
Abstract
Study Design
A Retrospective Cohort Study.
Objective
To introduce a new Doppler sonography-assisted pedicle screw fixation technique that enables vertebral artery (VA) monitoring during surgery and compares the accuracies of Doppler sonography-assisted cervical pedicle screw fixation and the conventional technique.
Methods
This retrospective study was performed on 164 consecutive patients that underwent pedicle-based screw fixation from C2 to C6 between January 2013 and August 2020. Surgery was performed without intraoperative Doppler sonography in 84 cases (the Control group) or with intraoperative Doppler sonography in 80 cases (the Doppler group). Proper positioning of pedicle screws was graded, and the incidences of VA injury and screw breach in the Control and Doppler groups were compared.
Results
Three hundred and ninety-nine screws were placed in the 164 patients (Doppler, 186 screws; Control, 213 screws). The percentages of well-positioned screws in the two groups were significantly different (Doppler, 97.8%; Control, 85.0%). There were two cases of VA injury in the Control group, an incidence of 2.4%, but no case in the Doppler group.
Conclusion
Doppler sonography can be used intraoperatively to help guide the trajectory of the cervical pedicle screw insertion. It can detect the VA inside the screw trajectory and may reduce the risk of VA injury during cervical pedicle screw fixation.
Keywords
Introduction
Cervical pedicle screw (CPS) fixation is attracting attention because of its biomechanical advantages over lateral mass screw fixation, shorter instrumentation, and greater deformity correction.1-3 However, there are safety concerns regarding the risk of neurovascular injury due to the anatomical environment during CPS.4-7
Ludwig et al 8 reported that 65.5% of transpedicular screws caused a critical breach when placed using only morphometric data, 39.6% when laminoforaminotomy was performed to place screws, and 10.6% when CT-assisted navigation was used. Reinhold et al described custom-made guidance, which in combination with conventional fluoroscopy, improved CPS placement.9,10 Although navigation systems have been demonstrated to be highly reliable, those using such systems should be aware of their limitations,11-13 which include hardware, software, and human failure, and changes in intersegmental relationships between vertebral segments during registration and actual positioning during surgery, especially in settings of traumatic or degenerative instability. In addition, the high costs of navigation systems limit their use by spine surgeons.
The present study was undertaken to evaluate the accuracy of Doppler sonography-assisted pedicle screw fixation of the cervical spine from C2 to C6 level, which is traversed by the V2 segment of the vertebral artery (VA), and compared results obtained with conventional screw implantation.
Materials and Methods
Study Design and Patient Population
This retrospective study was performed on 164 consecutive patients that underwent pedicle-based screw fixation from C2 to C6 between January 2013 and August 2020. Patient records and imaging studies were reviewed after obtaining approval from our institutional review board, which waived the requirement for informed consent.
Characteristics of Patients.
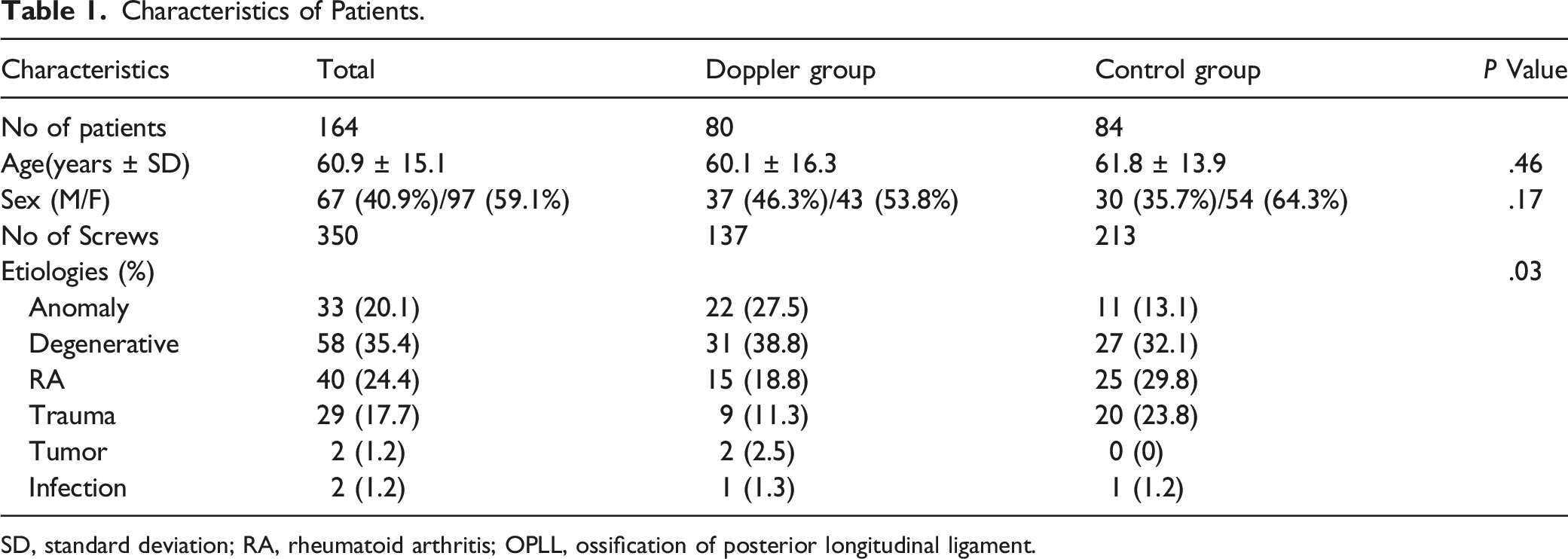
SD, standard deviation; RA, rheumatoid arthritis; OPLL, ossification of posterior longitudinal ligament.
