
Abstract
Study design
Retrospective cohort study.
Objectives
This study evaluated the outcomes of radiation therapy (RT) as the initial treatment for Bilsky grade 2 metastatic epidural spinal cord compression (MESCC) and identified the risk factors associated with RT failure.
Methods
This retrospective cohort study enrolled 151 patients diagnosed with Bilsky grade 2 MESCC. Patients were divided into 2 groups, viz. those who initially underwent RT (n = 127) and those treated with surgery at presentation (n = 24). The patient demographics, treatment outcomes, and risk factors for RT failure were analyzed. The Spinal Instability Neoplastic Score (SINS) and clinical outcomes such as ambulatory status and neurological function were compared. Logistic regression was performed to identify factors predictive of RT failure.
Results
RT was successful in 85.8% (109/127) of patients, and only 14.2% (18/127) required surgery due to symptom progression. The SINS were significantly higher in the RT-failure group (9.6 ± 3.2) than in the RT-success group (7.4 ± 2.8, P = 0.003). SINS scores >8 were associated with a higher risk of RT failure. Patients the surgery group were younger and presented more frequently with neurological deficits. No significant differences in final ambulatory status or survival were observed between the RT-success and RT-failure subgroups.
Conclusions
RT can be a viable initial treatment option for Bilsky grade 2 MESCC in the absence of neurological deficits or severe mechanical pain. However, patients with greater spinal instability (SINS >8) face a higher risk of RT failure and may benefit from surgical intervention at diagnosis.
Keywords
Introduction
Approximately 10% of patients with spinal metastasis develop metastatic epidural spinal cord compression (MESCC) during the disease course.1,2 Limited ambulatory function due to MESCC diminishes the patient’s ability to perform self-care, and erodes the willingness to seek systemic treatment, ultimately reducing life expectancy. 3 Therefore, timely management of MESCC with radiation therapy (RT) or surgery is essential to improve the patient’s functional independence and survival.4-6
The severity of MESCC is classified using the Bilsky classification.7,8 Bilsky grade 1 is considered low-grade MESCC and is often initially managed with RT, as the metastatic mass does not directly compress the spinal cord. 7 Considering the morbidity associated with surgical treatment in patients with multiple comorbidities, RT is often sufficient for impeding the progression of grade 1 MESCC.5,9 However, for severe cases, such as Bilsky grade 3, surgery is considered more frequently due to the high risk of neurological deficits. 9
The selection of the initial treatment for patients with Bilsky grade 2 MESCC is often challenging.5,10,11 Although grade 2 MESCC poses a risk of neurological deficit due to spinal cord compression, the risk of weakness may not be very high for some patients owing to the partial preservation of the space within the dural sac.9,12 If the risk of post-RT symptom progression is high enough to necessitate surgery for grade 2 MESCC, it should be considered at the initial presentation. 9 Conversely, RT may be preferable if it can effectively prevent clinical exacerbation in patients with Bilsky grade 2 MESCC. 5
While previous studies have shown that higher grades of MESCC are associated with greater symptom severity at presentation and worse outcomes, the prognosis of Bilsky grade 2 has not been thoroughly evaluated. Therefore, this study aimed to 1) assess the risk of RT failure when performed as local treatment for Bilsky grade 2 MESCC and 2) identify the risk factors that increase the likelihood of RT failure, necessitating additional surgery.
Materials and Methods
Study Design and Population
This retrospective cohort study was approved by the relevant institutional review board Patient Selection Process MESCC, Metastatic Epidural Spinal Cord Compression; RT, Radiation Therapy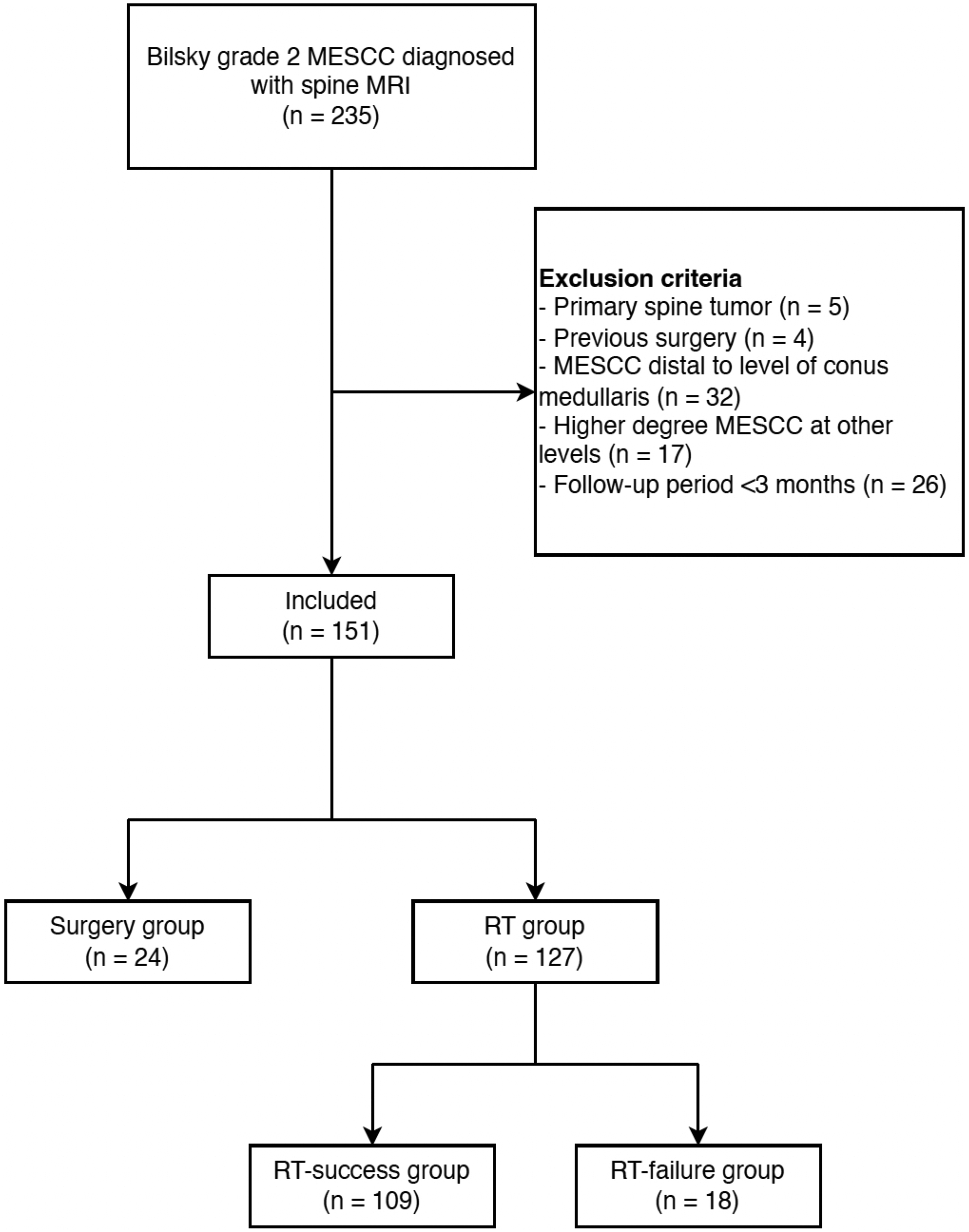
The primary outcome of this study was failure of RT since we intended to clarify whether RT is an optimal initial treatment for grade 2 ESCC and analyze the factors associated with the failure of RT. Failure of RT was defined as progression or recurrence of neurological deficit or mechanical pain warranting surgical management despite administering RT at the level of MESCC. Symptom occurrence due to new onset, distant level metastasis was not considered failure of RT. Furthermore, persistence of cord compression only identified by imaging not accompanied by symptom aggravation was not considered as RT failure.
