), reoperation, blood transfusion, and medical costs during hospitalization.
Detailed information on preoperative comorbidities and perioperative complications was extracted from the database. Preoperative comorbidities include diabetes mellitus (ICD-10 code; E10-14), cardiovascular disease (I48, 110, 200, 201, 208–214, 219–221, 228, 229, 238, 500, 501, and 509), cerebrovascular disease (I614, 619, and I630–639), respiratory disease (J13, 14, 150–159, 180–182, 188, 189, 441, 448, and 449), renal failure (N17–19, 289, and I120), hepatic failure (K704, 711, 719, 720, 729, and 769), gastric ulcer and hemorrhage (K250–270, 279, and 922), malignancy (C00–97), rheumatoid arthritis (M690–698), and osteoporosis (M800–805, 808–816, 818, and 819). In addition, perioperative systemic and local complications include systemic complications [i.e., cardiovascular disease, cerebrovascular disease, respiratory failure, pneumonia, dysphagia (K918 and R13), renal failure, hepatic failure, gastric ulcer and hemorrhage, deep venous thrombosis (I801, 802, and 828), pulmonary embolism (I269), sepsis (A394, 400–403, 409-415, 418, and 419), and delirium (F050, 051, and 059)], local complications [i.e., surgical site infection (T793 and 814), paralysis (G823–825, 831, and 832), meningitis (G001–003, 008–009, 039, A390, and 392), spinal fluid leakage (G960 and 961), and hematoma (S064, 141, 241, 341, and T093)], and reoperations for perioperative complications [treatment for wound trouble (K-code: K000) and debridement (K002)]. The medical costs during hospitalization were compared between patients with OPLL and CSM and further analyzed for each group with and without complications (systemic, local, and total) after propensity score matching.
Statistics
Univariate analysis was performed between the 2 groups (OPLL and CSM groups) with crude data. Fisher’s exact test and the chi-square test were used to compare categorical variables, and the student’s t test was used to compare continuous variables. One-to-one propensity score matching17-19 was performed after crude data analysis, and the same analysis was performed on eligible patients only after matching.
The procedure for propensity score matching is explained below. A propensity score is calculated by performing a logistic analysis using explanatory variables for only those items preoperatively known. The explanatory variables with the logistic regression analysis were age, gender, BMI, smoking status, admission type, emergency transport, hospital type, ADL score for admission, and preoperative comorbidities (diabetes mellitus, cardiovascular disease, cerebrovascular disease, respiratory disease, renal failure, hepatic failure, gastric ulcer and hemorrhage, malignancy, rheumatoid arthritis, and osteoporosis). Patients diagnosed with OPLL were matched with those diagnosed with CSM in terms of the propensity score using calipers with a width <.2 and the one-to-one nearest neighbor-matching method. Thus, a 1:1 pair with aligned patient backgrounds in the OPLL and CSM groups is formed, resulting in a selection bias-adjusted cohort. All statistical analyses were executed using Stata IC version 16 (StataCorp, College Station, TX, USA) with P values <.05 considered statistically significant.
