
Abstract
Study Design:
Narrative Summary Review for Navigation & Robotics Focus Issue.
Objective:
To discuss the challenges and complications of S2-Alar-Iliac (S2AI) spinopelvic fixation using freehand techniques, and to introduce the utility of navigation & robotics to enhance patient safety.
Methods:
This study involved search of literature using the PubMed database, including retrospective clinical studies, anatomic reports, and surgical reports. The intention was to find literature that discussed complications regarding screw malfunction from manual S2AI placement, anatomical complexity of the sacroiliac joint, and outcomes of S2AI procedures conducted with robotic guidance systems.
Results:
The sacroiliac joint presents numerous complexities that can lead to challenges in free-hand placement of the S2-alar-iliac screw. Anatomic considerations of the S2AI screw involve close proximity to vital neurovascular structures, including: superior gluteal vessels, external iliac vessels, pudendal vessels, superior gluteal nerves, sciatic nerve, sympathetic chain ganglia, and pudendal nerves. The complications associated with manual S2AI screw installation include screw misplacement, breach of cortical bone, and injury to neurovascular structures. Robotic techniques for establishing S2AI screws involve greater accuracy of screw placement and reduced complications.
Conclusions:
Accurate placement of S2AI screws is compromised by variation in pelvic anatomy and by a pathway that traverses dense cortical bone of the sacroiliac joint. Accurate placement of S2AI screws is important for patient safety regarding neurovascular structures, and for effective, stable fixation across the SI joint. Robotic navigation of S2AI fixation offers significant utility in improving the accuracy of screw placement and patient safety.
Background
Pelvic fixation is important in spine surgery constructs that involve significant stress across the lumbosacral junction and spinal fixation at the lumbosacral spine for conditions including spinal deformity, dysplastic spondylolisthesis, multilevel fixation to the sacrum, fixed obliquity of the lumbosacral junction, and tumor or trauma at the lumbosacral junction. The technique is necessitated due to high stresses placed across the lumbosacral junction. 1 The purpose of pelvic fixation is to reduce strain on S1 screws, and to improve stability of lumbosacral fixation and fusion rates. Cunningham et al demonstrated that cantilever forces for long segment constructs become critical when the sacral fusion extends to L3 or higher. 1 Biomechanical studies have demonstrated that pelvic fixation extending beyond the pivot point at the anterior margin of the sacrum significantly reduces S1 screw strain in moments of anterior flexion, posterior extension, and lateral bending.2,3 The S2 Alar Iliac(S2AI), technique is an important method for pelvic fixation, proposed in 2007, to achieve pelvic fixation with a lower profile and more cortical fixation than traditional iliac fixation. 4 As described by Jain et al, the procedure involves a starting point midway between the S1 and S2 dorsal foramina, with the screw crossing the sacroiliac joint and terminating at the anterior inferior iliac spine (AIIS). 5 Advantages of the procedure compared to traditional iliac screws include less screw prominence, reduced necessity for dissection, and presence of structures that can be easily palpated to guide the screw pathway. 5 Figure 1 displays a representation of pelvic fixation utilizing the S2-alar-iliac screw.

Posterior spinal arthrodesis supplemented with pelvic fixation involving iliac and S2-alar-iliac screws.
The path of the S2AI screw involves crossing the sacroiliac joint, a complex structure that can present challenges for accurate screw placement. Moreover, traversing across 3 cortical regions presents additional complexity to the procedure, which is further exacerbated by proximity to many neurovascular structures that can be at risk of breach with improper placement. 6 The freehand technique is challenging due to variation in the anatomy of the sacroiliac joint, difficulty in cortical bone deflecting a gearshift, and a relatively narrow intraosseous and interosseous channel, with significant risk to neurovascular injury from anterior or posterior deflection across the SI joint. 6 Even with fluoroscopic guidance, which can enhance the clinician’s ability to visualize the joint space, the S2AI screw positioning is still challenging due to the complex anatomy of the sacral-pelvic region. 7
Robotic-assisted surgery presents the capability to improve the quality and safety of the S2AI procedure. Capabilities described by Laratta et al include effective tracing of path trajectory through utilization of imaging software. 8 The purpose of this paper is to discuss the challenges of S2AI freehand techniques and to introduce the utility of navigation and robotics to improve the safety of the procedure.
