
Abstract
Study Design:
Retrospective cohort review.
Objective:
To assess whether immediate postoperative neck pain scores accurately predict 12-month visual analog scale–neck pain (VAS-NP) outcomes following Anterior Cervical Discectomy and Fusion surgery (ACDF).
Methods:
This was a retrospective study of 82 patients undergoing elective ACDF surgery at a major academic medical center. Patient reported outcomes measures VAS-NP scores were recorded on the first postoperative day, then at 6-weeks, 3, 6, and 12-months after surgery. Multivariate correlation and logistic regression methods were utilized to determine whether immediate postoperative VAS-NP score accurately predicted 1-year patient reported VAS-NP Scores.
Results:
Overall, 46.3% male, 25.6% were smokers, and the mean age and body mass index (BMI) were 53.7 years and 28.28 kg/m2, respectively. There were significant correlations between immediate postoperative pain scores and neck pain scores at 6 weeks VAS-NP (P = .0015), 6 months VAS-NP (P = .0333), and 12 months VAS-NP (P = .0247) after surgery. Furthermore, immediate postoperative pain score is an independent predictor of 6 weeks, 6 months, and 1 year VAS-NP scores.
Conclusion:
Our study suggests that immediate postoperative patient reported neck pain scores accurately predicts and correlates with 12-month VAS-NP scores after an ACDF procedure. Patients with high neck pain scores after surgery are more likely to report persistent neck pain 12 months after index surgery.
Keywords
Introduction
In the United States, the frequency of which cervical fusions are performed has been rising at a remarkable rate. 1,2 From 1992 to 2005, Medicare data illustrates a 206% increase in cervical fusions. 1 –3 Notably, anterior cervical discectomy and fusion (ACDF) has become one of the most commonly performed, and cost-effective, procedures that provide symptomatic relief for patients with cervical myelopathy, radiculopathy, or myeloradiculopathy. 4 –9 Many studies have demonstrated high success rates and relatively low complication profiles after ACDF. 1,2,10,11 Unfortunately, a subset of patients report persistent refractory neck pain after surgery.
The incidence of persistent neck pain after an ACDF procedure varies throughout the literature. 12 –14 In a study of 24 461 patients undergoing single or multilevel ACDF procedures, Cole et al 12 demonstrated that 1% of patients were newly diagnosed with chronic pain after surgery. 12 However, in a prospective of 258 patients undergoing single or multilevel ACDF procedures, Lied et al 14 found that 35.6% of patients had persistent neck pain after surgery. Furthermore, studies have also demonstrated that the incidence of postoperative neck pain seems to increase with the more levels being operated on. 13 While the underlying reasons for refractory postoperative pain are likely multifactorial, it may include preoperative duration of narcotic use, high baseline levels of affective disorders, unrealistic patient expectation, inadequate decompression, or oversized interbody graft; early identifications of at-risk patients may facilitate timely intervention to optimize the surgical outcomes in this patient subpopulation.
Clinically, measuring quality of care is difficult to do objectively, and relies heavily on subjective evaluation. Patient-reported outcomes (PROs) provide the necessary subjective assessment in determining health-related quality of life, and have become increasingly popular as a proxy of quality of care provided. 15 In spine surgery, prospective registries tracking longitudinal quality and outcomes have emerged to track the effectiveness of surgical interventions. However, prospectively obtaining long-term PROs remains a challenge, making it difficult to ascertain the success of a surgical interventional. 16,17 Identifying patient factors that are associated with better or worsening longitudinal outcomes is vital in determining the long-term trajectory of patient care.
The aim of this study was to assess whether immediate postoperative neck pain scores accurately predict 12-month visual analog scale–neck pain (VAS-NP) outcomes after an ACDF procedure.
Methods
This was a retrospective study of 82 adult patients undergoing index elective ACDF surgery at a major academic medical center from 2008 to 2013. Institutional review board approval was obtained prior to the study’s initiation. Inclusion criteria consisted of patients (1) ≥18 years of age, (2) available demographics and medical record, (3) who underwent elective ACDF, (4) available patient reported VAS-NP scores immediately after surgery and 1-year postoperatively. All patients in this study had neck pain scores collected at the first postoperative day, then at 6 weeks, 3 months, 6, months, and 12 months after surgery. Indications for the surgery include neck pain, radiculopathy, myelopathy, and stenosis.
