
Abstract
Objectives
To compare the effect of delaying surgery on clinical outcome in patients with chronic sciatica secondary to lumbar disc herniation.
Methods
Patients with sciatica lasting 4–12 months and lumbar disc herniation at the L4–L5 or L5–S1 level were randomized to undergo microdiscectomy (early surgery) or to receive 6 months of nonoperative treatment followed by surgery if needed (delayed surgery). Outcomes were leg pain, Oswestry Disability Index score (ODI), back pain, SF–36 physical component (PCS) and mental component (MCS) summary scores, employment, and satisfaction measured preoperatively and at 6 weeks, 3 months, 6 months, and 1 year after surgery.
Results
Of the 64 patients in the early surgery group, 56 underwent microdiscectomy an average of 3 ± 2 weeks after enrollment. Of the 64 patients randomized to nonoperative care, 22 patients underwent delayed surgery an average of 53 ± 24 weeks after enrollment. The early surgery group experienced less leg pain than the delayed surgery group, which was the primary outcome, at 6 months after surgery (early surgery 2.8 ± .4 vs delayed surgery 4.8 ± .7; difference, 2.0; 95% confidence interval, .5–3.5). The overall estimated mean difference between groups significantly favored early surgery for leg pain, ODI, SF36-PCS, and back pain. The adverse event rate was similar between groups.
Conclusions
Patients presenting with chronic sciatica treated with delayed surgery after prolonging standardized non-operative care have inferior outcomes compared to those that undergo expedited surgery.
Introduction
Surgery to treat acute sciatica secondary to lumbar disc herniation is recognized to provide a faster recovery compared to prolonged conservative care followed by delayed surgery if needed, but outcomes become equal by 1 year. 1 In contrast, microdiscectomy for chronic sciatica from lumbar disc herniations provides superior and sustained benefit over conservative care. 2 In the case of acute sciatica, delayed surgery did not appear to negatively affect the ultimate outcome.1,3 This may not be the case for more chronic disc herniations.4–7
In our previously published randomized controlled trial (RCT) comparing microdiscectomy to standardized conservative care for sciatica from lumbar disc herniation lasting greater than 4 months the cross-over of non-operative patients to surgery before 6 months after enrollment was minimized by design. 2 This design therefore created a cohort of patients that received early surgery and a cohort of patients that received non-operative care followed by delayed surgery. In the current study, we present a secondary analysis of patients that underwent early surgery compared to those that received non-operative care followed by delayed surgery (waiting 6 months or longer) for chronic sciatica secondary to a lumbar disc herniation. The primary aim of the current study was to examine the hypothesis of whether patients report less leg pain at 6 months after early surgery as compared to those that received delayed surgery.
Methods
Eligibility and Randomization
The trial was approved by our institutional research ethics board and is registered (ClinicalTrials.gov number, NCT01335646). All participants provided written informed consent before enrollment in the study.
Consecutive patients referred to the London Health Science Centre, London Canada, from February 2010 through August 2016 were screened for this study by a research coordinator by telephone and by a study physician at an initial screening visit. Inclusion criteria were age 18–60 years, unilateral radiculopathy lasting 4–12 months, and posterolateral disc herniation at L4–5 or L5–S1 on the appropriate side with compression of the corresponding traversing nerve root confirmed on magnetic resonance imaging. Patients were excluded if they had radiculopathy secondary to the following at the involved level: herniation within the foramen or far lateral disc, spinal stenosis, deformity (i.e., Scoliosis >10°), or previous lumbar spine surgery. Patients were also excluded if they had epidural spinal injection or exercised-based physiotherapy for the presenting episode of sciatica. Patients were randomly assigned in a 1:1 allocation to early surgery or nonoperative care followed by surgery if needed (delayed surgery) by a computer-generated random number list using a permuted block design. Patients were stratified according to work’s compensation status.8,9
Trial Interventions
Early Surgery
An open or minimal-access approach was used for microdiscectomy with loupe or microscope assistance/magnification. All surgeries were performed as day surgery or 1-night stay.
Delayed Surgery
Patients in the delayed surgery group received initial nonoperative care while waiting on the surgical waiting list. Non-operative treatment included patient education, oral analgesics (non-steroidal anti-inflammatory drugs, acetaminophen, or acetaminophen with codeine/oxycodone/tramadol, and amitriptyline/gabapentin/pregabalin as tolerated), an active exercised-based physiotherapy program, and up to 3 epidural steroid injections/therapeutic nerve root block. The standard wait on the waiting list was greater than 6 months. Therefore, patients with persistent symptoms underwent surgery following this standard wait.
