
Abstract
Study Design
This study is a retrospective case control.
Objectives
This study aims to determine whether cervical degenerative spondylolisthesis (DS) is associated with increased baseline neck/arm pain and inferior health quality states compared to a similar population without DS.
Methods
Patient demographics, pre-operative radiographs, and baseline PROMs were reviewed for 315 patients undergoing anterior cervical decompression and fusion (ACDF) with at least 1 year of follow-up. Patients were categorized based on the presence (S) or absence of a spondylolisthesis (NS). Statistically significant variables were further explored using multiple linear regression analysis.
Results
49/242 (20%) patients were diagnosed with DS, most commonly at the C4–5 level (27/49). The S group was significantly older than the NS group (58.0 ± 10.7 vs 51.9 ± 9.81, P = .001), but otherwise, no demographic differences were identified. Although a higher degree of C2 slope was found among the S cohort (22.5 ± 8.63 vs 19.8 ± 7.78, P = .044), no differences were identified in terms of preoperative visual analogue scale (VAS) neck pain or NDI. In the univariate analysis, the NS group had significantly increased VAS arm pain relative to the S group (4.93 ± 3.16 vs 3.86 ± 3.30, P = .045), which was no longer significant in the multivariate analysis.
Conclusions
Although previous reports have suggested an association between cervical DS and neck pain, we could not associate the presence of DS with increased baseline neck or arm pain. Instead, DS appears to be a relatively frequent (20% in this series) age-related condition reflecting radiographic, rather than necessarily clinical, disease.
Introduction
Although degenerative cervical spondylolisthesis (DCS) is not entirely uncommon in clinical practice and well recognized by the practicing spine surgeon, it has been infrequently reported and studied in the spine literature. In fact, most prior series, while noting its rarity, have reported rates of approximately 10–30% in their cohorts.1-4
Conversely, in the lumbar spine, degenerative spondylolisthesis (DS) has been extensively studied with good-to-excellent outcomes when managed surgically.5,6 Some have suggested that fusion for lumbar spondylolithesis has been associated with improved back pain post-operatively, and many have identified an association between spondylolisthesis in this setting and preoperative back pain.5-8 However, this association, while proposed in the cervical spine as well, has never been systematically or objectively evaluated.
Radiogaphically, the facets in DCS have been described “ground down” and “thinned.” 9 These findings represent advanced degenerative disease and have been promoted as a potential cause of neck pain. Small case series have identified rates of neck pain in DCS of 60–100% among their own cohorts.1,10-12 However, there has been no qualification or quantification of severity in these studies nor comparisons to controls. Similarly, there have been no studies examining patient-reported outcomes more generally in the setting of DCS.
Therefore, we have evaluated the preoperative status of our patients undergoing anterior cervical decompression and fusion (ACDF) and compared cohorts of those with and without the presence of a DCS to more precisely examine the association of DCS with clinical findings. Comparison of post-operative outcomes was not the objective of this study. We hypothesized that given prior reports, those with DCS would have worse baseline PROMs than those without in this setting.
Materials and Methods
315 patients undergoing ACDF between 2014–2018 with at least 1 year of prospectively collected post-operative patient-reported outcomes served as the study sample to assess preoperative disease state and were reviewed. Patients were categorized based on the presence (S) or absence (NS) of a degenerative spondylolisthesis. Any patients with previous cervical surgery; less than 1 year of patient-reported outcomes; or undergoing surgery for tumor, trauma, or infection were excluded. 25 patients had incomplete PROMs, and 48 had incomplete preoperative imaging, all of whom were excluded, leaving a total of 242 patients to be included.