Methods
This narrative review involved search of published literature through the PubMed database, which consists of citations from a variety of life science journals. The intention was to find literature that discussed the anatomical complexity of the sacroiliac joint in relation to the S2AI surgical procedure, complications due to screw malfunction from manual S2AI placement, and outcomes of S2AI procedures conducted with robotic guidance systems. The study inclusion criteria were broad and included retrospective clinical studies, anatomic reports, and surgical reports. The literature search utilized key words corresponding to each section of this study.
To determine the standard methodology of S2AI surgical techniques and associated challenges, key words such as “surgical techniques,” “challenges,” and “S2-Alar-Iliac” were utilized. A variety of surgical technique reviews and surgical reports delineating step-by-step instructions for the procedure were found. After screening results through abstract review, focus was given on studies that included common challenges and pitfalls of the surgical techniques. Such studies were deemed most relevant.
To find published literature on complications of the freehand S2AI screw installation, relevant key words such as “screw misplacement,” “screw breakage,” “S2AI accuracy,” “S2AI safety,” and “perioperative S2AI complications” were utilized. The final portion of this focus issue was to determine the potential for robotics and navigation to enhance S2AI screw placement and prevent complication rates. Literature search was conducted through PubMed to identify clinical studies that analyzed the accuracy and rates of screw misplacement or breakage in S2AI procedures conducted with robotic navigation and guidance systems. For all studies identified, references to included publications were also examined to determine additional sources of relevance.
The Sacroiliac Joint
The sacroiliac joint presents numerous complexities that can lead to challenges in free-hand placement of the S2-alar-iliac screw. As the largest axial joint with complex ligamentous support and common dysmorphism that is poorly understood, interventions present numerous complexities. Portions of the regular pelvic anatomy of the joint as well as the variability in shape due to various pathologies can lead to difficulties in carrying out the procedure. The procedure itself is outlined by Jain et al, who describes the 6 main steps of S2-alar-iliac screw insertion: patient positioning, surgical approach, channel creation, screw placement, rod placement, and wound closure. 6 As described, the screw must begin at the junction between the 1st and 2nd dorsal sacral segments, cross the sacroiliac joint, travel caudally toward the sciatic notch, cross between the inner and outer tables of the ilium, and end close to the anterior inferior iliac spine cranial to the acetabular roof closure. A surgical technique review by Laratta et al emphasizes that the path of the insertion must be precise. 8 This technique review gives a rough estimate of the starting point for the S2-alar-iliac screw as 1 mm inferior and lateral to the S1 dorsal foramen, with the screw angulated 40º inferiorly and 40º laterally from a line connecting the posterior-superior-iliac spine. However, the exact medial to lateral angulation can vary depending on patient variation in pelvic anatomy. 9 Due to the necessity for a precise angle as well as important neurovascular structures that come within close proximity to the sacropelvic area, it is clear that the procedure can present challenges when conducted with free-hand techniques.
Profuse Bleeding due to Violation of Soft Tissue Overlying S1 and S2 Dorsal Foramina
As stated by Jain et al, a limited dissection of soft tissue is conducted between the S1 and S2 dorsal foramina, followed by palpation to locate the S1 and S2 foramina with a blunt surgical instrument. 6 Following the dissection, the starting point of channel creation is then determined in-line at the mid-point of the foramina. The study highlights that excessive violation of soft tissue can occur and result in profuse bleeding that can hamper visualization and the remaining procedural techniques.
Cortical Breach of Ilium
Typically, a cannulated screw is advanced over a guidewire that is directed from the mid-line of the S1 and S2 dorsal foramina toward the anterior inferior iliac spine (AIIS). A variety of studies point to an approximate trajectory of 20º-40º angle caudally with a 30º-40º angle laterally.5,10,11 Jain et al points out that cortical breaches are common laterally along the outer table of the ilium, and that such breaches can be prevented by directing the screw at a more caudal angle, closer to the bone proximal to the sciatic notch. 6 However, the study indicates that if resistance is encountered when advancing the drill or awl, it can suggest that the device is about to breach the lateral ilium wall, necessitating either a new starting point or redirection of the awl.
Redirection of Surgical Instruments Resulting in Mal-Positioning
Jain et al also indicates that when an awl or drill crosses the sacroiliac joint, there is potential for anterior deflection, and a curved probe may be required to correct the angle and redirect the surgical instrumentation. 6
Variation in Pelvic Anatomy due to Individual Patient Variation and Pathologies
Individual patient anatomies can present the necessity to vary angulation of the S2AI screw. Ko et al conducted a case-control study in which 27 patients with scoliosis and severe cerebral palsy underwent computed tomography, with measurement of angles of the upper and lower ilium with respect to sacrum, acetabular anteversion, and sacroiliac joint angles. 9 Results from the study showed that subjects had significantly more iliac angle asymmetry (P = 0.01) and asymmetry of at least 10 degrees in the following categories: upper ilium, above the sciatic notch, and the sacroiliac joint. It is quite feasible that a transverse plane asymmetry of the pelvis may increase the risk for lateral breach of the iliac wing, especially given the deviation in caudal and lateral screw angulation needed to achieve proper fixation.