Outcome Measures
Outcomes were assessed preoperatively and at 6 weeks, 3 months, 6 months, and 1 year after surgery. The primary outcome was the visual analog scale (VAS) for intensity of leg pain (range 0–10: 0 = no pain, 10 worst pain) measured at 6 months following surgery. Secondary measures which were measured at 3 months, 6 months, and 1 year were the VAS intensity for leg pain, VAS for intensity of low back pain, the Oswestry Disability Index (ODI), 10 the Medical Outcomes Study 36-item Short-Form General Health Survey (SF36) physical component summary (PCS) score and mental component summary score,11,12 employment status, and satisfaction with treatment. 13 Adverse events related to surgical treatment were documented for up to 1 year after surgery.
Statistical Analysis
The sample size was determined for the parent RCT and was not calculated specifically for the purpose of this analysis. For the parent RCT, 15 patients per group were determined to be required to detect a minimal important difference of 2 points in leg pain intensity at 6 months after surgery between the cohort treated with early surgery and that treated with delayed surgery. We assumed a standard deviation of 1.9 points, a statistical power of .80, and a 2-tailed significance level of .05. All analysis was performed using SPSS software, version 26 (SPSS Inc, Chicago, IL, USA). Significance was set at a two-sided alpha level of 5% with no adjustments made for multiple comparisons.
Differences at baseline were examined with the use of a Students t-test, Mann U Whitney test, chi-square test, or Fisher’s exact test as appropriate. Participants with missing data at the 12-month time point were compared to those who participated in all visits.
Linear mixed effects models were used to compare continuous outcomes between groups, using a random effect for participant and a compound symmetry assumption on the correlation of residuals. Treatment (early surgery vs delayed surgery), time (categorical), treatment × time interaction, baseline score, and covariates associated with baseline and missing values including sex and smoking status were included in the model. The estimated marginal difference between groups taking