Results
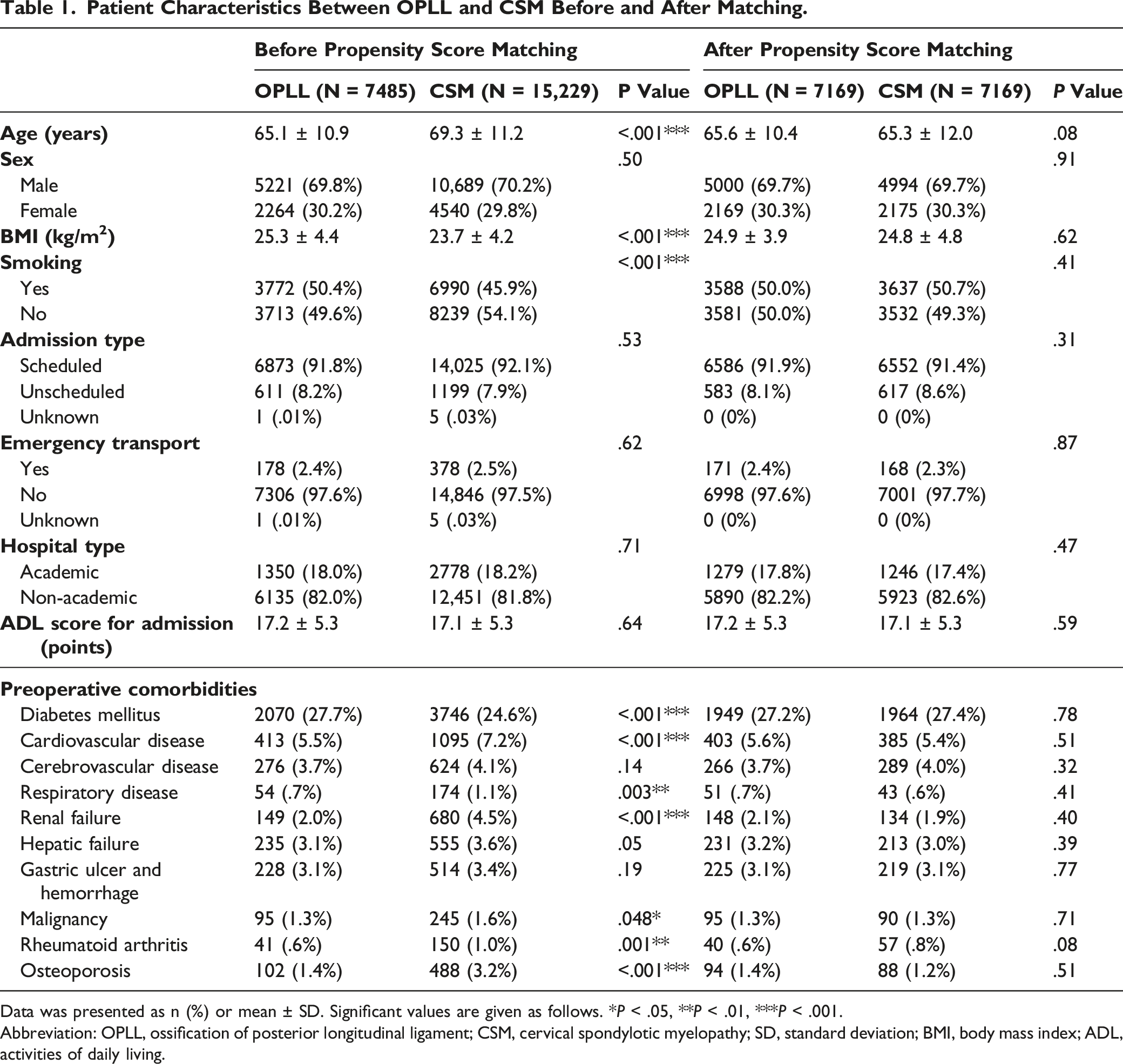
Data was presented as n (%) or mean ± SD. Significant values are given as follows. *P < .05, **P < .01, ***P < .001.
Abbreviation: OPLL, ossification of posterior longitudinal ligament; CSM, cervical spondylotic myelopathy; SD, standard deviation; BMI, body mass index; ADL, activities of daily living.
Systemic Complications and Blood Transfusion After Propensity Score Matching.