Anatomic Considerations for the S2AI Screw
Osseous Anatomy
The insertion of the S2AI screw requires careful probing into the starting point between the dorsal sacral foramina, navigation across the sacroiliac joint, and successful route through the ilium to reach the AIIS (anterior inferior iliac spine). A variety of anatomical features are easily visible and can be palpated within the sacrum and pelvis to ensure proper insertion of the screw. Relevant osseous landmarks for reference of the S2AI screw are displayed in Figure 2 for the posterior view, and Figure 3 in the anterior view along with major vasculature.
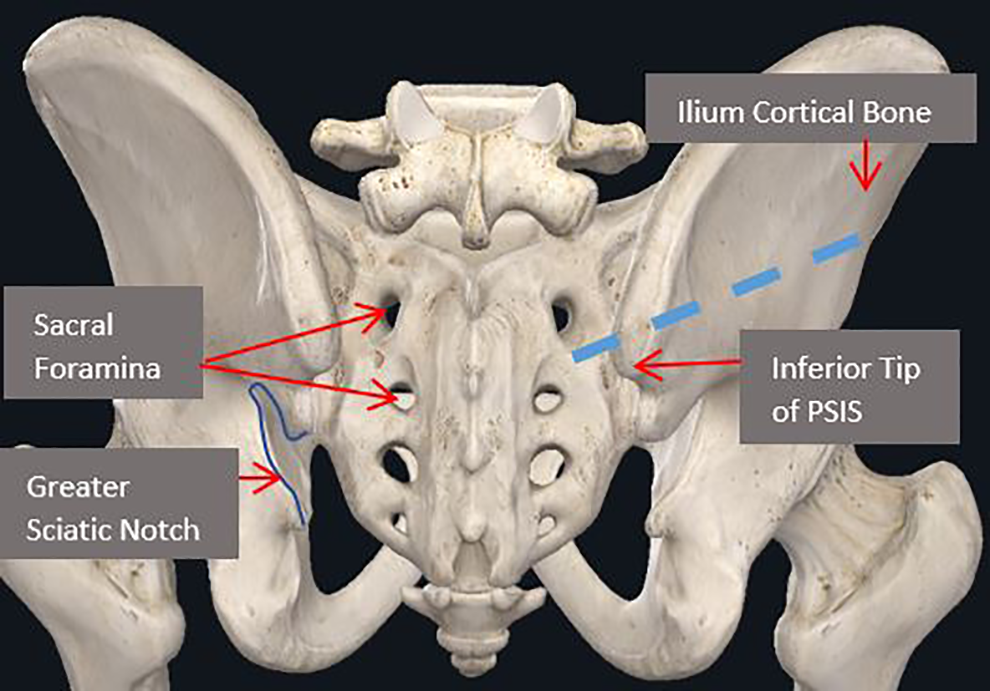
Posterior view of osseous landmarks. Note that blue dashed lined is path for the S2AI screw. Image courtesy of complete anatomy.