Demographic variables evaluated included gender, age, body mass index (BMI), and smoking status. Comorbidities included diabetes, hypertension (HTN), hyperlipidemia (HLD), coronary artery disease (CAD), and prior myocardial infarction (MI). Operative variables included median number of fusion levels, estimated blood loss (EBL), length of surgery (LOS), occurrence of nerve root injury, and of cerebrospinal fluid (CSF) leak. Postoperative variables included urinary tract infection (UTI), pneumonia, surgical site infection, deep vein thrombosis (DVT), pulmonary embolism (PE), and 30-day readmission rates.
The primary outcome of this study was to assess whether neck pain scores obtained within 24 hours of surgery accurately and independently predicted neck pain scores 1-year after index cervical spine surgery. These pain scores are based off of Numerical Pain Rating Scale (NPRS), while the follow-up outcomes are based off of VAS-NP scale. Parametric data was expressed as mean ± standard deviation (SD) and nonparametric data was expressed as median [interquartile range]. The correlation between immediate pain scores and VAS-NP scores at 6 weeks, 3 months, 6 months, and 12 months after surgery was assessed using pairwise method. Relationship between independent variables with VAS-NP scores at 6 weeks, 3 months, 6 months, and 12 months after surgery was assessed using a multivariate logistic regression model. All tests were 2-sided and statistically significant if P < .05. Statistical analysis was performed using JMP, Version 12 (SAS Institute Inc, Cary, NC, 1989-2007).
Results
