
Abstract
Study design:
Retrospective comparative study.
Objective:
Whereas smoking has been shown to affect the fusion rates for patients undergoing an anterior cervical discectomy and fusion (ACDF), the relationship between smoking and health-related quality of life outcome measurements after an ACDF is less clear. The purpose of this study was to evaluate whether smoking negatively affects patient outcomes after an ACDF for cervical degenerative pathology.
Methods:
Patients with tumor, trauma, infection, and previous cervical spine surgery and those with less than a year of follow-up were excluded. Smoking status was assessed by self-reported smoking history. Patient outcomes, including Neck Disability Index, Short Form 12 Mental Component Score, Short Form 12 Physical Component Score (PCS-12), Visual Analogue Scale (VAS) arm pain, VAS neck pain, and pseudarthrosis rates were evaluated. Outcomes were compared between smoking groups using multiple linear and logistic regression, controlling for age, sex, and body mass index (BMI), among other factors. A P value <.05 was considered significant.
Results:
A total of 264 patients were included, with a mean follow-up of 19.8 months, age of 53.1 years, and BMI of 29.6 kg/m2. There were 43 current, 69 former, and 152 nonsmokers in the cohort. At baseline, nonsmokers had higher PCS-12 scores than current smokers (P = .010), lower VAS neck pain than current (P = .035) and former (P = .014) smokers, as well as lower VAS arm pain than former smokers (P = .006). Postoperatively, nonsmokers had higher PCS-12 scores than both current (P = .030) and former smokers (P = .035). Smoking status was not a significant predictor of change in patient outcome in multivariate analysis.
Conclusions:
Whereas nonsmokers had higher function and lower pain than former or current smokers preoperatively, smoking status overall was not found to be an independent predictor of outcome scores after ACDF. This supports the notion that smoking status alone should not deter patients from undergoing ACDF for cervical degenerative pathology.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) remains a mainstay in the treatment of degenerative disorders of the cervical spine, decompressing traversing nerve roots and restoring anatomical lordosis. 1 It has been well established in the literature that smoking has a negative impact on fusion rate, rate of adjacent segment disease, amount of dysphagia, and wound healing postoperatively. 2 -4 Given its major impact on microvascular circulation and pulmonary function, smoking cessation becomes a very important modifiable risk factor for improving the success rate following ACDF.
Whereas the increased risk of morbidity has been clearly established, the relationship of smoking and health-related quality of life (HRQOL) outcome measurements remains poorly delineated in patients undergoing ACDF. Epidemiological studies have demonstrated an overall decrease or loss of HRQOL years in smokers compared with nonsmokers. 5 The association of smoking and decrease in HRQOL has been defined in the lumbar spine but has not been clearly established in the cervical spine. 6 -8 Jansson et al 6 demonstrated that in patients undergoing a lumbar decompression for disc herniation, less improvement in HRQOL was seen in smokers compared with nonsmokers.
A successful patient selection algorithm for ACDF requires the identification of modifiable risk factors and their optimization preoperatively. Preoperative smoking cessation for patients undergoing ACDF leads to decreased pseudarthrosis, postoperative dysphagia, and wound complications. However, the relationship of smoking status, especially overall smoking history, and change in HRQOL after ACDF is poorly understood. The purpose of this study was to identify changes in HRQOL measures over time—or “treatment effect”—between active smokers, former smokers, and nonsmokers undergoing ACDF.
Methods
After institutional review board approval was obtained, a retrospective review of medical records was performed. The data was collected from fellowship-trained orthopaedic spine surgeons from January 1, 2015, until December 31, 2016, with all procedures performed at a single institution. Patients older than 18 years and with a diagnosis of cervical myelopathy, radiculopathy, or radiculomyelopathy who underwent an elective 1-5 level ACDF were included. Patients were sorted into 3 groups based on their self-reported smoking status: nonsmoker, former smoker, and current smoker. Patients younger than 18 years and those undergoing surgery for trauma, infection, metastatic disease, and revision surgery and those with less than 1 year of follow-up were excluded from the study.