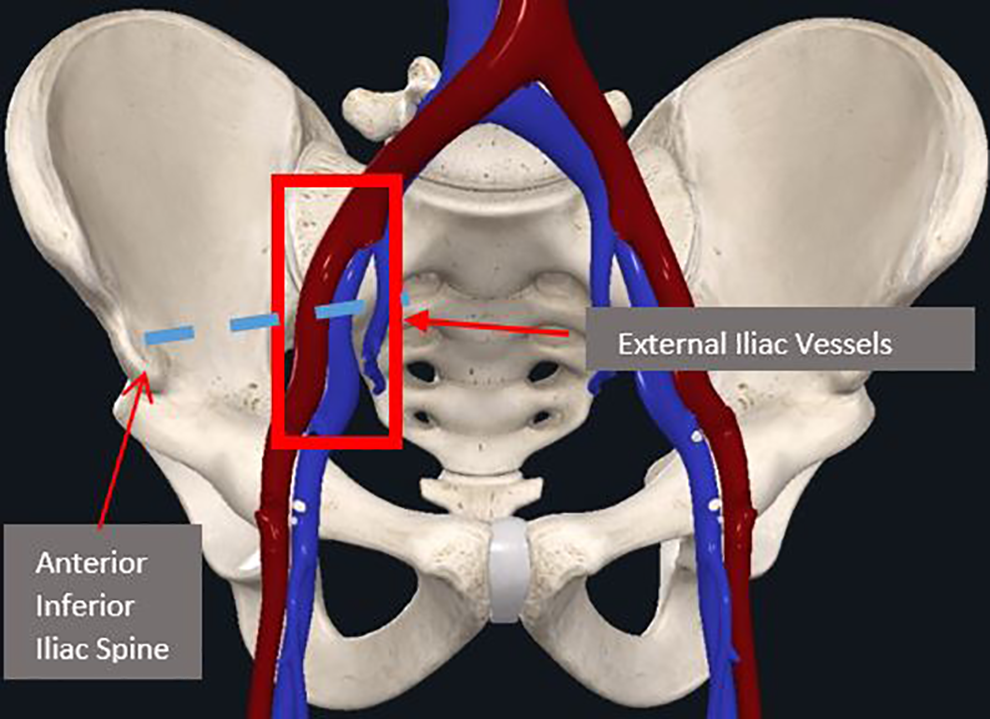
Anterior view of vascular structures. The red box indicates vessels that lie in anterior pelvis within proximity to the S2AI screw, within the sciatic notch. Moreover, the S2AI screw terminates at the AIIS, indicated by the arrow. Note that blue dashed lined is path for the S2AI screw. Image courtesy of complete anatomy.
As described by Shillingford et al, the procedures can be completed with or without fluoroscopic guidance. 12 However, the path of the screw remains the same and involves passing through 3 cortical surfaces. A technical considerations manual by Laratta et al gives insight into the S2AI screw progression through the osseous structures. 8 First, the entry point is located lateral to the midpoint between the S1 and S2 foramina, a burr is used to establish a 5 mm cortical breach, and then a pedicle probe is advanced toward the sacroiliac joint. The next step indicated in the manual involves breaching the sacroiliac joint, where the probe is directed posteriorly to avoid an anterior perforation. This is likely necessary to avoid the common iliac vessels, which lie close to the anterior edge of the sacroiliac joint.
After passing the joint, the pedicle probe is directed toward the AIIS through the thick iliac cortical bone by aiming to a point superior (cephalad) to the posterior distal edge of the PSIS. 8 The benefit of aiming superior to the PSIS is possibly to ensure that the screw avoids the sciatic notch, which houses many neurovascular structures. The majority of literature is in agreement that the optimal position of the screw must lie directly superior to the sciatic notch, within the thick cortical bone of the ilium.6,8,12
Vascular Anatomy
The S2AI screws are within close proximity to a variety of vascular structures that lie both inferiorly and superiorly to the starting point entrance (mid-point between dorsal sacral foramina). Anteriorly to the insertion site lie the common iliac vessels, which can be at risk of puncture during the procedure. 13 Observe Figure 3 for reference. Inferiorly, within the sciatic foramen, lie the superior gluteal vessels as well as the internal pudendal vessels, all of which are close to the S2AI screw insertion. 14 See Figure 4 for reference.
