
Abstract
Study Design:
Retrospective literature review of spine surgical site infection (SSI).
Objective:
To perform a review of SSI risk factors and more specifically, categorize them into patient and surgical factors.
Methods:
A review of published literature on SSI risk factors in adult spine surgery was performed. We included studies that reported risk factors for SSI in adult spinal surgery. Excluded are pediatric patient populations, systematic reviews, and meta-analyses. Overall, we identified 72 cohort studies, 1 controlled-cohort study, 1 matched-cohort study, 1 matched-paired cohort study, 12 case-controlled studies (CCS), 6 case series, and 1 cross-sectional study.
Results:
Patient-associated risk factors—diabetes mellitus, obesity (body mass index >35 kg/m2), subcutaneous fat thickness, multiple medical comorbidities, current smoker, and malnutrition were associated with SSI. Surgical associated factors—preoperative radiation/postoperative blood transfusion, combined anterior/posterior approach, surgical invasiveness, or levels of instrumentation were associated with increased SSI. There is mixed evidence of age, duration of surgery, surgical team, intraoperative blood loss, dural tear, and urinary tract infection/urinary catheter in association with SSI.
Conclusion:
SSIs are associated with many risk factors that can be patient or surgically related. Our review was able to identify important modifiable and nonmodifiable risk factors that can be essential in surgical planning and discussion with patients.
Introduction
Surgical site infection (SSI), with its associated morbidity, mortality, hospital length of stay (LOS), and cost, remains a common problem among spine surgery patients. The rate of SSI (superficial and deep) can range from 0.2% to 16.7%, depending on a number of patient-, pathology-, and procedure-related factors. 1,2 The treatment for SSI can be challenging requiring prolonged antibiotics, multiple revision surgeries, prolonged hospital stay, and in some patients, advanced soft tissue reconstructions. Numerous studies have attempted to identify the unique risk factors associated with SSI but are all too often limited to one specific diagnosis or procedure. Among previously identified factors associated with increased risk of SSI are excessive intraoperative blood loss, longer operative time, preoperative smoking, obesity, and higher degree of case complexity (as estimated by the Spine Surgery Invasiveness Index). 3 The purpose of this study is to perform a review of risk factors for spine SSI and to categorize them into patient- and surgical-related factors.
Methods
Study Design and Search Strategy
We conducted a review of all published literature discussing risk factors for SSI in adult spine surgery. The search was performed using PubMed from its inception to July 20, 2017. Search terms used were (risk factor) AND (surgical site infection) AND (spine).
Study Selection
We included studies that reported risk factors for SSI in adult spinal surgery. Exclusion criteria included those which reported on pediatric patient populations, systematic reviews, meta-analyses, those articles published in languages other than English or articles without an abstract.
Results
Search Results
The initial PubMed search returned 389 unique titles, of which 138 were included. Of those initially included, 1 was in a language other than English, 4 were meta-analyses, 18 were systematic reviews, 19 reported on pediatric populations, and 2 were excluded as full text could not be obtained. This left 94 unique studies for final and complete review.
Overview of Included Studies
A total of 72 cohort studies, 1 controlled-cohort study, 1 matched-cohort study, 1 matched-paired cohort study, 12 case-controlled studies (CCS), 6 case series, and 1 cross-sectional study were identified. A summary of these studies can be found in Table 1. Twenty-one studies evaluated only a single potential risk factor, while 73 studies evaluated multiple potential variables as risk factors. Variables identified as associated or not associated with SSI are summarized in Tables 2, 3, and 4, arranged by study.
Characteristics of Studies Included in Review.

Abbreviations: ACDF, anterior cervical discectomy and fusion; ASA, American Society of Anesthesiologists class; BMI, body mass index; CAD, coronary artery disease; CCS, case-controlled study; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CSF, cerebrospinal fluid; CVA, cerebrovascular accident; DM, diabetes mellitus; DVT, deep vein thrombosis; EBL, estimated blood loss; EtOH, alcohol use; GCS, Glasgow Coma Scale; HTN, hypertension; IA, inflammatory arthropathy; IVDU, intravenous drug use; LOS, length of stay; MI, myocardial infarction; MIS, minimally invasive surgery; MUST, Malnutrition Universal Screening Tool score; NNIS, National Nosocomial Infection Surveillance index; NS, not specified; NSAID, nonsteroidal anti-inflammatory drug; NSQIP, National Surgical Quality Improvement Program; OSA, obstructive sleep apnea; PE, pulmonary embolus; Pro, prospective; PVD, peripheral vascular disease; RA, rheumatoid arthritis; Retro, retrospective; SCI, spinal cord injury; SII, surgical invasiveness index; UTI, urinary tract infection; XLIF, extreme lateral interbody fusion. C, cervical; T, thoracic; L, lumbar; A, anterior; P, posterior; Comb, A/P combined.
Patient-Associated Variables and Association With Surgical Site Infection by Study.