Patient-reported scores, including the Neck Disability Index (NDI), Short Form 12 Physical Component Score (PCS-12), Short Form 12 Mental Component Score (MCS-12), and Visual Analogue Scale Neck (VAS Neck) and Arm (VAS Arm) pain scores were prospectively maintained and collected preoperatively and postoperatively up to the 1-year time point. Demographic data, including age, body mass index (BMI), smoking status, and gender was also recorded.
Analysis comparing pseudarthrosis rates between smoking groups was then conducted based on physician-reported diagnosis of clinical pseudarthrosis and measurements performed on imaging from the institution’s Picture Archiving and Communication System (PACS, Siemens Magic Software, Munich Germany; precision of 0.1 mm). Because routine CT scans are not typically obtained postoperatively, the authors of this study used flexion and extension X-rays in PACS, excluding images taken before 6 months postoperatively. Criteria for radiographic pseudarthrosis were based on those described previously by Song et al, 9 where a superjacent segment motion ≥4 mm and interspinous distance ≥1 between any of the fused vertebrae indicates presence of pseudarthrosis. 9 The groups were also compared for differences in revision surgery rates.
Standard descriptive statistics, including mean and 95% CI, were used to analyze patient demographic data and outcomes for the entire cohort. Baseline differences between groups were compared using 1-way ANOVA and Bonferroni post hoc analysis. Recovery ratios (RRs) were calculated to compare improvements in each outcome between groups. The RR was calculated as follows: (Postoperative score − Preoperative score)/(Optimal score − Baseline score). Optimal scores for PCS-12 and MCS-12 were defined as 100, whereas those for NDI, VAS Neck pain, and VAS Arm pain were 0. 10 The change in outcomes after surgery, pseudarthrosis parameters, and revision surgery between groups were compared using either linear or logistic regression analysis controlling for age, sex, BMI, months followed up, preoperative symptom duration, number of levels fused, graft type, preoperative diagnosis, American Society of Anesthesiologist physical status classification system, and Charlson Comorbidity Index. Pearson χ2 analysis was used to determine any difference in revision surgery or pseudarthrosis rates with respect to smoking status. Binary logistic regression, controlling for age, sex, BMI, and so on, was used to determine whether smoking status was an independent predictor of revision surgery or pseudarthrosis. A P value <.05 was considered to be statistically significant. A power analysis for each preoperative and postoperative outcome was performed to determine whether the study was powered sufficiently to detect a difference equal to or greater than the appropriate minimum clinically important difference (MCID) between groups at a significance level of α < .05 using the variance measured in our sample. 11 The following MCID values were used: NDI, 15 points; PCS-12, 8.1; MCS-12, 4.7; VAS Neck pain, 2.6; and VAS Arm pain, 4.1. 12,13
Results
A total of 264 patients were included in the study: 43 (16.3%) patients were identified as current smokers, 69 (26.1%) were former smokers, and 152 (57.6%) were nonsmokers in the cohort. There were 123 (46.6%) male and 141 (53.4%) female patients in the cohorts. The average follow-up for outcome scores was 19.8 [19.0, 20.6] months. The mean follow-up for radiographic measurements was 12.0 [1.4, 22.7] months. The mean age was 53 [52, 54] years, and the mean BMI was 29.6 kg/m2 [28.8, 30.3]. There were a total of 61 one-level fusions (23%), 125 two-level fusions (47%), 65 three-level fusions (25%), 12 four-level fusions (5%), and 1 five-level fusion (<1%). Baseline demographic data for patients in the cohort are given in Table 1.
Descriptive Statistics of Cohort by Smoking Status (n = 264).
