
Abstract
Study Design.:
Retrospective study.
Objective.:
Cervical pedicle screw (CPS) placement is technically demanding because of the great variation in pedicle size, dimension, and angulations between cervical levels and patients and the lack of anatomical landmarks. This retrospective study was conducted to analyze novice neurosurgeons’ experience of CPS placement by using the technique with direct exposure of pedicle via para-articular minilaminotomy.
Methods.:
We retrospectively reviewed 78 CPSs in 22 consecutive patients performed by 2 surgeons. All pedicle screws were inserted under the direct visualization of the pedicle by using para-articular minilaminotomy without any fluoroscopic guidance. We analyzed the direction and grade of pedicle perforation on the postoperative computed tomography scan. The degree of perforation was classified as grade 0 to 3. Grades 0 and 1 were classified as the correct position and the others, as the incorrect position.
Results.:
In total, the correct position (grade 0 and 1) was found in 72 (92.3%) screws and the incorrect position (grade 2 and 3) in 6 (7.7%). Among the 16 pedicle perforations (grade 1, 2, and 3 perforations), the directions were lateral in 15 (93.8%) and superior in 1 (6.2%). There were no neurovascular complications related to CPS insertion.
Conclusion.:
Free-hand CPS placement by using para-articular minilaminotomy seems to be feasible and reproducible.
Introduction
Cervical pedicle screw (CPS) can achieve a more rigid fixation force than other posterior cervical fixation methods such as the lateral mass screw or translaminar screw. 1 -4 Because of these advantages, CPS fixation can be applied in various cervical spinal disorders, and reliable clinical results have been reported. 5 -10 However, this procedure is technically difficult and challenging because of the great variation in pedicle size, morphology, and angulations between cervical levels and patients and the lack of anatomical landmarks. They had been generally criticized for the potential risk of neurovascular injury. 11 -15 Therefore, accurate and safe CPS insertion techniques are developed. Recently, the availability of image-guidance systems—for example, computer-assisted navigation system based on computed tomography (CT) and 3-dimensional (3D) fluoroscope—has helped improve the accuracy of CPS insertion. 3,16 -20 However, the high cost and complicated registration procedure restrict the application of these systems. Moreover, the navigation systems have some limitations because of misregistration and navigation errors caused by the motion of the spine during the procedure. 20
The objectives of this study were to present the CPS insertion technique under direct visualization of the pedicle via para-articular minilaminotomy without any image guidance to show that this technique can be learned and implemented without difficulty and to evaluate the accuracy and validity of CPS placement in patients. In addition, we focused on providing a detailed description of insertion of CPSs throughout this article.
Materials and Methods
This study was approved by the institutional review board of our institute (KANGDONG 2019-08-007). The corresponding author (operator 1) had already applied this technique clinically; however, the first author (operator 2) had experience only in the insertion of lateral mass screws to the subaxial cervical spine before. Operator 2 started free-hand insertion of pedicle screws to the subaxial cervical spine by learning from operator 1.
Operator 1 inserted 38 pedicle screws to the subaxial cervical spine without any image guidance in 9 patients (7 male and 2 female; mean age 56.1 years, range 42-67 years) from April 2012 to July 2013. Operator 2 inserted 40 pedicle screws in 13 patients (8 male and 5 female; mean age 64.0 years, range 42-85 years) from April 2016 to January 2018. In all cases, CPS insertion was performed before decompressive laminectomy.
Preoperative Radiographic Evaluation
In all cases, preoperative CT scans were performed. Pedicle morphology was evaluated preoperatively using the 3D CT scan. On preoperative CT scans, the diameter of the pedicles, the convergence angle for exact trajectory, and the imaginary line on which the CPS should be placed were measured for each cervical level. Pedicle screw insertion was not performed when the pedicle diameter was less than 3 mm and when the pedicle was not complete because of anatomical deformity or trauma. We skipped the level with an incomplete pedicle.
Based on the imaginary line, we figured out an approximate entry point on the lateral mass, which became a reference for how much to dissect muscle laterally (Figure 1). The length of the screw was decided on the basis of reaching the anterior one-third of the vertebral body on 3D-CT images.
