
Abstract
Study Design:
Cadaveric biomechanics study.
Objective:
Subchondral bone mineral density (sBMD) reflects the long-term mineralization and distribution of stress on joints. The use of 3-dimensional (3-D) methods to evaluate sBMD, including computed tomography osteoabsorptiometry (CT-OAM), enables the assessment of density distribution with emphasis on subchondral bone. This study sought to measure the sBMD of cervical endplates using CT-OAM and correlate it to mechanical implant subsidence in a cadaveric model.
Methods:
Fourteen fresh human cadaveric cervical spines were subjected to dynamic testing after single level discectomy and instrumentation using a PEEK interbody spacer. Specimens were imaged with CT 3 times: 1st) whole intact cervical spine, 2nd) after implantation, and 3 rd) after testing. These images were used to assess sBMD distributions using CT-OAM directly underneath the spacer. Subsidence was defined as the displacement of the device into the endplates.
Results:
The observed “failure mode” was consistently recorded as subsidence, with a mean of 0.45 ± 0.36 mm and 0.40 ± 0.18 mm for the C4-5 and C6-7 levels, respectively. There were no differences by level. The experimental cyclic test showed that denser endplates experienced less deformation under the same load.
Conclusions:
This study achieved its stated aim of validating the use of CT-OAM as a method to analyze the sBMD of the cervical endplates. Studies such as this are providing new information on available technology such as CT-OAM, providing new tools for clinicians treating spinal conditions in need of augmentation and stabilization via interbody devices.
Keywords
Introduction
Cervical degeneration secondary to intervertebral disc degeneration is among the leading causes of disabling radiculopathy and myelopathy, with an estimated prevalence between 54% and 80% worldwide.1,2 In a healthy spine, the intervertebral disc (IVD) and cartilaginous endplates play a crucial role in the overall nutrition and biomechanical integrity of the associated spinal motion segment, with past studies suggesting that age-related microstructural and sclerotic changes at the cartilaginous endplate contribute to chondrocyte apoptosis and altered metabolic homeostasis.3,4 Furthermore, loss of the cartilaginous layer results in impaired axial load absorption, thereby subjecting the bony tissue to an increased burden. These interactions are instrumental to degeneration of the IVD and the progression of spondylotic changes.5-8 In addition, an aging population with rising incidence of osteomalacia is subject to weakened corticocancellous bone structure.
The global ubiquity of degenerative disease in the cervical spine has created an increased demand for surgical intervention. Anterior cervical discectomy and fusion (ACDF) is a standard treatment for spondylotic radiculopathy or myelopathy when conservative treatment options fail. However, the increased utilization of ACDF has been paralleled by a rise of osteoporosis and osteopenia attributed to age-related and disease-specific processes contributing to poor bone health. Poor bone quality and low subchondral bone mineral density (sBMD) are significant risk factors for postoperative complications and ACDF failure, with subsidence of the prosthetic interbody cage into the adjacent vertebral endplates contributing to significant morbidity.9-12 Cage subsidence can lead to the development of pseudarthrosis, loss of lordotic correction, graft extrusion, pathologic fracture of the adjacent vertebral bodies, and foraminal collapse, all of which may result in debilitating pain and neurologic compromise with the need for revision surgery.
While Dual-Energy X-Ray Absorptiometry (DXA) has long been considered the clinical gold standard for measuring BMD and evaluating for poor bone integrity, it is limited to 2-dimensional (2-D) assessment. Computed tomography osteoabsorbptiometry (CT-OAM) can describe the subchondral BMD of any joint through 3-dimensional (3-D) volumetric measurements, with the addition of several key advantages.13-17 While most 3-D techniques measure the absolute bone density of a certain area, including cortical and cancelous bone, CT-OAM can record differences in the density distributions of areas of interest, specifically that of subchondral bone.14,17 By utilizing this technology to evaluate location-specific subchondral bone density distributions, we can further elucidate the loading patterns at the vertebral endplates. There is currently a patent need in literature to bridge this gap in the understanding of spinal mechanics.
This study used the cervical vertebrae of cadaveric specimens with the aim of: i) comparing CT-OAM to the current gold standard DXA for the qualitative evaluation of subchondral bone mineral density; ii) biomechanically inducing subsidence of the interbody cage after ACDF between contiguous vertebral levels; iii) evaluating whether lower subchondral bone mineral density as measured by CT-OAM could accurately predict ACDF failure in order to validate CT-OAM as a clinical tool for the assessment of bone integrity.
Materials and Methods
Specimen Selection
This study was exempt from obtaining informed consent and did not require Institutional Review Board approval. A total of 14 (n = 14, equal number of females and males, age range 27-89 y.o.) deidentified fresh human cadaveric cervical spines were obtained from an approved tissue bank (Science Care, Phoenix, AZ). Inclusion criteria were specimens between the age of 40 and 90 years of age with varying bone quality. The exclusion criteria were a history of prior surgery to the cervical spine, trauma, or malignancy. These criteria were selected in order to accurately depict a sample of the patient population normally undergoing anterior cervical surgery.
Specimen Testing
Specimens were assigned to 2 groups: a) those selected for static loading testing and b) those selected for dynamic (cyclic) testing. Static and dynamic groups were further subdivided by spinal level. The Static group was comprised of 6 C4-C5 and 8 C6-C7 motion segments; the Dynamic group was composed of 8 C4-C5 and 6 C6-C7 motion segments. All motion segments were potted in polymethylmethacrylate (PMMA). Polyetheretherketone (PEEK) cervical interbody spacers were inserted at each motion segment with cage heights between 6 and 8 mm depending on individual specimen size. The cages were not supported anteriorly by a plate. The footprint geometry of the cervical cage was obtained via micro-computed tomography (uCT 50, Scanco, Brutisellen, Switzerland) at a resolution of 20 micron, to be used later as input in the CT-osteoabsorbptiometry analyses.