Determination of DCS was made based on measurements of a standing neutral lateral cervical spine plain film X-ray. Radiographs were obtained using a standard radiographic technique with the beam centered at approximately the C3–4 level. The distance between the posteroinferior corner of the cranial vertebra and a point perpendicular to the tangential line of the posterior vertebral body of the caudal vertebra was measured, and a DS was called in the presence of a translational distance of 2 mm or greater (Figure 1). This method and listhesis distance were chosen based on measurements and techniques previously described for the evaluation of DCS.2,11-14 Method for measuring vertebral translation. After drawing a line tangential to the posterior vertebral body of the caudal level (Line AB), a line from the posteroinferior corner of the cranial level (Point D) perpendicular to the previously drawn tangent is drawn (Line CD) and that line is measured.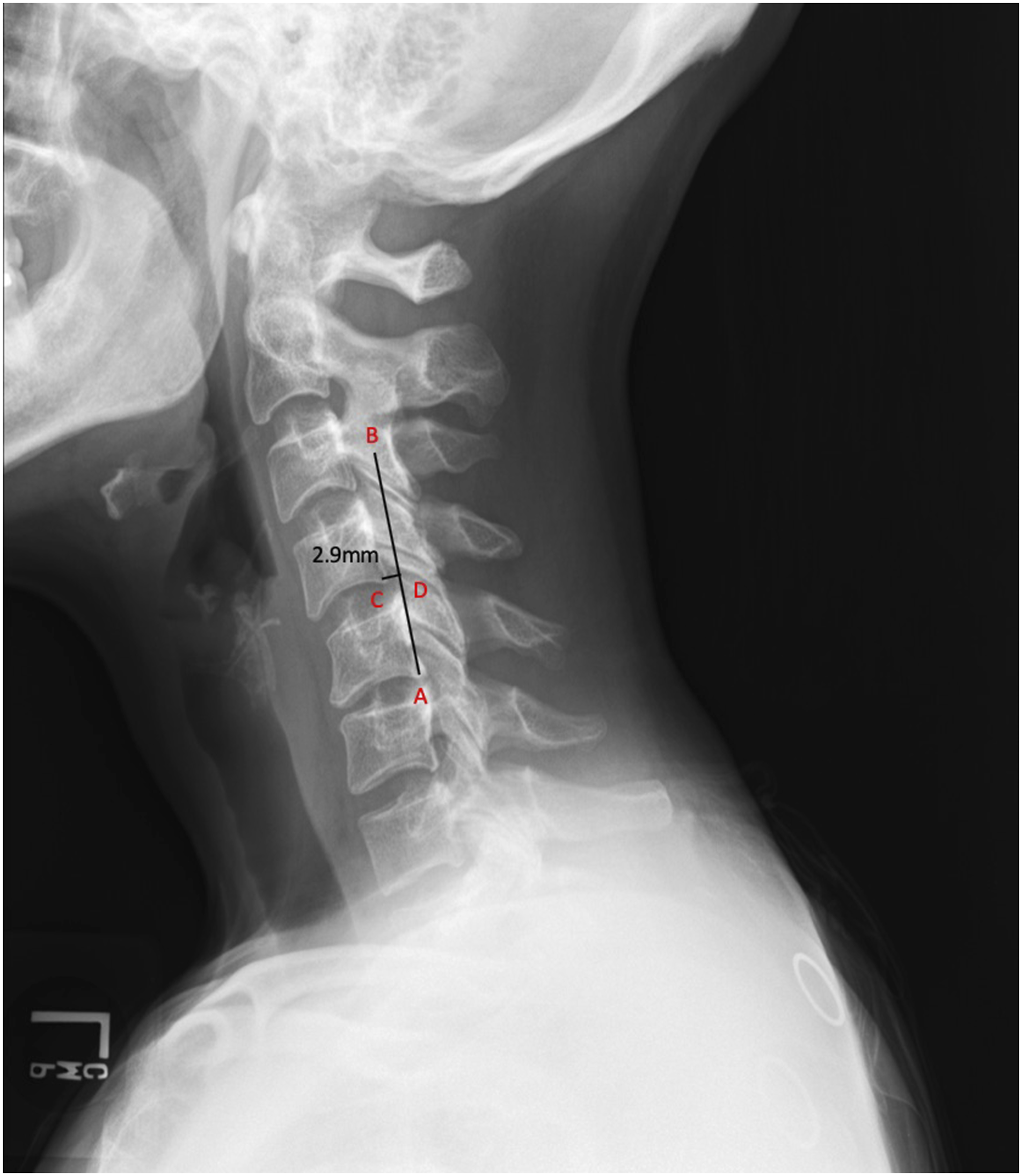
Patient demographics, including age, sex, body mass index (BMI) (kg/m2), smoking status, comorbidities, preoperative radiographs, and baseline PROMs, were reviewed. PROMs were recorded for each individual through OBERD (OBERD, Columbia, MO) and included the Neck Disability Index (NDI), the Physical and Mental Component Scores of the Short Form-12 Health Survey (PCS-12 and MCS-12), and the Visual Analogue Scale Neck and Arm (VAS Neck and VAS Arm) pain scores.