Bases on the initial treatment performed at first presentation, patients were assigned to the RT group or surgery group. In the RT group, patients who did not require surgery at the level of MESCC until the final follow-up were subclassified into the RT-success subgroup, and into the RT-failure subgroup when surgery was needed due to clinical aggravation caused by MESCC. Surgery was performed by 4 spine surgeons. The decision to operate was based on multidisciplinary consultation involving the medical oncologist, radiation oncologist, general surgeon, and spine surgeons. 4 Patient performance status, available systemic therapy options, characteristics of metastatic lesion, and required surgical procedures were considered. When needed, emergent surgery was performed based on the operating surgeon’s discretion. The surgical strategies were individualized, and based on the patient’s general health status, location of metastasis, and spinal instability. However, separation surgery which included posterior instrumentation combined with laminectomy and epidural tumor tissue removal in order to restore cerebrospinal fluid space surrounding the spinal cord was considered the standard surgical procedure. 15 Instrumentations were performed by midline posterior open approach.
Radiographic Evaluation and Variables
Although the spinal MRI was initially reviewed by a radiologist specializing in musculoskeletal disorders, a spine surgeon with 5 years’ experience reviewed the MRI again and graded the MESCC based on the Bilsky system. MESCC was graded as 2 when the mass compressed the spinal cord with cerebrospinal fluid space visible around the cord. 7
The patient’s demographic factors, primary pathology, initial patient symptom, location of MESCC, Spine Instability Neoplastic Scores (SINS), Eastern Cooperative Oncology Group (ECOG) performance scale, ambulatory status, and motor grade were recorded. The motor grade was assessed using American Spinal Injury Association impairment scale (AIS) and recorded as the greatest strength of the level involved. Patient survival was assessed as the period between the initial presentation with MESCC and death or discharge.
In the RT group, the RT dosage per fraction, number of fractions, and total dosage were recorded. For patients who required surgery after RT, symptoms that required surgical management, type of surgery, and interval between termination of RT and surgery were identified.
Statistical Analysis
Comparisons were performed between the RT and surgery groups. Subgroup analysis within the RT group comparing patients who needed RT alone and those who subsequently needed surgery was also conducted. Normality of continuous variables was assessed using the Shapiro–Wilk test. All continuous variables followed a normal distribution (P> 0.05) and were analyzed using independent t-tests (Supplemental Table 1). Categorical variables were analyzed using the