all time points into consideration (overall treatment effect), and the adjusted mean differences between groups and the 95% confidence intervals (CIs) at each predetermined time point were compared. For binary outcomes, generalized estimating equations were used to fit repeated measures. Post-operative follow-up time points were based on the time of surgery with the baseline assessment taken at enrollment for the early surgery group and immediately prior to surgery for the delayed surgery group.
Results
A total of 790 patients were screened for eligibility by telephone interview (Figure 1). Of these patients, 128 were enrolled with 64 randomized to early surgery and 64 randomized to initial non-operative treatment with delayed surgery if needed. The majority of the 622 patients excluded had either improved (46%) or declined to participate (16%). Flow diagram showing early surgery and delayed surgery cohorts, and follow-up. patients were randomized to receive 6 months of nonoperative treatment followed by surgery if needed (delayed surgery). bcumulative over time.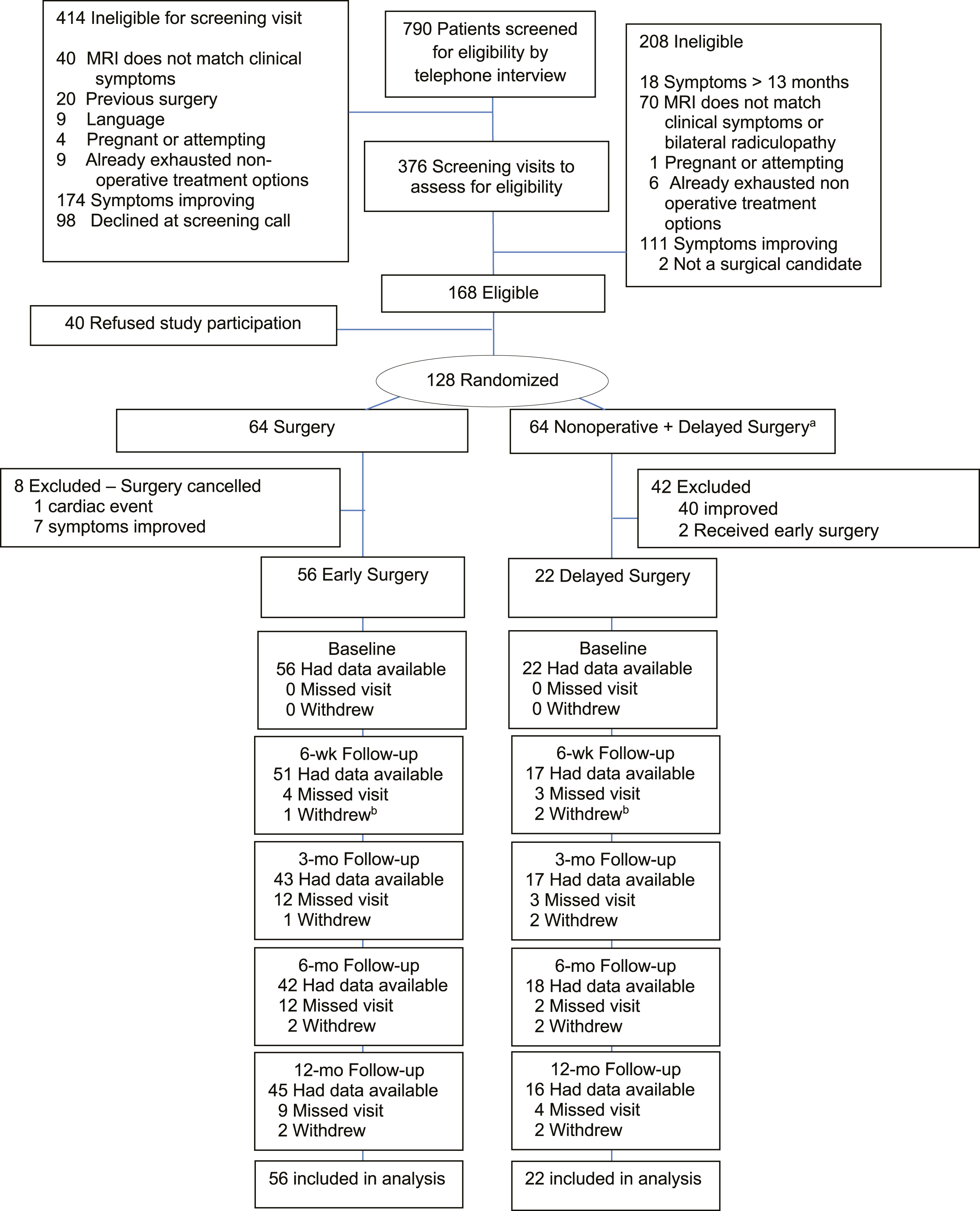
Of the 64 patients in the early surgery group, 56 received surgical treatment per protocol. Seven patients canceled their surgery because they felt their symptoms had improved. One patient developed a cardiac arrhythmia during the pre-operative work-up and was not able to undergo surgical treatment. Out of the 64 patients randomized to initial non-operative care followed by surgery if needed, 2 patients sought treatment at another facility and received early surgical treatment within 8 weeks after enrollment. Of the remaining 62 patients, 22 patients graduated to delayed surgery following 6 months of non-operative care for the initial presenting radiculopathy. The follow-up rate ranged from 87% at the 6-week visit to 73% at the 12-month visit with losses due to missed visits or withdrawals (Figure 1). Patients that missed their 12-month follow-up appointment were more likely to smoke (71% vs 19%, P = .004) and were more likely to be male (49% vs 88%, P = .005) compared to patients that did not miss this appointment.
Demographic and Clinical Characteristics of Patients at Baseline.