We started to use Doppler sonography (DVM-4500, Hadeco Inc, Japan) intraoperatively to monitor the VA status from August 2017. Surgery was performed without intraoperative Doppler sonography in 84 cases (the Control group) and with intraoperative Doppler sonography assistance in 80 cases (the Doppler group).
All patients underwent CT and MRI before surgery. When a preoperative imaging study suspected an anomalous VA, additional advanced imaging, such as CT angiography (CTA), was used to define the course of the VA and its relationship to the cervical spine, thus reducing the risk of intraoperative VA injury. Postoperative CT was also performed in all patients to check fusion status. We checked the screw breach outside the pedicle and into the transverse foramen using the postoperative CT scan. CT angiography or conventional angiography was performed when VA injury was suspected. Proper positioning of pedicle screws was graded, and the incidences of VA injury and screw breach in the Control and Doppler groups were compared. Regarding posterior screw fixation in the cervical spine around the V2 segment, high-risk of VA injury was defined as the following: 1) a high-riding VA at the C2 level, 2) a narrow C2 pedicle, 3) subaxial pedicle screw fixation from C3 to C6, and 4) when the surgeon was unsure of VA location during surgery.
A high-riding VA was defined as an isthmus height of ≤5 mm and/or an internal height of ≤2 mm on a sagittal image, that is, at 3 mm lateral to the cortical margin of the spinal canal wall at C2.3,14-18 A narrow pedicle was defined using pedicle width measured on axial CT scan images at levels where the lateral cortical margin of the pedicle was clearly observed. A narrow pedicle was considered present when the largest pedicle width was ≤4 mm because the diameter of commonly used screws was 4.0 or 3.5 mm.
Doppler sonography was performed intraoperatively to monitor the VA during pedicle screw fixation in those with a high risk of VA injury since August 2017.
Conventional Pedicle Screw Placement
The C2 pedicle screws are placed via the freehand technique. The screw starting point at C2 is the superomedial quadrant of the C2 articular mass to avoid the VA, which turns superolateral through the inverted L-shaped transverse foramen of C2. The craniocaudal trajectory of the C2 pedicle screws is determined under direct intraoperative visualization by the slope of the C2 pedicle. The medial trajectory is determined by identifying the medial margin of the C2 pedicle, which is the lateral edge of the spinal canal at the C2 level, lateral to the dura mater. We dissect the superior and medial margin of the C2 pedicle to identify the sagittal slope and medial margin of the C2 pedicle. The trajectory is then aimed to be tangential to the medial margin of the C2 pedicle, which is more cortical than the lateral part of the C2 pedicle and far from the C2 transverse foramen.
Once the entry point and screw trajectory are determined, pedicle preparation is performed using either a curved pedicle probe or a drill, and then the screw hole is palpated with a ball tip probe for cortical violation. The tap is sequentially advanced, and the C2 pedicle screw is then placed.
On the other hand, anteroposterior and lateral fluoroscopy is used during the subaxial cervical pedicle screw placement. The starting points of C3 to C6 screws are slightly lateral to the articular mass center, and close to the inferior margin of the inferior articular process of cranially adjacent vertebrae, as is performed for the Abumi technique. 1 Subaxial pedicle screws are implanted by identifying anatomical landmarks and using lateral and anteroposterior fluoroscopy. A lateral image intensifier is used to confirm the pedicle axis and craniocaudal orientation at the screw insertion point. We usually make a funnel-shaped hole at the screw insertion point to enable a broader range of screw insertion angles. A curved pedicle probe, a tap, and screws are inserted into pedicles under lateral C-arm imaging to confirm screw direction and insertion depth. Tactile feedback should be of uniform resistance from cancellous bone within the pedicle. We constantly check screw insertion paths with a small ball tip probe after each step (eg, probing and tapping) of the procedure. The tactile loss of resistance may indicate excessive medial angulation into the spinal canal or penetration into the transverse foramen.
Doppler-Assisted Screw Placement
Surgical steps and procedures were as described for the conventional technique. 1 Subaxial pedicle screws were implanted by identifying anatomical landmarks under fluoroscopic guidance. The craniocaudal orientations of screws at insertion points were confirmed using a lateral image intensifier.
A small-curved pedicle probe, a tap, and screws were inserted into the pedicle under the lateral C-arm image to confirm the direction and insertion depth. The surgeon checked a proper screw insertion path with a cervical pedicle sounder with a small ball tip after probing and tapping. Intraoperative Doppler sonography was used to evaluate the adequacy of screw trajectories during surgery. Because the violation into the transverse foramen is difficult to evaluate by fluoroscopy, we used a Doppler sonography with a 2 mm tip to monitor VAs inside screw holes after each step of pedicle screw implantation.
