
Abstract
Study Design:
Prospective single-cohort analysis.
Objectives:
To compare the outcomes/complications of 2 robotic systems for spine surgery.
Methods:
Adult patients (≥18-years-old) who underwent robot-assisted spine surgery from 2016-2019 were assessed. A propensity score matching (PSM) algorithm was used to match Mazor X to Renaissance cases. Preoperative CT scan for planning and an intraoperative O-arm for screw evaluation were preformed. Outcomes included screw accuracy, robot time/screw, robot abandonment, and radiation. Screw accuracy was measured using Vitrea Core software by 2 orthopedic surgeons. Screw breach was measured according to the Gertzbein/Robbins classification.
Results:
After PSA, a total of 65 patients (Renaissance: 22 vs. X: 43) were included. Patient/operative factors were similar between robot systems (P > .05). The pedicle screw accuracy was similar between robots (Renaissance: 1.1%% vs. X: 1.3%, P = .786); however, the S2AI screw breach rate was significantly lower for the X (Renaissance: 9.5% vs. X: 1.2%, P = .025). Robot time per screw was not statistically different (Renaissance: 4.6 minutes vs. X: 3.9 minutes, P = .246). The X was more reliable with an abandonment rate of 2.3% vs. Renaissance:22.7%, P = .007. Radiation exposure were not different between robot systems. Non-robot related complications including dural tear, loss of motor/sensory function, and blood transfusion were similar between robot systems.
Conclusion:
This is the first comparative analyses of screw accuracy, robot time/screw, robot abandonment, and radiation exposure between the Mazor X and Renaissance systems. There are substantial improvements in the X robot, particularly in the perioperative planning processes, which likely contribute to the X’s superiority in S2AI screw accuracy by nearly 8-fold and robot reliability by nearly 10-fold.
Keywords
Introduction
In recent years, there has been a growing interest among spine surgeons in robot-assisted surgery.1-4 One of the first FDA approved robot-assisted systems was the SpineAssist (Mazor Robotics) in 2004.5,6 Since that time, Mazor has released next generation systems, such as the Renaissance (2011) and Mazor X (2016). 7 Currently, the Mazor systems are available at 250 centers in 40 countries worldwide. 8 According to the literature, Mazor robots appear to be the most widely used and studied systems in the US.1-3,9,10
A plethora of literature exists on robotic systems with emphasis on pedicle screw accuracy, radiation exposure, and safety profile.11-14 In addition, much of the literature has compared robot-assisted spine surgery to freehand techniques. The increased accuracy of pedicle screw placement has been extensively studied, with multiple studies reporting accuracy as high as 99%.10,15-17 In 1 of the largest studies to date, only 1.7% of patients required revision surgery due to screw misplacement in 413 surgeries involving 2,067 pedicle screws. 16 In another study of 3,271 robot-assisted pedicle screw placements, 98% of screws were clinically acceptable when assessed with intraoperative fluoroscopy with only 4 cases (0.63%) requiring revision and no neurologic deficits after revision. 5 Overall, reported complication rates due to screw misplacement utilizing robotic assistance have been extremely low, ranging between 0% and 4%. 1 According to a recent systematic review, radiation exposure has decreased over time, thereby reducing the radiation risk to the operative team and patient. 9
Although robot-assisted spine surgery continues to be extensively studied, there is limited literature on the Mazor X system and no studies have compared the Mazor X and the Renaissance systems. It is important to investigate if recent advances in robotic technology have any clinical significance. The purpose of this study is to compare the screw accuracy, robot operative efficacy, and radiation exposure between the Mazor X and Renaissance robot systems. A single center investigation enables a detailed exploration of robot complications and radiation exposure that may be difficult for larger databases or multicenter studies. Furthermore, in comparison to prior studies, our study includes an assessment of both pedicle and S2 Alar-Iliac (S2AI) screws.