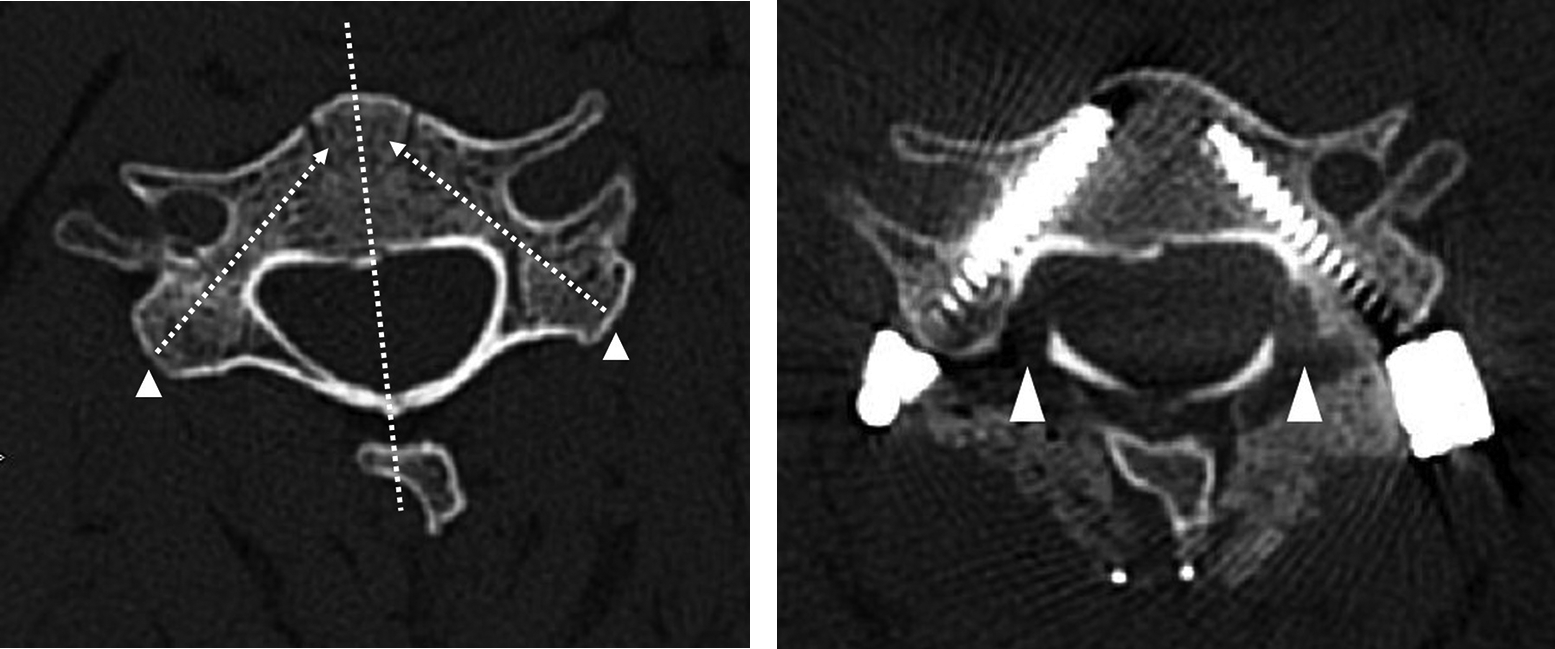
A. Pedicle morphology was evaluated preoperatively by a 3-dimensional computed tomography (CT) scan. The diameter of the pedicles, the convergence angle for exact trajectory, and the imaginary line (white dotted line) on which the cervical pedicle screw should be placed were measured for each cervical level. An approximate entry point on the lateral mass (white arrowhead) was indicated. It will become a reference for how much to dissect muscle laterally. B. Postoperative CT scan reveals that the screws were inserted along the entry point and trajectory planned preoperatively. Adequate laminotomy is indicated by a white arrowhead.