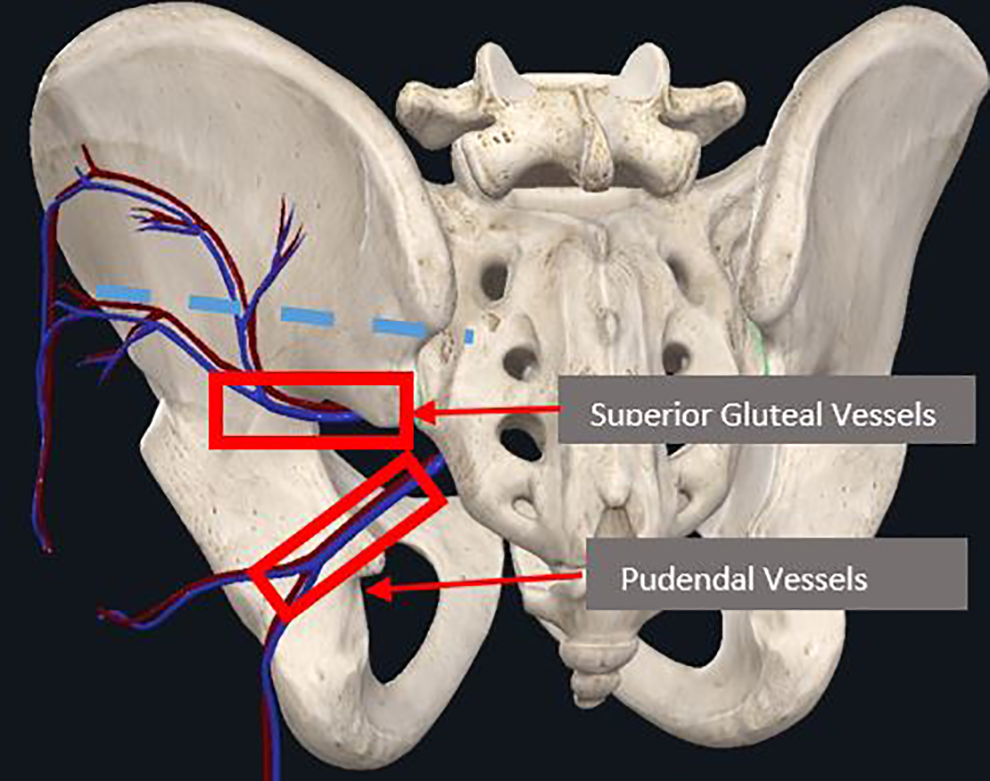
Posterior view of vascular structures. The red box indicates vessels that lie inferior to the starting point of the S2AI screw, within the sciatic notch. Note that blue dashed lined is path for the S2AI screw. Image courtesy of complete anatomy.
Neural Anatomy
The S2AI screws also lie within close proximity to a concentration of critical neural structures. Such structures can be compromised from both inferior and anterior violations during S2AI installation. 5 Anteriorly, the sympathetic chain ganglia, L5 & S1 nerve roots, as well as the femoral nerve are potentially comprisable structures (Figure 5). 15 Inferiorly, within the sciatic foramen, lie the sciatic nerve and the pudendal nerves, while posterior-superiorly lie the superior gluteal nerves (Figure 6). Inferior violations and cortical breaches, respectively, could lead to damage of the structures.
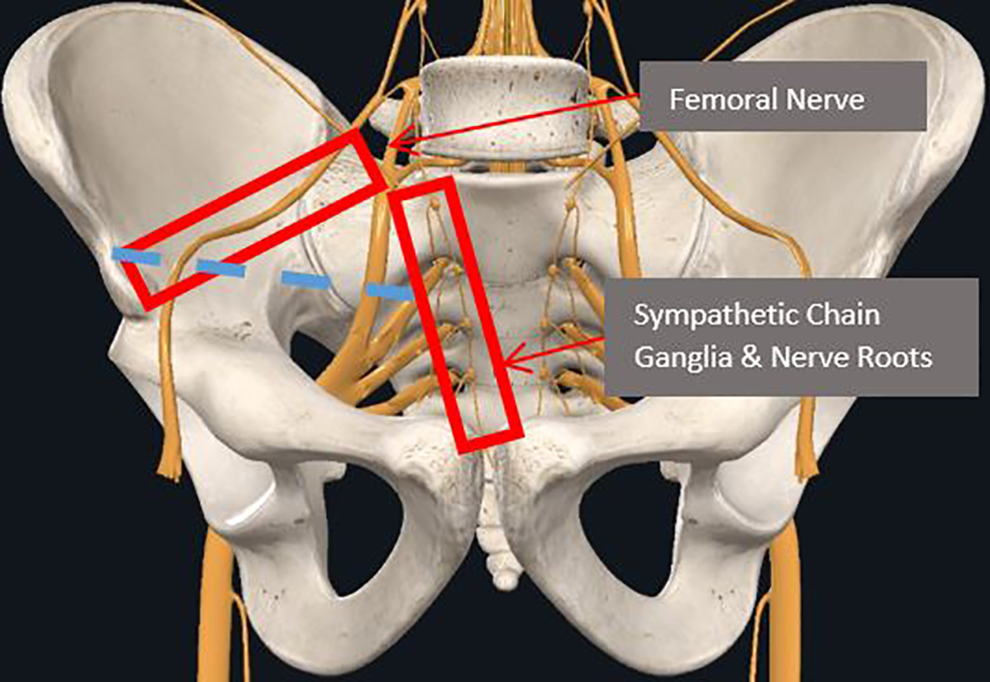
At-risk neural structures that lie anterior to the S2AI screw. Note that blue dashed lined is path for S2AI screw. Image courtesy of complete anatomy.