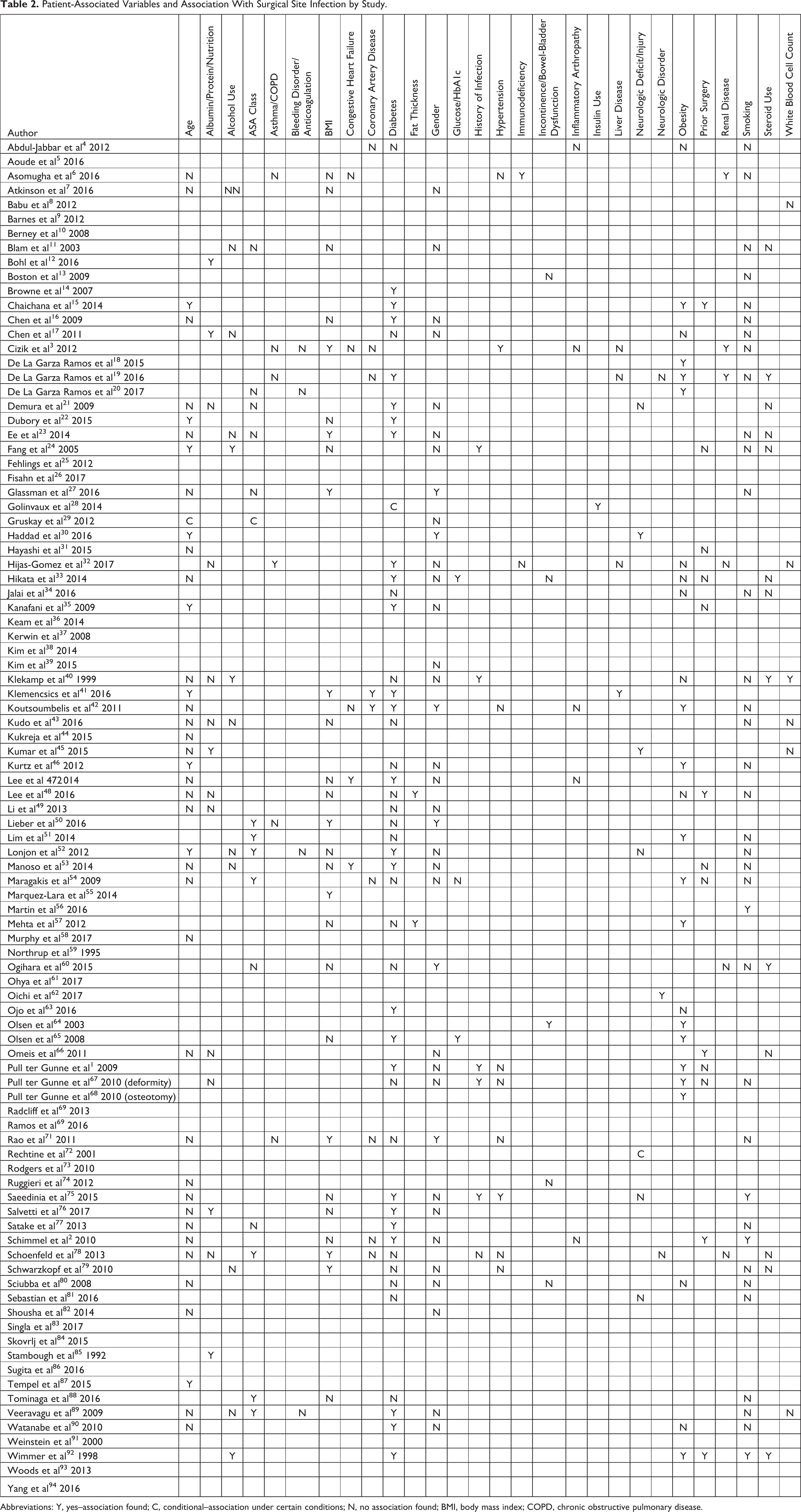
Abbreviations: Y, yes–association found; C, conditional–association under certain conditions; N, no association found; BMI, body mass index; COPD, chronic obstructive pulmonary disease.
Diagnosis-Associated Variables and Association With Surgical Site Infection by Study.