Materials and Methods
Patient Selection
We included adult (≥18 years old) patients who underwent robot-assisted spine surgery with either the Renaissance or Mazor X system (Mazor Robotics Ltd) between 2016 and 2019. The senior author used robot assistance for all consecutive cases which required instrumented fusion during the study period. After June 2017, only the Mazor X robot was used by the senior author. Patients with missing data were excluded from this study. All patients had a preoperative CT scan, intraoperative fluoroscopy for robot registration purposes, and an O-arm scan to verify appropriate screw placement. Two independent surgeons, who were not directly involved in the primary care of these patients, reviewed the intraoperative fluoroscopic images and O-arm CT scans of each patient. To more accurately measure screw trajectory and screw breaches, particularly for patients with irregular anatomy, the Vitrea Core (Vital Images, Minnetonka, MN) interactive imaging software was used. This software allows for three-dimensional analysis based on CT or O-arm imaging. Patients who did not have or were missing an intraoperative O-arm scan were excluded. This study was approved by the institutional review board.
Data Collection
Patient factors included gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA), Charlson Comorbidity Index (CCI), prior or current smoker, and osteoporosis. Indications for surgery were included as well. Operative factors included prior spine surgery, pelvic fixation, instrumented levels, interbody fusion, planned robot screws per patient, and discharge disposition. Several outcomes were of interest in this comparative analysis. Operative efficacy was characterized as operative time (minutes), robot time (minutes), and robot time per screw (robot time per screw). Robot-related complications included exchange of screw for breach and robot abandonment. Other operative complications unrelated to the robot included dural tear, intraoperative loss of motor/sensory function, perioperative blood transfusion, and return to the operating room during the same inpatient stay.
Propensity Score Matching
Patients in each robot cohort were matched using a propensity score matching algorithm to account for the potential selection bias in the 2 robot systems used. Various perioperative factors including patient demographics, comorbidities, primary diagnosis, and operative factors (e.g. instrumented levels, pelvic fixation, prior surgery, and number of planned robot screws per patient) were included in this algorithm.
For comparative and descriptive purposes, bivariate analyses were performed for perioperative factors and outcomes between the Renaissance and X. The Chi-square or Fisher’s exact test (where appropriate) and t-tests/ANOVA were used for categorical and continuous variables, respectively. Statistical significance was defined as a P-value < .05. Propensity score matching was performed in R version 3.0.2 (Vienna, Austria, http://www.R-project.org/) using the Matchlt (Ho, Imai, King, & Stuart, 2011) package. SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC). We used “nearest” matching method and discarded “treated” units outside the support of the distance measure of the control units.
Screw Analysis
The Vitrea Core software was used to review intraoperative O-arm CT scans and assess the screw trajectory in the axial, sagittal, and coronal planes simultaneously. Screw accuracy was measured according to the Gertzbein and Robbins classification. If there was no breach, the screw was classified as a Grade A; <2 mm deviation was a Grade B, <4 mm deviation was a Grade C, <6 mm deviation was a Grade D, and >6 mm deviation was a Grade E. The breach distance was recorded as well.
Robotic Systems
In 2011, the SpineAssist was replaced by Mazor’s 2nd generation robotic system, Renaissance. In comparison to the SpineAssist, the Renaissance had considerable advancements including proprietary software which enabled surgeons to preoperatively plan implant size and trajectories more accurately, several mounting platforms to serve as an interface between the patient and the robotic system, and the renaissance robotic device (RBT), which was a portable computer-controlled platform that spatially positioned and oriented surgical tools in accordance to the preoperative plan.
In 2016, the Mazor X system expanded upon the core technology of Renaissance to include a more sophisticated three-dimensional analytical software to improve preoperative planning and allow for intraoperative planning (“scan & plan” method) if a preoperative CT scan was not available. A major advantage of the Mazor X is the Mazor X Align application, which allows surgeons to better plan for spinal deformity cases. This application combines standing spine x-rays with CT-scan to predict the impact of corrective changes, such as osteotomies, on spinal alignment in sagittal and coronal planes. Other improvements of this system include an integrated three-dimensional camera with spatial tracking, a surgeon control panel in the sterile area, and a robotic arm which is designed to be serial, rather than parallel, to allow for a greater unrestricted range of motion and reduce the need for additional surgical tools in comparison to the Renaissance. The three-dimensional camera allows the robot to better self-detect its location and potentially reduce collision with the surgical environment. Furthermore, the Mazor X Eye camera enhances the precision and accuracy of implant placement by verifying the appropriate surgical arm position and trajectory prior to instrumentation at each level.