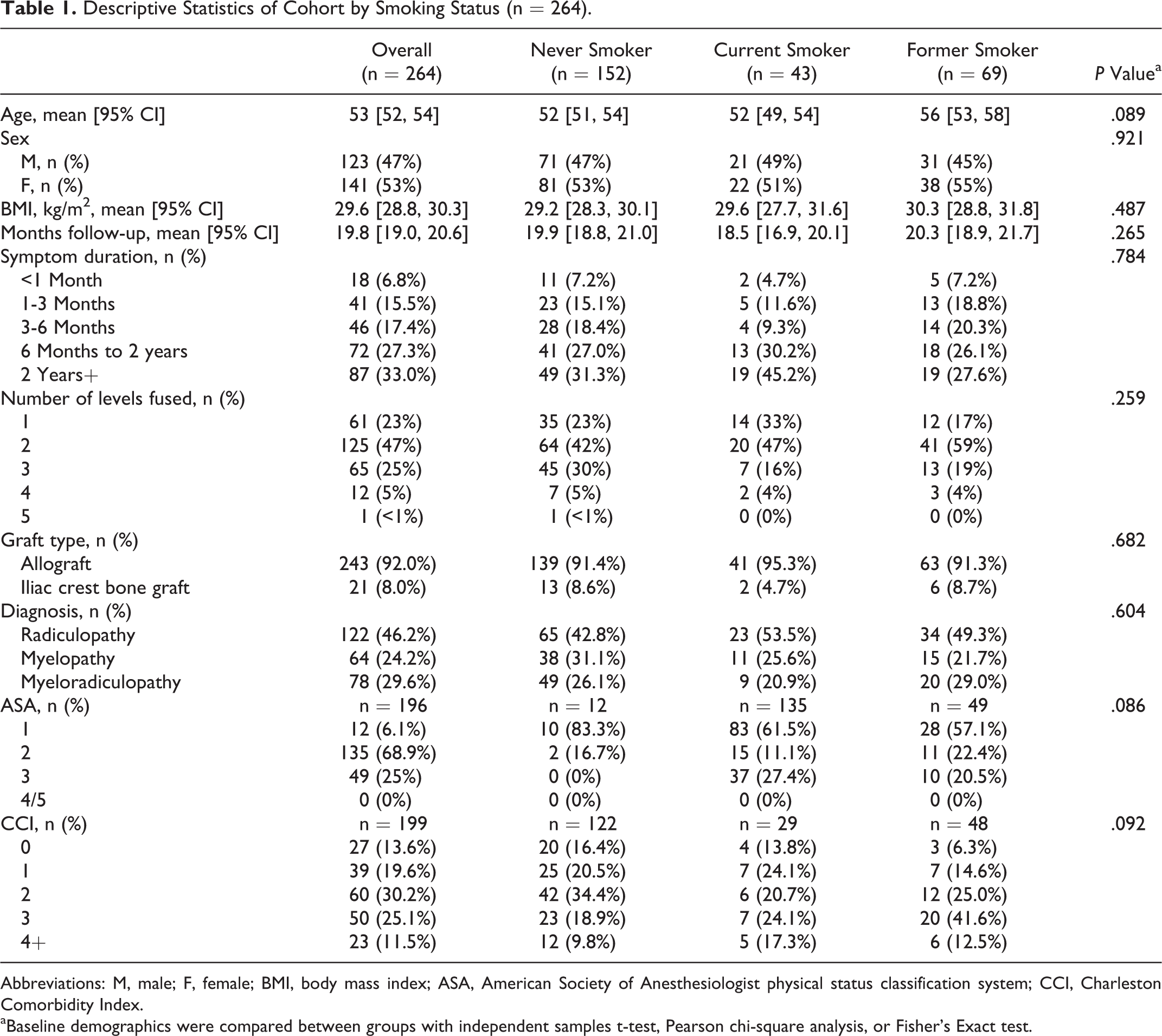
Abbreviations: M, male; F, female; BMI, body mass index; ASA, American Society of Anesthesiologist physical status classification system; CCI, Charleston Comorbidity Index.
aBaseline demographics were compared between groups with independent samples t-test, Pearson chi-square analysis, or Fisher’s Exact test.