A total of 82 adult patients who underwent ACDF were included in this study; 46.3% of participants were male. The mean ± SD age and BMI were 53.7 ± 12.5 (range 25-79) years and 28.3 ± 7.0 (range 14.8-60.2) kg/m2, respectively (Table 1). The prevalence of comorbidities amongst the cohort were 42.7% with HTN, 28.4% with HLD, 12.2% with CAD, 12.2% with diabetes, and 3.66% having a history of MI (Table 1). In all, 25.6% of patients were smokers (Table 1).
Baseline Preoperative Variables and Patient-Reported Outcomes for All Patients.
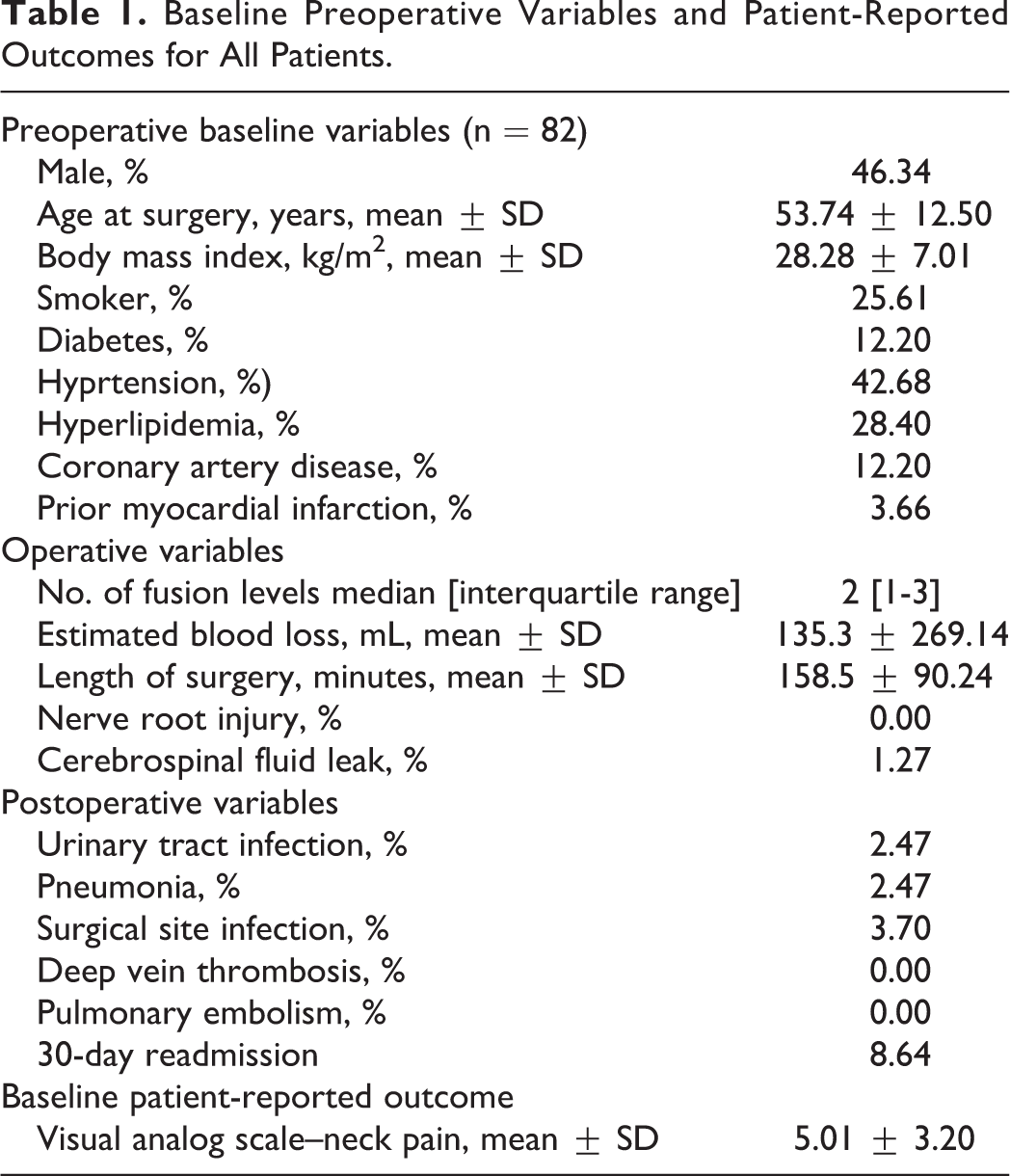
The median number [IQR] of fusion levels performed was 2 [1-3] (Table 1). The mean ± SD EBL was 135.3 ± 269.1 (range 17.5-1700) mL (Table 1). There was no occurrence of nerve root injury and only 1 patient experienced a CSF leak during the procedure (Table 1). The mean ± SD baseline VAS-NP score of 5.01 ± 3.20 (range 0-10) (Table 1).
Relationship Between Immediate Neck Pain and 6-Week, 3-Month, 6-Month, and 12-Month Scores
The mean ± SD neck-pain score on postoperative day 1 was 3.9 ± 2.3 (range 0-10) (Table 2). There were moderate correlations between immediate pain scores and neck pain scores at 6 weeks (R = 0.4114, P = .0015), 6 months (R = 0.3291, P = .0333), and 12 months (R = 0.3503, P = .0247) after index surgery (Table 2). While there was a low correlation between immediate pain scores and 3 months following surgery (R = 0.2514), it was not statistically significant (P = .1725) (Table 2). The changes in VAS-NP scores from immediate to each follow-up were relatively similar with 6 weeks having the lowest change and 12 months having the greatest change: 6 weeks (1.2 ± 2.9), 3 months (2.4 ± 3.4), 6 months (1.8 ± 3.1), and 12 months (2.6 ± 2.7).