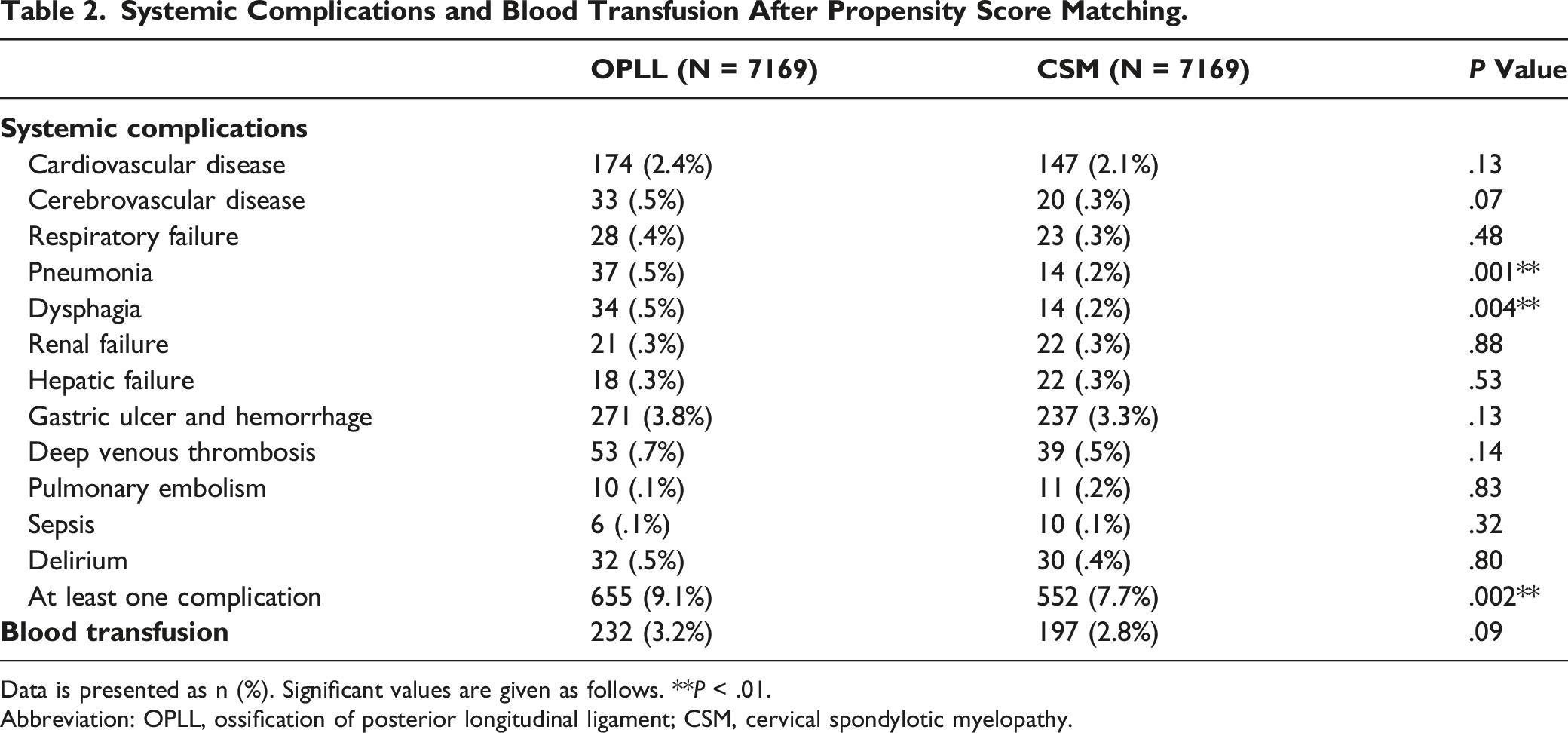
Data is presented as n (%). Significant values are given as follows. **P < .01.
Abbreviation: OPLL, ossification of posterior longitudinal ligament; CSM, cervical spondylotic myelopathy.
Local Complications and Reoperation After Propensity score Matching.