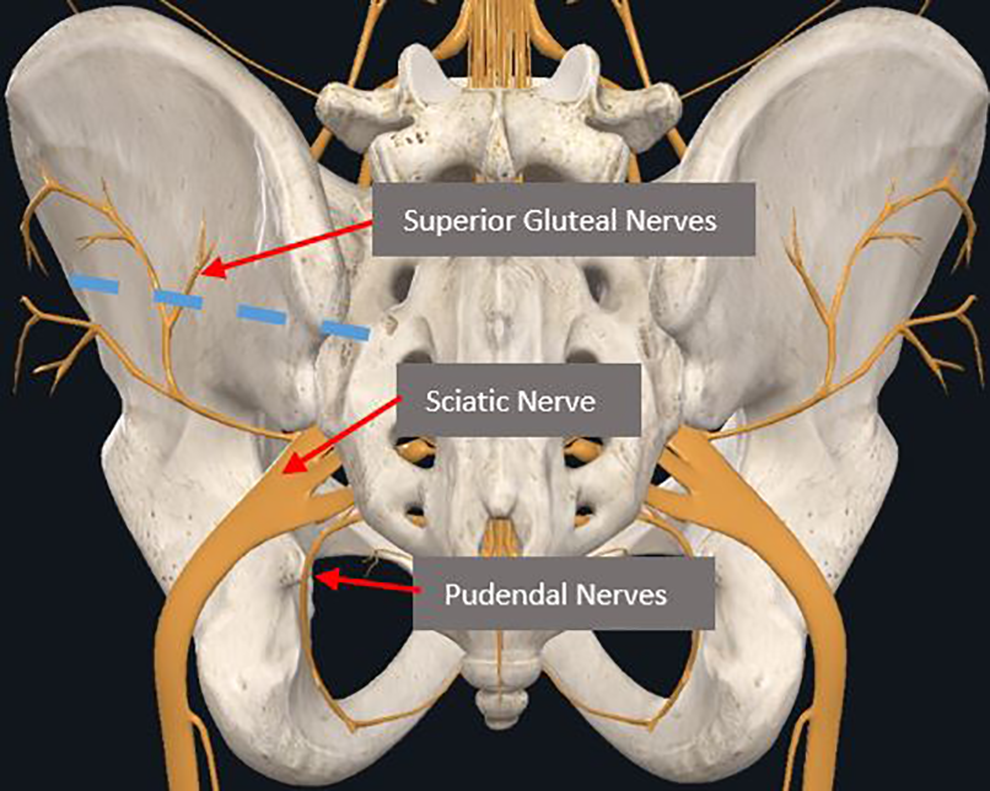
At-risk neural structures that lie inferior & posterior-superior to the S2AI screw. Note that blue dashed lined is path for S2AI screw. Image courtesy of complete anatomy.
Complications in Freehand S2 Alar Iliac Techniques
Complications in S2-Alar-iliac pelvic fixation fall into 3 categories: screw misplacement with cortical breach, misplacement without cortical breach, and neurovascular complications. Select case, anatomic, and clinical studies have documented potential devastating consequences in settings where freehand fixation has been used alone or along with CT and fluoroscopic guidance systems.
Screw Misplacement
Screw misplacement is a broad term that includes improper angulation of the S2-Alar-Iliac screw, breach of the cortical wall, or anterior and posterior violation while probing across the sacroiliac joint.5,7,8 Each error could result in surgical complications ranging from re-positioning of the screw to injury of neurovascular structures.15,16 Many studies have detailed such breaches. In a retrospective clinical study of 45 patients undergoing spinopelvic fixation via S2AI screws, Shillingford et al examined screw angles and accuracy through CT evaluation, measurement of caudal & sagittal angles, and presence of anterior or posterior breaches. 12 The study found that the difference in the average horizontal angle approached significance: 38.9º ± 8.2º for screws without breach compared with 44.4º ± 6.8º for those demonstrating a posterior breach (P = 0.082), effectively showing that very slight changes in angulation can produce risky cortical breaches, requiring salvage of path through repositioning. Moreover, an anatomic study of the S2AI technique by O’Brien et al was conducted on 10 cadaveric specimens that underwent placement of S2AI screw. 16 Using CT scanning to determine structures at risk of injury, cortical violations, and characteristics of screws placed, the study found that articular violation occurred in 60% of the placed S2AI screw. It is noted that even despite CT guidance to enhance visualization, such articular violations still occurred-highlighting the challenges posed by complex sacroiliac joint anatomy.