HRQOL Outcome Measurements
At baseline, PCS-12 was significantly higher in the nonsmoker group than in the current smoker group, with a significant mean difference of 4.2 points ([0.8, 7.7], P = .010) between the groups. Additionally, VAS neck scores were significantly lower preoperatively for nonsmokers than both current and former smokers, with mean differences of −1.2 ([−2.5, −0.1], P = .035) and −1.0 ([−2.2, −0.2], P = .014) points, respectively. VAS arm pain scores were only significantly different between never and former smokers by a mean difference of −1.3 ([−2.5, −0.3], P = .006) points. Neither MCS-12 nor NDI were found to significantly differ between smoking groups at baseline (Table 2). Postoperatively, only PCS-12 was found to be significantly higher in nonsmokers than both current smokers and former smokers, with mean differences of 5.1 ([0.4, 9.8], P = .030) and 4.1 ([0.2, 8.0], P = .035) points, respectively. None of the other outcome scores significantly differed between the smoking groups at postoperative measurements (Table 2).
Health-Related Quality-of-Life Outcome Measurement Comparisons Between Smoking Groups.
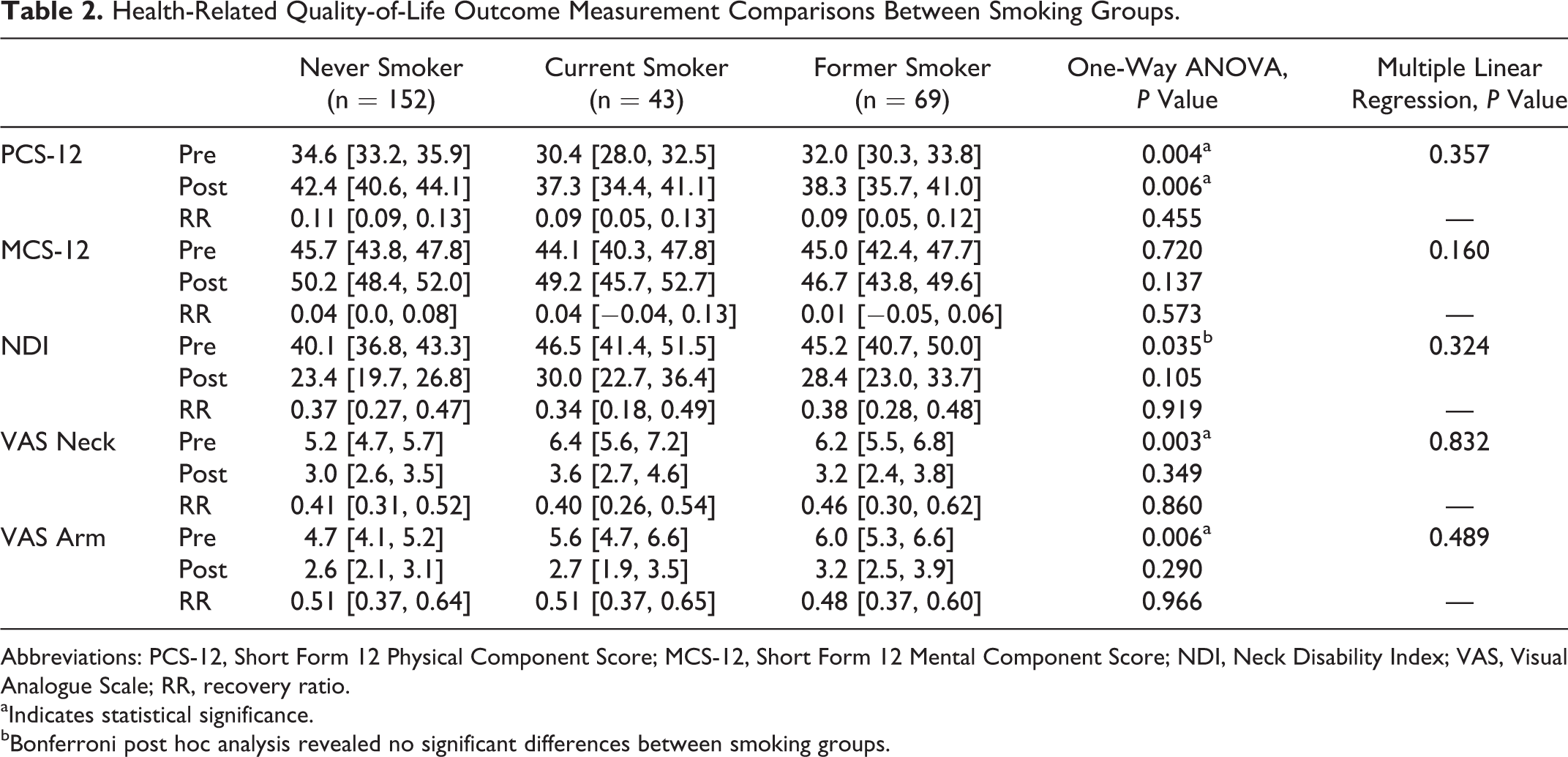
Abbreviations: PCS-12, Short Form 12 Physical Component Score; MCS-12, Short Form 12 Mental Component Score; NDI, Neck Disability Index; VAS, Visual Analogue Scale; RR, recovery ratio.
aIndicates statistical significance.
bBonferroni post hoc analysis revealed no significant differences between smoking groups.