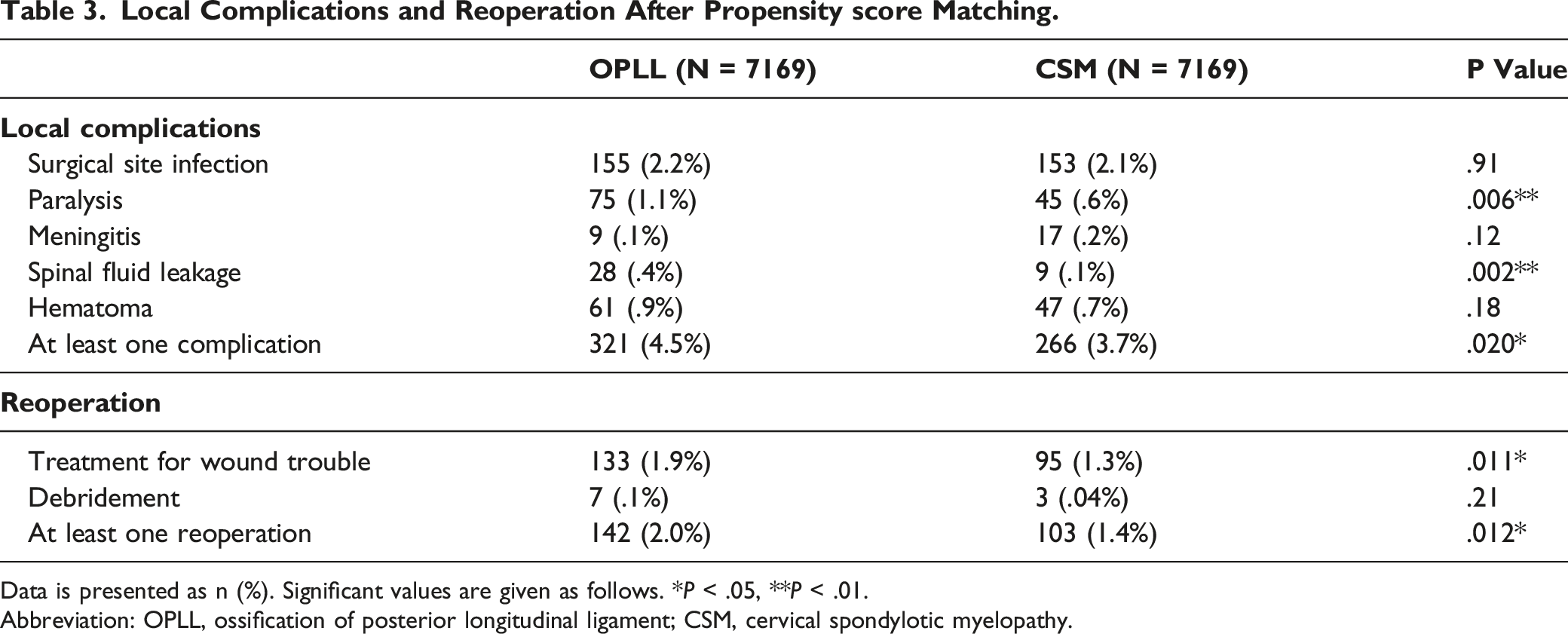
Data is presented as n (%). Significant values are given as follows. *P < .05, **P < .01.
Abbreviation: OPLL, ossification of posterior longitudinal ligament; CSM, cervical spondylotic myelopathy.

Data is presented as n (%) or mean ± SD. Significant values are given as follows. ***P < .001.
Abbreviations: OPLL, ossification of posterior longitudinal ligament; CSM, cervical spondylotic myelopathy; SD, standard deviation; ADL, activities of daily living.
Cost Between Complication (+) and (-) in OPLL, CSM, and Total Patients After Propensity Score Matching.
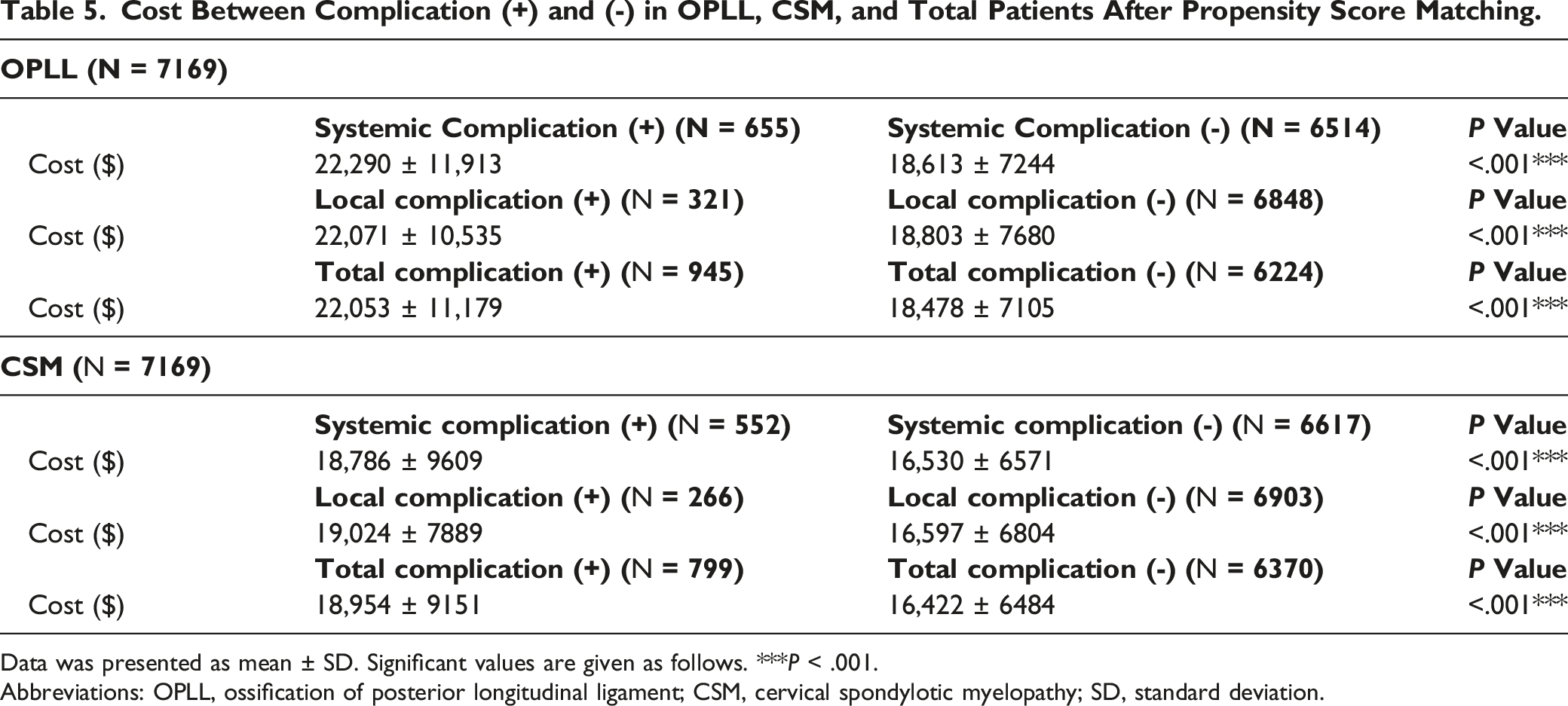
Data was presented as mean ± SD. Significant values are given as follows. ***P < .001.
Abbreviations: OPLL, ossification of posterior longitudinal ligament; CSM, cervical spondylotic myelopathy; SD, standard deviation.
Discussion
This study examined the perioperative complication rates of patients who received LAMP for cervical OPLL or CSM using a nationwide inpatient database in Japan. In addition, Japan is one of the highest aged countries, and the database included patients with relatively high ages (OPLL: 65.1 years old; CSM: 69.3 years old) compared with a similar database study with posterior cervical surgeries performed in Western countries (60.6 years old). 20 Therefore, the results of this study can provide important information when surgeons perform surgery on aged patients. Patients with CSM and OPLL in our study are different because those in the latter category have higher average BMI and an increased incidence of diabetes. Therefore, this study strictly matched the patient’s backgrounds between OPLL and CSM using propensity score matching analysis to accurately assess the perioperative LAMP complication rates.