For differences between the cohorts, continuous variables were compared using Student’s t-test, and categorical variables were compared using either chi-square or Fischer’s exact tests. Parameters identified as significantly different were further explored using multiple linear regression analysis to account for confounding.
This study was approved by the Thomas Jefferson University Hospital Institutional Review Board (IRB).
Results
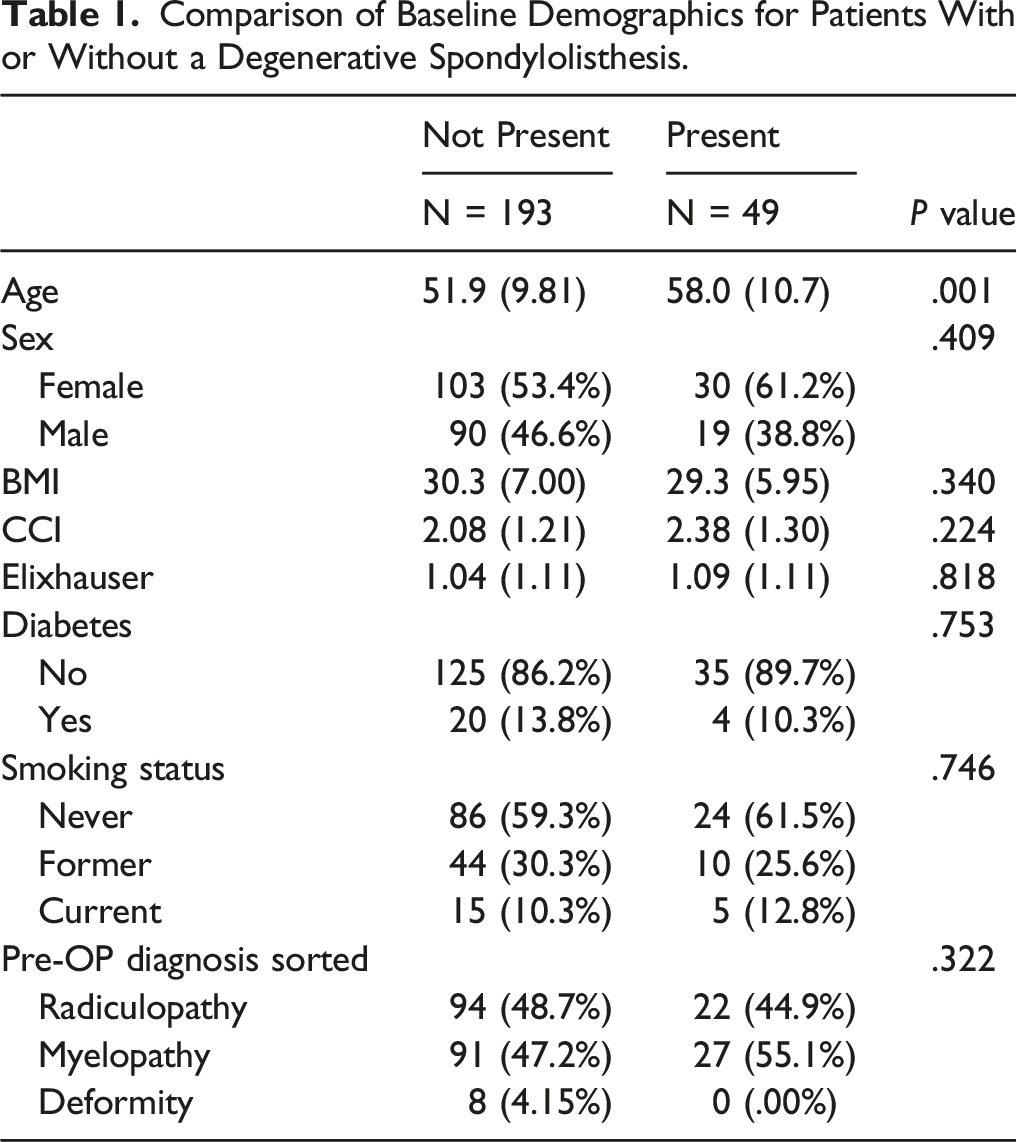
Comparison of Baseline Demographics for Patients With or Without a Degenerative Spondylolisthesis.