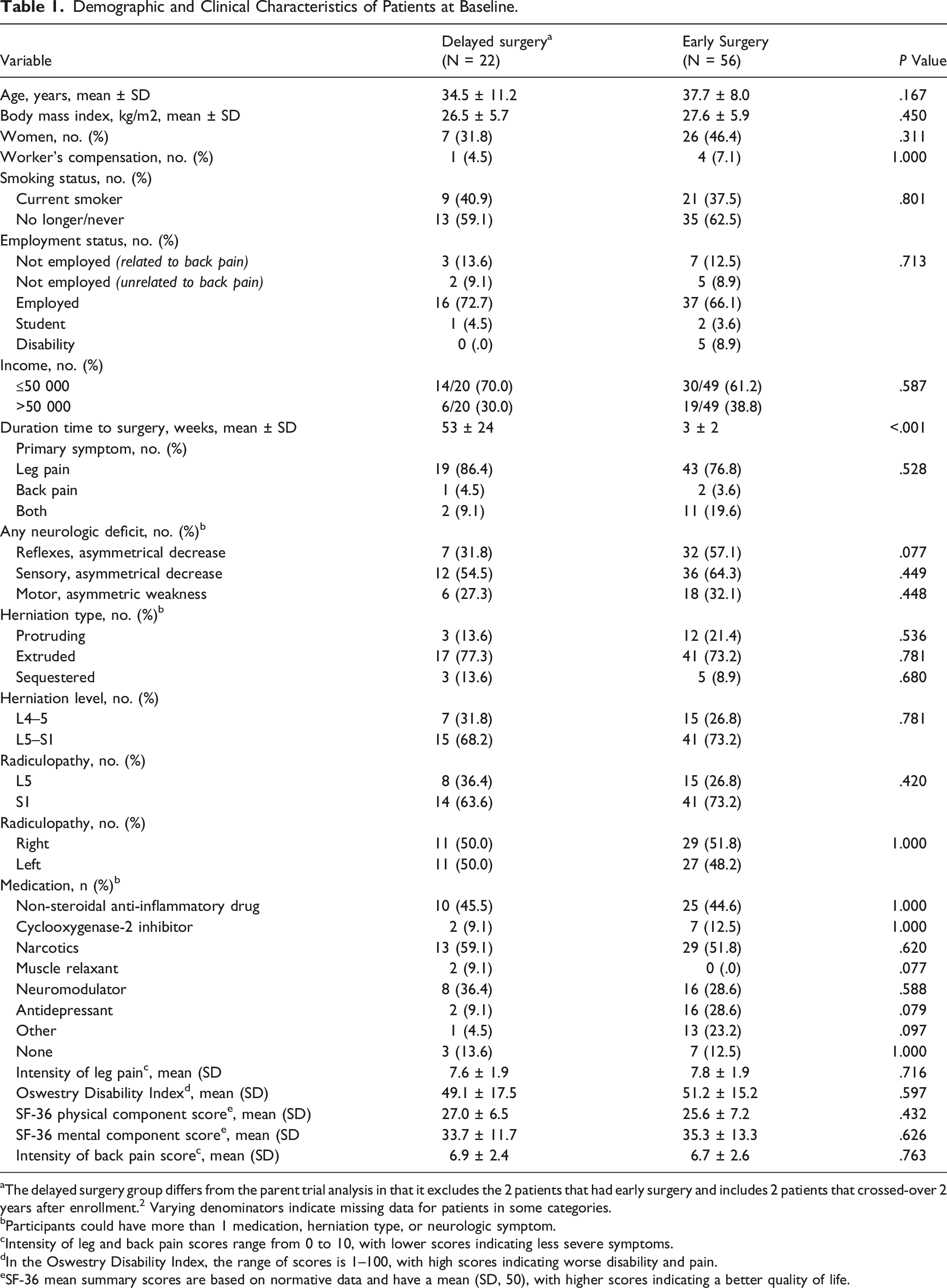
aThe delayed surgery group differs from the parent trial analysis in that it excludes the 2 patients that had early surgery and includes 2 patients that crossed-over 2 years after enrollment. 2 Varying denominators indicate missing data for patients in some categories.
bParticipants could have more than 1 medication, herniation type, or neurologic symptom.
cIntensity of leg and back pain scores range from 0 to 10, with lower scores indicating less severe symptoms.
dIn the Oswestry Disability Index, the range of scores is 1–100, with high scores indicating worse disability and pain.
eSF-36 mean summary scores are based on normative data and have a mean (SD, 50), with higher scores indicating a better quality of life.
Adjusted Mean or Percentage and Difference for Primary and Secondary Outcomes.