On multiple linear regression analysis, smoking status was found to not be a significant predictor of HRQOL changes after surgery for any of the outcome measures (Table 2). Other variables that came to significance included the following: greater follow-up (months) for NDI (β = 0.468 [0.078, 0.857]; P = .019), VAS Neck pain (β = 0.084 [0.028, 0.139]; P = .003), and VAS Arm pain (β = 0.074 [0.016, 0.132]; P = .012) and use of iliac crest bone graft for VAS arm pain (β = 1.529 [0.111, 2.948]; P = .035). When assessing RR for each outcome, all groups noted similar amounts of improvement from baseline (Table 2).
Pseudarthrosis/Revision Surgery and Smoking Status
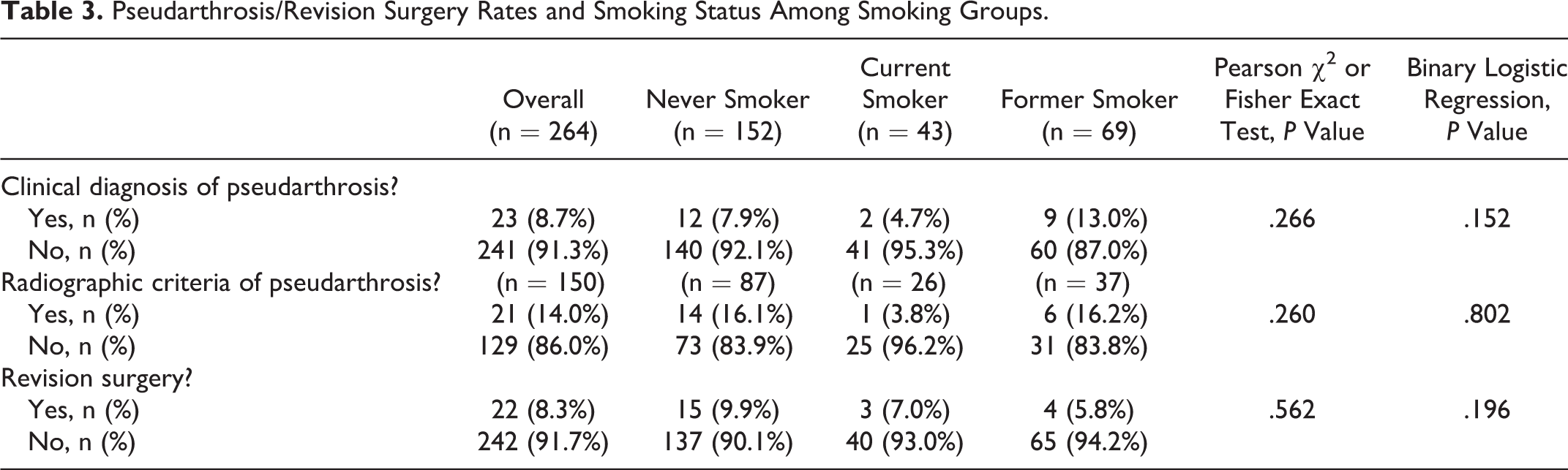
There were a total of 23 patients (8.71%) with a clinical diagnosis of pseudarthrosis. Of these, 12 were in the nonsmoker group (52.2%), 2 were in the current smoker group (8.7%), and 9 were in the former smoker group (39.1%); however, these differences were not statistically significant (P = .266). Based on the criteria used by Song et al, 9 21 of 150 patients (14.0%) had radiographic evidence of pseudarthrosis. There were 14 patients in the nonsmoking group (16.1%), 1 patient in the current smoking group (3.8%), and 6 patients in the former smoking group (16.2%), with no significant differences between groups (P = .260). Using binary logistic regression, smoking status was not a significant predictor of clinical pseudarthrosis (P = .152) or radiographic pseudarthrosis (P = .802). There was no significant difference between groups with regard to revision rates (P = .562), with 15 nonsmokers (9.9%), 3 current smokers (7.0%), and 4 former smokers (5.8%) undergoing revision surgery. Binary logistic regression did not identify smoking status as a significant predictor of revision surgery (P = .196; Table 3). Based on results of the post hoc power analysis, preoperative and postoperative outcome comparisons were sufficiently powered (Power = 0.99).