When the pedicle probe was located at the posterior vertebral line on the C-arm image, the surgeon checked a proper creation of the screw insertion path with a small ball tip and Doppler after probing and tapping. If the surgeon feels a loss of resistance at the bottom of the cervical pedicle, it means a violation of transverse foramen. Also, if the Doppler detects arterial blood flow around the posterior vertebral line, screw trajectory is deviated laterally and directed to transverse foramen (Figure 1).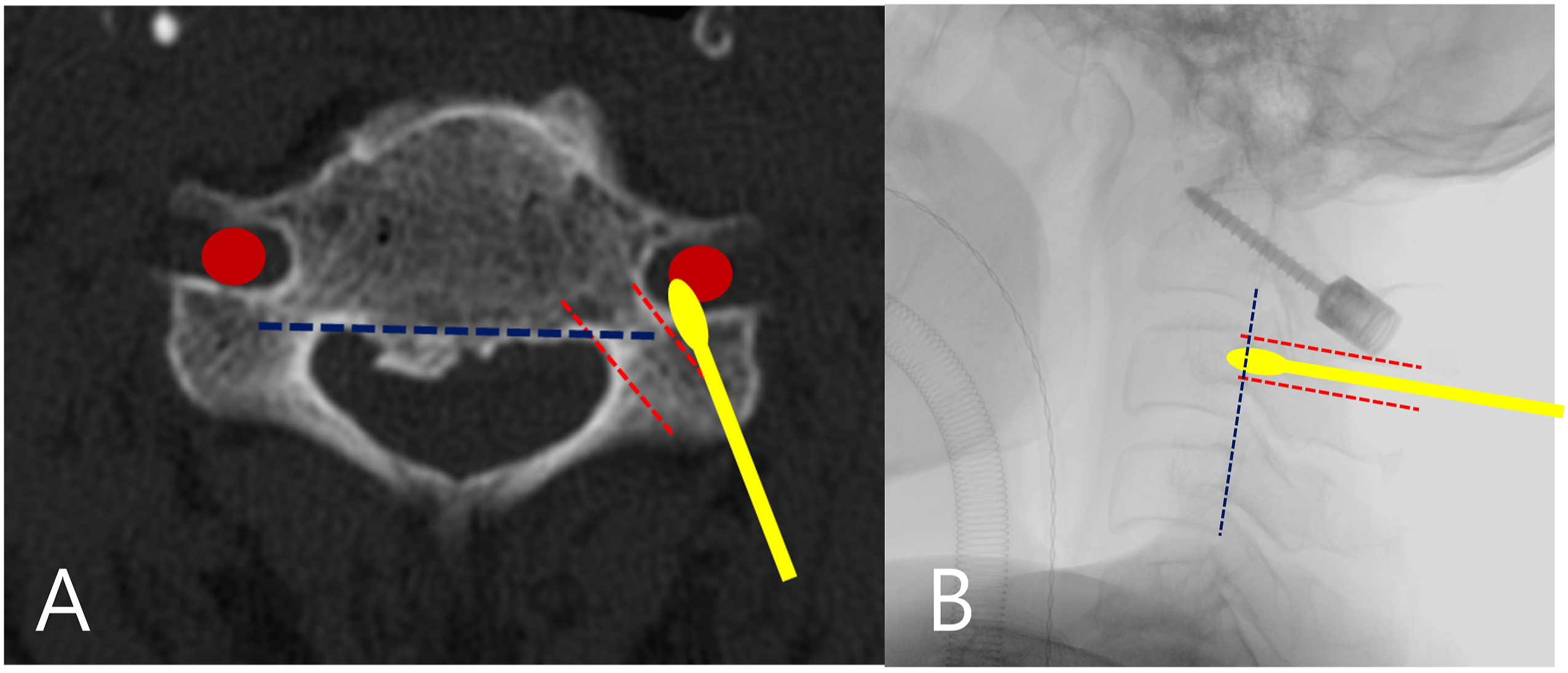
Doppler sonography enables VA monitoring by detecting blood flow and velocity as the VA gets closer and provides the surgeon with auditory and visual feedback. So, inadequate lateral deviation of screw trajectory can be easily detected by intraoperative Doppler sonography and probing using auditory, visual, and tactile feedback when screw trajectory is directed toward a transverse foramen. Moreover, intraoperative Doppler sonography is especially useful for accurately measuring the lengths of C2 pars screws to prevent violating the C2 transverse foramen. This short screw insertion technique can also be used for subaxial pedicle screw insertion. For example, when it is challenging to change screw trajectory for long pedicle screw implantation, a short paravertebral foramen screw can be placed instead to avoid the VA injury, and the length of this screw can be accurately determined using intraoperative Doppler sonography.19,20
Study Parameters
The primary study endpoint was screw position as assessed using CT images by an independent surgeon blinded to the implantation technique. Cortical breaches of pedicle borders by screws were measured in millimeters in the medial, lateral, cranial, and caudal directions. The modified Gertzbein and Robbins classification was used to evaluate the accuracy of screw placement.21,22 This classification consists of five grades: grade 1 represents screw position with pedicle wall perforation of < 1 mm, grade 2 pedicle wall perforation of < 2 mm, grade 3 pedicle wall perforation of < 3 mm, and grade 4 pedicle wall perforation of < 4 mm. Grade 5 represents a cortical breach of > 4 mm and obstruction of transverse foramen by more than half a screw diameter. Screw positioning was defined as “good” for grades 1 or 2 and “bad” for grades 3, 4, or 5. 21
Statistical Analysis
The significances of differences between proportions and ordinal data in the Doppler and Control groups were analyzed using the t-test, chi-square test, and the signed rank-sum test. The analysis was performed using SPSS version 18.0 (SPSS Inc, Chicago, IL, USA), and statistical significance was accepted for P values of <.05.