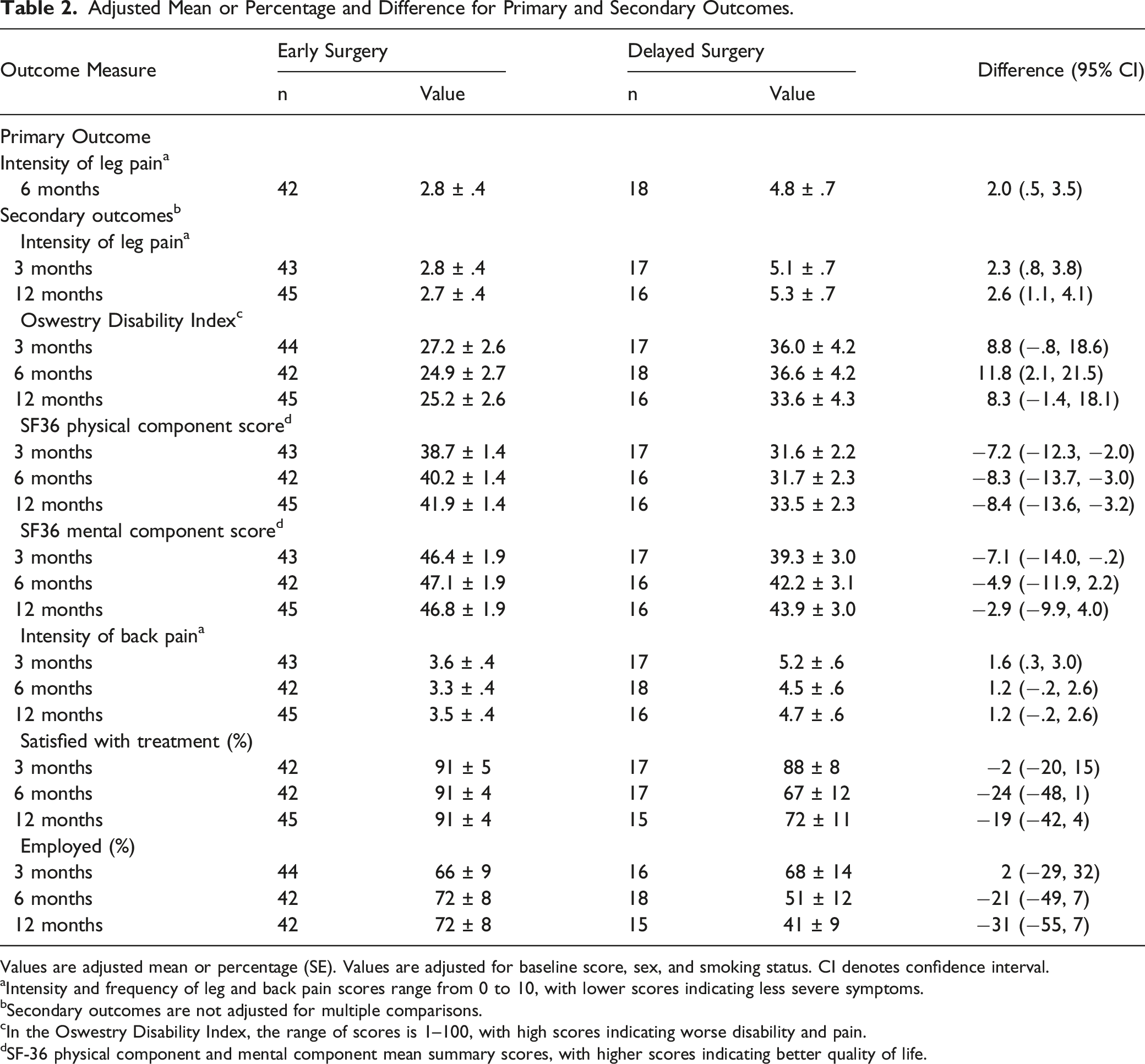
Values are adjusted mean or percentage (SE). Values are adjusted for baseline score, sex, and smoking status. CI denotes confidence interval.
aIntensity and frequency of leg and back pain scores range from 0 to 10, with lower scores indicating less severe symptoms.
bSecondary outcomes are not adjusted for multiple comparisons.
cIn the Oswestry Disability Index, the range of scores is 1–100, with high scores indicating worse disability and pain.
dSF-36 physical component and mental component mean summary scores, with higher scores indicating better quality of life.

Time course of patient-rated clinical outcomes. Scores over time are shown for (A) Leg-pain intensity (primary outcome), (B) Oswestry Disability Index, (C) Back-pain intensity, (D) SF-36 physical component summary score, (E) SF-36 mental component summary score, (F) satisfaction with treatment, and (G) the employment status. At 0 months, the data points represent the observed means. The data points on the plot lines represent the estimated means or proportions from mixed effects longitudinal analysis adjusted for baseline score and covariates associates with baseline and missing values, with error bars denoting 95% confidence interval (CI). The overall mean (taking all time points into consideration) of each group, standard error, difference between groups, and the corresponding 95% CI are indicated. Intensity of leg and back pain scores range from 0 to 10, with lower scores indicating less severe symptoms. In the Oswestry Disability Index, the range of scores is 1–100, with high scores indicating worse disability and pain. In the SF-36 physical component and mental component summary scores, higher scores indicate better quality of life.
