
Abstract
Study Design
This study is a retrospective review.
Objective
Central sensitization (CS) is a neurological phenomenon that involves hypersensitivity of the central nervous system. The central sensitization inventory (CSI) was developed as a screening tool to assess CS-related symptoms. The purpose of this study was to evaluate the association of preoperative CSI scores with patient-reported outcome measures (PROMs) including neurological symptoms for patients who underwent spine surgeries in a multicenter study.
Methods
A consecutive 673 patients who underwent spine surgery at 8 different institutions were included in this study. Preoperative CSI scores were assessed for all subjects. The participants completed the following PROMs: the Oswestry Disability Index (ODI), the Japanese Orthopaedic Association (JOA) back pain evaluation questionnaire (JOABPEQ) for lumbar spinal diseases, and the JOA cervical myelopathy evaluation questionnaire (JOACMEQ) for cervical spinal diseases. The association of CSI scores with PROMs was statistically evaluated.
Results
The average CSI score for the total subjects was 23.6 ± 13.5. The subjects with CS-related symptoms (CSI ≥ 40) were 13.2% (n = 89). The CSI score showed a significant and weak-to-moderate correlation with the PROMs including neurological symptoms that included all the domains of the JOACMEQ for cervical spinal diseases, and JOABPEQ and ODI for lumbar spinal diseases. Among these, psychological factors had the most influence on the correlation with CSI score.
Conclusion
Central sensitization evaluated by the CSI is related to neurological symptoms and health-related quality of life in patients undergoing elective spine surgery.
Keywords
Introduction
Central sensitization (CS), which is a neurological phenomenon that involves hyper sensitization of the central nervous system, is defined as the increased responsiveness of nociceptive neurons in the central nervous system to normal or subthreshold afferent input. 1 Central sensitization has been proposed as an underlying mechanism of chronic pain conditions, including restless leg syndrome, fibromyalgia, and irritable bowel syndrome. 2 It has recently been reported that CS is also related to the mechanism of pain generation in musculoskeletal disorders,3-6 including osteoarthritis 7 and low back pain.8,9 Interestingly, CS-related pain disorders often share symptoms, including anxiety, depression, headache, fatigue, and sleeplessness, with central sensitization syndrome (CSS). 2 Based on these symptoms, the central sensitization inventory (CSI) was developed as a screening tool to assess CS-related symptoms. 2 The CSI has recently been widely used in clinical research, and its excellent internal consistency, reliability, and content validity has been reported. 10
The central sensitization inventory score has been reported to be significantly associated with pain-related disability and quality of life (QOL) of patients with musculoskeletal disorders.5,11 However, few reports are available on whether CS, including CSI evaluation, is related to the neurological symptoms caused by central or peripheral nervous system disorders resulting from spinal diseases. Recently, Bennet et al 12 evaluated the CSI scores of 664 patients who underwent spinal fusion surgery and reported that a preoperative high CSI score was associated with worse QOL outcomes and increased length of hospital stay. These authors suggest that a preoperative CSI score can be used as an additional outcome measure for assessing successful surgical outcomes of spinal fusion surgery. Therefore, we hypothesized the possibility that evaluation of preoperative CSI scores for spinal diseases, including those of the cervical, thoracic, and lumbar spine, would be of importance for appropriate patient selection and the prediction of surgical outcomes.
The purpose of this preliminary study was to evaluate the association of preoperative CSI scores with patient-reported outcome measures (PROMs), including neurological symptoms and health-related QOL, for patients undergoing elective spinal surgeries in a multicenter study.
Material and Methods
Study Design and Setting
This is a retrospective review of prospectively collected data from a multicenter cohort study. This study was approved by the Institutional Ethics Committee (IRB reference number: H2020-028). Informed consent was obtained in the form of opt-out on the website.
Participants
Consecutive patients undergoing spinal surgery at 8 different institutions from January 2019 to April 2020 were included in this study. Patients who underwent spine surgeries because of adolescent or congenital scoliosis, acute spinal injury, spinal hematoma, infection, and spinal metastasis were excluded from this study. 708 patients were initially included; however, 35 patients were excluded from the study because of missing more than one outcome measure. Finally, data of 673 subjects (425 males, 248 females; average age 65.0 ± 14.4) were analyzed for this study.
Measurement Properties
Demographic information, including age, gender, and spinal disease diagnosis, was collected. The location of spinal levels where spinal surgeries was classified into 3 locations: cervical, thoracic, and lumbar spine. The thoracolumbar level was included with those of the lumbar spine.
The participants completed the following PROMs preoperatively. The Japanese Orthopaedic Association (JOA) cervical myelopathy evaluation questionnaire (JOACMEQ) and original JOA score for cervical myelopathy were evaluated for the patients who underwent cervical surgeries. Oswestry Disability Index (ODI), JOA back pain evaluation questionnaire (JOABPEQ), and original JOA score for back pain were assessed for patients who underwent lumbar surgeries. The CSI was assessed for all subjects, including those receiving thoracic surgeries.
Central Sensitization Inventory
The CSI is a self‐reported measure for quantifying the extent of individual somatic and emotional complaints associated with CS. 2 The Japanese version of the CSI, the high reliability and validity of which has been reported, 6 was used in this study. The Japanese CSI is a 25‐item questionnaire to assess health‐related symptoms common in CS conditions, where each item can be scored on a 5‐point Likert scale ranging from 0 = “never” to 4 = “always.” The total score ranges from 0 to 100 points. CSI severity was classified into 5 categories according to the total score points as follows: (1) subclinical (0 to 29 points), (2) mild (30 to 39 points), (3) moderate (40 to 49 points), (4) severe (50 to 59 points), and (5) extreme (60 to 100 points). 13 A 40-point CSI score was used as a cut-off value to identify CSS. For evaluating the association between the CSI severity and PROMs, CSI severity was classified into 3 groups: subclinical (0 to 29 points), mild (30 to 39 points), and moderate to extreme (≥ 40) in this study.
Oswestry Disability Index
The ODI, scored from 0 to 100, is the questionnaire most used to assess LBP-related QOL with higher scores indicating worse condition. The ODI, developed by Fairbank et al 14 consists of 10 items that assess the level of pain and physical activities, including sleep, self-care, sex life, social life, and traveling. The Japanese version of the ODI, the high reliability and validity of which has been reported, 15 was used in this study. The total score, excluding the item for sex life, was analyzed in this study.
Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire
The JOACMEQ is a self-administered questionnaire for evaluation of specific outcome measures, including patient disability, handicaps, and general health of cervical myelopathy.16-21 The JOACMEQ comprises 24 questions in 5 domains: cervical spine function, upper extremity function, lower extremity function, bladder function, and QOL; and the range of the score for each domain is from 0 to 100, with higher scores indicating better condition.
The degree of pain or stiffness in the neck or shoulder, tightness in the chest, pain and numbness in the arms or hands, and pain or numbness from chest to toe was evaluated by a visual analogue scale (VAS) of 0 to 100 (mm), with 0 as “no pain or numbness at all” and 100 as “the most intense pain or numbness imaginable.”
Japanese Orthopaedic Association Back Pain Evaluation Questionnaire
The JOABPEQ measures multidimensional conditions of low back disorders, including pain intensity, disability, and QOL.17,18,22 The JOABPEQ is composed of 25 items across 5 subscales: LBP (4 items), lumbar function (6 items), walking ability (5 items), social life function (4 items), and mental health (7 items). The evaluation of scores for each domain is the same as that for the JOACMEQ.
The degree of LBP, pain in the buttocks and lower limb(s) and numbness in the buttocks and lower limb(s), was evaluated by a visual analogue scale (VAS) of 0 to 100 (mm), with 0 as “no pain or numbness at all” and 100 as “the most intense pain or numbness imaginable.”