Results
One hundred and sixty-four consecutive patients were enrolled in this study (Table 1). The mean patient age was 60.9 ± 15.1 years (range, 17–90 years); 67 (40.9%) were male, and 97 (59.1%) were female. The pathologies of enrolled patients were congenital anomaly (n = 33), degenerative disease (n = 58), rheumatoid arthritis (RA, n = 40), trauma (n = 29), tumor (n = 2), and infection (n = 2).
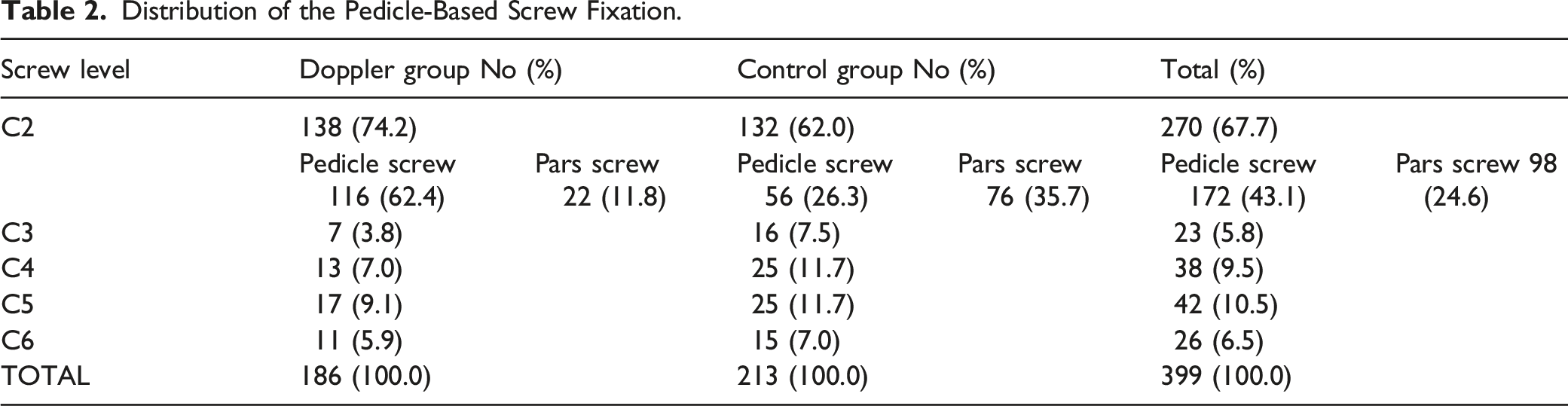
During the study period, 399 cervical screws were inserted into cervical pedicles, and 270 (67.7%) of these were inserted into C2 pedicles. Of these 270 screws, 88 sides (32.6%) had a high-riding VA.
Distribution of the Pedicle-Based Screw Fixation.
Screw Position According to the Modified Gerzbein and Robbins Classification.
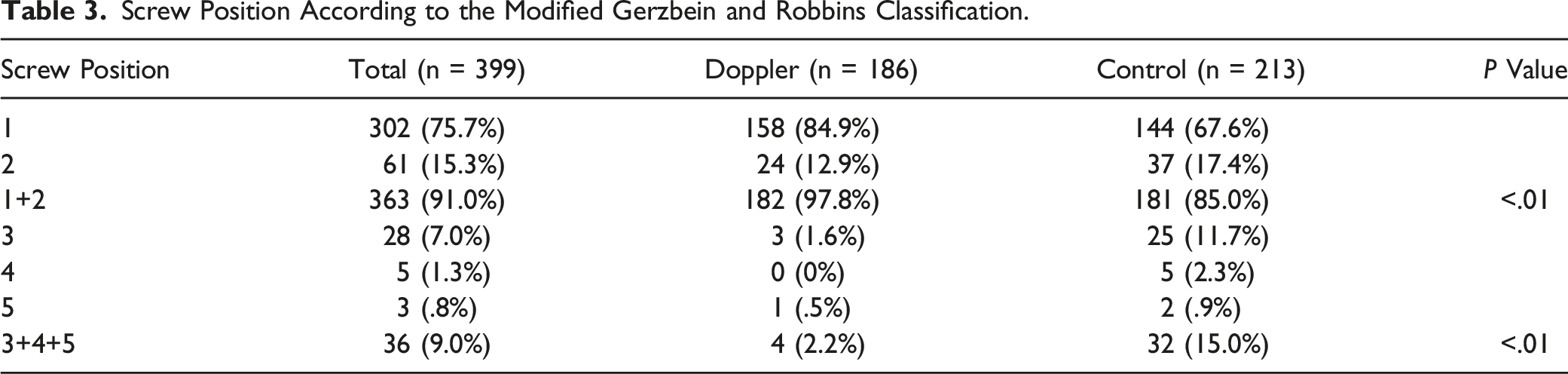
The percentages of well-positioned screws were significantly different in the two groups (Doppler, 97.8%; Control, 85.0%), and no VA injury occurred in the Doppler group.