Surgical Technique
All patients were placed in a prone position with the head fixed by using a Mayfield 3-pin clamp. A standard posterior midline incision was made and paravertebral muscles were subperiosteally dissected and retracted laterally to expose the lateral border of the lateral mass.
First Step: Identification of the Entry Point and the Pedicle by Para-articular Minilaminotomy
Under the microscope, the medial and superior walls of the pedicle were exposed via para-articular minilaminotomy by using a 3-mm diamond burr (Figures 2A and 2B). Because we only need to check the pedicle, we do not have to remove the ligament flavum. By dissecting and retracting the ligament flavum and epidural venous plexus free from the pedicle using a microdissector into the laminar window, we can identify the superior and medial border of the pedicle and the junction of the pedicle and posterior wall of the vertebral body. We can confirm them visually or by probing it with a blunt hook. The most bulging part of the pedicle is the center of the pedicle. Along the imaginary line that follows the center of the pedicle, we can determine the entry point on the lateral mass as well as the convergence angle and direction of the pedicle (Figure 2C). The entry point was determined by considering preoperative measurements of the pedicle on 3D-CT scans as well as the surgical field findings.
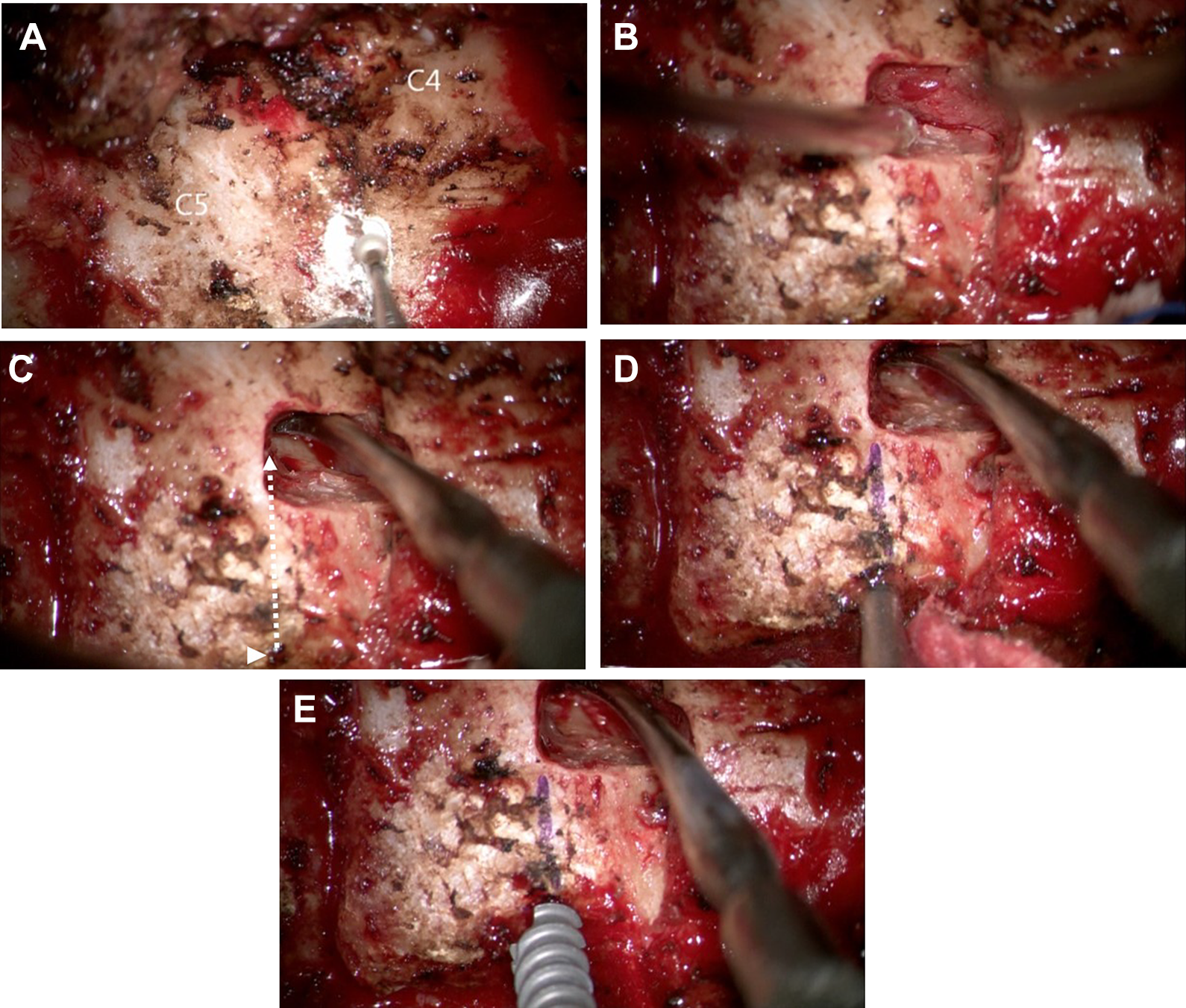
Right C5 pedicle screw insertion. A. Right C4 and C5 lamina were exposed. Drilling starts at the lamino-facet junction for a para-articular minilaminotomy. B. After para-articular minilaminotomy, ligament flavum and epidural venous plexus were observed. C. Exposure of the medical and superior wall of the pedicle by using a dissector without removal of the ligament flavum. Along the imaginary line that follows the center of the pedicle (white dotted line), we can determine the entry point on the lateral mass (white arrowhead), and the convergence angle and the direction of the pedicle. D. Marking on the lateral mass of the direction of the pedicle; gentle probing using a Lenke probe. E. Insertion of the screw under direct visualization of the pedicle.