Relationship Between Immediate Neck Pain Score and 6 Weeks, 3 Months, 6 Months, and 12 Months.a
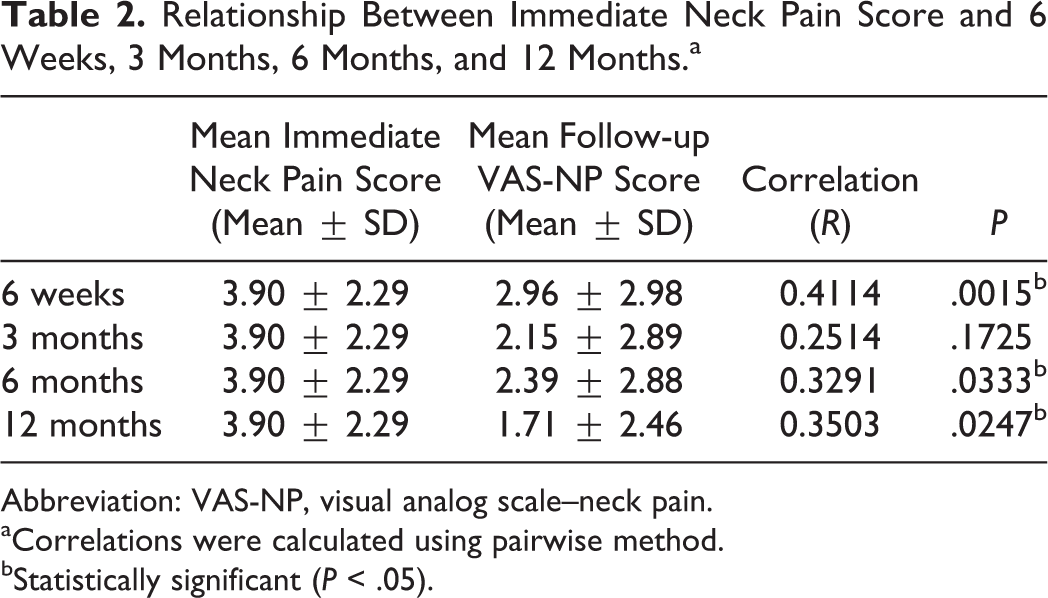
Abbreviation: VAS-NP, visual analog scale–neck pain.
aCorrelations were calculated using pairwise method.
bStatistically significant (P < .05).
In a multivariate regression model, patient age, gender, number of fusion levels, and length of surgery were not predictive of pain scores at 6 weeks, 6 months, or 12 months (Table 3). However, neck pain scores on postoperative day 1 statistically significantly predicted VAS-NP scores at 6 and 12 months (P = .0145, and P = .0442), respectively (Table 3)—meaning that patients with high neck pain scores on postoperative day 1 were more likely to have persistently high neck pain at 6 and 12 months after surgery. When assessing all comorbidities and impact on immediate and follow-up pain scores, there were no statistically significant associations.
Multivariate Regression Model Accurately Predicting 6-Week, 6-Month, and 12-Month VAS-NP Scores From Immediate Postoperative Pain Score.
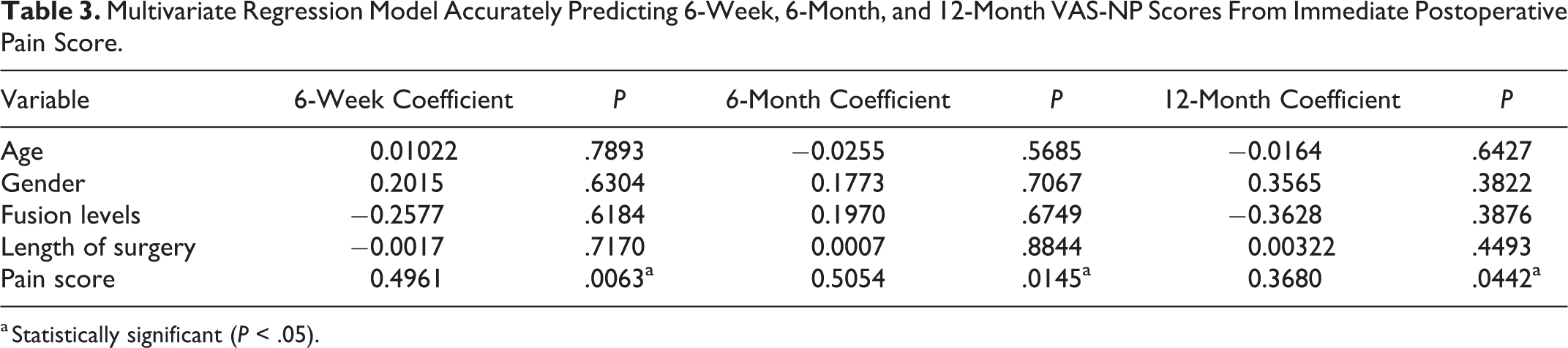
a Statistically significant (P < .05).