Results
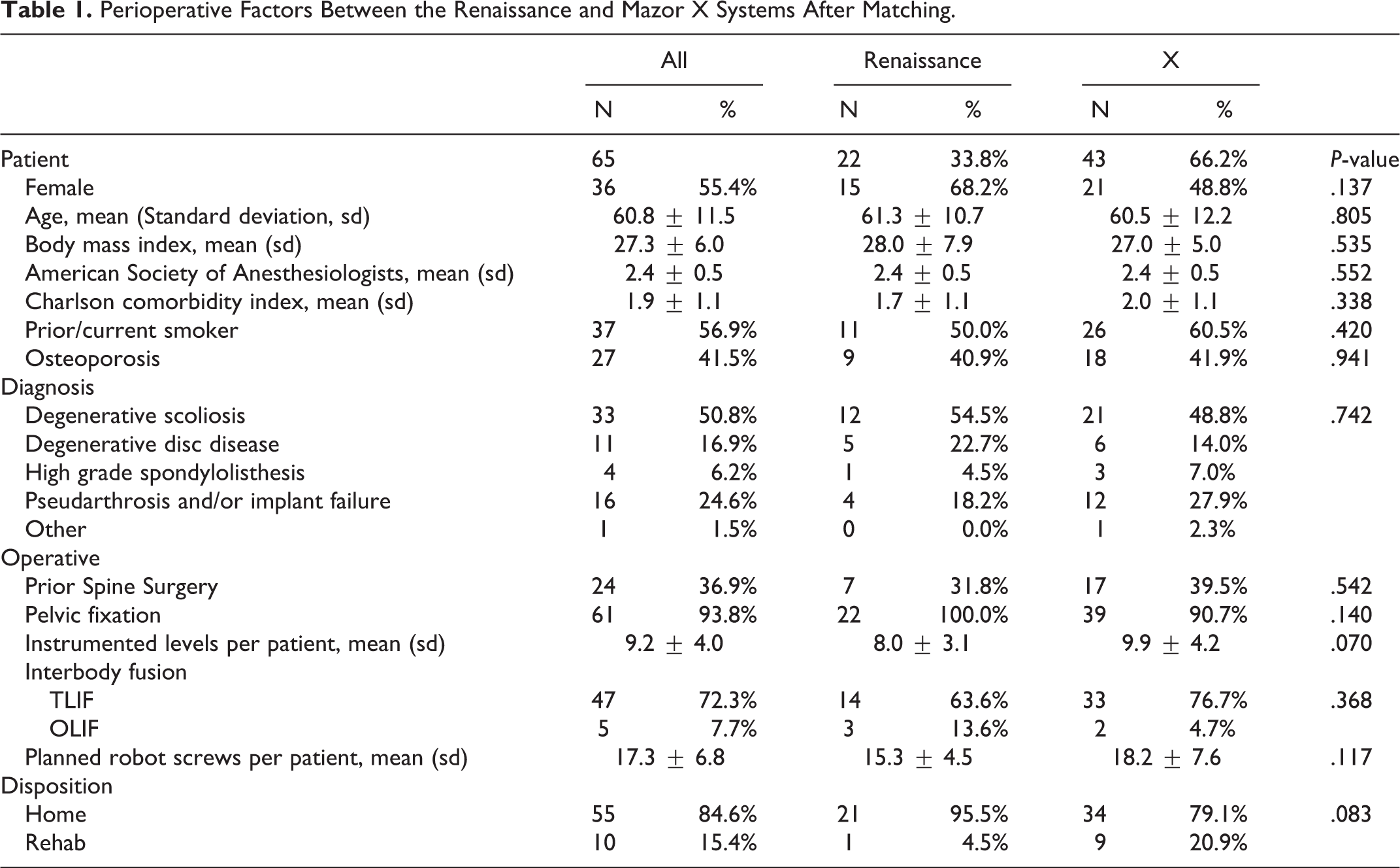
A total of 65 patients remained after propensity score matching (Renaissance: 22; X: 43). The patient demographics, comorbidities, indications for surgery, and operative factors were similar between cohorts as seen in Table 1. The mean age (standard deviation) was 60.8 (11.5) and 55.4% (N = 36) of patients were female. The mean ASA was 2.4 (0.5), mean CCI was 1.9 (1.1), and 56.9% (N = 37) of patients were prior or current smokers. The most common diagnoses included degenerative scoliosis (50.8%, N = 33), pseudarthrosis and/or implant failure (24.6%, N = 16), and degenerative disc disease (16.9%, N = 11). Overall, 36.9% (N = 24) of patients had prior spine surgery, and 93.8% (N = 61) of patients had pelvic fixation. The mean number of instrumented levels per patient was 9.2 (4.0), mean number of planned robot screws per patient was 17.3 (6.8), and 72.3% (N = 47) of patients had a transformainal lumbar interbody fusion (TLIF). The majority of patients were discharged home (84.6%, N = 55) (Table 1).