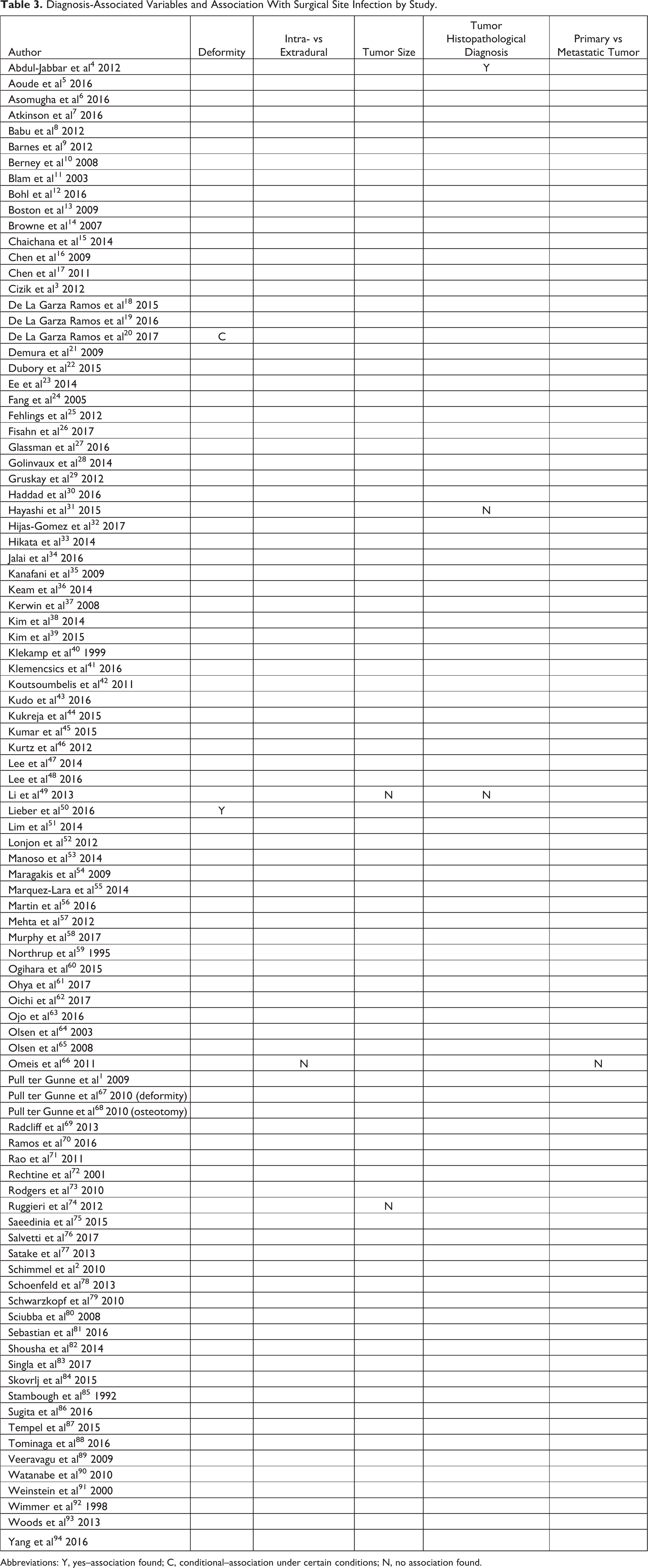
Abbreviations: Y, yes–association found; C, conditional–association under certain conditions; N, no association found.
Surgery-Associated Variables and Association With Surgical Site Infection by Study.
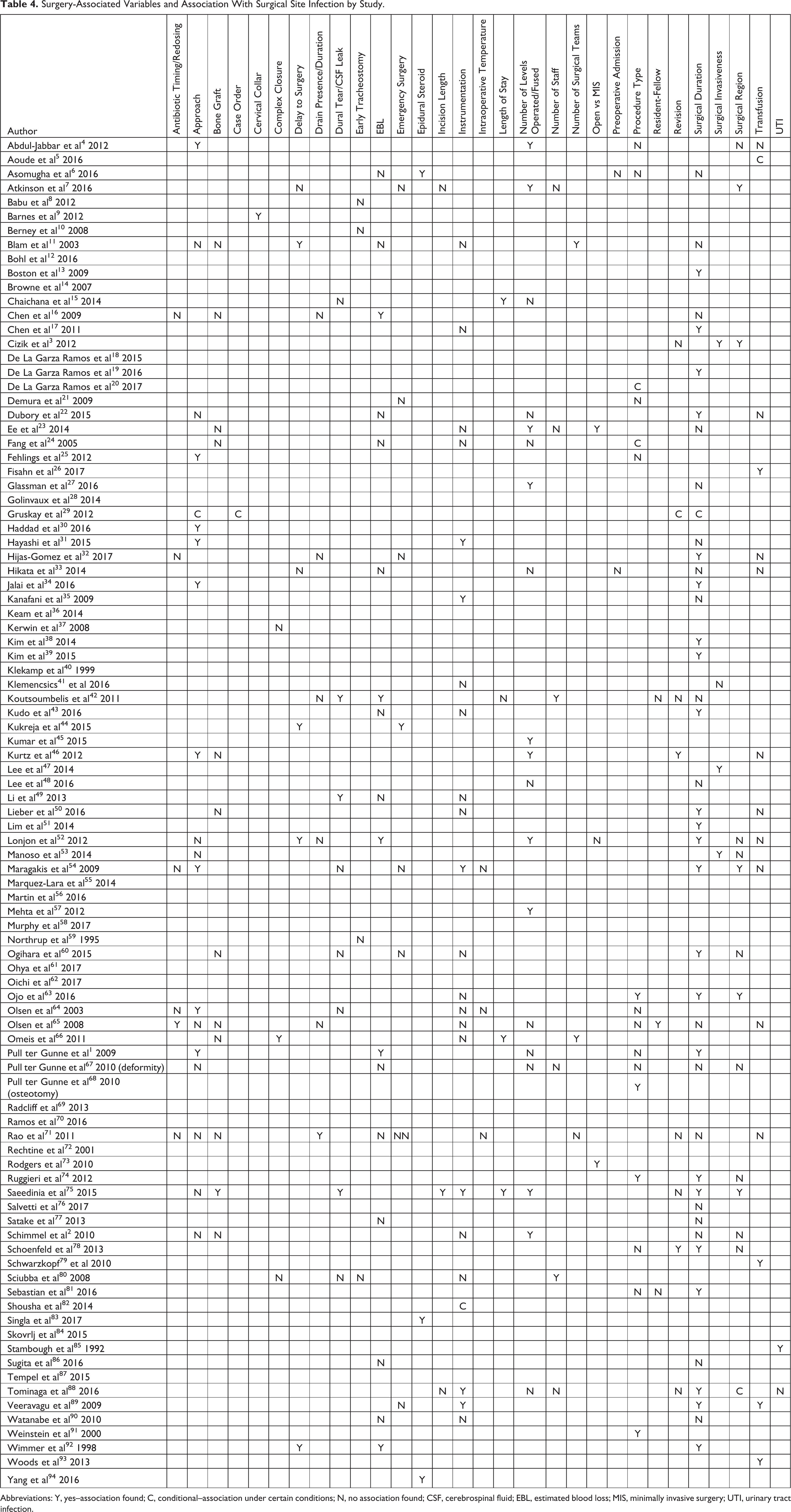
Abbreviations: Y, yes–association found; C, conditional–association under certain conditions; N, no