Table 4 demonstrates the mean differences in baseline, 6 weeks, 3 months, 6 months, and 12 months VAS-NP scores when grouped the cohort by immediate postoperative pain score, “Low-Pain” (≤5 pain score) and “High-Pain” (>5 pain score) cohorts. There was a significant difference between the cohorts at baseline (Low-Pain, 4.3 ± 3.1 vs High-Pain, 6.8 ± 2.8; P = .0077) and 6 weeks (Low-Pain, 2.4±2.8 vs High-Pain, 4.8±2.8; P = .0101) (Table 4). Even though not significant, the High-Pain cohort trended to have high mean VAS-NP scores than the Low-Pain cohorts at 3-, 6-, and 12-month follow-ups (Table 4).
Difference Between Baseline, Short- and Long-Term VAS-NP Scores by Immediate Postoperative Pain Scores: Low-Pain (≤5 Pain Score) and High-Pain (>5 Pain Score) Cohorts.
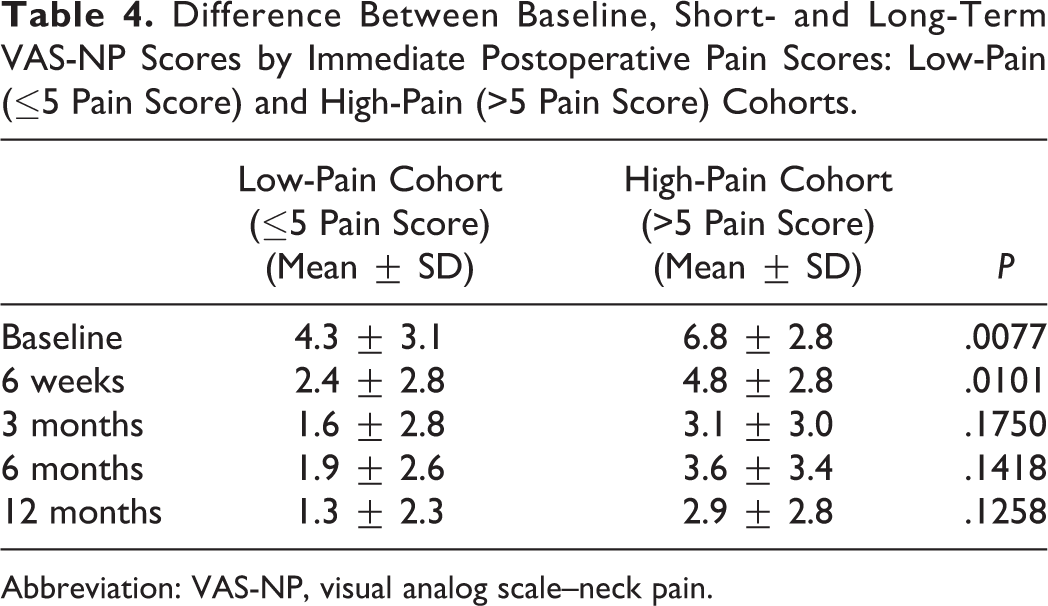
Abbreviation: VAS-NP, visual analog scale–neck pain.