Second Step: Pedicle Probing and Screw Insertion
We made an entry hole over the entry point with a 3-mm diamond burr, approximately 3 mm in depth. Under direct visualization of the medial wall of the pedicle, a gentle probing using the Lenke probe through the cancellous channel of the pedicle was performed (Figure 2D). As with the thoracolumbar spine, if the probe follows the cancellous channel of the pedicle, it advances almost without resistance. It is important to proceed parallel to the pedicle and to confirm that the convergence angles measured intraoperatively and preoperatively are well maintained. It is important to confirm 5 bony walls (medial, lateral, superior, inferior, and bottom) through ball-tip probing. Tactile feedback can perceive the intraosseous placement of the screw trajectory and lack of pedicle breach. If the breach was palpated within the pedicle, the trajectory was changed or skipping the breached segment was considered.
If the process is performed well, there is no need to check with lateral fluoroscopic imaging. Then, sequential drilling, tapping, and screwing were performed (Figure 2E).
Postoperative Evaluation of Screw Placement
The accuracy of the CPS placement was evaluated on 3D-CT scans postoperatively. The degree of perforation was classified as grade 0 if the screw was located within the pedicle; grade 1, if perforation was made by the screw by less than 25% of the screw diameter; grade 2, if perforation was made by 25% to 50% of the screw diameter; and grade 3, if perforation was made by >50% of the screw diameter (Figure 3). Grades 0 and 1 were classified as the correct position and the others, as the incorrect position. 7,21 The direction of the pedicle breach was assessed as follows: medial, lateral, superior, and inferior.