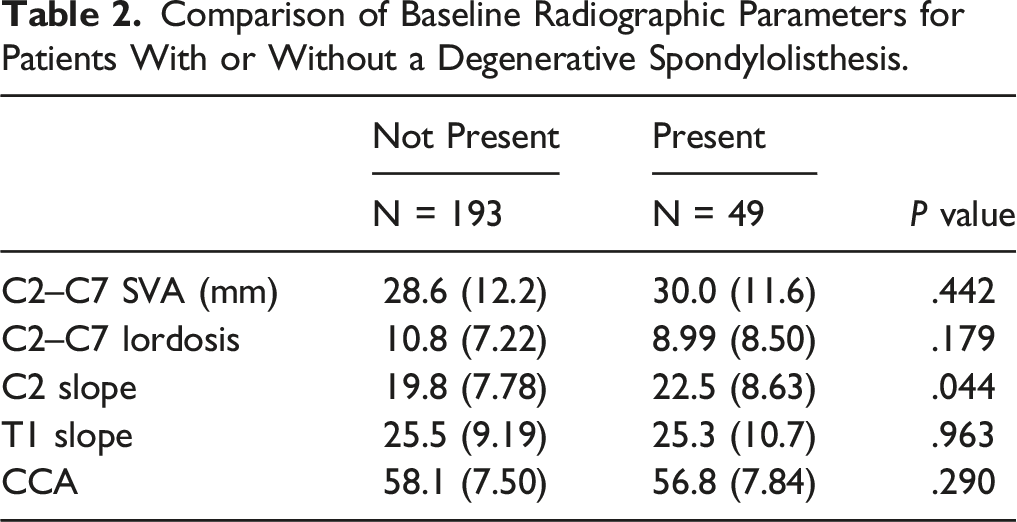
Comparison of Baseline Radiographic Parameters for Patients With or Without a Degenerative Spondylolisthesis.
Comparison of Baselines Proms for Patients with or Without a Degenerative Spondylolisthesis.
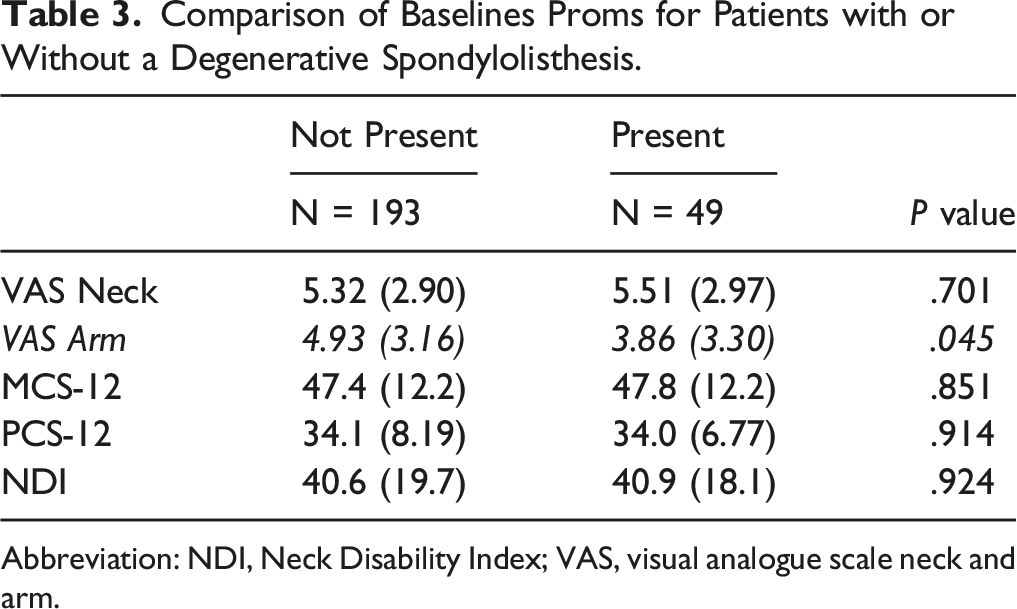
Abbreviation: NDI, Neck Disability Index; VAS, visual analogue scale neck and arm.