Relationship Between Baseline Scores and Immediate Neck Pain and Baseline, 6-Week, 3-Month, 6-Month, and 12-Month Scores
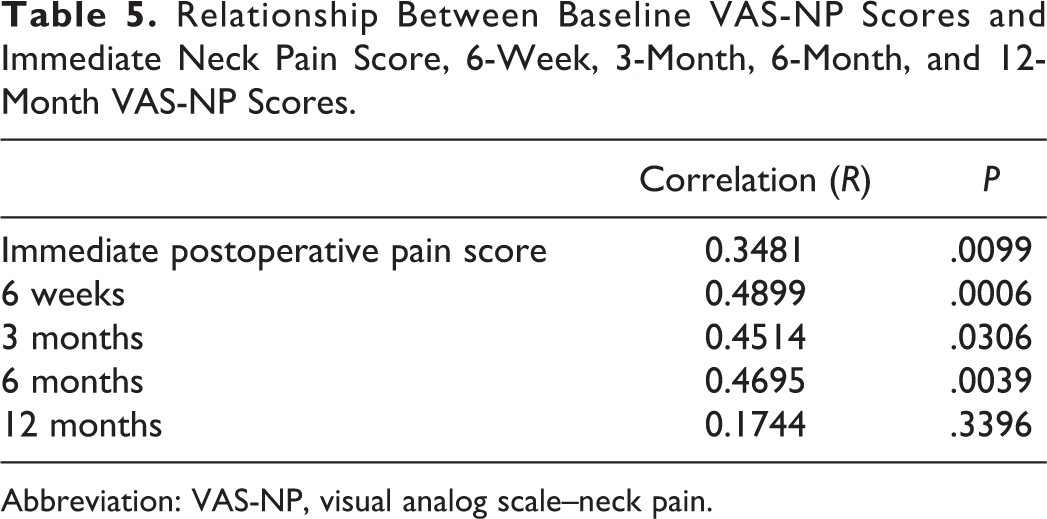
There were significant moderate correlations between baseline VAS-NP scores and immediate postoperative pain scores (R = 0.3481, P = .0099), 6 weeks (R = 0.4899, P = .0006), 3 months (R = 0.4514, P = .0306), and 6 months (R = 0.4695, P = .0039) (Table 5). While there was a low correlation between baseline scores and 12 months following surgery (R = 0.144), it was not statistically significant (P = .3396) (Table 5).
Relationship Between Baseline VAS-NP Scores and Immediate Neck Pain Score, 6-Week, 3-Month, 6-Month, and 12-Month VAS-NP Scores.
Abbreviation: VAS-NP, visual analog scale–neck pain.
Discussion
In this retrospective study of patients undergoing elective spine surgery, we demonstrate that patients with high neck pain scores on the first postoperative day were more likely to have persistently high neck pain scores 6 and 12 months after an index ACDF procedure. Moreover, in a multivariate regression model, immediate postoperative neck pain scores significantly predicted neck pain scores at 6 weeks, 6 months, and 12 months following ACDF surgery.
Comparatively high levels of pain immediately after surgery may be associated with elevated pain levels long term. In a prospective study of 30 patients who underwent lateral thoracotomy, Katz et al 18 demonstrated that early postoperative pain significantly predicted long-term pain. Furthermore, the authors found that pain intensity 24 hours after surgery was significantly greater among patients who developed long-term pain compared with pain-free patients. 18 Similarly, in another prospective study of 625 patients who underwent elective surgery across the various subspecialties—general surgery, plastic surgery, orthopedics, ophthalmology, gynecology, ear-nose-throat, maxillofacial surgery, urology, neurosurgery, or thoracic surgery—Peters et al 19 found that increased pain intensity 4 days after surgery was associated with increased pain duration, increased functional limitations, poor global recovery, and inferior quality of life 6 months following surgery. In a retrospective study of 150 patients who underwent thoracic surgery and were followed for 2 years, Kalso et al 20 demonstrated that patients with persistent chronic postthoracotomy pain for more than 6 months were more likely to report severe levels of acute postoperative pain and require treatment for pain the first week after surgery. Similarly, in a study of 98 patients who underwent breast surgery, Fassoulaki et al 21 found that patients with chronic pain experienced significantly higher pain levels during the first 9 postoperative hours, and required significantly more analgesics, than patients without postoperative chronic pain. Furthermore, the authors demonstrated that the acute postoperative pain accurately predicted chronic pain and long-term analgesic utilization. 21 Interestingly, in a prospective study of 390 consecutive patients undergoing ACDF procedure, Lied et al 22 demonstrated that all potentially life-threatening complications were observed within 6 hours postoperatively and concluded that patients can be safely discharged after a 6-hour observation. Therefore, it is probable that the severity of the pain scores immediately after surgery may serve as an underlying indicator of how the patient will report their pain scores long term. Analogous to these studies, we observed that patients with comparatively high levels of pain on the first postoperative say were likely to report persistent pain 1 year after surgery.