Pseudarthrosis/Revision Surgery Rates and Smoking Status Among Smoking Groups.
Discussion
In this study, the major aim was to determine the effect of smoking status on the HRQOL outcomes after an ACDF. Despite the well-known increase in general morbidity following ACDF and its relationship to fusion status, the effect of smoking on HRQOL outcome measurements is not as well studied. 11 -15 HRQOL outcomes may be used as a proxy for overall well-being for patients receiving various types of spine surgery, including ACDF. 14 -16 Both surgeons and patients must be cognizant of the potential associated risks of smoking prior to performing ACDF.
In the current study, nonsmokers exhibited higher baseline PCS-12 scores than the current smoker group, with a mean difference of 4.3 points ([0.8, 7.7], P = .010). This group was also found to have higher postoperative PCS-12 scores than both the current and former smoking groups, with mean differences of 5.1 ([0.4, 9.8], P = .030) and 4.1 ([0.2, 8.0], P = .035) points, respectively. The nonsmoking group also had lower baseline VAS neck pain scores than both the current and former smoking group, with mean differences of −1.3 ([−2.5, −0.1], P = .035) and −1.2 ([−2.2, −0.2], P = .014), respectively, and lower baseline VAS arm pain scores than the former smoking group by a mean difference of −1.4 ([−2.5, −0.3], P = .006) points. VAS neck and arm pain scores were not significantly different between groups at postoperative measurements. Additionally, neither NDI nor MCS-12 scores were significantly different between groups at baseline or during postoperative measurements. Finally, both linear regression and RR analyses indicated no significant change in treatment effect between groups for any of the outcome measures examined.