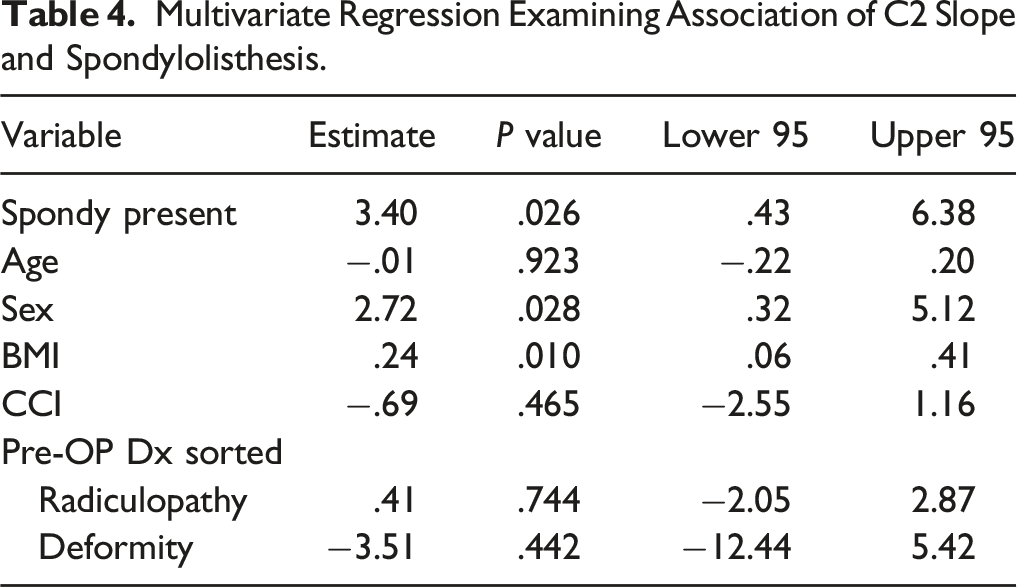
Multivariate Regression Examining Association of C2 Slope and Spondylolisthesis.
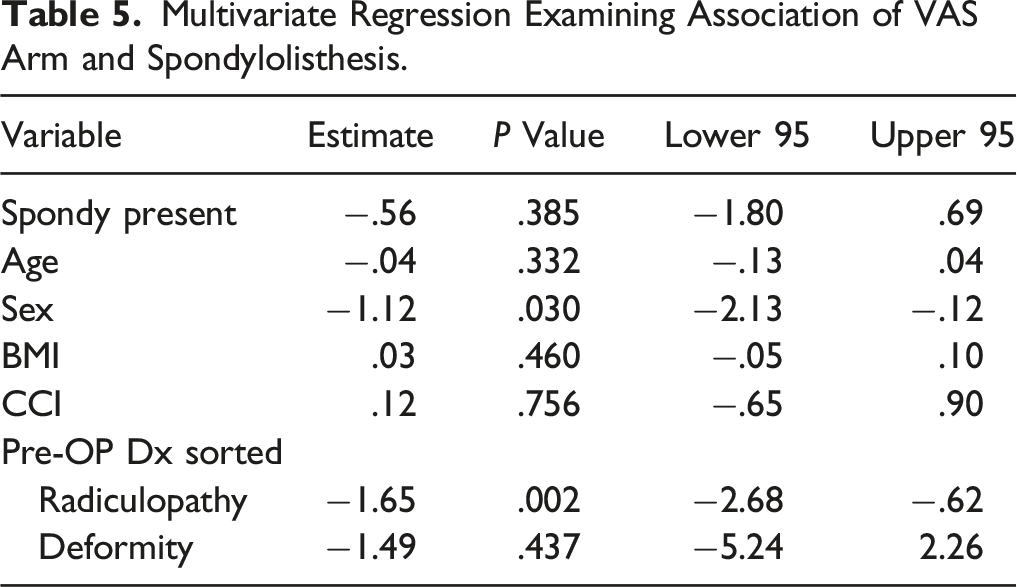
Multivariate Regression Examining Association of VAS Arm and Spondylolisthesis.