chi-square test. Logistic regression analysis was performed to identify the risk factors associated with the need for surgery after initial RT. Kaplan–Meier survival analysis was performed for the RT-success group. Receiver operating characteristic (ROC) curve analysis was performed to identify the cut-off value of each risk factor identified in the logistic regression analysis. Statistical analysis was performed using the Statistical Packages for the Social Science for MAC (version 29.0.0; SPSS Inc, Chicago, IL, USA). P-values <0.05 were considered statistically significant.
Results
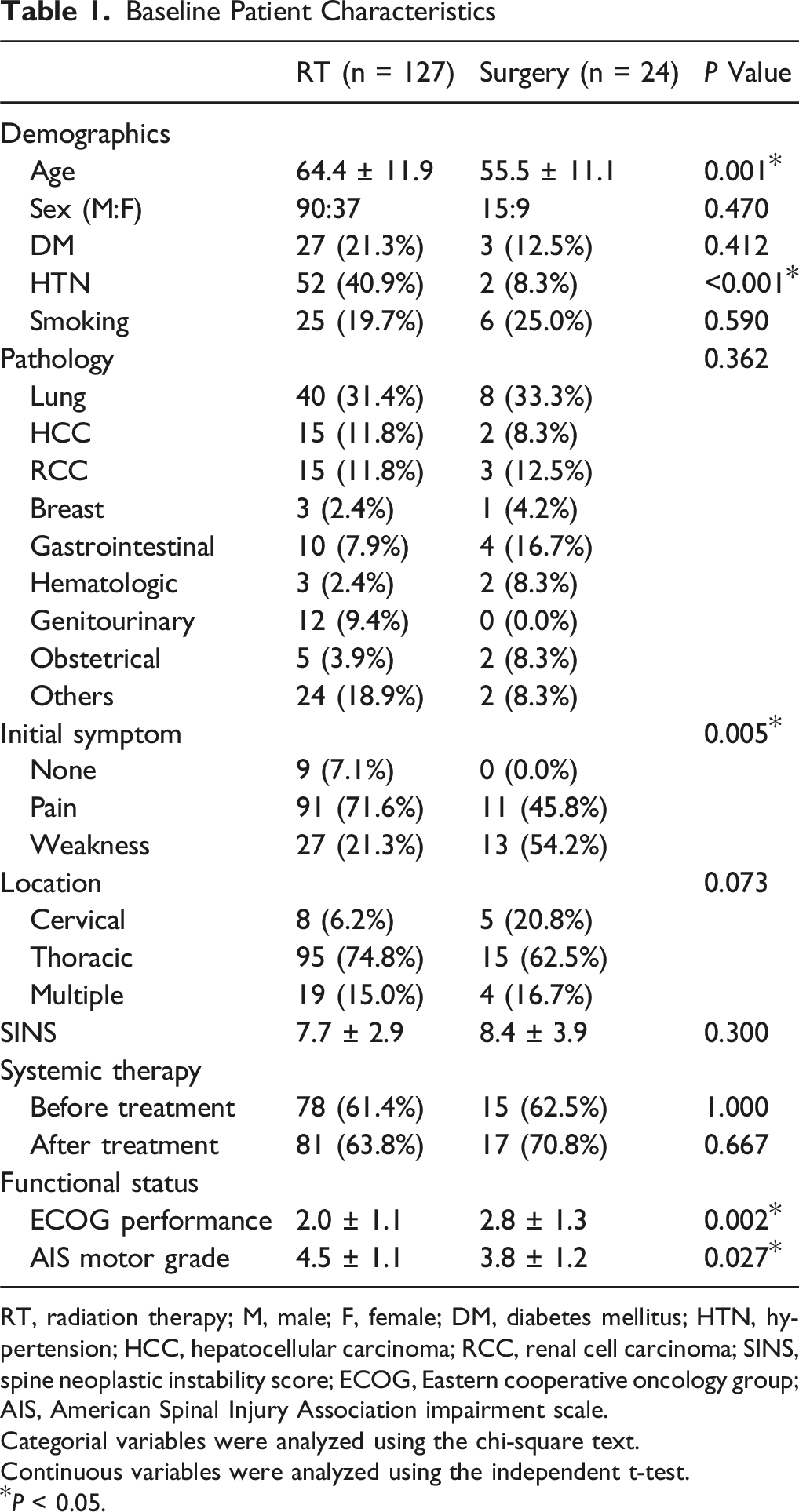
After meeting the eligibility criteria, 151 patients were enrolled in the study. Upon reassessment, 135 patients (89.4%) had Bilsky grade 2, 6 patients (4.0%) had grade 1c, and 10 patients (6.6%) had grade 3. Twenty-four patients (15.9%) underwent surgery at initial presentation (surgery group; age, 55.5 ± 11.1 years; 15 men, 62.5%) (Figure 2), while the remaining 127 patients (84.1%) were initially treated with RT (RT group; age, 64.4 ± 11.9 years; 90 men, 70.9%). Two patients (8.3%) in the surgery group underwent cervical corpectomy, while 22 patients (91.7%) underwent posterior instrumentation and separation of the tumor from the spinal cord. Lung cancer was the most common primary origin in both groups (RT group, 31.4%; surgery group. 33.3%). Patients in the surgery group (55.5 ± 11.1 years) were significantly younger than those in the RT group (64.4 ± 11.9 years; P = 0.001). Furthermore, neurological weakness was the predominant symptom in the surgery group (13/24, 54.2%) compared to pain (11/24, 45.8%), while patients in the RT group had a higher frequency of pain (91/127, 71.6%) than neurological deficit (27/127, 21.3%; P = 0.005). The surgery group had worse general performance (P = 0.002) and motor grade (P = 0.027) compared to the RT group (Table 1). Illustrative Case 1 A 75-Years-old Man With a History of Lung Cancer Presented to the Emergency Department With Back Pain and Paraplegia. His Motor Grade was 2 Throughout the Lower Extremities. Baseline Patient Characteristics RT, radiation therapy; M, male; F, female; DM, diabetes mellitus; HTN, hypertension; HCC, hepatocellular carcinoma; RCC, renal cell carcinoma; SINS, spine neoplastic instability score; ECOG, Eastern cooperative oncology group; AIS, American Spinal Injury Association impairment scale. Categorial variables were analyzed using the chi-square text. Continuous variables were analyzed using the independent t-test. *P < 0.05.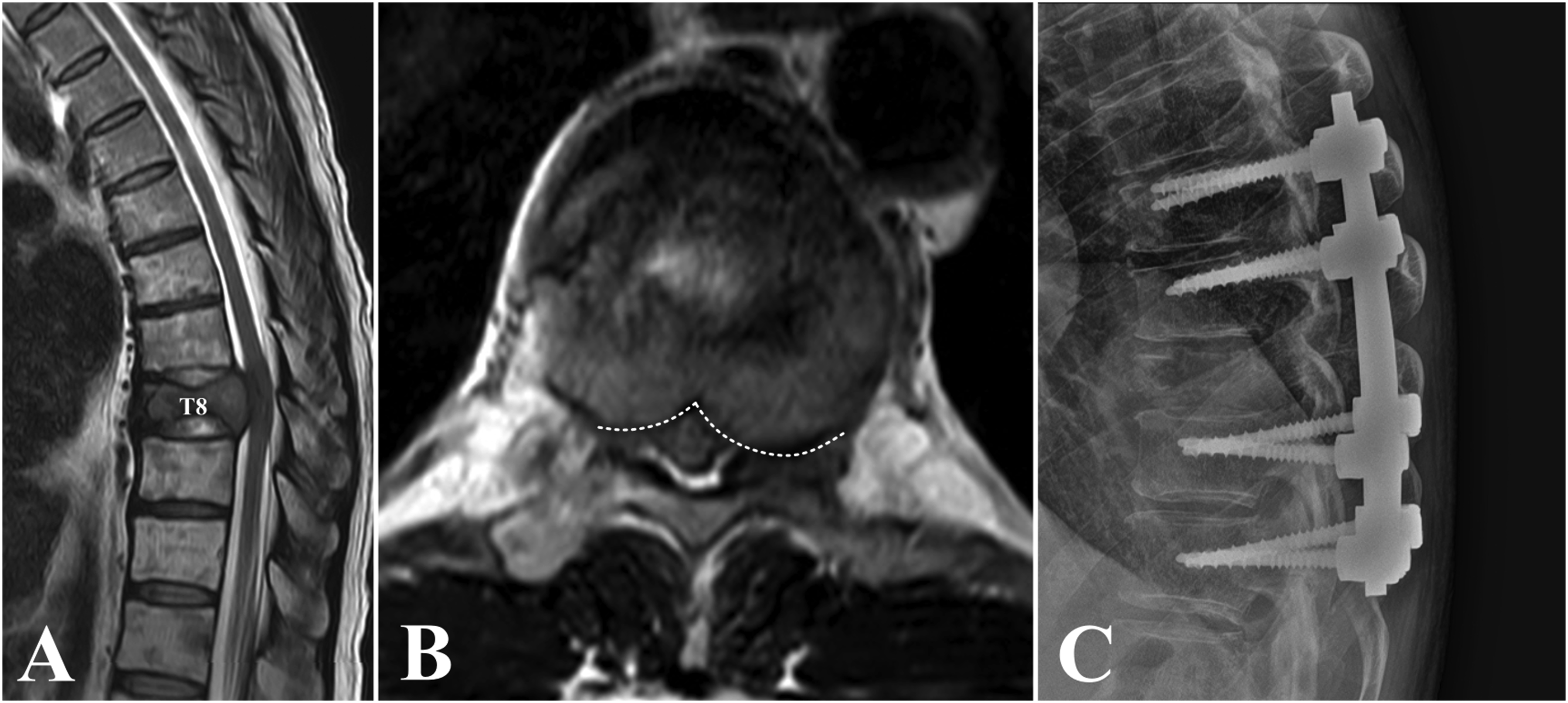
Two patients (8.3%) in the surgery group required additional treatment due to wound infection; 1 patient (4.2%) died 2 weeks after surgery due to pulmonary thromboembolism. In the RT group, median total dose was 30 Gy (range, 8-45), and median number of fractions was 5 (range, 1-15). Median dose per fraction was 4 Gy (range, 3-10).