Perioperative Factors Between the Renaissance and Mazor X Systems After Matching.
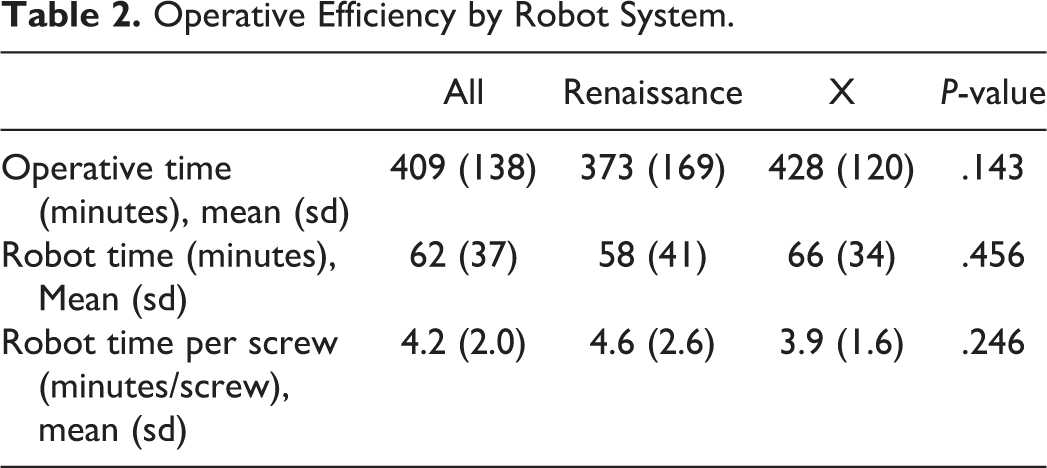
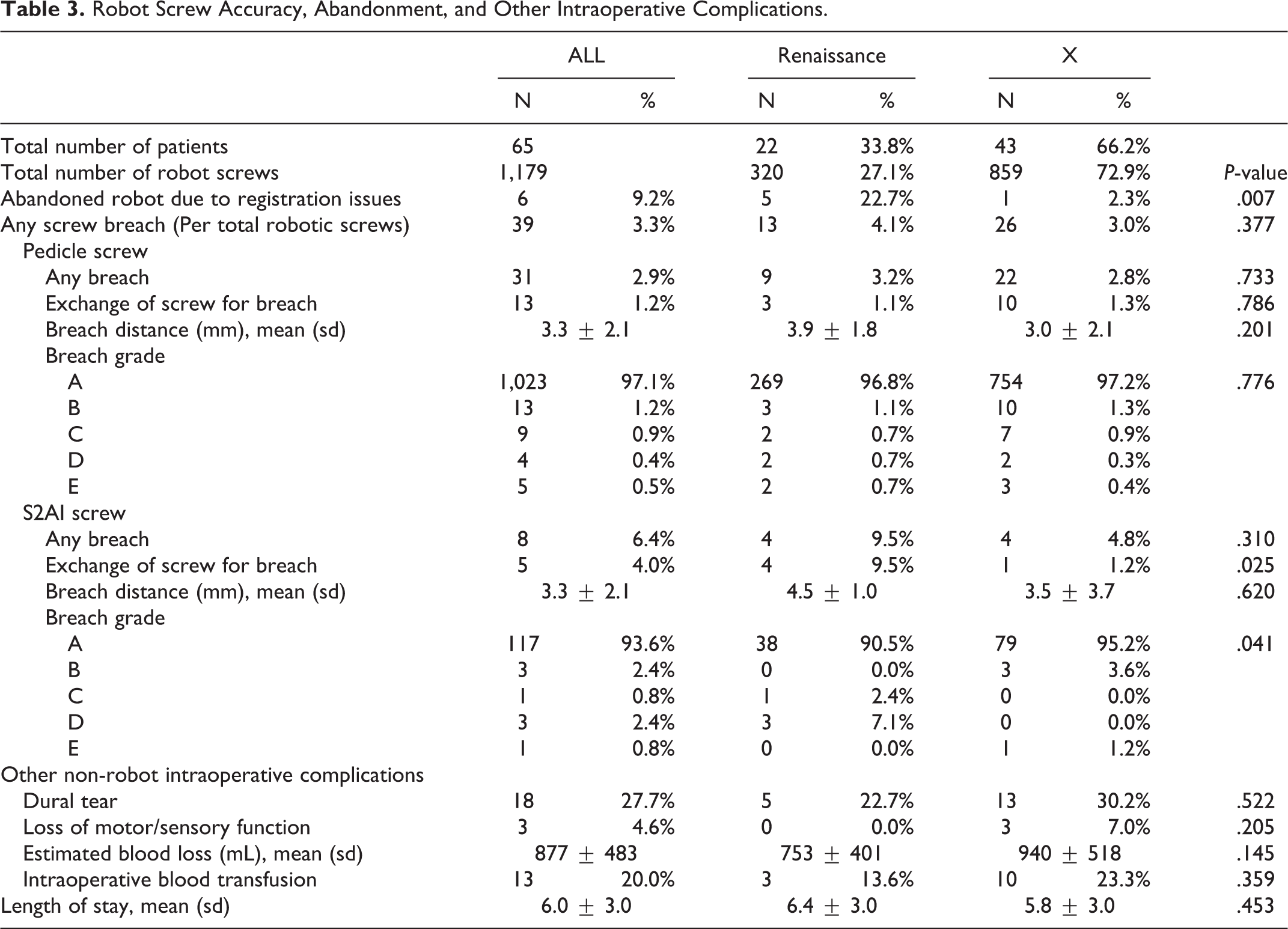
No statistically significant difference was observed for the operative efficiency between robot cohorts (Table 2). The overall mean robot time per screw was 4.2 (2.0) minutes (Renaissance: 4.6 (2.6) vs. X: 3.9 (1.6), P-value = .246). The robot abandonment rate was significantly lower for the Mazor X than the Renaissance (Overall: 9.2% (N = 6); Renaissance: 22.7% (N = 5) vs. X: 2.3% (N = 1), P-value = .007) (Table 3). The rate of screw breach requiring an intraoperative screw exchange was 1.2% (N = 13). No statistically significant difference was observed between robot groups for pedicle screws (Renaissance: 1.1% (N = 3) vs. X: 1.3% (N = 10), P-value = .786). The mean breach distance for pedicle screws was 3.3 (2.1) mm. The breach grade distribution for pedicle screws was not statistically different between groups (P-value = .776). For S2AI screws, the rate of exchange for screw breach was 4.0% (N = 5); however, the screws placed by the Mazor X (1.2%, N = 1) was significantly more accurate than those placed by the Renaissance (9.5%, N = 4, P-value = .025). The breach grade distribution between cohorts was significantly different between groups with a larger proportion of Grade A and B observed for Mazor X than the Renaissance (P-value = .041). Other non-robot related complications and outcomes included dural tear (27.7%, N = 18), intraoperative motor/sensory function loss (4.6%, N = 3), estimated blood loss (877 (483) mL), intraoperative blood transfusion (20%, N = 13), and length of stay (6.0 (3.0). No statistically significant differences for these outcomes and complications were observed between robot groups (P-value > .05).