Adverse Events Related to Surgery.
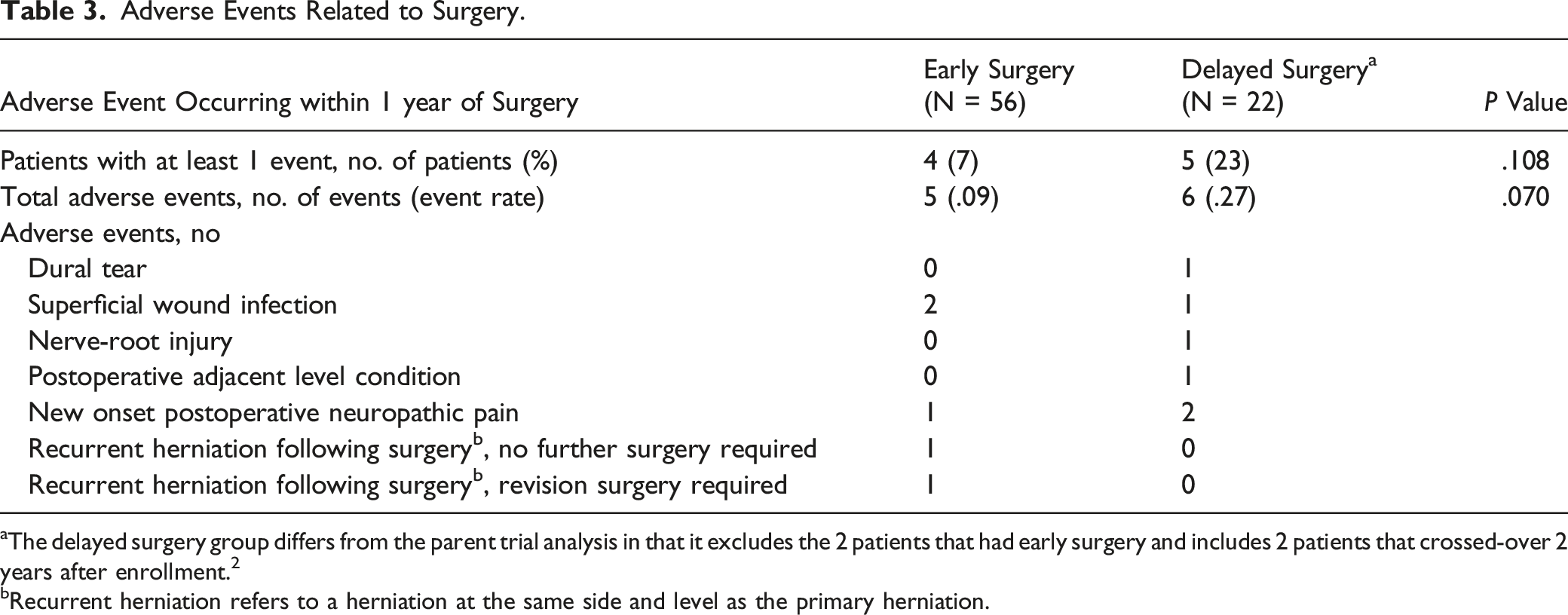
aThe delayed surgery group differs from the parent trial analysis in that it excludes the 2 patients that had early surgery and includes 2 patients that crossed-over 2 years after enrollment. 2
bRecurrent herniation refers to a herniation at the same side and level as the primary herniation.
Discussion
This study demonstrates that patients who undergo delayed surgery for a chronic disc herniation following failure of 6 months of standardized non-operative care, had overall poorer patient rated-outcome measures than those that received early surgery. This finding has important implications for the shared decision-making process in the treatment of lumbar disc herniations. Not only does prolonged non-operative care have inferior results compared to early discectomy 2 (as found in the original RCT on which this analysis is based) but this follow-up study further demonstrated that delayed surgery resulted in inferior outcomes. Therefore, the consideration to “try” non-operative care for a patient presenting with chronic sciatica with the expectation of defaulting to surgery should that trial fail, will potentially increase the risk of a lesser improvement compared to early surgery. It is important to note that chronic sciatica was defined as lasting more than 4 months and excluded patients that presented with more than 12 months of sciatic when generalizing our study’s findings.