Japanese Orthopaedic Association Score for Cervical Myelopathy
The JOA score 23 consists of 6 domain-scoring systems including the following: (1) motor dysfunction in the upper extremities, (2) motor dysfunction in the lower extremities, (3) sensory function in the upper extremities, (4) sensory function in the trunk, (5) sensory function in the lower extremities, and (6) bladder function, with the minimum total score of −2 to 17. Higher scores indicate better condition.
Japanese Orthopaedic Association Score for Back pain24,25
The JOA score was established and validated in 1986 for evaluating LBP and lumbar spinal diseases. The JOA score consists of 3 domains: subjective symptoms (0–9), clinical signs (0–6), activities of daily living (ADL) (0–14), and bladder function (0 to −6), with the minimum total score of −6 to the maximum total score of 29. Higher scores indicate better condition.
Statistical Analysis
Differences in the ratio between the spinal location and CSI severity groups were analyzed by chi-square test. Differences in age, CSI, ODI (%), and VAS (mm) were assessed for statistical significance by one-way analysis of variance (ANOVA), followed by the Bonferroni post-hoc test or unpaired T-test. Differences in each domain of the JOACMEQ and JOABPEQ were analyzed by the Kruskal–Wallis test or Mann–Whitney U test. Correlations between CSI and each parameter were evaluated using the Pearson’s correlation coefficient test or Spearman rank-order correlation test. Multiple regression analysis was performed to identify factors contributing to the scoring of CSI as a dependent variable with subject parameters. Significance was accepted at P < .05. All the statistical analyses were performed using IBM SPSS Statistics (IBM Japan, Tokyo).
Results
The CSI in Spinal Disorders
The average CSI score of the total 673 subjects was 23.6 ± 13.5. According to CSI severity group, the subjects were classified as subclinical 71.0% (n = 478), mild 15.8% (n = 106), moderate 8.3% (n = 56), severe 3.9% (n = 26), and extreme 1.0% (n = 7). The subjects with CSS (CSI ≥ 40) represented 13.2% (n = 89) of the total subjects. The average CSI score of women (27.4 ± 13.6) was significantly higher than that of men (21.6 ± 13.0, P < .0001). No significant correlation was found between age and CSI score (P = .07).
The number of patients who underwent cervical surgery was 130 (19.3% of the total), with thoracic surgery was 28 (4.2%), and with lumbar surgery was 515 (76.5%). A significant difference in CSI score was identified among the location of spinal diseases (P < .01) (Figure 1). The post-hoc test revealed that the CSI score of thoracic spinal diseases (30.3 ± 17.1) was significantly higher than that of lumbar spinal diseases (23.2 ± 12.7, P < .05, Figure 1). A similar trend identified between thoracic and cervical diseases (24.5 ± 15.5) did not achieve statistical significance (P = .13, Figure 1). Central Sensitization Inventory (CSI) score by spinal locations.** indicates P < 0.05.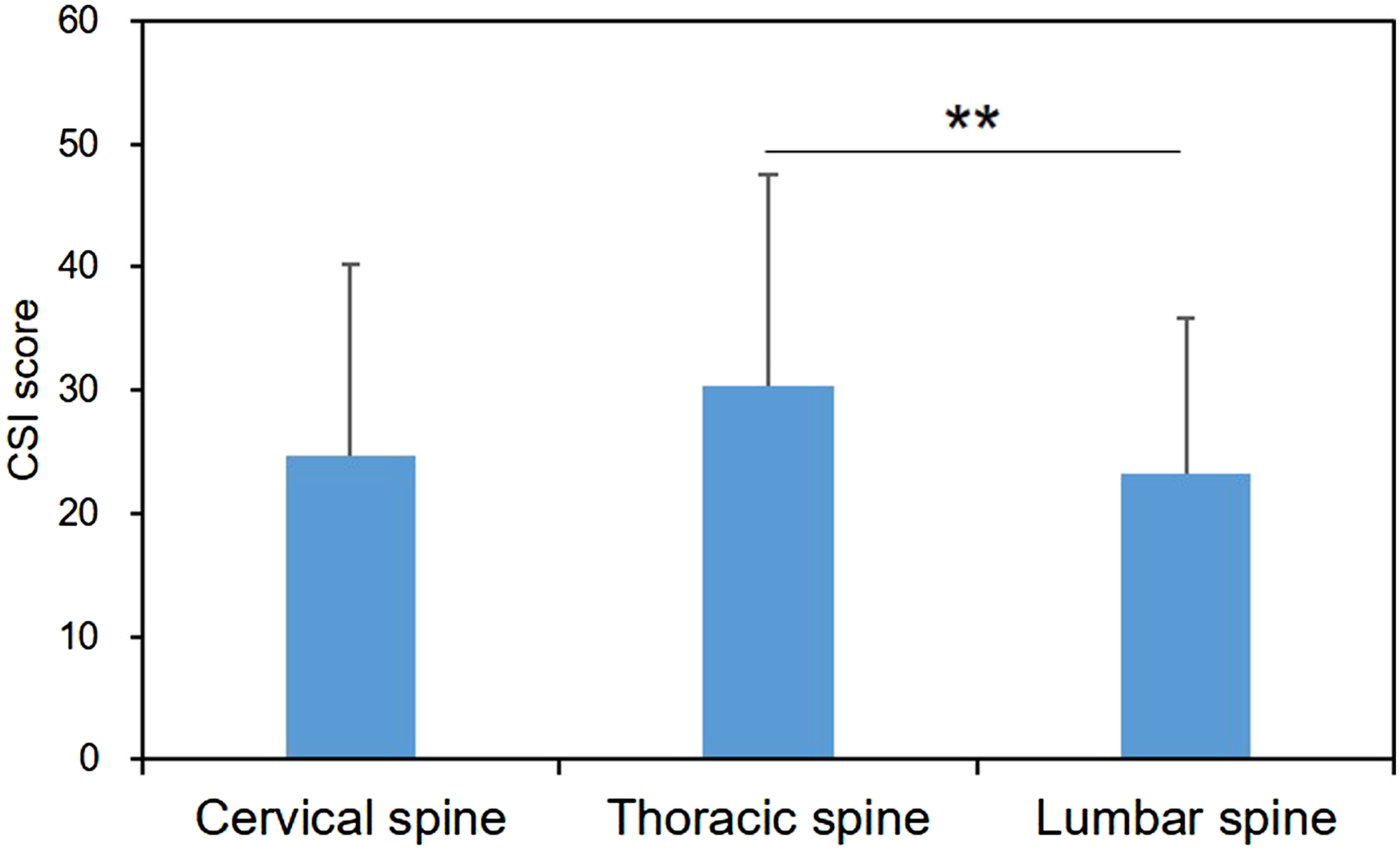
Central Sensitivity Inventory (CSI) score by spinal disease classification.