Case Presentation
Case 1
A 66-year-old male patient presented with severe neck pain and occipital headache with atlantoaxial instability. A preoperative imaging study showed a relatively narrow C2 pedicle on both sides (Figure 2).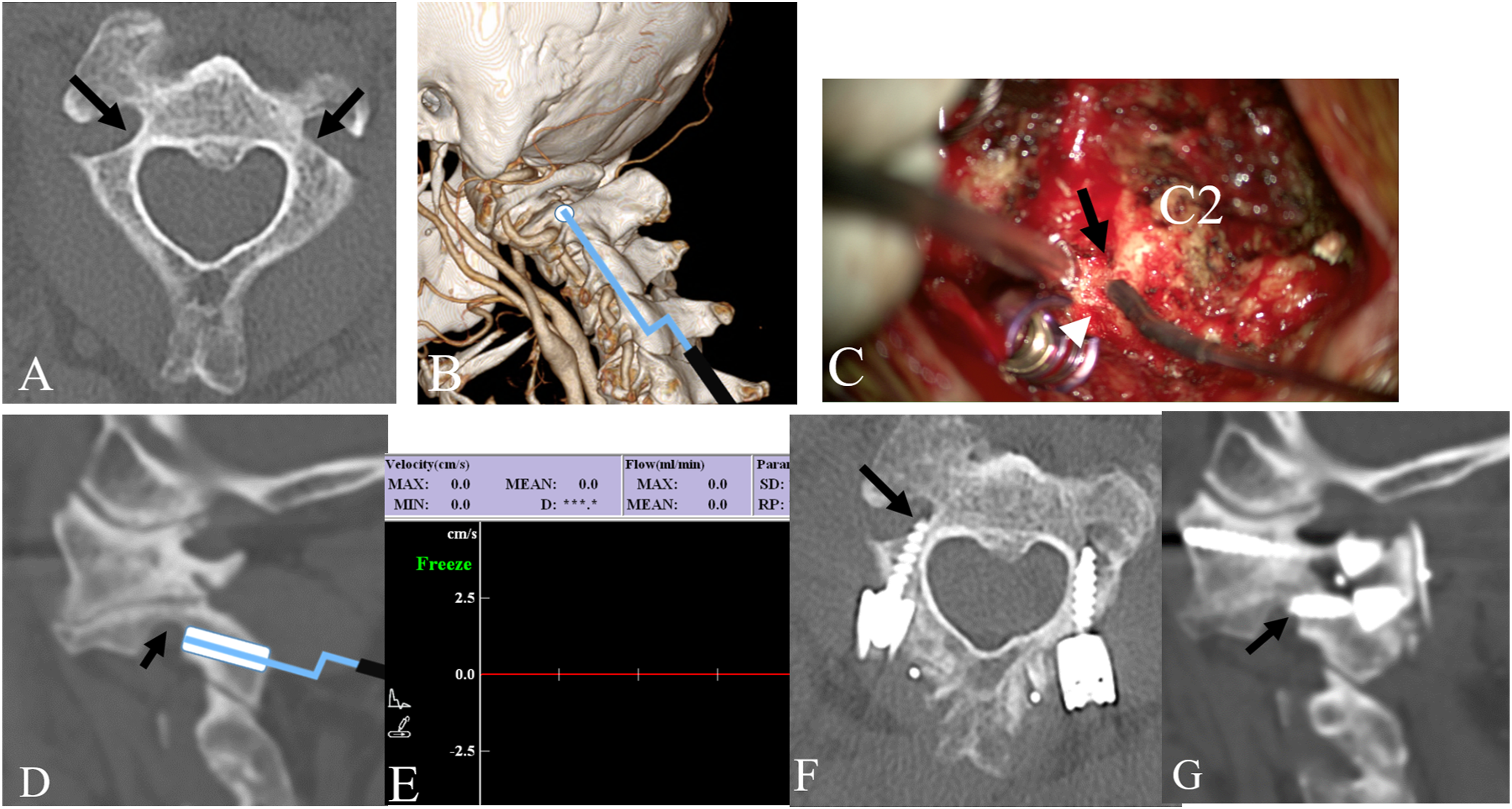
We planned C1–2 posterior instrumentation and inserted C2 pars screws bilaterally to avoid VA injury during screw insertion. The VA inside the C2 pedicle and outside of the C2 transverse foramen were monitored during surgery. In addition, the maximal length of the C2 pars screw was measured by intraoperative Doppler sonography, and violation of C2 transverse foramen was avoided. Postoperative CT showed the C2 pars screw point was just behind the C2 transverse foramen and a minimal breach (grade 2) of the transverse foramen on the right side.
Case 2
A 58-year-old female patient presented with gait disturbance.