Our findings are in contrast to those for acute sciatica from a lumbar disc herniation. Peul et al compared early vs prolonged conservative care followed by (delayed) surgery for acute sciatica, defined by symptoms of 6–12 weeks, and found that the results of delayed surgery were similar at 1 year follow-up to early surgery.1,3 However, beside the difference in chronicity of sciatica between the 2 studies, the length of the delay to surgery was also shorter, averaging 14.6 weeks as compared to our average wait of 53 weeks. Our RCT was designed within the constraints of the Canadian health care system, which provided for a minimum surgical wait in the delayed group of 6 months. This reflects the normal wait-time to have a surgical consult and receive surgery. Similar waits in other public systems are likely, and given this prolonged wait, the potential negative consequences of deferring the decision to operate needs to be carefully considered. Furthermore, enhanced access to microdiscectomy within these medical systems should be considered recognizing the potential morbidity in delayed treatment.
Other studies have found duration of sciatica to negatively correlates with post-discectomy outcomes. Nygaard et al. found that after 8 months of leg pain, there may be increased risk of a poor surgical outcome. 4 Rihn et al. performed an as-treat analysis of the Spine Pain and Outcomes Research Trial to demonstrate that symptom duration greater than 6 months led to inferior outcomes. 7 This study differed from ours with their inclusion of patients with a more acute sciatica presentation and that patient preference was a key deciding factor in the decision to operate as the analysis combined the observational arm and randomization arm (which had substantial cross-over due to patient preference). However, Quon et al, showed that patients in a system-imposed wait, as opposed to patient preference, of more than 12 weeks had a comparatively higher chance of experience a worse outcome then patients waiting less than 12 weeks. 5 They also found that self-reported symptom duration negatively correlated with surgical outcome at 6 months. This study, however, also combined patients with both acute and chronic sciatica and defined outcome based on the patient’s predominant pain symptom which could be either leg or back pain. Our study supports the findings of these previous trials in that the results are of higher quality evidence and represent a relatively homogenous population of patients with chronic sciatica single payer public health system from a universal public health system.
Our finding that patients undergoing delayed surgery had worse outcomes compared to those undergoing early surgery is likely due to the delay in treatment and the potential centralization of chronic pain. Once such explanation may be due to sensitization of the central nervous system elicited by a prolonged inflammatory and immune mediated response.14-16 Ongoing nociceptive sensitization in animal and in vitro human models is thought to evoke changes in plasticity and remodeling of spinal and supraspinal pain pathways that maintain chronic pain even after mechanical compression of the nerve is relieved and the inflammation has resolved.14-16
A number of potential limitations exist in this study. Firstly, this was a secondary analysis of a randomized controlled study, for which the primary comparison was operative vs non-operative care and not specifically delayed surgery. From an ethical perspective, patients randomized to delayed surgery required non-operative treatment while awaiting surgery. As expected, patients did improve with non-operative care and approximately only a third of patient’s ultimately chose to undergo delayed surgery following their trial of standardized non-operative care. There was no difference between these surgical groups in baseline demographics or clinical characteristics. However, as this is a secondary analysis there may be confounding variables that were not accounted for in the trial design. Another caveat is that selection bias may exist at the time of enrollment, as both the participating surgeons and patients may be less inclined to pursue non-operative care if they suffer from severe sciatica. However, only a small percentage of patients declined participation at the time of recruitment; suggesting our study population is well representative of the population referred in a universal health care system with chronic sciatic from lumbar disc herniation. Although, this was a RCT by design, only the accessors, but not the surgeons, physicians, therapists, or patients were blinded to the treatment. Further, secondary outcomes were not adjusted for multiple comparisons and thus these findings should be interpreted with caution. Our lost to follow-up rate was initially good at early follow-up periods but declined to 73% by the 1-year time point. The baseline characteristics of patients with missed visits at this time point were similar to the rest of the cohort except these patients were more likely to be male and smoke. Finally, we included only patients with an L4–5 and L5–S1 disc herniation which may limit the findings generalizability to a patient with an upper lumbar disc herniation.17,18
In conclusion, this study found that patients treated with delayed surgery presenting with chronic sciatica from a lumbar disc herniation have inferior outcomes compared to those that undergo expedited surgery. For patient and surgeon preference, this has important implications in the decision to pursue non-operative vs operative care. Furthermore, it demonstrates the potentially deleterious effect a system-imposed wait, such as that experienced in publicly funded health care system, could have in outcome following lumbar discectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Physicians’ Services Incorporated Foundation.