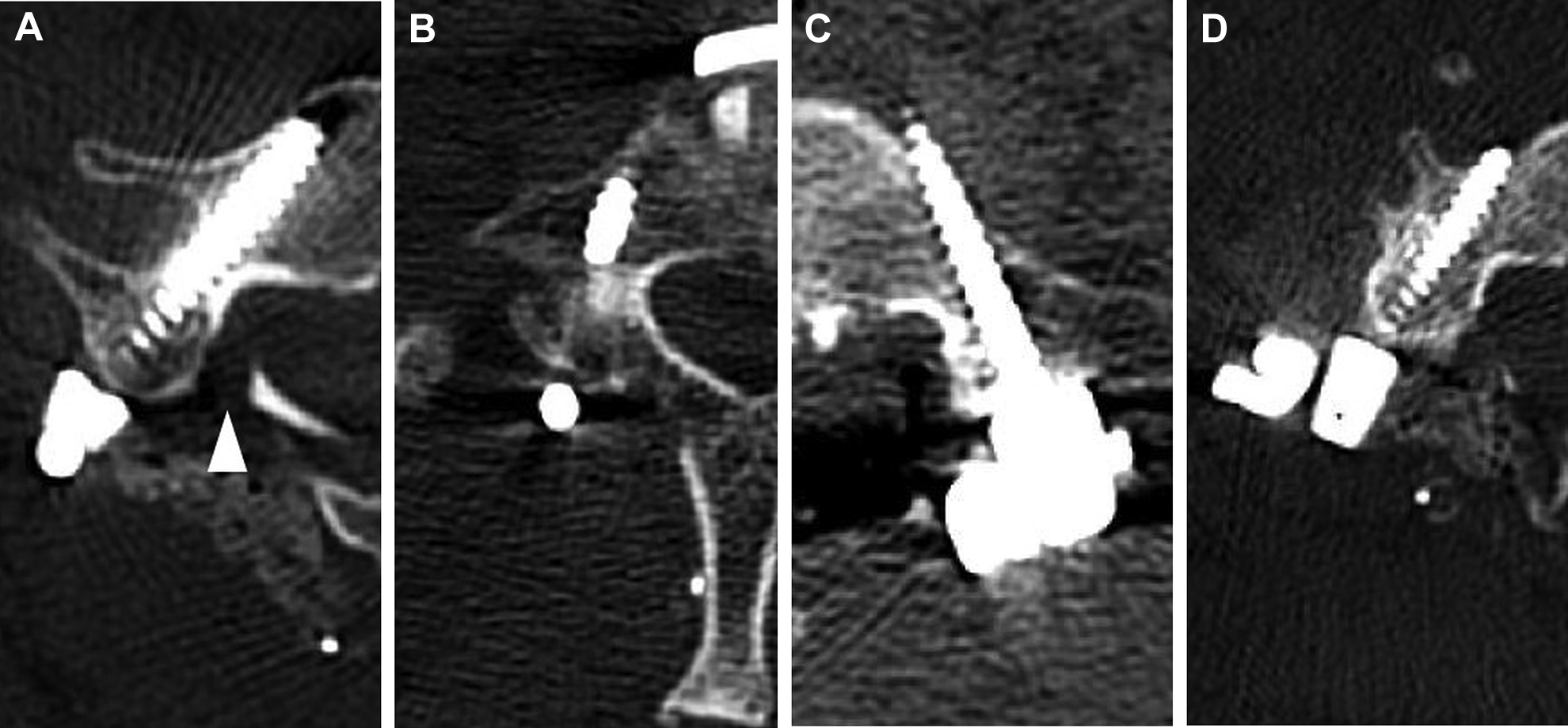
The grading system for pedicle perforation. A. Grade 0: the screw is located within the pedicle. B. Grade 1: perforation less than 25% of the screw diameter. C. Grade 2: 25% to 50% of the screw diameter. D. Grade 3: >50%.
Results
The pathology of the patients was as follows: 19 were trauma patients; 1 patient had cervical spondylotic myelopathy; 1 patient had infectious spondylitis; and 1 patient had metastatic pathological fracture from prostate cancer.