Preoperative imaging studies demonstrated os odontoideum with atlantoaxial instability and multilevel cervical stenosis with myelopathy. C1–2 fusion and combined C3–4 selective laminectomy were performed. Preoperative CT showed a narrow C2 pedicle on the left side. Intraoperatively, the C2 pedicle screw trajectory was guided by Doppler ultrasonography to avoid VA injury (Figure 3, Supplementary Video 1). Postoperatively, neurological disturbances gradually improved without any neurovascular complications.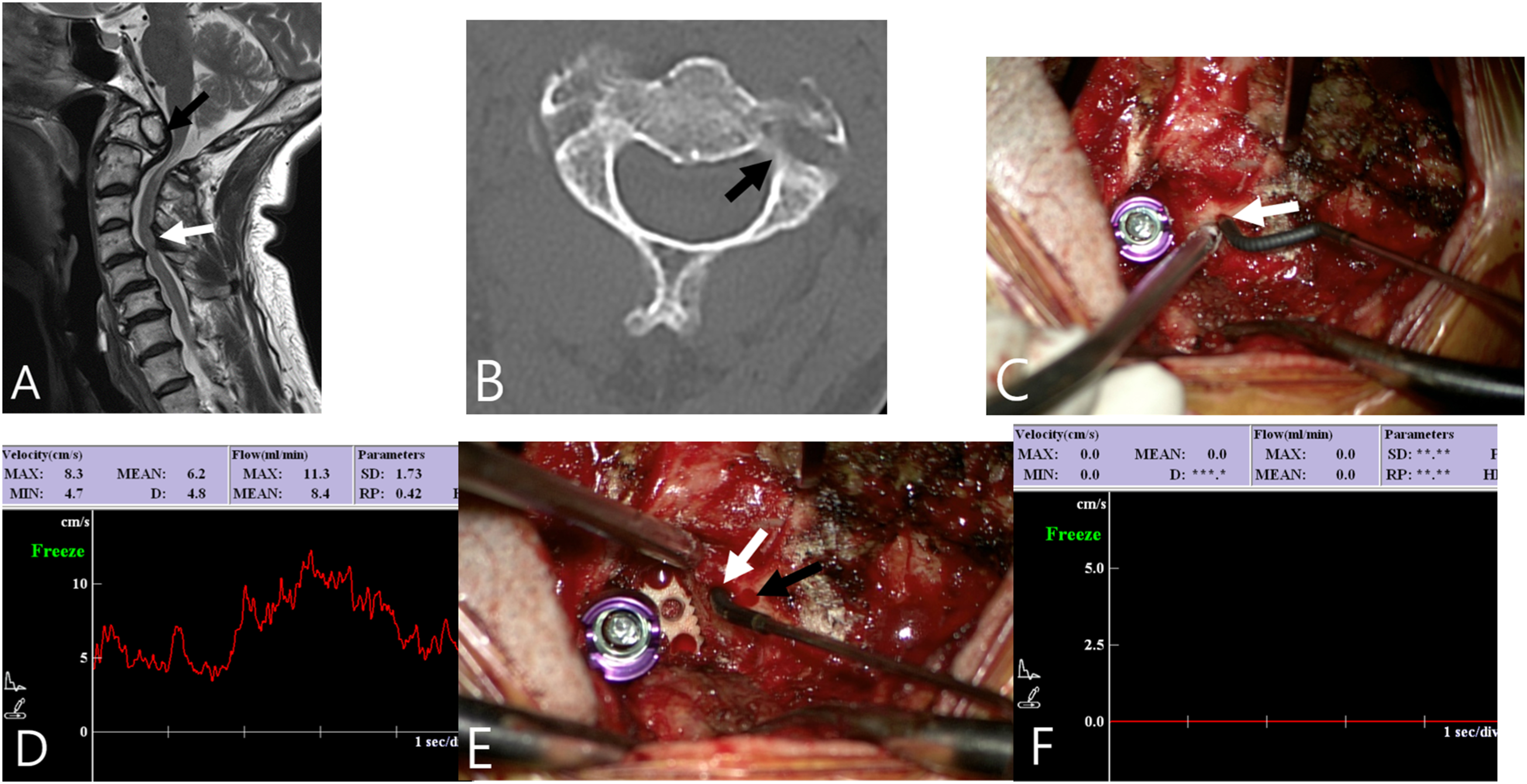
Case 3
A 50-year-old male patient presented with neck pain and progressive quadriparesis. Preoperative imaging studies demonstrated subaxial cervical kyphosis and multilevel cervical stenosis with myelopathy. Anterior and posterior reconstructive surgery was performed to realign the cervical spine and decompress cervical stenosis. The surgical aims were posterior column osteotomy and pedicle screw fixation in the subaxial cervical spine from C3 to C7. Intraoperatively, the cervical pedicle screw trajectory was guided by Doppler ultrasonography to avoid VA injury (Figure 4). Postoperatively, neurological disturbances gradually improved without any neurovascular complications.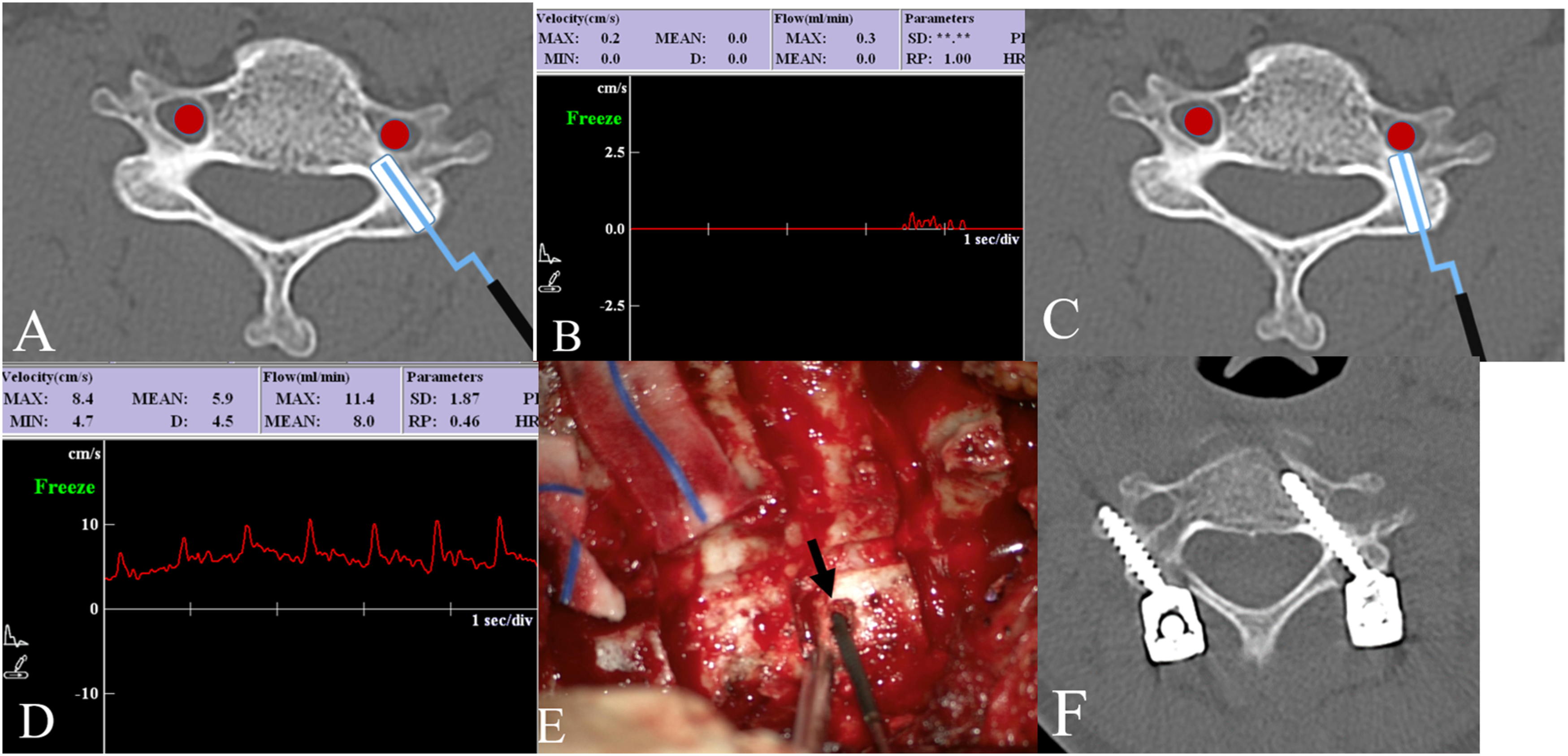
Discussion
The cervical spine demonstrates high anatomical variability, and this increases surgical risks and suboptimal screw positioning.2,3,17,23-32 Therefore, accurate and safe navigation techniques have been developed. However, several studies have shown that navigation techniques cannot guarantee the prevention of neurovascular complications.33,34 Iatrogenic