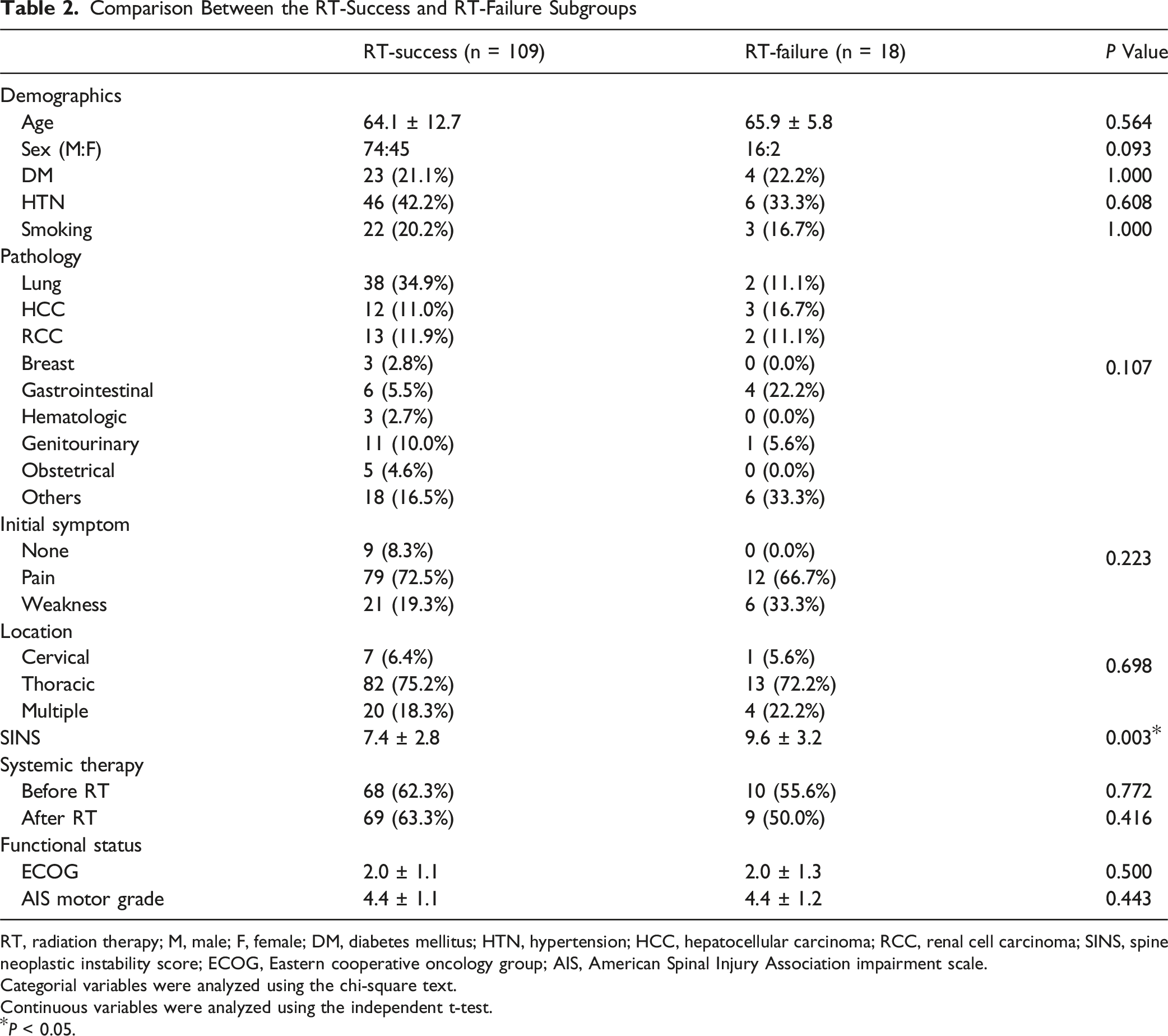
Comparison Between the RT-Success and RT-Failure Subgroups
Among 127 patients who were initially treated with RT, 18 patients (14.2%) needed surgery due to MESCC progression and were assigned to the RT-failure subgroup (Figure 3); 109 patients (85.8%) who did not need further surgical treatment were designated as the RT-success group. The interval between RT and surgery in the RT-failure subgroup was 7.0 ± 5.2 months. Ten patients (55.6%) needed surgery due to progression of neurological deficits, while 8 patients (44.4%) needed surgery due to mechanical back pain unresponsive to conservative management. The baseline demographic factors did not differ significantly between the 2 groups. Lung cancer (38/109, 34.9%) was the most common primary origin in the RT-success subgroup, while gastrointestinal malignancy (4/18, 22.2%) was most common in the RT-failure subgroup. Furthermore, the SINS was significantly higher in the RT-failure subgroup (9.6 ± 3.2) than in the RT-success subgroup (7.4 ± 2.8, P = 0.003). Two patients (2/18, 11.1%) in the RT-failure subgroup required wound revision after initial surgery, and 1 patient (1/18, 5.6%) underwent revision instrumentation due to