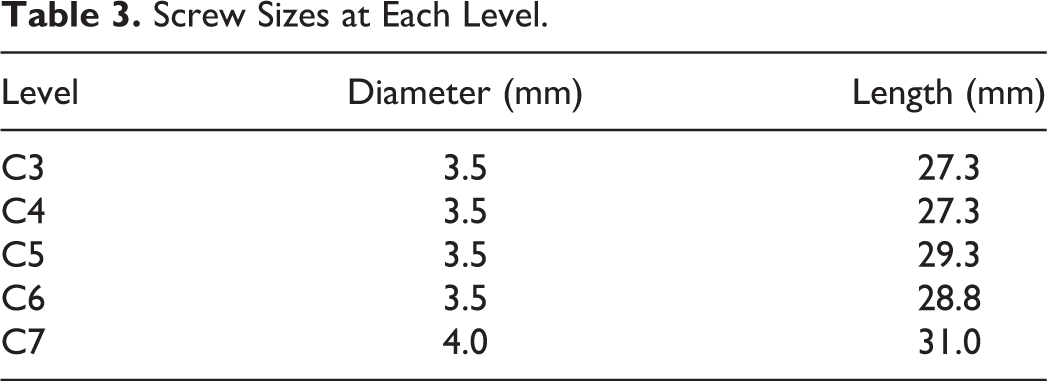
The number of screws inserted was 8 at C3, 5 at C4, 8 at C5, 11 at C6, and 6 at C7 by operator 1, and 6 at C3, 4 at C4, 6 at C5, 6 at C6, and 18 at C7 by operator 2 (Table 1). The correct position (perforation grades 0 and 1) was found in 36 (94.7%) screws and the incorrect position (perforation grades 2 and 3) in 2 (5.3%) screws for operator 1, and the correct position in 36 (90%) screws and the incorrect position in 4 (10%) screws for operator 2. In total, the correct position was found in 72 (92.3%) screws and the incorrect position in 6 (7.7%). The direction of perforation was lateral in 8 (88.9%), followed by superior in 1 (11.1%) screw for operator 1, and lateral in 7 (100%) for operator 2 (Table 2). Among the 16 total pedicle perforations, the direction was lateral in 15 (93.8%) and superior in 1 (6.2%). No perforation to the medial and inferior pedicle was observed for both operators. Even in grade 3 perforations, VA injury or symptoms suggesting nerve root irritation were not observed in any case. The diameter and length of the screws at each level were summarized in Table 3.
Results of Pedicle Screw Placement at Each Level, per Operator.
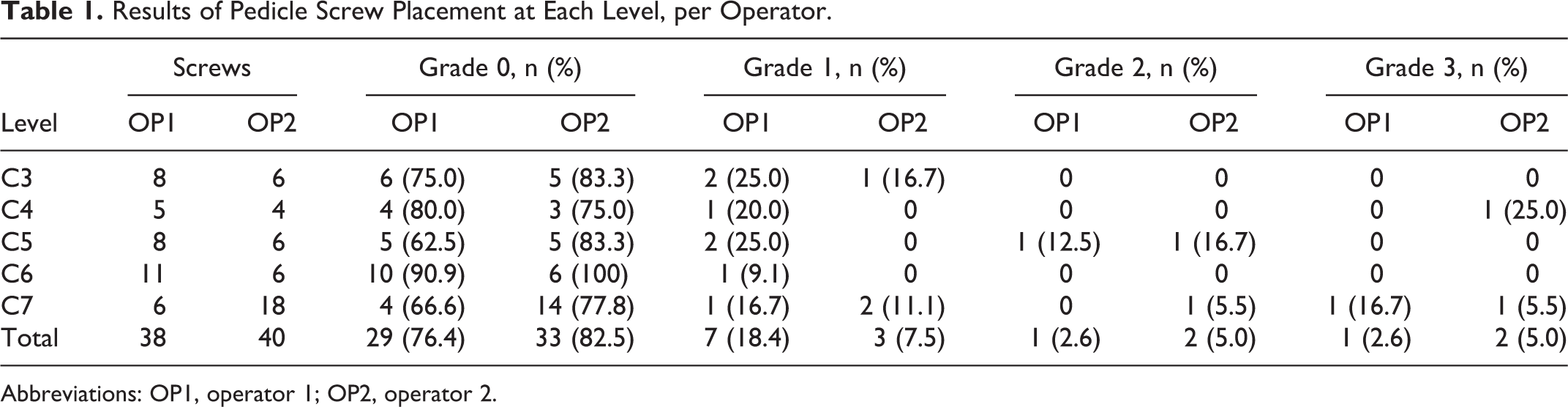
Abbreviations: OP1, operator 1; OP2, operator 2.