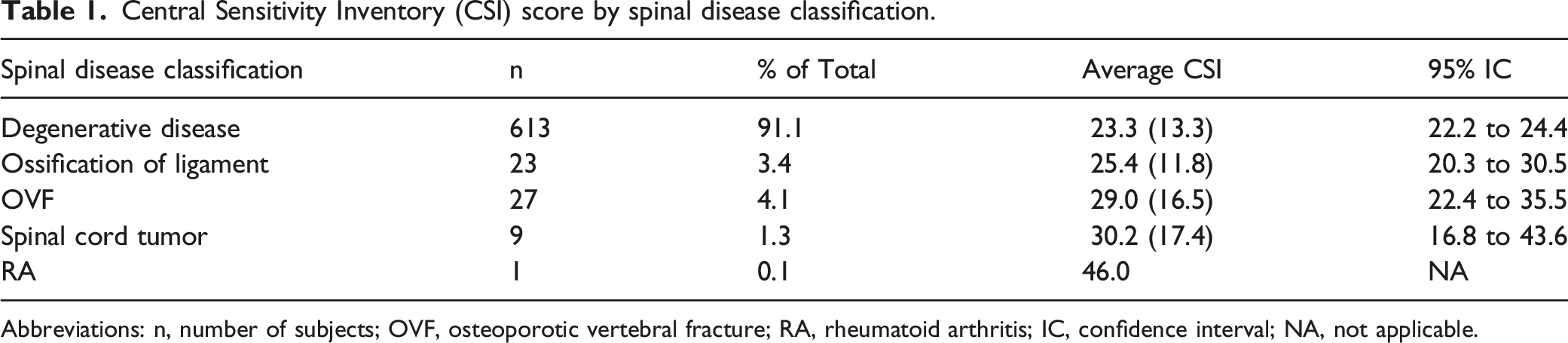
Abbreviations: n, number of subjects; OVF, osteoporotic vertebral fracture; RA, rheumatoid arthritis; IC, confidence interval; NA, not applicable.
Central Sensitivity Inventory (CSI) score by spinal diseases.
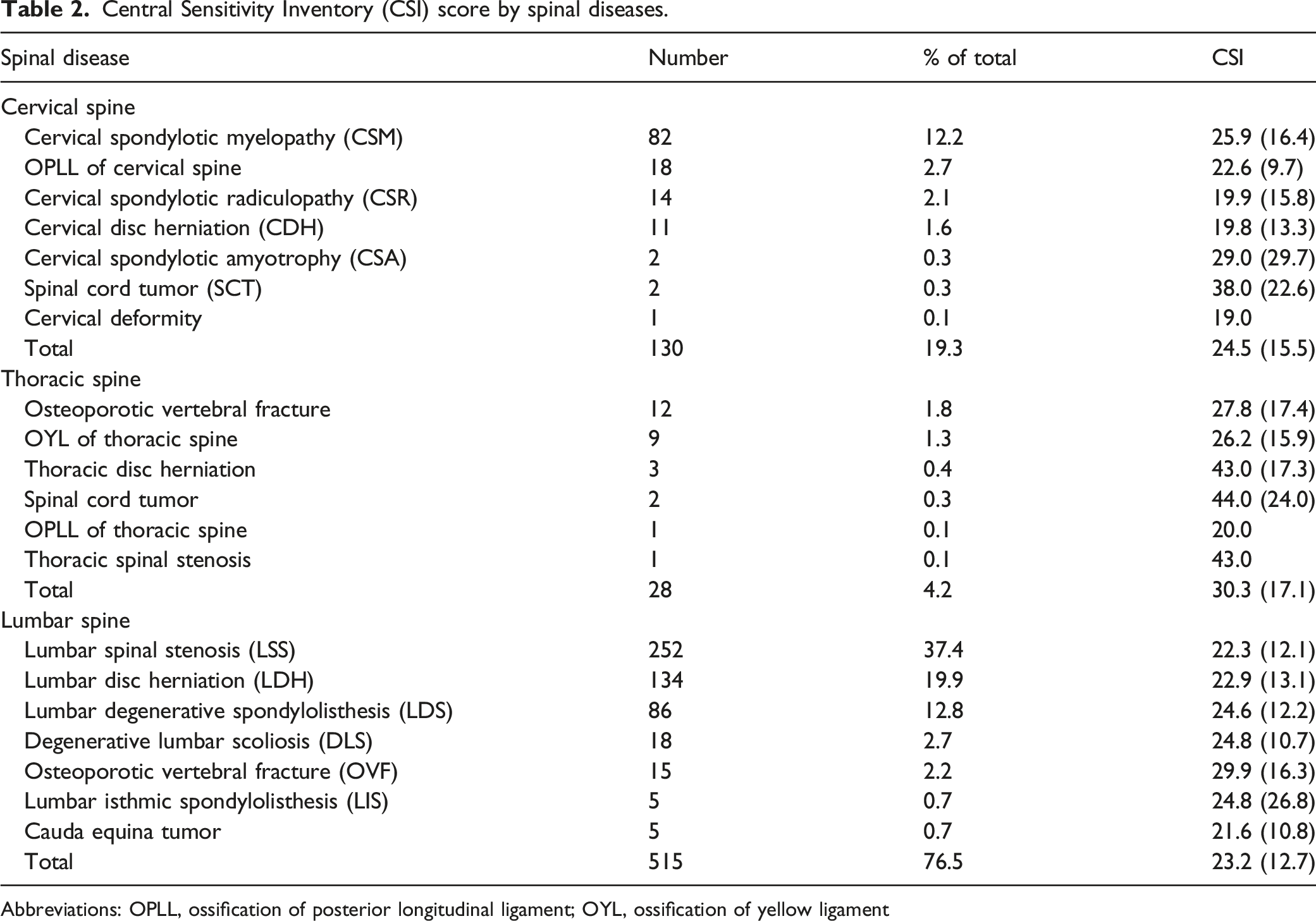
Abbreviations: OPLL, ossification of posterior longitudinal ligament; OYL, ossification of yellow ligament
Central Sensitization Inventory in Cervical Spine Diseases
Characteristics of patients with cervical spine diseases.
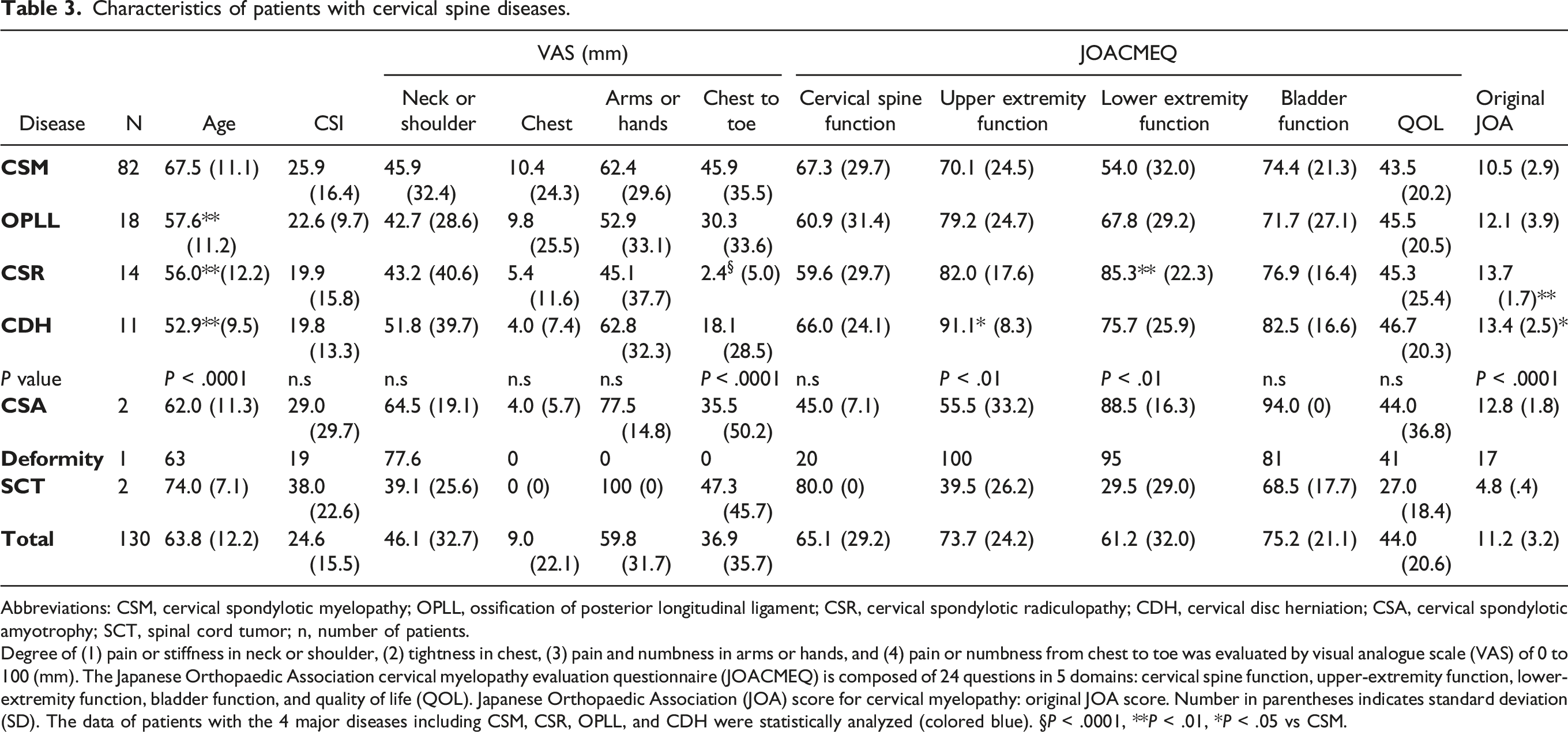
Abbreviations: CSM, cervical spondylotic myelopathy; OPLL, ossification of posterior longitudinal ligament; CSR, cervical spondylotic radiculopathy; CDH, cervical disc herniation; CSA, cervical spondylotic amyotrophy; SCT, spinal cord tumor; n, number of patients.