Numerous studies have shown a positive correlation between postoperative short- and long-term outcomes following surgery. In a recent retrospective study of 89 patients who underwent a 1- or 2-level ACDF, Massel et al 7 found that patients had a significant reduction in neck pain VAS scores at 6 weeks postoperatively compared with preoperative scores. Furthermore, the authors illustrated that the neck pain VAS score at 6 weeks was relatively maintained at 12 weeks, 6 months, and 1 year postoperatively. 7 In a multi-institutional prospective study of 969 patients that underwent lumbar spine surgery, Adogwa et al 6 demonstrated that patient-centered measures of surgical effectiveness obtained at 12 months adequately predict long-term (24-month) outcomes after lumbar spine surgery. Similarly, in a retrospective study examining 40 patients undergoing surgical resection of intradural extramedullary spinal tumors, Zuckerman et al 23 observed that both postoperative 3- and 12-month PROs were improved by the minimum clinically importance difference criteria. In another ambispective study examining 63 611 patients undergoing breast reduction surgery, Cohen et al 24 observed no significant difference in patient reported outcomes measures 3 and 12 months after surgery, suggesting that 3-month measures of surgical effectiveness accurately may predict 12-month PRO scores. Important to note, pain scores are subjective as patients are the one assessing their own pain at the time of reporting. Therefore, the correlation of pain scores could be due to patients who report high pain scores immediately after surgery would tend to report high pain scores at follow-up, rather than the patient experiencing increased pain levels.
Few studies have identified independent predictors of acute postoperative pain. In a study of 1490 patients who underwent various surgical procedures, Sommer et al 25 showed that preoperative pain, expected pain, surgical fear and pain catastrophizing were significant predictors of acute postsurgical pain. Similarly, Peters et al 19 observed that that fear of the long-term consequences of the operation was associated with increased pain, poor global recovery, and worse quality of life 6 months later, whereas optimism was associated with improved recovery and greater quality of life. However, in the prospective study by Lied et al, 14 the authors did not find a significant correlation between pain relief after ACDF and multiple factors such as sex, age, number of levels fused, disc level fused, previous neck surgery or trauma, or preoperative symptom duration.
The reasons for persistent postoperative pain after surgery are multifactorial. Peolsson et al 26 and An et al 27 found that smoking status was an independent predictor of acute postoperative pain. Perkins et al 28 suggest that preoperative factors (patient expectation, smoking, depression, and anxiety) as well as intraoperative factors (nerve root injury/irritation or suboptimally positioned hardware) contribute to the development of intractable pain. However, when assessing all comorbidities and impact on immediate and follow-up pain scores, we did not find any statistically significant associations. Interestingly, other studies have attributed the differences in postoperative pain tolerance to underlying genetic variations between patients. In a study of 90 patients who experienced increased thoracotomy pain on postoperative day 3, Ochroch et al 29 found natural variation in the μ-opioid gene OPRM1 predicted increased self-reported postoperative pain. Furthermore, the authors suggest that the haplotypes of the OPRM1 receptors they found could alter the functionality of the receptor through altered oligomerization, β-arrestin interaction, receptor-expression profiles, ligand binding, or receptor signaling that may potentially induce an increasing perception of postoperative pain. 29
This study has limitations, thus ensuing possible implications for its interpretation. First, the duration of preoperative pain and narcotics utilization was not available, which could admittedly bias the results and does not allow us to assess the impact of acute and/or chronic narcotic use on pain scores. Second, other demographic factors and comorbidities, such as employment status and affective disorders were not collected and could affect the results. Third, immediate preoperative VAS-NP scores were not collected and therefore the associate of immediate preoperative pain scores with immediate postoperative and follow-up pain scores could not be assessed. Fourth, the data was reviewed retrospectively and is limited by the weaknesses of a retrospective analysis. Fifth, since patients were not followed for more than 12 months, it is unknown how many developed a delayed onset of pain. Sixth, because of the number of patient we have included in the study, we are limited in the number of variables we can include in the multivariate analysis to assess the impact of the variables collected. Seventh, because of the data being reviewed retrospectively we are limited to what is reported in the patient medical charts, such as surgical and hospital complications. Despite these limitations, the study has demonstrated that immediate postoperative neck pain scores can accurately predict long-term, 12-month VAS-NP scores.
Conclusion
Our study suggests that immediate postoperative patient-reported neck pain scores accurately predicts and correlates with 12-months VAS-NP scores 12 months after ACDF surgery. Patients with high neck pain scores after surgery are more likely to report persistent neck pain 12 months after index surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.