Results of Pedicle Perforation Direction, per Operator.
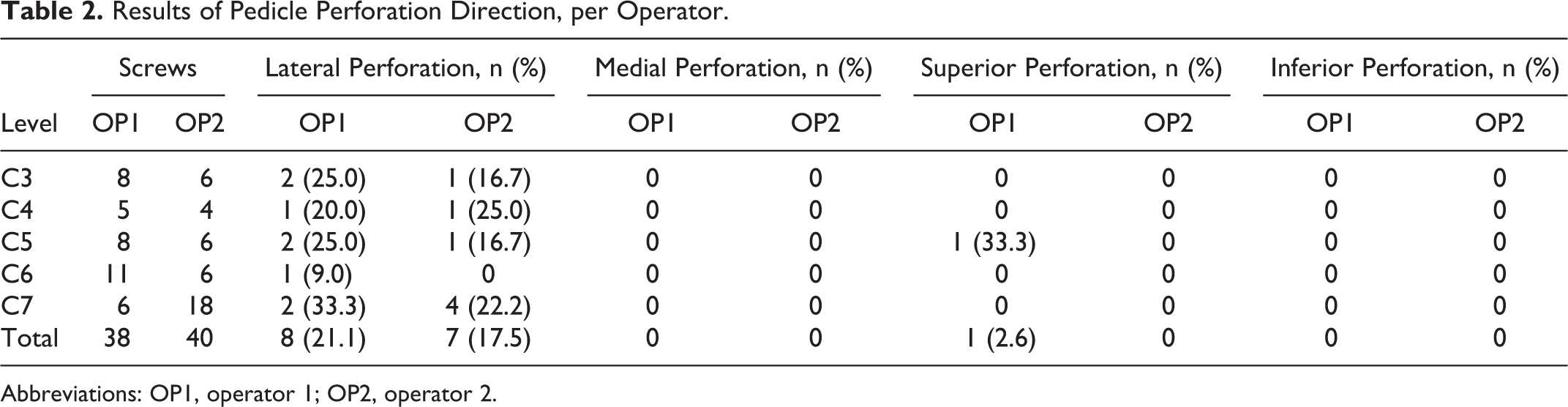
Abbreviations: OP1, operator 1; OP2, operator 2.
Screw Sizes at Each Level.
Discussion
Biomechanical studies have reported that CPS provides greater stability than other posterior cervical fixation procedures. 2,22,23 Therefore, the fusion level can be reduced compared with a lateral mass screw and wide lateral mass can be secured to obtain a sufficient fusion bed. If the screw-rod system is used for cervical fixation, secure screw fixation should be as firm as possible for optimal initial stability. Therefore, a tight fixation of screws is required to obtain sufficient initial stability of cervical segments. It would be another potential salvage option to convert to a CPS. Patients with poor bone quality, severe spinal trauma/injuries (eg, lateral mass fracture), multilevel instability, and cervical spine deformity can be good candidates. CPS can provide more rigid stability for posterior instrumentation, although it is a more technically demanding procedure with potential risk for neurovascular complications. Several complications of CPS have been reported. 11,24 -26 First, the most terrifying complication is vertebral artery (VA) injury. However, direct VA tear or rupture is extremely rare, and narrowing of the VA canal rarely causes actual symptoms associated with VA insufficiency. Consideration should also be given to root injury from misplaced screws. However, root injury has been reported to be rare, and when it occurred, it was mostly transient.