VA injury is a potentially severe complication of cervical spine surgery with the potential to cause catastrophic bleeding, permanent neurological impairment, and even death.5,18,35-37 Thus, preoperative radiological evaluations are required to identify VA anomalies and determine cervical pedicle morphologies before cervical pedicle screw placement.
We performed CT and MRI on all patients before surgery. When a preoperative imaging study suspected an anomalous VA, we performed additional advanced imaging such as CTA or MRA to define the course of the VA and its relationship to the cervical spine and delineate VA anomalies that might increase the risk of intraoperative VA injury. We previously reported that the incidence of V2 segment anomaly is not uncommon in the adult population based on CTA data and that abnormal VA entrance was observed in 5.1% of specimens with entrances into C4, C5, or C7 transverse foramina in 1.6%, 3.3%, and .3%, respectively.2,5
Vertebral arteries also occasionally loop near vertebral bodies, and an irregular VA pathway or irregular cervical pedicle anatomy may be present in up to 23.6% of patients. 25 The highest incidence of irregularities is found at C2. In the present study, 88 sides (32.6%) of the C2 pedicle had a high riding VA, and its incidence was not significantly different between the two groups. A morphometric study by Tomasino et al 38 demonstrated significant individual variations in pedicle diameter, safe zone, and space occupied by the VA, which highlights the importance of evaluating potential risks to neurovascular structures before inserting cervical pedicle screws.