This study showed that dysphagia after LAMP was more frequent in the OPLL group than in the CSM group. Interestingly, OPLL showed a high incidence of postoperative dysphagia even in posterior laminoplasty that did not require direct manipulation of the retropharyngeal and retrotracheal tissues. OPLL-specific disease characteristics that differ from CSM potentially influence swallowing function. Moreover, OPLL is associated with a high ossification rate of the anterior longitudinal ligament (OALL) in the cervical spine, 21 which possibly causes dysphagia due to narrowing of the retropharyngeal and esophageal cavities.22,23 Furthermore, normal swallowing requires cervical motion (decreased cervical lordosis and backward shift of the subaxial cervical spine), which can be restricted by OPLL and OALL. 24 A previous study reported that decreased cervical spine mobility can cause dysphagia, 23 which supports the increased occurrence of dysphagia in OPLL, where cervical mobility can be decreased.
The results of this study also indicated that OPLL was associated with a higher incidence of respiratory events, especially pneumonia. Postoperative dysphagia in OPLL patients may lead to respiratory complications (e.g., pneumonia) because dysphagia is one of the major risk factors for aspiration pneumonia. 25 Additionally, approximately 50% of patients with cervical OPLL have coexisting diffuse idiopathic skeletal hyperostosis (DISH) according to a previous study, and its development is especially marked at the thoracic level. 21 In addition, DISH can reduce thoracic cage mobility, which restricts pulmonary function. 26 The limited thoracic function may lead to increased pneumonia in patients with OPLL in addition to the occurrence of dysphagia.