However, some retrospective clinical studies point to lesser incidence of complications due to screw misplacement. Park et al, in a clinical case series of 23 patients undergoing S2AI placement for pelvic fixation, found that there were no cases of neurological deficit and violation of acetabulum or sciatic notch. 17 The only abnormalities found at the study’s conclusion were a peri-screw halo in 1 patient and cortical wall violation in 4 patients, and the number of lateral and medial breaches were 2 and 3, respectively. Although the study reported that all patients were asymptomatic, it is notable that screw misplacement is still a common event even if complications do not result. A similar result was found by Zhao et al, who utilized bilateral S2AI placement under guidance of a 3D printed surgical template for 27 patients in a retrospective clinical study in which placement of the screw was postoperatively graded on a scale ranging from grade 0(screw fully surrounded by bone) to grade 3(severe, breakthrough distance >6 mm), with the breakthrough distance defined as the shortest distance from the furthest end of the penetrating screw to the adjacent cortical bone. 18 During the operation, all screws were successfully placed in the ilium, except for 2 screws that slightly invaded the medial cortical bone (grade 1). Therefore, the results from studies regarding screw misplacement yield the conclusion that small variations in angulation can produce potential breaches, and that although such breaches may or may not result in complications, they can occur relatively frequently.
Neurovascular Complications
Although not documented in large clinical studies, individual case and anatomic studies have determined that the freehand S2AI screw insertion poses risk to neurovascular structures.19-21 Abdul-Jabbar et al found in an anatomic study that removing the bone around the S2AI-screw illustrated the close relationship to the medial internal neurovascular structures, including the obturator nerve, lumbosacral trunk, sacral plexus, S1 ventral ramus, and iliac vein and artery. 19 The anatomic study found that by removing the outer cortex of the ilium, there was also a close proximity to the superior gluteal artery, vein, and nerve, as well as the internal iliac vessels.
In addition to presence of neurovascular structures located in proximity to the site of insertion, variations in individual patient anatomy can place such structures at increased risk of breach. 9 Marmor et al documents a case in which the superior gluteal artery was injured during iliosacral screw placement due to aberrant patient anatomy, in which the patient’s superficial branch of the superior gluteal artery measured more than twice the average length. 20 Therefore, the possibility of anatomic variance paired with presence of neurovascular structures in close proximity to the screw only increases risk of complications. Collinge et al also details risks to the superior gluteal neurovascular bundle during percutaneous bilateral freehand iliosacral screw insertion in an anatomical cadaver study of 29 cadaver pelvises. 15 Here, the study reported that 10 of the 58 (18%) iliosacral screws caused injury to the superior branch of the superior gluteal nerve and vessels, with 8 of the screws violating neurovascular bundles, and the remaining 2 entrapped between the screw head and ilium; most importantly, all such screws that caused gluteal neurovascular injury were also located within the intended area of insertion. In conclusion, it is evident that the potential for injury to neurovascular structures during S2-Alar-Iliac spinopelvic fixation is high when the current standard freehand techniques are utilized.
Role of Navigation and Robotics to Improve Accuracy and Safety in Pelvic Fixation
S2AI fixation requires a precise screw trajectory with little room for error to avoid breaching the cortical wall and neurovascular structures. 10 The incremental value of navigation and robotics needs to be understood in context of fluoroscopy-based screw placement. 22
S2AI Screw Fixation Assisted by Freehand or Fluoroscopy-Based Navigation: Advantages and Disadvantages
S2AI screw fixation procedures can be conducted with reasonable accuracy by freehand techniques but fall short in the control of radiation exposure and minimization of blood loss. 21 In essence, fluoroscopy-based navigation requires multiple fluoroscopic projections that are attained in the intraoperative setting to improve accuracy of screw placement.23,24 However, the usage of such imaging can present difficulties for the clinician, especially when adapted to the S2AI procedure. For example, Yamada et al suggests that the success of fluoroscopic guidance in preventing anterior deviated S2AI screws hinges on having a pelvic inlet view tilted precisely at 60º-70º from the S1 slope, with an additional lateral view needed to confirm that there is no caudal deviation. 25 Moreover, radiation exposure to the clinician and to the patients is significantly higher with intraoperative fluoroscopy compared with CT guided navigation. 26 A retrospective study by Baky et al compared outcomes in 217 patients who had pedicle screws placed via low-dose CT-guided navigation and fluoroscopic guidance, finding no significant difference in blood loss, accuracy, or operative time. 27 Therefore, while live fluoroscopic guidance for S2AI screw placement is feasible and accurate, the radiation exposure and variance in image quality favor a CT-guided system. It is clear from these findings that the clinician must adhere to very narrow instrumentation settings and keep in mind such technical details. Image quality can vary depending on the imaging system, while clinician and operator experience also play a role in success with fluoroscopic guidance. 25