Operative Efficiency by Robot System.
Robot Screw Accuracy, Abandonment, and Other Intraoperative Complications.
Overall Radiation (mGy and seconds) Exposure by Robot Systems.
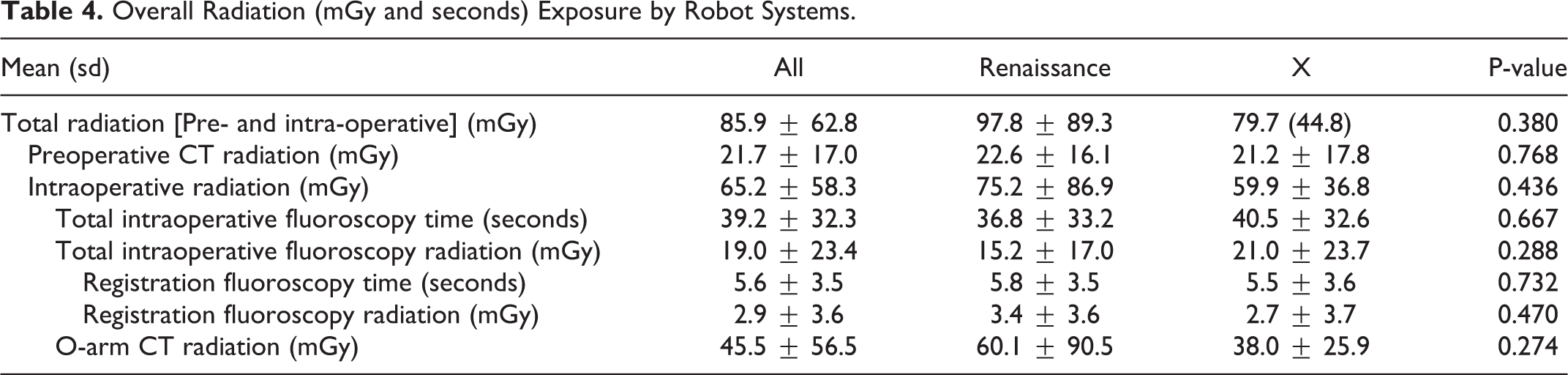
Radiation exposure (dose and time), including preoperative and intraoperative levels were not different between robot systems (Table 4). The total radiation dose (preoperative and intraoperative) was 85.9 (62.8) mGy (Renaissance: 97.8(89.3) vs. X: 79.9(44.8), P-value = .380). The total intraoperative fluoroscopy time was 39.2 (32.3) seconds (Renaissance: 36.8(33.2) vs. X: 40.5 (32.6), P-value = .667). The O-arm CT radiation dose was 45.5 (56.5) mGy (Renaissance: 60.1 (90.5) vs. X: 38.0 (25.9), P-value = .274).
Discussion
Robot-assisted technology has been well received in spine surgery and the indications for its use continue to expand. 7 In patients with severe spinal deformities, distorted pedicle anatomy, and revision procedures, robot assistance can be advantageous. 13 The increased use of robot systems in spine surgery is expected to continue with some projecting the global market for robotic technologies to increase from $26 million to $2.77 billion by 2022. 8 The expansion of robot-assisted spine surgery is likely a result of the numerous potenital advantages robots offer over conventional methods.