association found; CSF, cerebrospinal fluid; EBL, estimated blood loss; MIS, minimally invasive surgery; UTI, urinary tract infection.
Patient-Associated Risk Factors
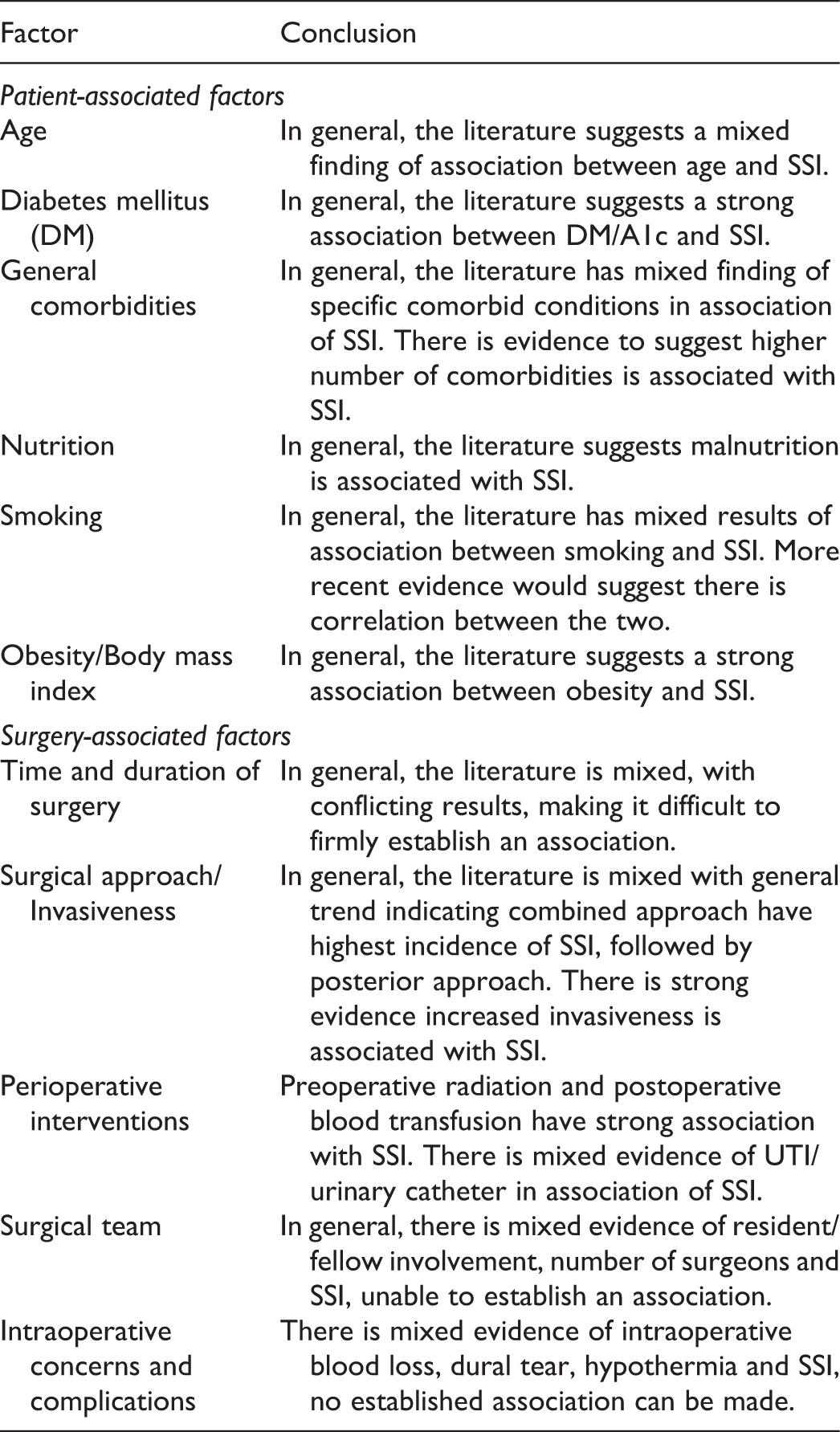
There were a number of modifiable and nonmodifiable patient-associated risk factors for SSI that were identified, including age, diabetes, nutritional status, smoking, and obesity.