mechanical failure (Table 2). One patient (5.6%) in the RT-failure subgroup received cervical corpectomy, 16 patients (88.9%) underwent posterior instrumentation with decompression, and 1 patient (5.6%) could not undergo surgery due to the general condition. Illustrative Case 2 A 73-Years-old Man Who was Being Treated for Malignant Pheochromocytoma Presented With Back Pain. He did Not Have Neurologic Compromise of the Lower Extremity and was Able to Walk Without Significant Difficulty. Comparison Between the RT-Success and RT-Failure Subgroups RT, radiation therapy; M, male; F, female; DM, diabetes mellitus; HTN, hypertension; HCC, hepatocellular carcinoma; RCC, renal cell carcinoma; SINS, spine neoplastic instability score; ECOG, Eastern cooperative oncology group; AIS, American Spinal Injury Association impairment scale. Categorial variables were analyzed using the chi-square text. Continuous variables were analyzed using the independent t-test. *P < 0.05.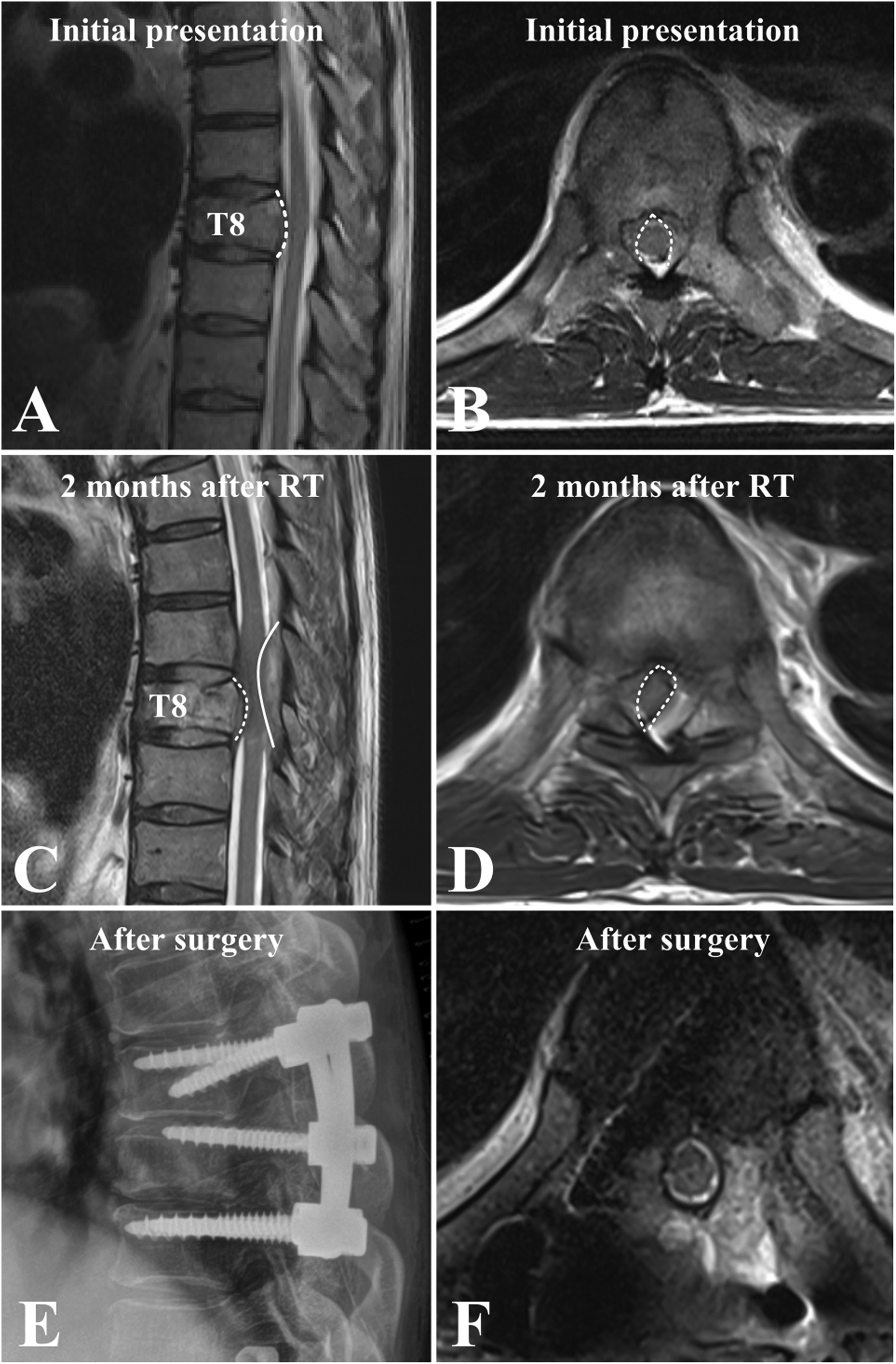
Outcomes at Final Follow-Up in the RT-Success Subgroup and RT-Failure Subgroup
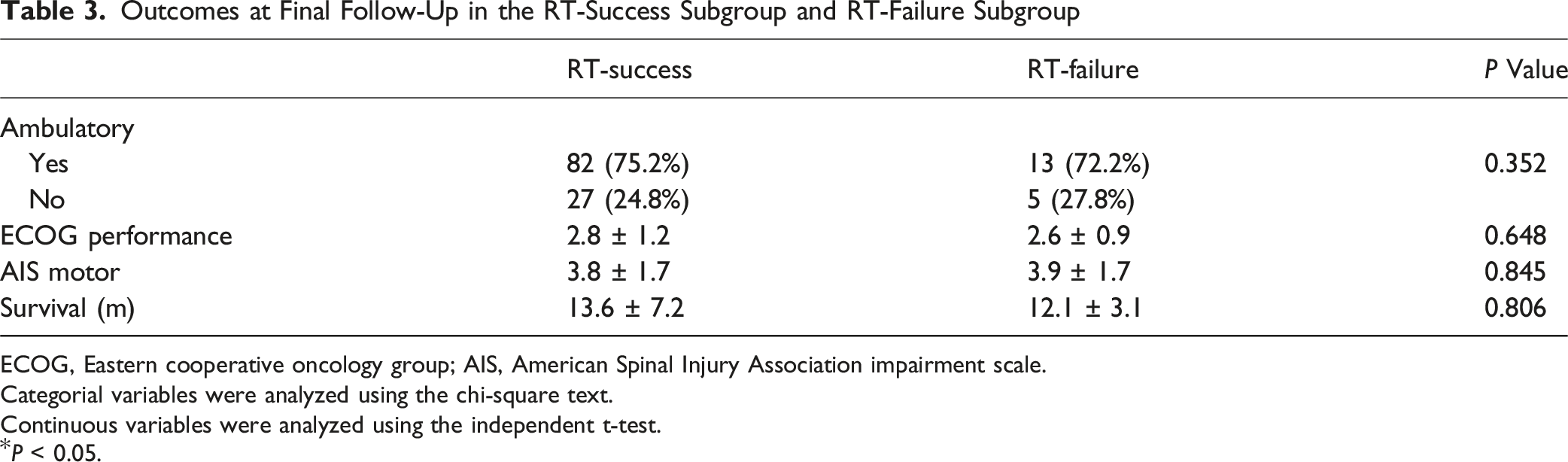
ECOG, Eastern cooperative oncology group; AIS, American Spinal Injury Association impairment scale.