Accuracy rates of pedicle screw insertion with robot-assitance have been studied extensively.7,18,19 Li et al performed a meta-analysis on 9 randomized controlled trials assessing the accuracy of pedical screw placement and clinical outcomes of the robotic-assisted technique versus conventional freehand technique. 20 The authors found that the accuracy of pedicle screw placement was higher and the rate of proximal facet violation was lower using robotic assistance. Hu et al, reviewed the experience 1 clinic had with using the Renaissance robot system. Of 960 screws placed with robotic-assisance, 949 (98.9%) were placed accurately with only 11 screws malpositioned (1.1%). 21 More recently, Khan et al, reported on the safety, feasibility, and learning curve using the Mazor X robot. In their study, they reported an accuracy rate of 98.7% with 74 of 75 pedicle screws rated Ravi grade I. A single screw was grade II. 22 Robot systems increase the degrees of motion in comparison to the human arm.23,24 This allows for more precise movement in the axial, coronal, and sagittal planes which in theory can enhance surgical accuracy and precision. 14
Despite numerous reports on pedicle screw accuracy using robot systems, the use of robots for S2 Alar-Iliac (S2AI) screw insertion has not been studied as extensively. 25 Still, however, there are some reports on S2AI screw insertion using robot systems. Shillingford et al performed a propensity-matched analysis comparing the accuracy of free hand versus robotic-assisted techniques for S2AI screw placement. 26 In their study, the Renaissance robot was used. The authors reported an accuracy rate of 97.8% which was not significantly different from 94.9% using fluoroscopy-guided freehand technique. Additionally, 95.7% of S2AI screws placed robotically were grade A which was not significantly different from 91.6% in the freehand group. Hu and Lieberman reported on the feasibility and accuracy of robot-guided S2AI screw placement. All 35 screws placed via the Renaissance robot had accurate trajectories. None were intrapelvic, risked neurovascular structures, or violated the cortex of the ilium. 27 Finally, Bederman et al, also assessed the feasibility and accuracy of robot-assisted S2AI screw insertion. Using either the SpineAssist or Renaissance robots, 31 screws were placed accurately with no proximal breaches of the anterior sacrum. Twenty screws protruded the ilium distally by less than 2 mm, 1 screw by 2-4 mm, and 10 screws by 4 mm or more. 25
To date, there have only been a few studies assessing the rate of robot abandonment in spine surgery. In their study of robot-assisted 2,067 pedicle screws with the Renaissance robot, Keric et al reported that 6 out of 309 cases (1.9%) were converted to fluoroscopic freehand technique due to failed registration. The causes of these failures were poor radiograph quality due to obesity and severe osteopenia. 16 Hu and Lieberman assessed outcomes of robotic-assisted pedicle screw placement with the Renaissance robot as a function of surgeon experience. 28 The authors found that the rates of robot abandonment with conversion to freehand placement decreased with time. Conversion rates were 17% in Group 1 (patients 1-30), 7% in Group 2 (patients 31-60), 8% in Group 3 (patients 61-90), 4% in Group 4 (patients 91-120), and 7% in Group5 (patients 121-150). Hu et al, reviewed 1 clinic’s experiences using the Renaissance robot. They found that robotic-assistance was aborted in 110 screws out of 949 total screws (10%). The reason for abandonment in their series was generally due to registration failure and issues with screw trajectory. Finally, Mao et al, compared O-arm navigation versus Mazor X with posterior spinal instrumentation. 29 Although they did not report the exact rate of robot abandonment, they state that a small subset of robotic cases required the use of additional imaging due to registration failure secondary to obesity.
Our study reports that robot-assisted instrumentation remain highly accurate and reliable. Furthermore, the more recent iteration of Mazor robot systems appears to demonstrate specific advantages for S2AI screws and lower rates of robot abandonment due to registration failure. Interestingly, the pedicle screw accuracy was similar between robots (Grade A/B: Renaissance: 97.9%, N = 272 vs. X: 98.5%, N = 764, P = .776). In addition, the pedicle screw exchange rate for breach was not different between robot groups (Renaissance: 1.1%, N = 3 vs. X: 1.3%, N = 10, P = .786); however, the S2AI screw accuracy was significantly higher for X vs. Renaissance (Grade A/B: Renaissance: 98.8%, N = 81 vs. X: 90.5%, N = 38, P = .041) and the breach rate was significantly lower for the X (Renaissance: 9.5%, N = 4 vs. X: 1.2%, N = 1, P = .025). Additionally, the X robot was significantly more reliable with a robot abandonment rate of only 2.3% (vs. Renaissance: 22.7%, P = .007). The added variability of several moutning platforms and accessory instruments required by the Renaissance likely contributes to the risk for robot registration error since any subtle shifts in movement between the patient and robot system can offset the robot registration. This becomes especially important for S1AI screws, which can be even more difficult to place than pedicle screws given the patient’s sloped anatomy, limited direct visualization of anatomy, and soft tissue tensioning which may offset the robot system. The introduction of a serially designed robot arm by the Mazor X system obviated the need for additional platforms or accessory instruments. The Mazor X three-dimensional camera designed to reduce collision error between the patient and surgical environment, as well as the Mazor X Eye camera which was used to verify appropriate arm position and trajectory at each instrumented level likely contributed to the decreased robot abandonment rate and improved S2AI srcrew accuracy.