Age
The relationship between patient age and the risk of SSI is not consistently reported in the literature, with numerous studies that implicating advanced age as a risk factor for SSI, and numerous studies finding no such association. Chaichana et al 15 reviewed 817 consecutive lumbar degenerative cases and found age of >70 years to be an independent risk factor for increased SSI. Manoso et al 53 found that Medicaid patients were at an increased risk for SSI but age alone was not an independent factor. In most studies, it was not possible to parse out the effect of age from other age-related comorbidities. Given the heterogeneity of results, it is not possible to definitively determine the role that age plays in the risk of SSI. The intuitive association between age and SSI is most likely related to other age-related comorbidities or the accumulation of co-morbidities that are globally manifest as patient frailty.
General Comorbidities
Koutsoumbelis et al 42 reviewed 3128 patients undergoing lumbar fusion at a single institution. The authors found several comorbidities that are associated with increased SSI, including diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), and osteoporosis. The hypothesis of osteoporosis and the association with SSI is thought to be related to loss of collagen in skin as well as bone, leading to aberrant wound healing. 42 Klemencsics et al 41 concluded that patients with DM, CAD, arrhythmia, chronic liver disease, and autoimmune disease were at a higher risk of SSI. Furthermore, patients with multiple comorbidities are at an increased risk for SSI. Kurtz et al 46 found that patients with Charleston comorbidity index (CCI) of 5 versus 0 had an adjusted hazard ratio of 2.48 in developing a postoperative SSI.
Diabetes Mellitus
It has been clearly established in the literature DM is an independent risk factor for SSI. There are several presumed pathophysiologies for this. Microvascular disease associated with DM can impair nutrition and oxygen delivery to the peripheral tissues and reduce the systemic ability to resist infection. Hyperglycemia can impair leukocyte functions such as adherence, chemotaxis, and phagocytosis. Furthermore, DM can lead to impaired collagen synthesis and fibroblast proliferation that delays wound healing. Browne et al 14 reviewed the Nationwide Inpatient Sample (NIS) database of 11 000 patients who underwent lumbar fusion. The reported that DM was associated with increased SSI, blood transfusion, increased LOS and nonroutine discharge. Chen et al 17 found that patients with DM had an adjusted relative risk of 4.1 of developing an SSI. Golinvaux et al 27 further delineated the risk factors by reporting that insulin dependent DM portends a higher SSI risk than non–insulin-dependent diabetes. In patients with the diagnosis of DM, preoperative glycemic control is essential in minimizing the risk of SSI. Since HbA1c reflects the average blood glucose over a period of 6 to 12 weeks, it is an important indicator of how well diabetes is being managed. Hikata et al 33 found that patients with DM had a higher rate of SSI than nondiabetics (16.7% vs 3.2%). Furthermore, while immediate perioperative glycemic control did not differ between those DM patients that did or did not develop an SSI, the immediate preoperative HbA1C was significantly higher in those who developed SSI (7.6%) than in those who did not (6.9%). In the same study, SSI developed in none of the patients with HbA1C <7.0% and in 35.5% of patients with HbA1C >7.0%. Thus, pre- and perioperative glycemic control are significant modifiable risk factors for SSI and should be part of a systematic infection prevention strategy.
Nutrition
There are several serum markers such as transferrin, prealbumin, albumin, total lymphocyte count that can be measured for early detection of nutritional deficits. Bohl et al 12 performed a retrospective review of the ACS-NSQIP database and found the overall prevalence of hypoalbuminemia (defined as <3.5 g/dL) as 4.8% in patients who underwent posterior lumbar fusion of 1 to 3 levels. The authors found patients with preoperative hypoalbuminemia had a higher risk of wound dehiscence, SSI and urinary traction infection. Furthermore, those patients also had longer inpatient stay and a higher risk of unplanned hospital readmission within 30 days of surgery. Chen et al 17 found that hypoalbuminemia was an independent risk factor for SSI in a cohort of patients who underwent sacral chordoma resection.