Categorial variables were analyzed using the chi-square text.
Continuous variables were analyzed using the independent t-test.
*P < 0.05.
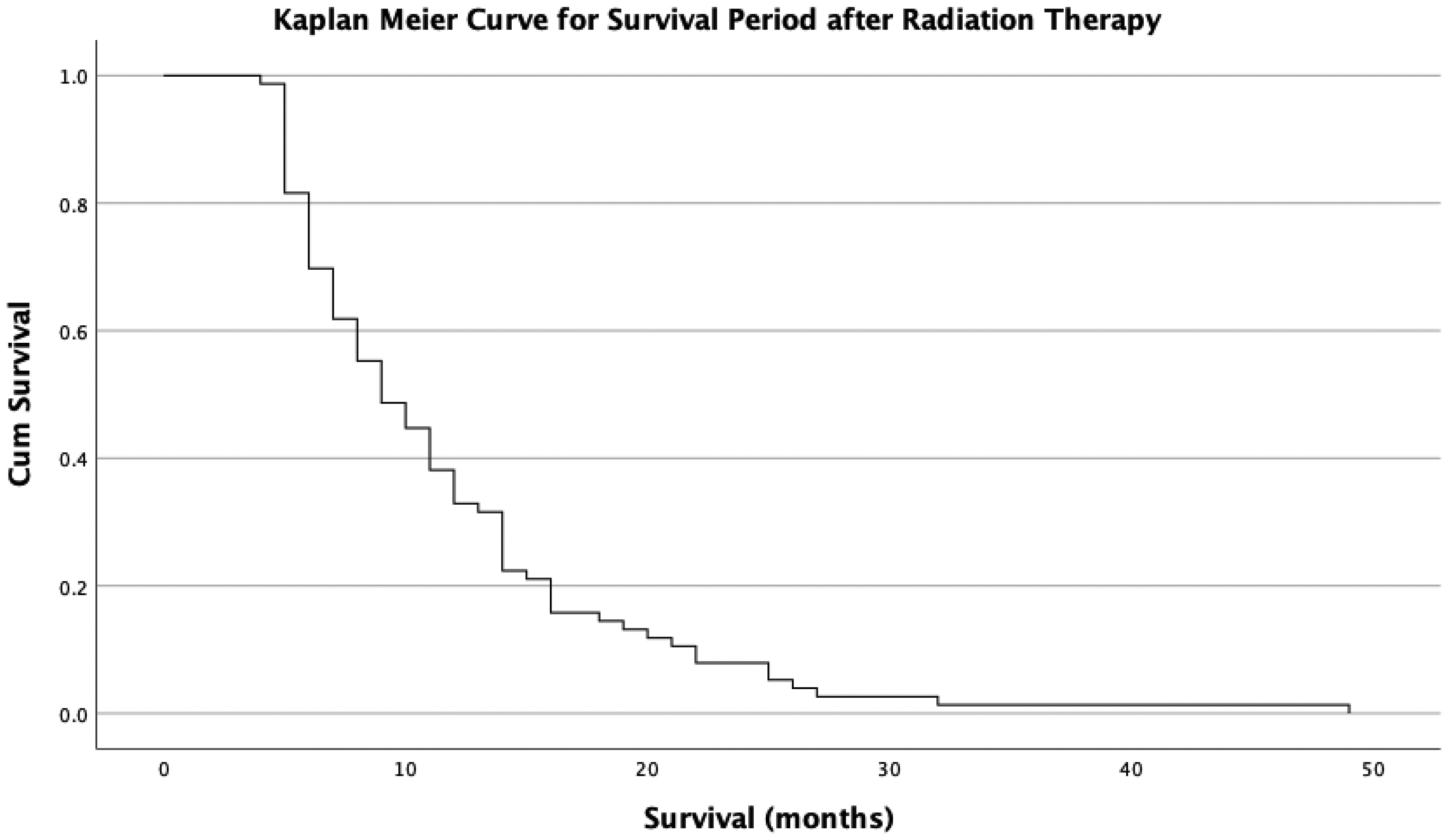
Kaplan-Meier Survival Curve of Patients in the RT-Success Group
Factors Associated with Failure of RT
Logistic Regression Analysis Demonstrating Factors Associated With the Need for Surgery After Initial RT
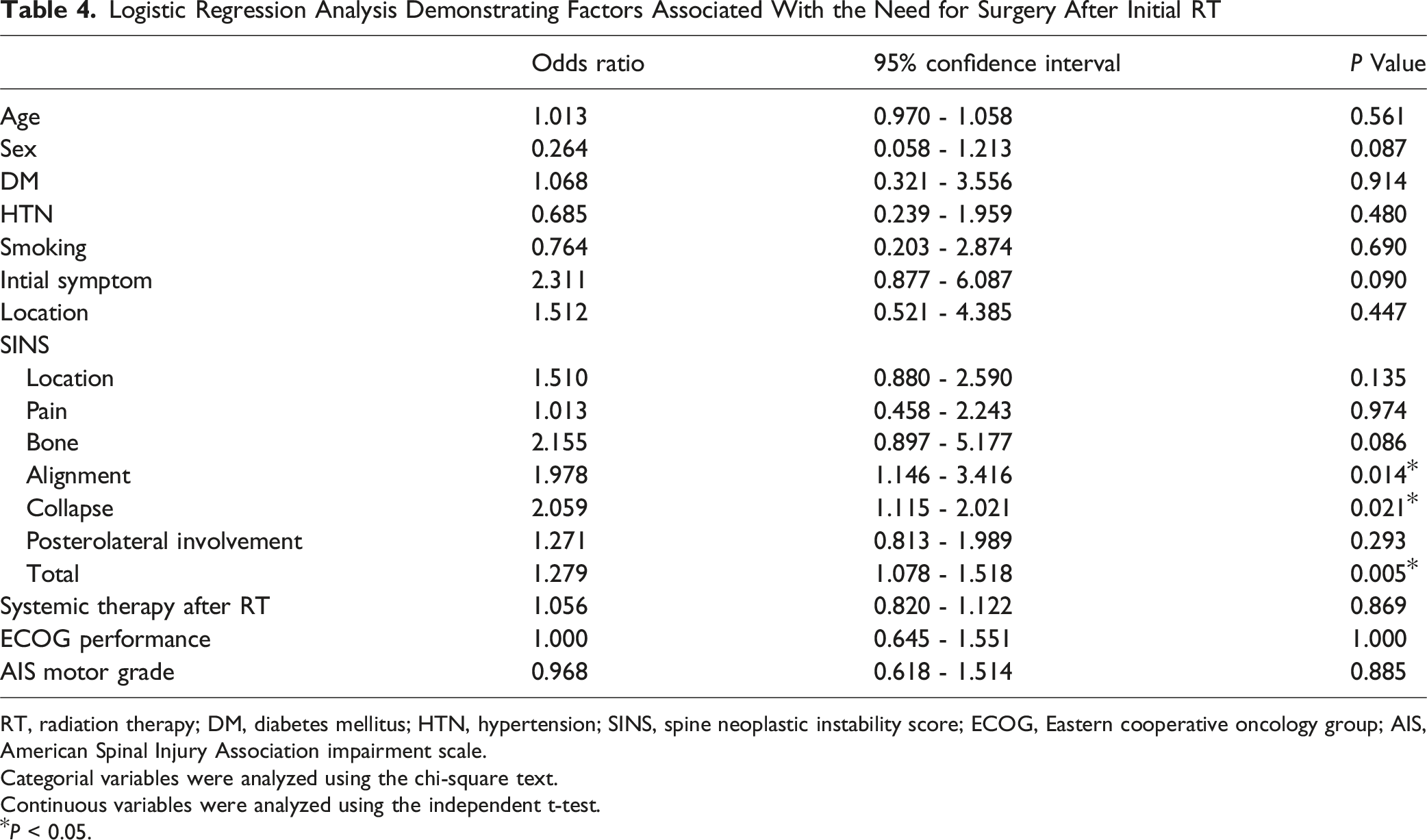
RT, radiation therapy; DM, diabetes mellitus; HTN, hypertension; SINS, spine neoplastic instability score; ECOG, Eastern cooperative oncology group; AIS, American Spinal Injury Association impairment scale.
Categorial variables were analyzed using the chi-square text.
Continuous variables were analyzed using the independent t-test.
*P < 0.05.
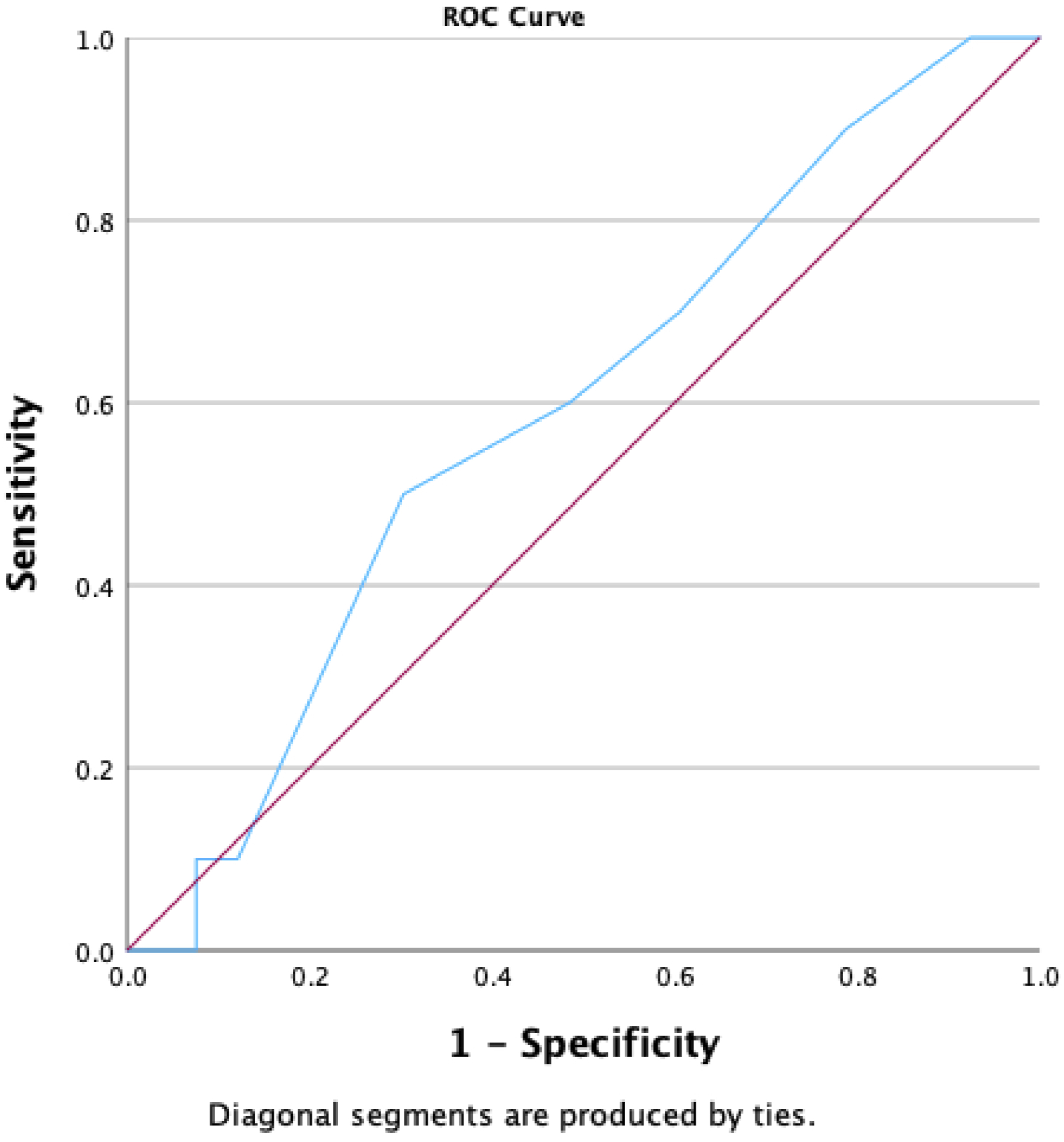
Receiver Operating Characteristics Curve for the SINS Score for Predicting Radiation Therapy Failure. SINS: Spinal Instability Neoplastic Score
Discussion
In the current study, 15.9% of patients diagnosed with Bilsky grade 2 MESCC were judged to need surgery at initial presentation. Patients who were younger but had worse performance and motor power tended to undergo surgery at the time of diagnosis. Among patients who were initially treated with RT, 85.8% did not need surgery for the rest of their survival, while 14.2% needed operative management due to progression of clinical symptoms caused by MESCC. The alignment, collapse, and total SINS were significantly associated with the risk of RT failure. Specifically, SINS >8 showed value in predicting RT failure. Outcomes at the final follow-up including ambulatory status, performance, and survival did not differ significantly between the RT-success and RT-failure subgroups.