Degree of (1) pain or stiffness in neck or shoulder, (2) tightness in chest, (3) pain and numbness in arms or hands, and (4) pain or numbness from chest to toe was evaluated by visual analogue scale (VAS) of 0 to 100 (mm). The Japanese Orthopaedic Association cervical myelopathy evaluation questionnaire (JOACMEQ) is composed of 24 questions in 5 domains: cervical spine function, upper-extremity function, lower-extremity function, bladder function, and quality of life (QOL). Japanese Orthopaedic Association (JOA) score for cervical myelopathy: original JOA score. Number in parentheses indicates standard deviation (SD). The data of patients with the 4 major diseases including CSM, CSR, OPLL, and CDH were statistically analyzed (colored blue). §P < .0001, **P < .01, *P < .05 vs CSM.
Next, the subjects were divided into 3 groups according to CSI severity (subclinical (0 to 29 points), mild (30 to 39 points), and moderate to extreme (more than 40 points)) (Figure 2). There were no significant differences with the VAS in “chest” and “arms or hands” depending on the severity of CSI score. However, the VAS in “neck or shoulder” (P < .05), “from chest to toe” (P < .01), and all 5 domains of the JOACMEQ (P < .0001), and original JOA (P < .0001) differed significantly among the 3 CSI severity groups (Figure 2). Patient-reported outcome measures (PROMs) by severity of the Central Sensitization Inventory (CSI) in cervical spine diseases.The subjects were divided into 3 groups according to CSI severity (subclinical (0 to 29 points), mild (30 to 39 points), and moderate to extreme (more than 40 points)). Degree of (1) pain or stiffness in neck or shoulder, (2) tightness in chest, (3) pain and numbness in arms or hands, and (4) pain or numbness from chest to toe was evaluated by visual analogue scale (VAS) of 0 to 100 (mm). The Japanese Orthopaedic Association cervical myelopathy evaluation questionnaire (JOACMEQ) comprises 24 questions in 5 domains: cervical spine function, upper-extremity function, lower-extremity function, bladder function, and quality of life (QOL). The Japanese Orthopaedic Association (JOA) score for cervical myelopathy: original JOA score. *P < .05, **P < .01, § < .0001.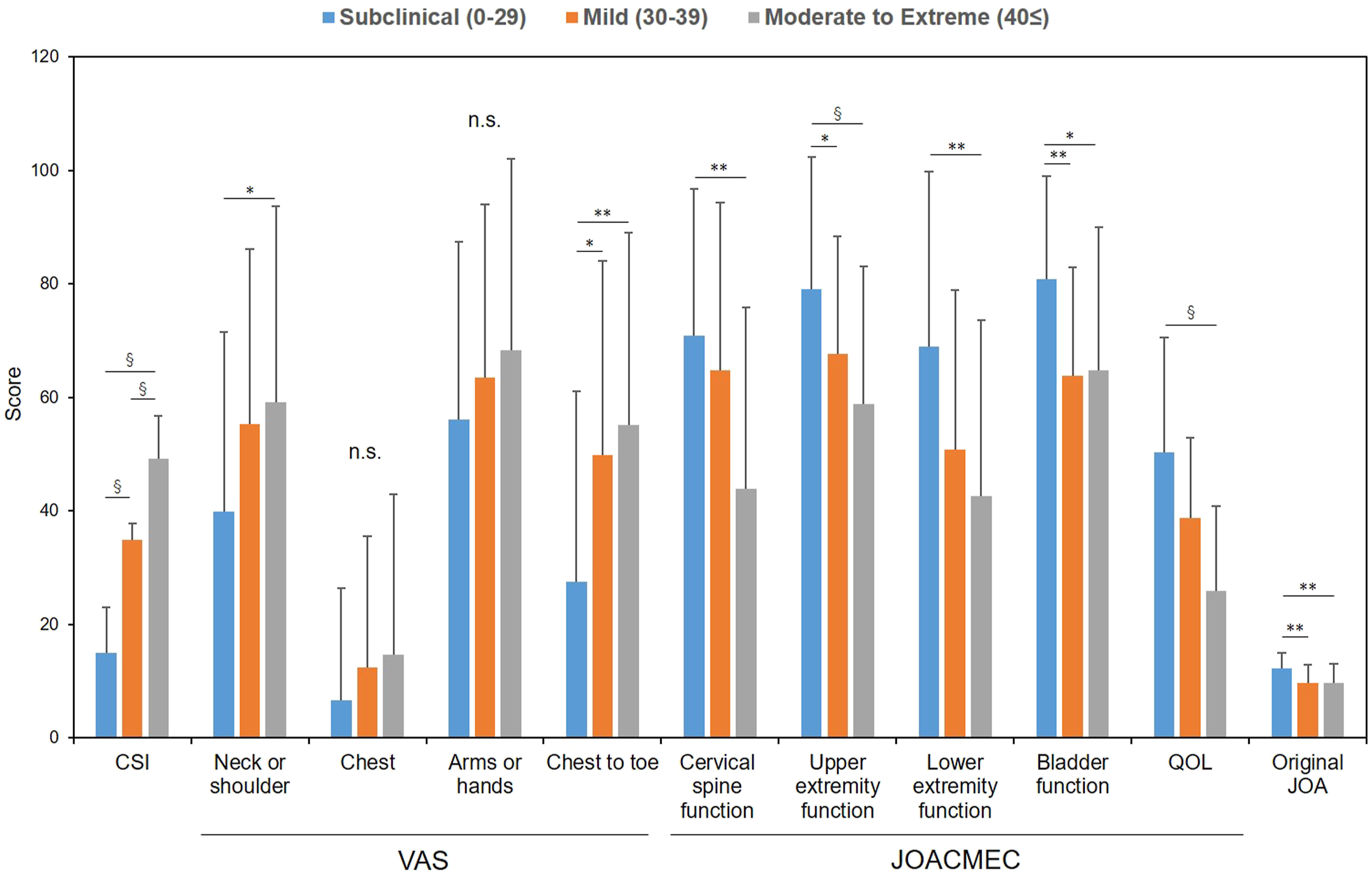