Injury to the V2 segment usually occurs because cervical spine implants have been malpositioned.2,5,26 However, successful cervical pedicle screw insertion is dependent on the surgeon’s ability to identify the optimum screw entry point and trajectory—both of which are facilitated by meticulous preoperative planning. Hojo et al evaluated over 1000 cervical pedicle screws by CT and found that the malposition rate of screws inserted using a freehand technique was high (26.7%) in rheumatoid patients. The authors attributed this to difficulty finding suitable screw entry points due to destructive changes in posterior elements and severe bone fragility. 39
In patients with a high risk of VA injury, surgeons may consider intraoperative CT or three-dimensional fluoroscopy-based navigation systems, which can help determine the accurate anatomy when landmarks are lost during instrument placement.
Several authors have reported the possibilities of using navigation techniques for cervical pedicle screw instrumentation. However, screw malpositioning rates of 4–20% have been reported. 21
When a navigation technique is used in the cervical spine, many potential sources of error may result in less accurate screw placement. For example, mobility of the cervical spine relative to the reference frame may cause errant screw placement. Additional concerns with intraoperative navigation are increased setup time, disruption of workflow, and radiation exposure. Moreover, navigation-guided surgery is just a morphometry-based guiding technique that cannot evaluate VA’s real-time patency and blood flow.
Some authors have reported the possibility and several advantages of freehand techniques for cervical pedicle screw fixation. 40 However, most spine surgeons are reluctant to use freehand pedicle screw fixation for the cervical spine due to the risk of VA injury. Therefore, to insert cervical pedicle screws with confidence, a new intraoperative tool is needed to monitor VA patency and flow during surgery. So, we used intraoperative Doppler sonography to evaluate the adequacy of screw trajectories during surgery.
Figures 2 and 3 illustrate a case of Doppler sonography-guided cervical pedicle screw fixation. Inadequate lateral deviation of a screw trajectory can be easily detected by intraoperative Doppler sonography due to the auditory, visual, and tactile feedback received when a screw is directed toward a transverse foramen.
This comparative study was undertaken to demonstrate if intraoperative Doppler sonography improves cervical pedicle screw fixation accuracy. Overall, 97.8% of screws were well-positioned (grade 2 or better) in the Doppler group, whereas 85% were well-positioned (grade 2 or better) in the Control group. These results show that Doppler-assisted pedicle screw fixation accuracy may be superior to freehand screw insertion in the cervical spine.
Doppler sonography enables VA monitoring during screw placement and providing informative feedback to the surgeon. 41 So, inadequate lateral deviation of screw trajectory can be easily detected intraoperatively based on simultaneous auditory, visual, and tactile feedback when a screw is directed toward a transverse foramen during instrumentation. 42 Thus, the Doppler-assisted technique reduces the risk of VA injury.
Intraoperative Doppler sonography is especially useful for accurately measuring the length of a C2 pars screw to ensure C2 transverse foramen is not violated (Figure 1). Furthermore, when a surgeon places C2 pars screw in patients with high-riding VA, Doppler probing can identify the VA inside C2 transverse foramen, which helps determine screw length, thus preventing over-drilling selection of excessively long C2 screws. This technique can also be used for subaxial pedicle screw insertion.19,43 When it is difficult to change the screw trajectory for long pedicle screws, a paravertebral foramen screw can be used instead to avoid VA injury, and the length of the screw can be accurately determined by intraoperative Doppler sonography. 19
The present study has several limitations that warrant consideration. First, the study was conducted using a single-center retrospective design. Although this single-surgeon experience may limit the generalizability of our results, the study describes the pattern of screw breach and complications associated with this particular type of surgery. It also suggests that VA-related complications could be reduced by Doppler sonography, even in high-risk patients. Second, we did not use a navigation-guided technique during the study period, and thus, the Doppler-assisted and navigation-guided techniques could not be compared. Third, this study had a heterogeneous patient population between groups. Fourth, the surgical experience of cervical pedicle screw placement differed in the 2 groups because Doppler-assisted pedicle screw fixation began in August 2017. By 2017, when Dopplers were first utilized, the surgeon had already placed 168 pedicle screws in 67 patients with a conventional technique. Therefore, the differing experience of the surgeon could also explain all the differences in VA injury rates between the Doppler and non-Doppler groups. Finally, although the accuracy of screw fixation with Doppler was significantly better than that of the conventional technique, we did not compare clinical outcomes between groups in this study. In general, screw accuracy does not always guarantee better clinical results.
This study is the first comparative analysis of the pedicle screw fixation technique between the conventional technique and the Doppler sonography-assisted technique. More extensive data and prospective multicenter studies are required to confirm the advantages of Doppler sonography-assisted cervical pedicle screw fixation over navigation-guided and freehand techniques. Nevertheless, based upon our experience, we believe that Doppler sonography can improve the accuracy of cervical pedicle screw placement, as it enables the assessment of VA and blood flow patterns in real-time during surgery.
Conclusion
Doppler sonography can be used intraoperatively to help guide the trajectory of the cervical pedicle screw insertion. It can detect the VA inside the screw trajectory and reduce the risk of VA injury during cervical pedicle screw fixation. Using Doppler sonography, we adjusted screw trajectory angles and determined appropriate screw lengths to help avoid VA injury during cervical pedicle/pars screw placement.
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.