Performing prophylactic decompressive surgery for MESCC in the absence of neurological deficits is often a challenging decision, since patients often present with multiple comorbidities and high risk of complications.1,16,17 Surgical damage to already fragile patients may shorten survival and worsen the quality of life.12,18 Therefore, selecting patients at high risk of developing progressive neurological deficit is crucial in the treatment of MESCC since they will benefit most from prophylactic surgery.3,5 Those who are not likely to require surgery during follow-up could be initially treated with RT considering the surgical morbidity and recent development of the RT technique.6,19
The current study was conducted under the hypothesis that each Bilsky grade of MESCC would have a differential prognosis, potentially guiding initial treatment modality selection. Previous studies have demonstrated that patients with Bilsky grade 2 or 3 MESCC are at high risk of rapidly progressive paralysis compared to those with Bilsky grade 1. 9 Oshima et al. demonstrated that patients with cord compression exceeding 50% of the circumferential ratio are at a high risk of paralysis. 20 Uei et al. reported that 30% of patients with Bilsky grade 2 or 3 develop neurological deficit during follow-up. 21 The present study focused on Bilsky grade 2 which is the intermediate grade of MESCC and may have a different prognosis than grade 3.
The present study demonstrated that the success rate of RT as the initial choice for grade 2 MESCC was 85.8%. This can be considered high considering the operative morbidity, surgical complication risk, and need to cease chemotherapy when surgical treatment is performed.8,9,11,12 Although RT is also accompanied by the risk of complications including radiation-induced myelopathy and compression fracture, patients often tolerate RT better than surgery.22-24 Therefore, RT could be considered as the initial treatment for grade 2 MESCC when there is no neurological deficit or severe mechanical pain at onset. The result of the current study that functional outcomes at final follow-up were not adversely affected when surgery was performed at the time of RT failure, also supports the application of RT as the initial treatment method. Patel et al. also demonstrated that RT could provide excellent local control for high grade MESCC with a cumulative local recurrence rate of 14.1% within 2 years. 25 Such a treatment approach for grade 2 MESCC may be distinct from that for grade 3 MESCC, in which the risk of RT failure is higher. Kim et al reported that the local progression rate after RT was 9.5% for grade 2 MESCC and 24.9% for grade 3. 5 This might be attributed to the severity and difficulty in identifying safe radiation field in grade 3. The result of the current study contradicts that of level 1 study conducted by Patchell et al. comparing surgery and RT as initial treatment for MESCC. That study suggested that initial surgery followed by postoperative RT yields a better prognosis compared to RT as the initial treatment modality. 3 However, this study did not classify MESCC according to cord compression grade, which limits its applicability in clinical practice.
Nevertheless, 14.2% patients experienced local progression despite RT, necessitating surgery. Therefore, this risk should be discussed with patients and caregivers when choosing RT as the initial treatment for grade 2 MESCC. Furthermore, greater spinal instability as represented by SINS >8 increased the risk of RT failure. Moreover, poor spinal alignment and greater vertebral body collapse increased the RT failure risk. Spinal column instability and pathologic vertebral compression fracture could exert dynamic compressive force over the spine during weight bearing, which would increase the risk of myelopathy. 26 This result coincides with that of a recent study by Versteeg et al, who demonstrated that patients with SINS >7 would benefit significantly from surgical stabilization. 27 Lam et al and McKibben et al also demonstrated that greater SINSs are a potential risk factor for RT failure.22,23,28 Hence, when there is significant spinal instability combined with grade 2 MESCC, surgical treatment could be considered as the initial treatment, due to a higher risk of RT failure. 27
Limitations
Our study has a few limitations. First, we did not consider the radiosensitivity of the pathology. Radiosensitivity is a crucial factor when choosing RT, as even tumors with a high degree of cord compression with high radiosensitivity could be treated with RT.2,16,29 Since radiosensitivity was not included in the risk factor analysis in this study, only radiographic findings such as the SINS demonstrated significant results. However, radiosensitivity could not be quantified for each patient, which is also the case in actual clinical practice. 16 While tumors may be radiosensitive or radioresistant, the actual tumor response to RT cannot be predicted before performing RT. The results of the present study should be verified with future investigation considering radiosensitivity. Second, the treatment method was not chosen based on defined criteria. Multiple factors including the patient’s desire and comorbidities were considered based on individual assessment. In the same context, randomization for selecting initial treatment method was not possible, which could lead to potential bias. Third, the MESCC grade after RT was not evaluated since post-RT MRI was not routinely performed if the symptoms were not aggravated. Fourth, the initial radiologist diagnosis and surgeon’s reassessment of the MESCC Bilsky grade lacked complete agreement. However, since the agreement rate was high (89.4%) and the discrimination between grades 1c, 2, and 3 could have been influenced by some degree of interobserver variability, all patients who were initially diagnosed as grade 2 were included in this study.
Conclusion
Overall, 85.8% patients who were initially treated with RT for grade 2 MESCC did not require additional surgery during follow-up. Therefore, in the absence of neurological deficit or intractable mechanical pain at initial presentation, patients with Bilsky grade 2 MESCC should first receive RT. However, when there is significant instability as suggested by SINSs >8, surgery could be considered as the initial treatment method since greater instability is associated with a higher risk of RT failure.
Supplemental Material
Supplemental Material - Treatment Approach for Bilsky Grade 2 Metastatic Epidural Spinal Cord Compression Based on Radiation Therapy Failure Risk
Supplemental Material for Treatment Approach for Bilsky Grade 2 Metastatic Epidural Spinal Cord Compression Based on Radiation Therapy Failure Risk by Sehan Park, Dong-Ho Lee, Chang Ju Hwang, Gumin Jeong, Ji Uk Choi, Hyuk-Joon Sohn, San Kim, Yeon Joo Kim, and Jae Hwan Cho, MD, PhD in Global Spine Journal
Footnotes
Ethical Considerations
This study was approved by our facility’s Institutional Review Board. (IRB approval number: 2024-0615)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.