Technical Procedural Considerations of Robotics That Lend Advantages Over Freehand Techniques
Robotic techniques for establishing S2AI screws lend a considerable advantage over those of freehand techniques conducted with or without navigation. As outlined in a technique review by Shillingford et al, freehand techniques involve repeated steps of removing the gearshift and confirming intraosseous placement with a ball-tipped pedicle probe, both while advancing toward the SI joint and after crossing it. 12 Moreover, the review indicates the curve blunt-tipped gearshift must be directed posteriorly to avoid anterior deflection while advanced toward the SI joint, then rotated anteriorly as the joint is breached. In essence, the techniques for freehand placement require repeated steps to ensure the trajectory is accurate, all which can potentially increase the operative time, radiation exposure, and possibility for error. Robotic techniques remove the necessity for utilizing repeated x-rays to ensure an accurate trajectory. 7
Utilization of Navigation & Robotics Enhances Procedure Times, Reduces Radiation Exposure, and Reduces Blood Loss
A variety of clinical studies within the literature support the enhanced patient safety and advantage of robotic-assisted spinopelvic fixation. One cadaveric implantation trial by Lieberman et al implanted 234 pedicle screws in 12 cadavers via robotic guidance system, finding that relative to freehand placement, the robotics group had lower surgeon radiation exposure (136 mrem vs 4.2 mrem), lower fluoroscopy time per screw(33.0 seconds vs 0.9 seconds), and shorter procedure time(1.98 hours vs 1.23 hours). 28 Another matched-cohort comparison study comparing free-hand guided pedicle screw insertion assisted by fluoroscopy and robot assisted pedicle screw insertion within the lumbar spine found that blood loss was significantly lower in the robot-assisted group. 29 While it is noted that these studies focused on pedicle screw fixation, as opposed to S2AI screws, parameters such as procedure time, radiation exposure, and blood loss still pose broad implications to patient and clinician safety. Combined with an enhanced intraoperative workflow, efficacy, and cost-effectiveness, robotics present a significant advantage in facilitating S2AI spinopelvic fixation procedures when compared to current freehand methods. 30
Complications & Screw Misplacement Rates From Robotically Guided S2AI Procedures Are Minimal
The complication rates from robotically guided S2AI screws are low and present a reasonable alternative to freehand techniques. Many clinical studies have verified high screw accuracy using robotic guidance. In one example, Shillingford et al conducted a retrospective matched cohort analysis of 51 patients, finding that there was no significant difference between the accuracy of screw placement in the freehand group with fluoroscopic guidance and the robotics group (94.9% vs 97.8%, P = 0.63). 21 Although not significant, the study reported 5 and 2 cortical breaches(P = 0.46) as well as 3 and 1 breaches(P = 0.63) in the free-hand group and robotically-guided group, respectively, with similar breach distances. Laratta et al, in a case series study of 23 patients who underwent spinopelvic fixation, found that the overall robotic S2AI screw accuracy rate was 95.7%, with no intraoperative neural, vascular, or visceral complications related to the placement of the S2AI screws. 8 Additional retrospective studies by Bederman et al, Shillingford et al, and Hu and Lieberman also report that all trajectories established via robotic assisted S2AI placement were accurate, with no risk to any neurovascular structures.12,31,32 In conclusion, screw placement accuracy from robotic guidance systems is, at the very least, equal or better to that of freehand techniques with fluoroscopy. Along with lower radiation exposure, reduced blood loss, and an enhanced workflow, robotics offer significant utility in S2AI screw placement.
Conclusions
Pelvic fixation is important in spinal instrumentation across the lumbosacral junction. The S2AI screw is an effective technique for pelvic fixation that has advantages compared with traditional iliac screws regarding implant profile and stability of fixation. Accurate placement of S2AI screws is compromised by variation in pelvic anatomy and by a pathway that traverses dense cortical bone of the sacroiliac joint. Accurate placement of S2AI screws is important for patient safety regarding neurovascular structures, and for effective, stable fixation across the SI joint. Robotic navigation of S2AI fixation offers significant utility in improving the accuracy of screw placement and patient safety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.