While albumin has been routinely used as a surrogate marker for nutritional status, recent studies have shown that prealbumin (half-life of 2 days) may also be used to assess a patient’s nutritional status in the perioperative period. Salvetti et al 76 found that preoperative prealbumin level of <20 mg/dL had higher risk of developing SSI with adjusted hazard ratio of 2.12. This collection of literature would suggest that for the reduction of SSI, it is advisable to assess nutritional status pre-operatively by checking prealbumin, albumin and total lymphocyte count. Nutritional supplementation may be considered if the patient is malnourished and undergoing complex surgical reconstruction.
Smoking
Nicotine leads to peripheral vasoconstriction and tissue hypoxia and results in impaired local angiogenesis and epithelialization. Smoking leads to decreased wound collagen production in in vitro and in animal studies. Martin et al 56 in 2016 found that active smokers are at a significantly higher risk of SSI compared with former smokers. That study from the ACS-NSQIP database, of patients who underwent elective lumbar surgery, categorized patients into: never smoked, former smoker (quit 12 months ago) and active smoker. Active smokers had a significantly higher risk of SSI compared with nonsmokers. Former smoker had an increased risk, but it was not significantly different from nonsmokers. Pack years of 1 to 20 and 20 to 40 were both found to have increased risk for SSI.
Obesity/Body Mass Index
Much has been studied about the relationship between obesity/body mass index (BMI) and SSI. Cizik et al 3 performed a retrospective review of all patients who had spine surgery at a single institution and found that BMI >35 kg/m2 was an independent risk factor for increased risk of SSI. In a retrospective cohort review, De la Garza-Ramos et al 18 found that obesity (BMI >30 kg/m2) resulted in an increased risk of SSI (risk ratio 3.11) in patients who underwent one to three level lumbar fusion surgery. Marquez-Lara et al 55 also found that BMI >30 kg/m2 (class I obesity) had increased risk of superficial wound infection. Furthermore, Mehta et al 57 found that body mass distribution, in particular increased skin to lamina distance and subcutaneous fat thickness, are independent risk factors for SSI. This study may indicate that although higher BMI is an independent risk factor associated with increased SSI, in patients with higher muscle mass, BMI may not be the most accurate variable to predict postoperative SSI. Lee et al 48 found that for every 1-mm of thickness in subcutaneous fat there was 6% increase in risk of SSI. Patients with at least 50 mm of posterior lumbar fat thickness had 4-fold increase in risk of SSI compared to those with less than 50 mm.
Surgery-Associated Risk Factors
Timing and Duration of Surgery
Most studies have found no significant association between “emergency surgery” and SSI. 7,21,31,52,54,60,71,89 Three studies have shown that increased duration from time of injury or admission to time of surgery was associated with increased risk of SSI. 11,44,52 Lonjon et al 52 found no association between the risk of SSI and surgery being done at night or after-hours.
A large number of studies have found that increased operative time increases the risk of SSI,* with a smaller number of contradicting studies. 6,11,16,23,27,35,48,67,71,86 Several studies used a cutoff of surgical duration in determining an association with SSI, although this varies between papers, ranging anywhere from 100 minutes to 5 hours, 13,24 and no conclusions can be made with regards to a specific duration as an inflection point in the risk for SSI.
Surgical Approach, Procedure, and Invasiveness
Surgical Approach: Anterior, Posterior, or Combined
If one considers studies that evaluate only cervical 25,30,34 or only lumbar procedures 2,46 separately, or separately analyzed approach in each spinal level subgroup, 28,64 most find an association between approach and SSI. In all studies with either cervical only groups or cervical subanalysis, 25,28,30,34,64 a posterior approach is consistently reported as a risk factor for SSI as compared with an anterior approach. Of those examining lumbar procedures, 2,28,46,64 for the most part, a combined anterior-posterior or posterior only approach was a risk factor for SSI as compared with anterior approach. Only 1 study had a thoracic subgroup analysis for approach, with Olsen et al 64 finding a posteriorly only approach to be associated with SSI as compared anterior alone. For the most part, those studies that have not found an association 11,22,52,65,68,71,75,77 have included a combination of cervical, thoracic, and lumbar procedures, which may confound the significance of approach given that the relative risk of an anterior versus posterior approach is different at various spinal levels. In those studies showing approach to be a risk factor for SSI, 1,4,25,28,30,31,34,46,54,64 the general trend is for a combined anterior-posterior approach to have the highest risk for SSI, followed by a posterior approach, with the anterior approach often reducing the risk for SSI.