Postoperative paralysis occurred in OPLL cases twice as often as CSM cases. Since spinal cord is strongly compressed in most cases of OPLL, neural damage may occur during the decompression. In addition, LAMP provides indirect spinal cord decompression by shifting the spinal cord posteriorly through posterior spinal canal expansion. 27 A previous study described a relatively high incidence of postoperative lower limb paralysis after LAMP for OPLL. 14 They stated that the greater the ossification occupancy, the higher the incidence of postoperative neurological sequelae. 14 Indirect decompression with LAMP, especially in large, asymmetrical OPLL, may result in disproportionate decompression, which may lead to paralysis. Furthermore, the anterior spinal cord compression in CSM is not as great or as disproportionate as in OPLL. Thus, posterior decompression may result in less paralysis.
This study showed that the incidence of postoperative cerebrospinal fluid (CSF) leakage in OPLL was about 4 times higher than in CSM. In ADF for OPLL, resection of the ossified dura mater and/or dural tear associated with detachment of the adhesions results in CSF leakage. 12 Interestingly, the trend toward a high incidence of CSF leakage in OPLL was similar in LAMP, which did not involve resection of the ossified dura mater. In a multicenter prospective study, dural tear frequency was also higher in patients with OPLL than in other types of DCM (OPLL vs other types of DCM: 5.2% vs 2.0%). 28 Hou et al also showed that LAMP and ADF have comparable incidences of CSF leakage in multilevel OPLL (LAMP vs ADF: 2.9% vs 3.3%). 29 A highly narrowed spinal canal by OPLL can cause severe adhesion between the dura and posterior elements, and thus dura mater may be damaged when opening the lamina posteriorly, leading to CSF leakage. Note that a significant risk of dural injury and spinal fluid leakage was noted in patients with OPLL even with LAMP, which does not directly touch the ossification.
Postoperative complications occurred more frequently in patients with OPLL, which led to higher health care costs. Medical costs during hospitalization were approximately $2300 higher in the OPLL group than in the CSM group (OPLL vs CSM: $19,024 vs $16,770; P < .001). Several previous studies have pointed out that the occurrence of perioperative complications leads to increased medical costs in spine surgeries.11,12,15,16,30 One previous study indicated that the incremental cost of treating severe complications exceeded $20,000. In the current cases, perioperative systemic/local complications caused higher hospitalization costs not only in patients with OPLL but also in patients with CSM. Consequently, the occurrence of perioperative complications increased medical costs by approximately $2000 to $3000 in both the OPLL and CSM groups. In particular, the total medical cost exceeded $20,000 when perioperative complications occurred in the OPLL group. Thus, how to reduce perioperative complications by devising a surgical technique is an extremely important issue either in CSM or OPLL.
This study has several limitations. The database only contained information during hospitalization and considering mortality and postoperative complications after hospital discharge was not possible. The database system is unable to reflect some clinically important findings due to the lack of imaging and laboratory data and the diagnosis by only coding with the ICD-10 code. For example, cervical spine alignment, the level of spinal cord compression, the severity of neurological symptoms as reflected in the Japanese Orthopedic Association score, and the actual techniques of laminoplasty (bilateral or unilateral openings) were not available in this database system. In addition, the definition of perioperative complications was not optimized. The incidence of perioperative complications in such database studies can be affected by diagnostic strategies and definitions.31,32 Further research would be needed with more clinical information and detailed diagnostic strategies and definitions.
Conclusions
A retrospective cohort analysis using a large national inpatient database revealed the perioperative OPLL and CSM complication rates in LAMP. More systemic complications (e.g, respiratory events, paralysis, and CSF leakage) were observed in the OPLL group. The findings of this study may provide useful information to surgeons planning to perform LAMP for DCM patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Ethical Statement
The study protocol was approved by the institutional review boards of Tokyo Medical and Dental University. (M2000-788-22). A statement of the location where the work was performed. All research work has been performed in Tokyo Medical and Dental University.