Pearson’s correlation coefficient analysis showed a significant, but weak correlation between CSI and VAS in “neck or shoulder” (r = .21, P < .05), “arms to hands” (r = .16, P < .05), and “chest to toe” (r = .35, P < .0001); however, there was no significant correlation of CSI score with VAS in chest (Figure 3A-D). A significant correlation between CSI and PROMs, including all 5 domains of the JOACMEC and original JOA, was identified (Figure 3E-J). Among the PROMS, a moderate correlation (r = .4 to .7) was found with bladder function (r = −.40, P < .0001) and QOL (r = −.58, P < .0001) of the JOACMEQ. Correlation between the Central Sensitization Inventory (CSI) and patient-reported outcome measures (PROMs) in cervical spine diseases.Degree of (A) pain or stiffness in neck or shoulder, (B) tightness in chest, (C) pain and numbness in arms or hands, and (D) pain or numbness from chest to toe was evaluated by a visual analogue scale (VAS) of 0 to 100 (mm). The Japanese Orthopaedic Association cervical myelopathy evaluation questionnaire (JOACMEQ) comprises 24 questions in 5 domains: cervical spine function (E), upper-extremity function (F), lower-extremity function (G), bladder function (H), and quality of life (I). The Japanese Orthopaedic Association (JOA) score for cervical myelopathy (original JOA score) (J). r: correlation coefficient.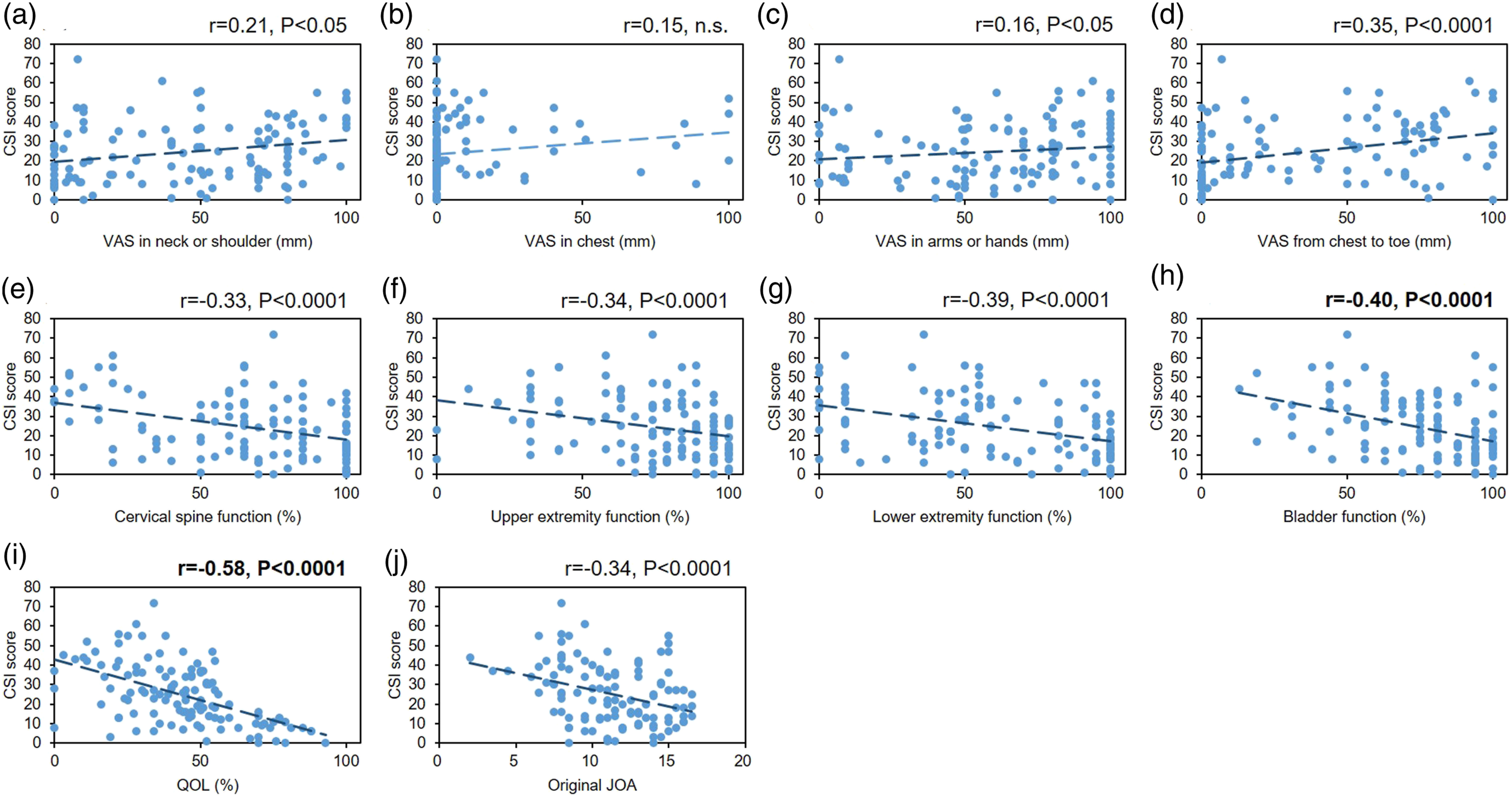
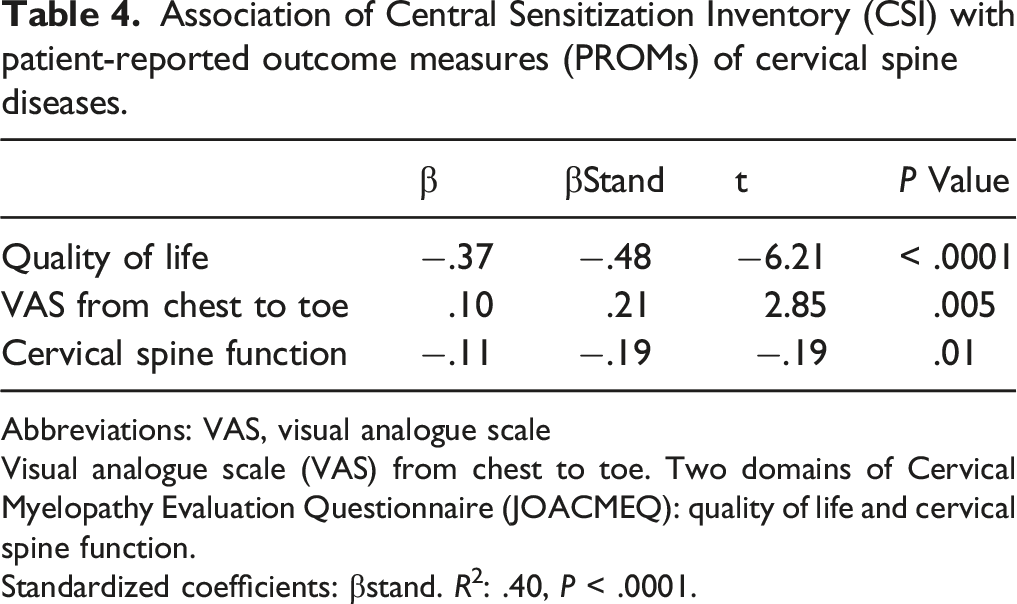
Association of Central Sensitization Inventory (CSI) with patient-reported outcome measures (PROMs) of cervical spine diseases.
Abbreviations: VAS, visual analogue scale
Visual analogue scale (VAS) from chest to toe. Two domains of Cervical Myelopathy Evaluation Questionnaire (JOACMEQ): quality of life and cervical spine function.