Minimally Invasive Versus Open Surgery
Both Ee et al 23 and Rodgers et al 73 found that open surgery was associated with a higher risk of SSI as compared to MIS techniques (procedures performed through a tubular retractor system or extreme lateral interbody fusion (XLIF)) in elective lumbar spine surgery. Dubory et al 22 and Lonjon et al 52 found no such difference in SSI rates in spinal trauma. It should be noted the latter studies come from the same group, one of two that utilized only univariate analysis, and the type of MIS technique used was not defined, making it difficult to compare these results with those of either Ee et al 23 or Rodgers et al 73
Surgical “Invasiveness”
Surgical invasiveness can be considered a composite of a number of variables as previously described, including number of levels operated on, the type of procedure performed at each level, and approach used. To allow comparison of the invasiveness of disparate spinal procedures, a surgical invasiveness index (SII) was developed by Mirza et al. 95 This index is a composite score based on the number of vertebral levels operated on, the type of intervention on each vertebra—decompression, fusion, instrumentation—as well as the approach used at each level, and has been validated against both blood loss and surgical duration. Of the 4 studies that evaluated SII as a variable with regards to SSI, 3 found that an increase in SII was associated with SSI. 3,48,53 However, Klemencsics et al 1 found no such association. This may be related to the populations and procedure types studied, as Klemencsics et al 1 looked at elective routine degenerative lumbar procedures, with a maximal SII of 15, while the other 3 studies looked across a broad range of surgery types using large databases and presumed higher maximal SII scores. 3,48,53 If this is the case, the association between SII and SSI may only exist in the upper range of the SII.
Perioperative Interventions
Tracheostomy
Despite theoretical concerns, all 3 studies evaluating the potential of cross-contamination, have found no increased SSI risk for early tracheostomy (either pre- or postoperatively) in anterior cervical spine surgery. Babu et al 8 and Berney et al 10 found a low rate of SSI with early tracheostomy after anterior cervical stabilization for acute cervical trauma with spinal cord injury. Northrup et al, 59 in a review of 11 spinal cord injury patients, concluded that an existing tracheostomy was not a risk factor for SSI for subsequent anterior cervical spine stabilization.
Cervical Orthosis
Barnes et al 9 reported that the use of a Philadelphia collar for a minimum of 48 hours postoperatively increased the rate of SSI in posterior cervical spine surgery. This is in keeping with the known effects of pressure on skin and soft tissue from cervical orthoses. 96
Blood Transfusion
Transfusion is an independent risk factor for SSI in other surgical specialties, 97,39,98 and it has been strongly suggested to similarly be a risk factor in adult spine surgery. There exists some conflict in the literature to date, with a majority of studies finding a significant increase in SSI associated with transfusion, 4,5,28,61,79,89,93 but others finding it not to be of significance. 22,31,33,46,52,54,71 However, of those studies that have focused on the implications of blood transfusion in adult spine surgery, 5,28,79,93 all 4 have shown transfusion to be an independent risk factor for SSI. The association of transfusion with SSI has been thought to be a result of transfusion-related immunomodulation (TRIM), a phenomenon whereby antigens in blood products may result in T-cell unresponsiveness and subsequent immunosuppression. 99 Bacterial contamination of blood products are another potential explanation for the effects of transfusion on SSI. 100
Urinary tract infection (UTI) has been investigated as a possible source and hence risk factor for SSI, 88,101 and presence of a catheter is a well-established risk for UTI. 102 However, there has been limited study into urinary catheters as an independent risk factor for SSI in spine surgery, with both articles on this topic coming from the same group. 22,52 While Dubory et al 22 found that presence of a bladder catheter was not a significant risk for SSI after multivariate analysis, Lonjon et al 52 did find that a prolonged duration of catheterization greater than five days was associated with SSI after univariate analysis, although no multivariate analysis was performed. Based on these results, limited if any conclusion about urinary catheterization and SSI can be made.
Radiation is known to have deleterious effects on tissue, both in short-term effects on wound healing such as skin breakdown, lower tensile strength, and delayed healing rates from damage to epithelial cells and fibroblasts, 103 and in long-term effects on soft tissue resulting in fibrosis, poor vascularity, and a higher propensity to go onto atrophy or necrosis. 104 As such, preoperative radiation, whether recent or remote, has been regarded as a substantial risk factor for SSI. In nonsacral tumors, 3 studies focused on risk factors for SSI in spinal metastases or primary spinal tumors found preoperative radiation to be a significant risk for SSI. 21,66,86 In primary sacral tumors, the results have been more mixed, with 2 studies suggesting no significant association between previous radiation and SSI 17,80 against 1 study finding previous radiation to be a risk factor. 49 This is unsurprising, given the complexities of sacral tumor resection, higher infection rates, and smaller case numbers within each study by which to find association.
Evidence from a single controlled-cohort study suggests that use of epidural steroid paste in lumbar decompression is a risk factor for SSI, with the rate of SSI in the steroid paste group being 5.83% as compared to 1.11% in the control group. 5 . Two studies from the same institution have shown preoperative lumbar epidural injections, if within 3 months of surgery, can also be a risk factor for SSI in both lumbar decompression 94 and lumbar fusion 83 surgery.