Discussion
In a series of 242 patients who ultimately underwent ACDF for myelopathy or radiculopathy, there was a 20% prevalence of DCS. By comparing patients with vs those without a DCS, we were able to compare baseline demographic, radiographic, and health-related quality-of-life measures. Among these, patients with DCS were slightly older and found to have slightly higher preoperative C2 slope than those without a listhesis.
Although in the univariate analysis, those without a listhesis were found to have a higher baseline VAS Arm than those without a listhesis, in the multivariate regression analysis, this difference was no longer significant. Similarly, there were no differences in any health-related quality-of-life measures between those with and without a cervical listhesis.
Previous studies examining patients with cervical spondylolisthesis have been limited. In 1995, Deburge et al 10 published one of the earliest series of unstable degenerative spondylolistheses and reported that this condition was “very rare.” In their series of 8 patients who ultimately underwent cervical surgery, 4 had severe neck pain with no neurological involvement and one had severe pain with “right brachialgia with no precise pattern of nerve-root involvement.” Even in the absence of neurological findings, these patients were ultimately recommended for surgical intervention for severe neck pain alone with all achieving “satisfactory results.”
This series was then followed a year later with another by Boulos and Lovely, 11 who reported on 5 patients with DCS managed with laminectomy and fusion. All were myelopathic, and 3 of 5 had severe baseline neck pain, who experienced a “subjective decrease” in their pain postoperatively.
In one of the largest reports of DCS, Dean et al 1 presented the clinical and radiographic features as well as operative outcomes for 58 patients. 38 of the 58 patients complained of preoperative axial neck or occipital pain. After anterior cervical surgery, almost 95% reported complete or significant improvement in neck pain.
Alternatively, Woiciechowsky et al 12 presented a series of 16 patients with DCS only 3 of whom had a primary complaint of neck pain in the subgroup analysis, although all 16 initially had neck pain as a dominant complaint.
Given that the mechanisms for the development of DCS and lumbar spondylolisthesis are similar, mainly facet degeneration and subluxation,9,10 the association of listhesis with pain identified in earlier case series is sensible. However, our results have suggested that while these patients may have pain, there are no significant differences between their presentation in terms of neck pain and disability from those without DCS.
Limitations
Although this study is the largest comparison of patients with and without DCS evaluating validated PROMs and several radiographic and demographic parameters, there are several limitations. First, we have defined spondylolisthesis as 2 mm or greater. The precise definitions in previously published series have been variable. At least one study defined listhesis as 1 mm of anterior translation, 15 which may be an excessively sensitive value. At least one other study defined listhesis based on the presence or absence of > 3 mm of translation between flexion and extension radiographs. 1 The most commonly used value,2,3,11-14 and the one utilized in the larger of the published series, 2 has been 2 mm on a neutral plain film X-ray, which we have adopted here. However, given the variability in definition, perhaps a more restrictive definition (e.g., 3 mm or greater) would have led to different results.
Second, this cohort specifically evaluated patients scheduled to undergo an ACDF for myelopathy or radiculopathy. We selected this cohort to minimize variability, and moreover, insisting on a minimum of 1 year follow-up (even though post-operative outcomes were not analyzed in this setting) was a further attempt at minimizing confounders. In Woiciechowsky et al’s 12 series of 16 patients with DCS, all 16 patients initially presented with neck pain. However, as other symptoms started to predominate (myelopathy and radiculopathy), the neck pain component lessened in severity. It is possible that in our preoperative cohort, given that these patients already had symptoms severe enough to warrant surgery—for either myelopathy and radiculopathy—the severity of their neck pain was relatively mitigated. However, given the use multiple concomitant validated HRQOL tools (NDI, VAS, and SF-12), if the neck pain component was substantial and different, it may have been identified, especially given that diagnosis (myelopathy and radiculopathy) was controlled in multivariate regression. Further study including a prospective evaluation of asymptomatic controls, perhaps among patients being seen for lumbar complaints, may provide new insights.
Ultimately, this is the first study to our knowledge which specifically aimed to qualify and quantify the influence of DCS on a variety of health-related quality measures. Although previous reports have suggested an association between cervical DS and neck pain, a comparison of 242 patients revealed no increased risk for baseline neck or arm pain whether or not a DCS was present. Instead, DS appears to be a relatively frequent (20% in this series) age-related condition reflecting radiographic rather than necessarily clinical disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval by the TJUH review committee has been obtained.