Standardized coefficients: βstand. R2: .40, P < .0001.
Central Sensitization Inventory in Lumbar Spine Diseases
Characteristics of patients with lumbar spine diseases.

Abbreviations: LSS, lumbar spinal stenosis; LDS, lumbar degenerative spondylolisthesis; LDH, lumbar disc herniation; DLS, degenerative lumbar scoliosis; LIS, lumbar isthmic spondylolisthesis; CET, cauda equina tumor; OVF, osteoporotic vertebral fracture; CSI, central sensitivity inventory; ODI, Oswestry Disability Index; VAS, visual analogue scale.
Degree of low back pain (LBP), pains in buttocks and lower limb(s), and numbness in buttocks and lower limb(s) was evaluated by a visual analogue scale (VAS) of 0 to 100 (mm). The Japanese Orthopaedic Association back pain evaluation questionnaire (JOABPEQ) is composed of 25 items across 5 domains: LBP, lumbar function, walking ability, social life function, and mental health. The Japanese Orthopaedic Association Score for Back Pain: original JOA. Five domains of the JOA Back Pain Evaluation Questionnaire: low back pain, lumbar function, walking ability, social life function, and mental health. The number in parentheses indicates standard deviation (SD). The data of patients with the 5 major lumbar diseases, including LSS, LDH, LDS, DLS, and OVF, were statistically analyzed (colored blue). §P < .0001, **P < .01, *P < .05 vs CSM.
When the subjects with lumbar diseases were divided into 3 groups according to CSI severity, ODI (P < .0001), VAS of low back pain (P < .01) and leg pain (P < .05), all 5 domains of the JOABPEQ (low back pain, lumbar function, walking ability, social life function, and mental health, all P < .0001), and original JOA (P < .0001) differed significantly by CSI severity groups (Figure 4). There were no significant differences on VAS of buttock and leg numbness by CSI severity group. Patient-reported outcome measures (PROMs) by severity of the Central Sensitization Inventory (CSI) in lumbar spine diseases.The subjects were divided into 3 groups according to CSI severity (subclinical (0 to 29 points), mild (30 to 39 points), and moderate to extreme (more than 40 points)). ODI: Oswestry Disability Index. The degree of “low back pain,” “pains in buttocks and lower limb(s),” and “numbness in buttocks and lower limb(s)” was evaluated by visual analogue scale (VAS) of 0 to 100 (mm). The Japanese Orthopaedic Association back pain evaluation questionnaire (JOABPEQ) is composed of 25 items across 5 domains: LBP, lumbar function, walking ability, social life function, and mental health. Japanese Orthopaedic Association Score for Back Pain: original JOA. *P < .05, **P < .01, § < .0001.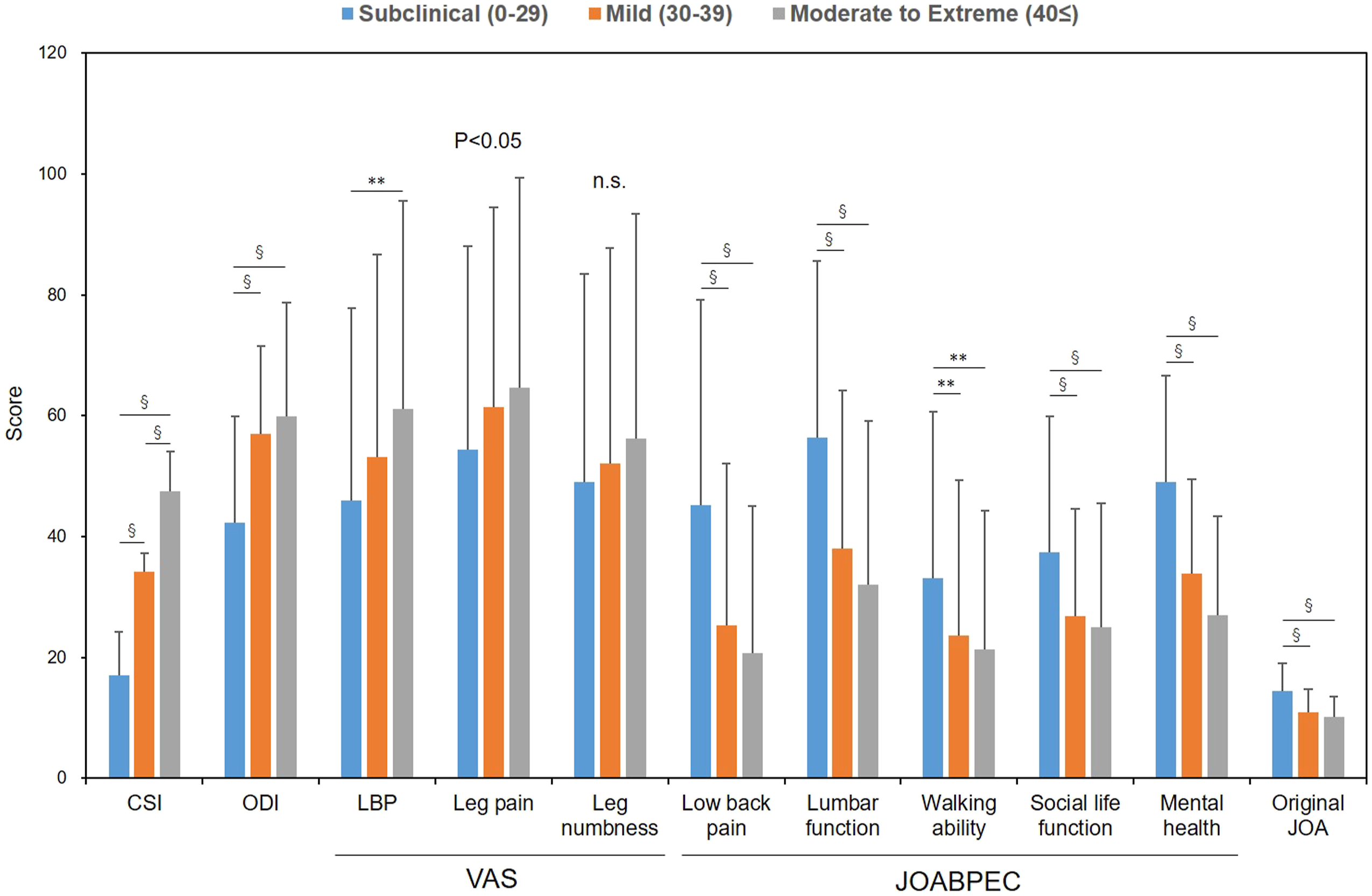