Surgical Team
Only 1 study has looked at surgeon experience in relation to SSI, with Skovrlj et al 84 finding that in adult scoliosis surgery, candidate members as compared with active members for the Scoliosis Research Society had a 2-fold increase in the rate of superficial, though not deep, SSI which was statistically significant. In regards to the effect of resident involvement and experience, 3 studies looking at different aspects of this have found an association with SSI. 61,65,78 Looking at seasonal variation in the risk of reoperation for SSI, Ohya et al. 61 found that April, during which medical staff turnover in Japan, was associated with the highest rate of SSI and reoperation for the same in academic centers while no such seasonal variation occurred in nonacademic hospitals, suggesting that the influx in new and henceforth inexperienced staff may be a contributor to this result. More directly, Schoenfeld et al. 78 found that resident involvement was an independent risk factor for SSI even after multivariate analysis encompassing procedure time and patient comorbidity, while Olsen et al. 65 found that the participation of 2 or more residents increased the risk of SSI although the latter assumed this to be a proxy for surgical complexity rather than a result of resident involvement. Koutsoumbelis et al, 42 however, found no significant association between number of residents and fellows and SSI and Sebastian et al 81 found no association between resident involvement and SSI. As such, it remains unclear as to the effect of residents on SSI.
The number of surgeons involved in spine surgery does not appear to be a significant risk factor, with 3 studies, 23,67,88 finding no significant association between number of scrubbed or senior surgeons and SSI. However, Sciubba et al. 80 found a larger number of surgeons to be associated with SSI in sacral tumor resection, where a multidisciplinary surgical team is often required. Koutsoumbelis et al 42 found that the overall number of personnel may be a risk if 10 or more personnel are present in the operating room. Operating room traffic and the number of personnel both have been linked to an increase in airborne contaminants 103 and could thereby increase the risk of contamination of the surgical wound.
The effects of involvement of more than one surgical team on SSI is not well studied and is confounded by the fact the presence of additional surgical teams may imply greater surgical complexity and therefore potential risk for infection. Blam et al 11 found that the combined involvement of both orthopedic and neurosurgical teams had a reduced rate of SSI as compared with orthopedics alone, with a trend toward the same as compared with neurosurgery alone, despite the greater operating room traffic involved although no clear explanation could be had for this effect. On the other hand, Rao et al 71 found no significant association between involvement of both services as compared with either orthopedics or neurosurgery alone. Involvement of more than 1 surgical team was found by Omeis et al 66 to be a risk for SSI in spinal tumors. However, in most cases this was due to involvement of plastic surgery and the requirement of a complex soft tissue reconstruction with its attendant risks with regard to infection, confounding the effect on SSI. In the case of sacral tumors, Sciubba et al 80 found no statistically significant association between having a plastic surgeon for closure and SSI.
Intraoperative Concerns and Complications
Increased intraoperative blood loss has not been clearly shown to be a risk factor for SSI, with a number of studies on either side of whether an association exists or not. † It is difficult to separate blood loss from other confounding variables such as surgical duration, invasiveness, as well as the need for transfusion. Only 3 studies reporting on intraoperative blood loss also reported on transfusion, with one showing an independent association between each and SSI, 93 one showing no association between either and SSI, 22 and one showing an association between blood loss but not transfusion and SSI. 52 Enough contradiction exists to preclude any conclusions with regard to blood loss as a possible risk factor.
Intraoperative hypothermia has been viewed as a potential risk factor for of SSI due to its induction of vasoconstriction and its negative effects on oxygenation, neutrophil function, and wound healing. 105 However, intraoperative temperature has not been found to be a risk factor so far for SSI in spine surgery, with all three studies including this variable demonstrating no significant association between intraoperative temperature and SSI. 54,64,71 In the lone study examining the effect of intraoperative inspired oxygen, Maragakis et al 54 found that intraoperative administration of fractionated inspired oxygen less than 50% was an independent risk factor for SSI, even after adjusting for other variables. The authors suggested that its effects may be related to the role of oxygen in the bactericidal process of leukocytes.
The argument behind a potential association between intraoperative dural tear and SSI is based on the longer surgical time required to repair a dural tear, as well as the risk of persistent cerebrospinal fluid leakage compromising wound healing. However, no clear relationship between intraoperative dural tear and SSI has been found. Three studies demonstrated no association between dural tear and spinal SSI, 54,60,64 in contrast to a single study finding dural tear to be associated with an increased risk of SSI. 42 In sacral tumors, no definitive association can be made between CSF leak and SSI, as the 2 studies found opposing results. 49,80
Discussion
SSIs are associated with many risk factors that can be patient or surgically related. Our review was able to identify important modifiable and nonmodifiable risk factors that can be essential in surgical planning and discussion with patients.
Footnotes
Notes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Supplement was supported by funding from AOSpine North America.