Whereas nonsmokers reported less disability at baseline in terms of PCS-12 and VAS arm and neck scores, they had similar pain scores and a similar improvement in RR as the other groups postoperatively. In addition, smoking status was not found to be a significant predictor of change in treatment effect for any of the included outcome measures. These results suggest that all patients may benefit to a similar degree when undergoing ACDF, regardless of smoking status. However, it is not clear to what degree smoking cessation will actually improve baseline scores in those who smoke. Moreover, the fact that the current study found no significant differences in treatment effect over time between smoking groups suggests that insurance companies need not deny coverage to smokers who require ACDF to address degenerative cervical symptoms, especially those who do not quit using tobacco 6 weeks prior to surgery. 17
Current literature regarding smoking status on cervical surgery show conflicting evidence. Davis et al 18 conducted a prospective study comparing nonunion rates in patients undergoing ACDF and cervical disc replacement. They identified that at 48 months of follow-up, nonsmokers had a greater improvement in NDI, VAS for neck pain, SF-12 MCS, and SF-12 PCS compared with smokers. 18 In a study evaluating multiple surgical techniques for patients with cervical myelopathy, Tetreault et al 19 reported that nonsmokers were more likely to experience improvement in the modified Japanese Orthopedic Association score outcomes than smokers at the 1-year postoperative mark. Similarly, although they did not use HRQOL outcome metrics, Eubanks et al 20 and Hilibrand et al 2 reported worse outcomes after cervical spine surgery in smokers than nonsmokers. 3 These findings are different from this study’s findings and suggest that more studies are needed to determine the relationship between smoking and patient outcomes for ACDF.
Although this current study was not designed to look at pseudarthrosis rates, clinical and radiographic data was used to analyze the cohort. Radiographic measurements described by Song et al 9 were used to determine the presence of a radiographic pseudarthrosis, with an overall rate of 14.0% in the cohort with no significant difference between groups (P = .260). Binary logistic regression found that smoking status was not a significant predictor of clinical (P = .152) or radiographic (P = .802) pseudarthrosis. This is consistent with current literature analyzing pseudarthrosis after ACDF that shows conflicting evidence. 2,7,8,16,20 -25 In a prospective study, An et al 21 compared the use of allograft-demineralized bone matrix composite versus autograft for treatment of 77 patients undergoing ACDF and found no significant difference in the fusion rate of smokers (52.9%) and nonsmokers (72.1%; P = .13). 21 Two other retrospective studies by Lau et al 23 and Luszczyk et al 24 found no significant differences in nonunion rates between nonsmokers and smokers (P = .163 and P = .867, respectively) who underwent anterior cervical surgery. Conversely, Lee et al 16 identified smoking, female gender, and the number of fusion segments as independent risk factors for reoperation in patients undergoing ACDF. Similarly, in the study by Bishop et al, 22 smokers were found to have an increased delayed union rate at 12 months based on radiological measurements than nonsmokers (60% for smokers vs 21% for nonsmokers). In addition, Hilibrand et al 2 also found that smokers had significantly lower fusion rates compared with nonsmokers (smokers: 62%; nonsmokers: 81%; P < .02).
Several limitations for this current study exist, including its retrospective nature, which can lead to potential observer and/or reporting bias. Additionally, some data points were not available for analysis, such as the duration of smoking cessation for patients in the former smoker cohort as well as the pack years for current and former smokers. An additional limitation is the fact that patients who actively use vaporizers only were not included in the study. Self-reporting also introduces recall bias or response bias because nonsmokers may actually be current or former smokers. Additionally, the study was not designed to evaluate pseudarthrosis, so although all patients were required to have more than a year of clinical follow-up, not all patients had appropriate imaging to determine fusion status after surgery. Had CT imaging been obtained for each patient, the present study would have been able to draw more significant conclusions regarding the association between smoking status and nonunion after ACDF.
Conclusion
In the current study, current and former smoking was associated with more severe symptoms at baseline for PCS-12, VAS Neck pain, and VAS Arm pain scores in patients undergoing ACDF. However, in spite of baseline differences, all groups showed similar rates of improvement, and smoking status was not found to be an independent predictor of patient outcomes. These findings suggest that smoking status alone does not influence patient-reported outcomes after ACDF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Board Review Statement
This study was approved by the institutional review board at the Thomas Jefferson University Hospital. Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.