A significant, but weak, correlation was identified between CSI score and VAS of low back pain (r = .21, P < .0001), buttock and leg pain (r = .18, P < .0001), and buttock and leg numbness (r = .11, P < .0001) (Figure 5B-D). A significant, but weak, correlation was also found with the 4 domains of the JOABPEC, including the low back pain domain (r = −.34, P < .0001), lumbar function (r = −.33, P < .0001), walking ability (r = −.18, P < .0001), social life function (r = −.25, P < .0001) (Figure 5E-H), and original JOA (r = −.37, P < .0001, Figure 5J). A moderate correlation (r = .4 to .7) was identified with the ODI (r = −.41, P < .0001, Figure 5A) and mental health domain of the JOABPEQ (r = −.53, P < .0001, Figure 5I). Correlation between the Central Sensitization Inventory (CSI) and patient-reported outcome measures (PROMs) in lumbar spine diseases. (A) ODI: Oswestry Disability Index. Degree of (B) “low back pain”, (C) “pain in buttocks and lower limb(s)”, and (D) “numbness in buttocks and lower limb(s)” was evaluated by visual analog scale (VAS) of 0 to 100 (mm). The Japanese Orthopedic Association back pain evaluation questionnaire (JOABPEQ) is composed of 5 domains: (E) low back pain, (F) lumbar function, (G) walking ability, (H) social life function, (I) and mental health. (J) The Japanese Orthopaedic Association Score for Back Pain: original JOA. r: correlation coefficient.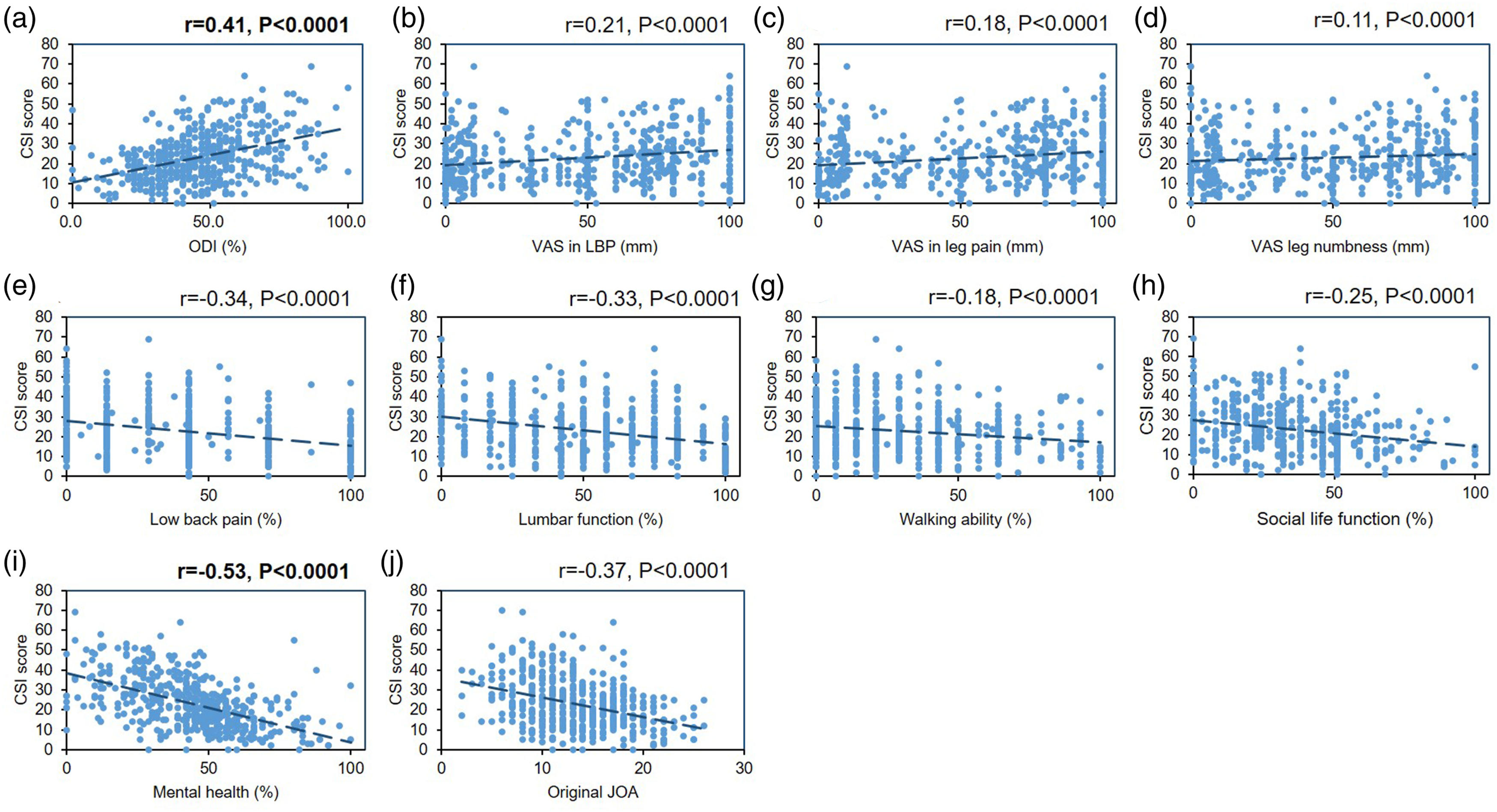
Association of the Central Sensitization Inventory (CSI) with patient-reported outcome measures (PROMs) of lumbar spine diseases.
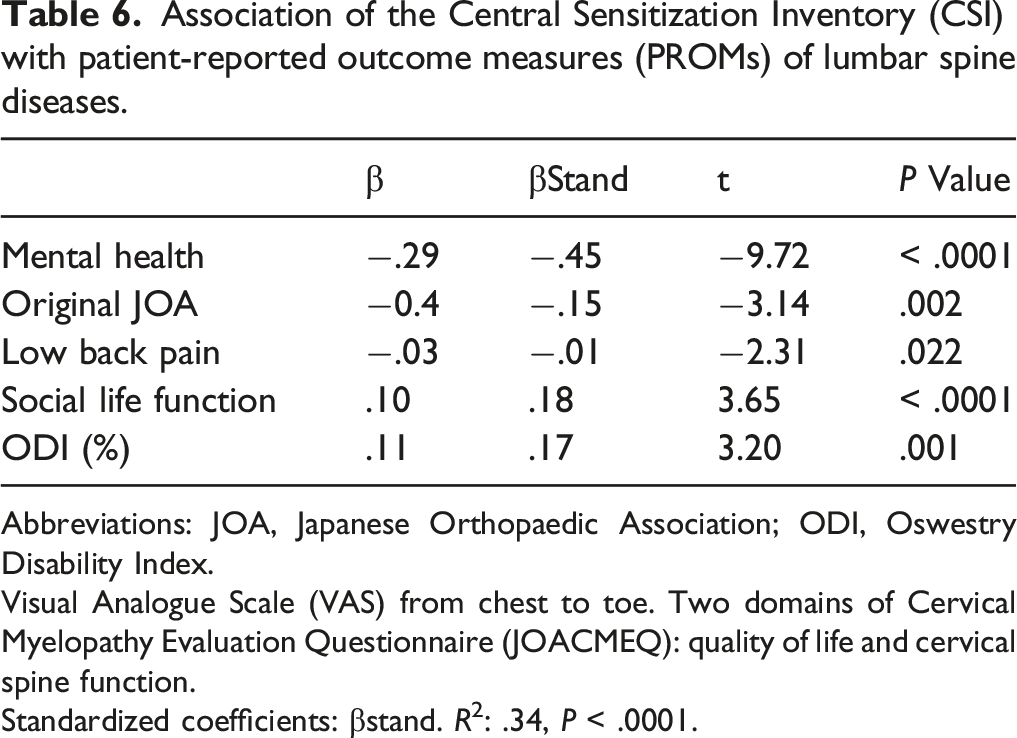
Abbreviations: JOA, Japanese Orthopaedic Association; ODI, Oswestry Disability Index.
Visual Analogue Scale (VAS) from chest to toe. Two domains of Cervical Myelopathy Evaluation Questionnaire (JOACMEQ): quality of life and cervical spine function.
Standardized coefficients: βstand. R2: .34, P < .0001.
Discussion
To determine the involvement of central sensitization (CS) with the neurological symptoms of chronic spinal diseases, the central sensitization inventory (CSI) was retrospectively evaluated for patients who underwent spinal surgeries in a multicenter study.