Since Abumi and colleagues described the first CPS insertion technique, several techniques have been reported to improve the safety of the CPS insertion. 5,7,21,27 However, the definite, detailed, and reproducible surgical method determining the entry point and trajectory of the CPS was not confirmed. Recently, various spinal image-guided techniques have been reported to encourage safe CPS insertion. 3,17,19,20,28 -30 With 3D image guidance, the rate of significant pedicle violation was 0.7% to 6.2%. 3,19,20,29,30 However, considering misregistration, the screw misplacement rate increased up to 23.4%, and navigation errors cannot be ignored, because of movable cervical vertebrae during the procedure. 20 Despite the higher rate of screw malposition with the technique without guidance, the incidence of neurovascular complication remains low. 7,9,11
The placement of pedicle screws using a free-hand technique is protective for surgeons from radiation exposure and effective for reducing operation time. 31,32 Because there is no fluoroscopy, it is possible to operate in a comfortable posture, and the surgeon’s concentration can be maintained. Therefore, an accurate and reproducible free-hand CPS technique combining the advantages of the CPS and free-hand techniques is needed. Our method does not require any fluoroscopic guidance at all and shows reproducible CPS insertion. As mentioned above, operator 2 could learn this technique from operator 1 without difficulty once and could perform it immediately.
Practical Considerations for CPS Insertion
The entry point differs from person to person and varies from level to level; thus, there is no definite and constant anatomical landmark. Our method does not have a fixed entry point; first, a minilaminotomy is performed to secure direct visualization of the pedicle, and the entry point is set accordingly. Thus, we can adopt the entry point to each pedicle. It is important to analyze the anatomical structure carefully, and the entry point and trajectory of screw placement should be individually customized via preoperative CT (Figure 1).
In our experience, there was no medial direction perforation in 78 screws in a series of 22 consecutive. The visualization of the medial wall of the pedicle throughout the whole procedure under the microscope makes the possibility of medial wall perforation rare. Otherwise, most of the pedicle violations were directed laterally. A lateral breach can cause catastrophic VA injury, and for this reason, many surgeons are reluctant to use CPS insertion, especially the free-hand technique. As with the pedicle screw insertion at the thoracolumbar spine, it is impossible to visually check the lateral breach of the pedicle when performing CPS. Therefore, it is important to check the trajectory of the cervical pedicle in the preoperative CT scan and ensure sufficient convergence angle during screw insertion. Tactile feedback through the Lenke probe during pedicle probing can also be an indicator that the screw trajectory entered the cancellous channel along the pedicle. Meticulous ball-tip probing to confirm pedicle walls help prevent critical pedicle wall breach. Finally, after CPS insertion, we confirm the position of the CPS with C-arm fluoroscopy.
Fortunately, despite lateral pedicle perforation, significant VA injury has been rarely reported. The present study revealed that, overall, there was a 20.5% pedicle perforation rate (grades 1, 2, and 3)—93.8% lateral and 6.2% superior and medial perforation rates—without neurovascular complications. Several reports explained that because of the relatively large space between the transverse foramen and artery, even if the screw is placed incorrectly, VA perforation or obstruction is rare. 23,32
We think that by replaying the operation procedure step by step with actual intraoperative photographs, many surgeons can learn the free-hand CPS insertion technique intuitively. The medial wall of cervical pedicles is significantly thicker than the lateral wall. This is one of the reasons why screws tend to perforate laterally. Considering the characteristics of the cervical pedicle, the tapper and screws should target somewhat medially more than the estimated trajectory. Therefore, it is important to dissect the paraspinal muscles laterally enough to secure the visual field and the convergent trajectory. Besides, inadequate laminotomy would cause insufficient visualization of the medial wall of the pedicle. During a laminotomy, it should be performed until the proximal segment of the pedicle continuing from the lateral mass is visible, so that a full length of the pedicle is exposed. Inadequate laminotomy could mask the pedicle and underestimate the convergence angle of the screw. The medial wall of cervical pedicles is usually concave laterally. If the distal segment of the medial wall is not visualized, the convergence angle could be underestimated. The medial wall should be dissected meticulously using a microdissector to visualize the full length of the medial wall under a microscope (Figure 2C).
Conclusion
We performed free-hand CPS insertion in patients with 92.3% correct position without any clinical complications. Free-hand CPS placement via para-articular minilaminotomy seems to be feasible and reproducible.
Footnotes
Authors’ Note
The manuscript submitted does not contain information about medical device(s)/drug(s).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) have no financial interests in any of the drugs, materials, or devices described in this article.
Supplemental Material
The supplemental material video is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.