Other outcomes and complications, such as operative efficacy, radiation exposure, and length of stay were not different between robot systems. Compared with the coventional fluoroscropy-guided free hand technique, studies have demonstrated that the use of robotic systems in spine surgery decreases the occupational exposures to ionizing radiation. 30 This is of particular importance as this can mitigate the 10- to 12-fold increase in radiation exposure that has been associated with increased levels of malignancy in spine surgeons and surgical staff later in life. 31 As robotic technology continues to progress in spine surgery, it is important to examine if these advancements translate into improved outcomes for the patient.
Our study has several limitations. First, this was a single-surgeon series with a relatively small sample size. Our power analysis accounted for the robot abandonment and screw accuracy rates reported in prior literature to reach a sufficient statistical power to detect a treatment effect. Given the single-surgeon design of this study, these results may not be generalizable to other spine surgical practices or other robot systems. For instance, robot abandonment rates may vary depending on surgeon familiarity with robot systems as well as surgeon technique and patient anatomy. However, our results closely agree with the findings of most retrospective studies that have been published on this topic. Multicenter studies can provide greater numbers to better discern differences in relatively rare complications. On the otherhand, a single center series allows for a closer examination of radiation exposure (e.g. dose and time in both the preoperative and intraoperative period), and screw accuracy as measured by third party systems (e.g. Vitrecore), which may be more difficult to do with a large, multicenter database. Second, cases were not randomly assigned by robot type. Propensity score matching accounted for several patient and operative factors, but it is possible that a learning curve exist with robot use and this may influence outcomes since Mazor X was the only robot used after June 2017. Interestingly, pedicle screw accuracy and robot time per screw were not significantly different between robot systems. Instead, robot abandonment and S2AI screw accuracy were significantly improved with the Mazor X. The recent advancements in Mazor X technology, namely the serial robot arm, three-dimensional camera, and Mazor X Eye camera likely contributed to improved robot reliability and S2AI screw accuracy as well. Third, we did not perform an analysis on the post-discharge outcomes. The focus of this paper was to examine specific differences in the intraoperative outcomes (e.g. screw accuracy, radiation, robot time, and robot-related complications) which we believe are more relevant when comparing robot system; however, future studies can examine the short- and long-term outcomes between robot systems. Finally, Mazor’s latest robot system, Mazor X Stealth Edition, was not included in this comparative analysis. This 4th generation robot integrates Medtronic’s Stealth navigation technology into the Mazor X platform. Future work is currently underway to determine the distinct advantages of this robot system compared to others.
Conclusion
This is the first comparative analysis of robot complications, radiation exposure, operative efficacy and outcomes between the Mazor X and Renaissance systems. There are substantial improvements in the X robot, particularly in the perioperative planning processes, which likely contribute to the X’s superiority in screw accuracy and robot reliability. Compared to the Renaissance, the Mazor X demonstrated a significantly higher rate of S2AI screw accuracy and a lower rate of robot abandonment due to registration issues. Continued research on robot-assisted systems are warranted as robotic technology continues to progress. Future studies may include larger prospective studies, and comparative analyses on cost and patient-reported outcomes.
Footnotes
Authors’ Note
This study was IRB approved (IRB-AAAT1470). No patient-informed consent was needed since a waiver of authorization was granted. The Robotic device is FDA-approved
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.