Our study showed that the average preoperative CSI score of the total subjects who underwent spinal surgeries for chronic spinal diseases was 23.6, with those subjects having a CSI score of more than 40 representing 13.2% of the total. Mibu et al 3 recently reported that the CSI score of 104 orthopedic clinic patients with chronic low back pain was 25.5. More recently, Miki et al 4 investigated the CSI score of 236 patients with degenerative lumbar diseases, and reported that the average CSI score was 24.4, with the percentage of their patients with a CSI score of more than 40 comprising 13.0% of the total. These previously reported data of spinal disease patients in the orthopedic fields were comparable with those of our study. On the other hand, Neblett et al 11 evaluated CSI scores in a cohort of patients with chronic spinal pain disorders who had been admitted to an interdisciplinary function restoration program; they showed the average CSI score of these patients was 45.8, with 53.1% having CS-related symptoms (CSI ≥ 40). This suggests that the CSI scores of chronic pain syndrome patients would be remarkably higher than those of chronic spinal disease patients who need a surgical and/or non-surgical orthopedic treatments. The population of patients in these 2 disciplines would differ significantly, including psychosocial status.
In our study, more than 90% of the patients had degenerative spinal diseases, and less than 5% had OVF, ossification of ligament diseases, or spinal tumors. CSI score of the latter 3 tended to be higher than that of degenerative spinal diseases; however, no significant changes were identified among the spinal diseases. The study authors speculate that, as the number of cases increases, statistically significant differences would be found.
The results of our study showed that the CSI score of thoracic spinal diseases was significantly higher than that of lumbar spinal diseases. The examination of the various thoracic diseases (Table 2) revealed the CSI score of OVF (27.8 ± 17.4), thoracic disc herniation (43.0 ± 17.3), and spinal cord tumor (44.0 ± 24.0) exhibited high CSI scores. The patients undergoing spinal surgery because of thoracic disc herniation exhibited an acute myelopathy with profound neurological deficit 26 and spinal cord tumor. These severe cases in the thoracic spinal diseases would have contributed to higher CSI scores.
In the cervical spinal diseases, the extent of pain evaluated by VAS in all 4 areas increased according to the severity of CSI; while a statistical significance was only identified in “neck or shoulder” and “from chest to toe,” these 2 areas showed a weak correlation (r = .2–.4) with CSI score. The CSI does not have questions asking about symptoms in the upper extremity, while CSI item 18 asks about muscle tension in the neck and shoulders, item 22 asks about uncomfortable and restless legs, and item 25 asks about pain in the pelvic area. Because these questions correspond to the VAS in “neck or shoulder” and “from chest to toe,” they would contribute to a significant correlation with the CSI score.
When evaluating the association of CSI score with the 5 domains of the JOACMEQ, the score of each domain significantly decreased according to CSI severity (Figure 2). “Cervical spine function,” “upper extremity function,” and “lower extremity function” showed a weak correlation with the CSI score, while “bladder function” exhibited a moderate correlation with CSI score. CSI item 11 and 21 ask about urological symptoms, sharing the question of “bladder function” with the JOACMEQ; this would be related to the moderate correlation of the JOACMEQ with the CSI score. Importantly, “QOL” showed the highest correlation (r = −.58) with CSI score among the 5 domains of the JOACMEQ. Questions within the QOL domain of the JOACMEQ ask about “discouragement,” “depression,” “exhaustion,” and “health status”; these are common to CSI items (1), (16), and (17) asking about emotional distress.
In patients with cervical spinal diseases, 18% were included in the subjects with CS-related symptoms (CSS) (CSI ≥ 40). The results of multiple regression analysis showed that “QOL,” “cervical spine function,” and “VAS of pain or numbness from chest to toe” were the independent factors that associated with CSI score; this suggests the possibility that the QOL of the patient, including psychological factors, sensory disturbance in the body and lower extremity, and also cervical spine motion has an influence on the patient’s CS.
In the lumbar spinal diseases, the number of subjects with LSS was highest, followed by those with LDH, LDS, DLS, and OVF; subjects with these 5 lumbar diseases accounted for 98% of the total lumbar spinal diseases. The CSI scores of LSS patients were lowest and highest in OVF patients, although no statistical significance was identified among the 5 diseases.
The ODI for assessing LBP-related QOL significantly increased according to CSI severity, and showed a moderate correlation (r = .41) with CSI score. Chiarotto et al 27 evaluated the correlation between ODI and CSI in a clinometric study targeted at chronic pain patients and showed a correlation coefficient (r) of .36, which is comparable to that of our study. Our results and those of Chiarotto et al 27 suggest that CSI may be of relevance to the QOL of patients that is associated with low back pain.
The scores of all 5 domains of the JOABPEQ significantly decreased according to CSI severity. Among these, “mental health” represented the highest correlation coefficient (r = −.53). The mental health domain of the JOABMEQ includes questions about “health condition,” “exhaustion.” and “depression,” which are similar to those of CSI items that ask about (3) anxiety attack, (4) exhaustion, (16) sadness or depression, and (17) low energy. These similarities between the JOABPEQ and the CSI would increase the correlation coefficient.
Subjects with lumbar spinal diseases with CS-related symptoms (CSI ≥ 40) represented 11.3% of the total subjects; this percentage was lower than that of subjects with cervical and thoracic spinal diseases. The results of multiple regression analysis suggest that not only the extent of low back pain and low back pain–related QOL, but also the psychological condition and social life would contribute to the extent of CS in the patients with lumbar spinal diseases.
Central sensitization has been defined as an amplification of neural signaling with the central nervous system that elicits pain hypersensitivity. 28 Central sensitization is also found in patients with musculoskeletal disorders, including chronic spinal disorders, and is associated with pain-related disability and QOL.5,11 However, little is known about whether CS is related to neuropathic symptoms caused by central or peripheral nervous system disorders due to spinal diseases. Theoretically, CS evaluated by the CSI should strongly correlate with the extent of neuropathic symptoms. Our results indicate that the extent of pain or numbness of patients with cervical and/or lumbar spinal diseases is significantly, but only weakly, correlated with the CSI score. The association between CS and neuropathic pain should be examined in the future. On the other hand, the CSI score showed a significant correlation with the PROMs that included the JOACMEQ, JOABMEQ, and ODI in this study. Previous studies also showed that CSI scores were significantly correlated with health-related patient-reported outcomes (HR-PROs) of patients with musculoskeletal disorders,3,4,6,11 as well as chronic pain syndrome (see review in Ref. 10). Tanaka et al 6 also reported that the Japanese version of the CSI scores were significantly correlated with the EuroQol 5-dimension (EQ-5D) (r = −.44). More recently, Miki et al 4 showed significant correlations between CSI scores, the Rolande Morris Disability Questionnaire (r = .28), and the EQ-5D (r = −.37). Importantly, our study identified that the best correlation of the CSI score is with psychological factors. The CSI itself involves many items regarding anxiety and depressive disorders. Van Wilgen et al 29 examined the convergent validity of the CSI by comparing the psychosocial factors and clinical features of CS in patients with chronic pain, and showed that psychological distress contributed significantly to the symptoms of CS.
There were several limitations to our study. First, the subjects of this study were limited to those with spinal diseases who underwent spinal surgeries; therefore, there is a great difference in the number of spinal diseases and the spinal levels. Second, the PROMs of our study were limited chiefly to the outcome assessment of spinal surgeries, and, therefore, general health-related QOL and specific assessments of psychosocial factors of our subjects were not examined. Thirdly, the duration of neurological symptoms until the treatment was not evaluated in this study; thereby, it might affect the extent of CS.
In conclusion, the authors established that CS evaluated by the CSI is related to neurological symptoms and health-related QOL in patients undergoing elective spine surgery. The extent of correlation was higher with health-related QOL, especially psychological factors, than the extent of neurological symptoms; this would be a characteristic feature of the CSI originating from the questions about CS-related symptoms. The results of this study would contribute to the next study that investigates the influence of the preoperative CSI score on surgical outcomes of spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.