The static mechanical tests consisted of the application of a compressive load in a cranio-caudal direction using a servo hydraulic testing frame (Instron 8874; Instron Corp., Norwood, MA) running in displacement control with a crosshead speed of 1.0 mm/min until failure. Structural stiffness in N/mm was recorded for all samples. For the fatigue test, a quasi-static test consisting of 5 compressive ramp loading cycles was applied with a load range from 50 to 250 N at a frequency of 0.5 Hz as a pre-conditioning approach. Following this, a compressive sinusoidal load with the same load range (50 -250 N) was applied at 2 Hz for 10,000 cycles. This loading range was selected to replicate normal in vivo working limits in cervical spines based on past work.18,19
Evaluation of Failure
The rationale behind the cyclic tests was to provide the opportunity to induce failure in the instrumented functional spine unit. This could be manifested as loosening or as the continuously deeper indentation of the interbody device into the endplate surface, which was labeled subsidence. Since the surgical placement was performed according to the intact disc height, the spinal alignment was meant to preserve or at least come close to the native state. The peak loads at cycles no.1 and no. 10,000 were chosen as the reference points (in this case both at 250 N) and the difference between these points in the displacement axis was the measured deformation of the endplate, which coincides with the above-mentioned definition of subsidence. Displacement data was collected at the maximum load limit every 10 cycles. Structural stiffness (the slope of the load vs. diagram in N/mm) and the displacement (mm) history of the specimen were recorded (Figure 1).
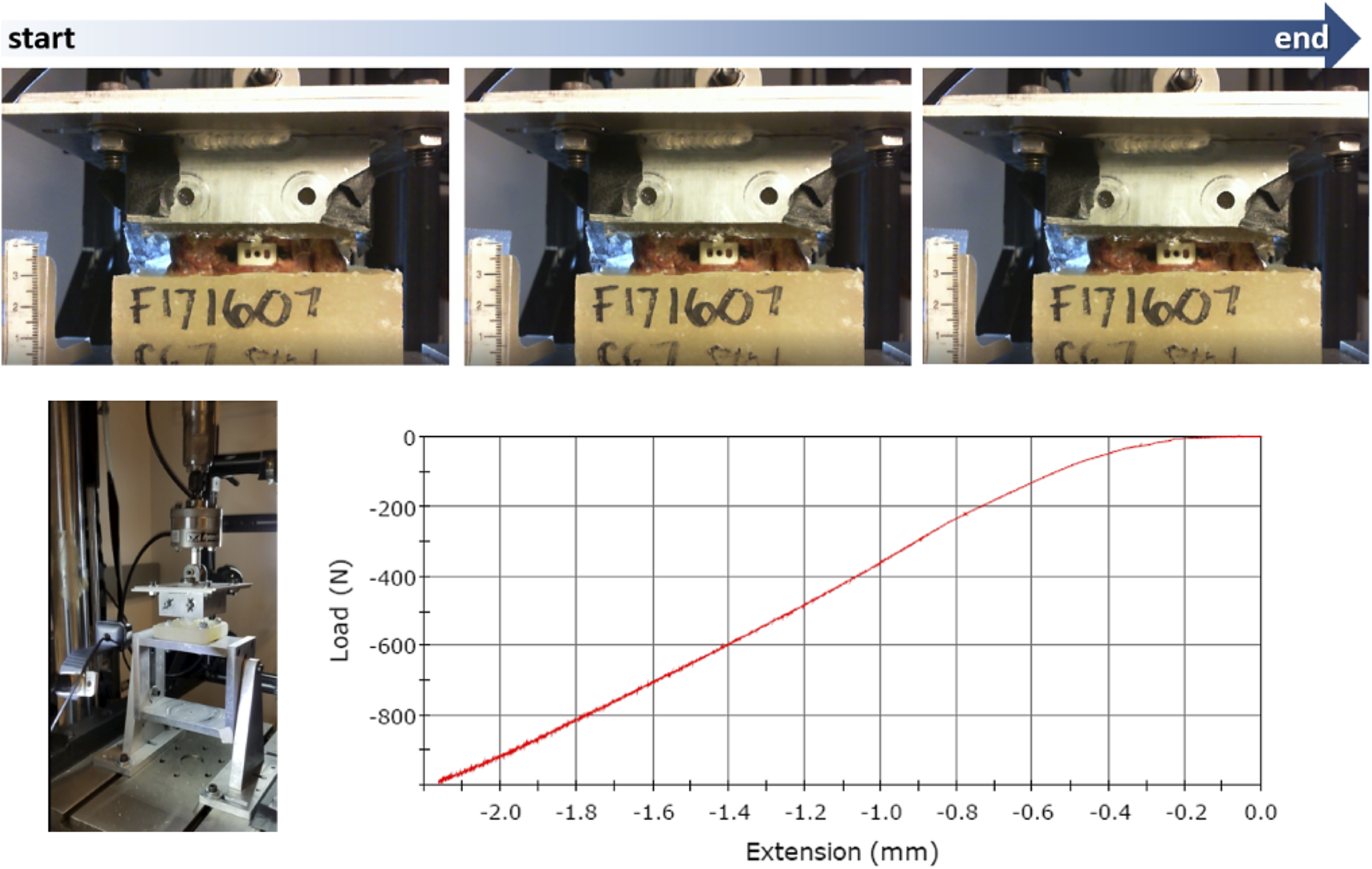
Static compressive test sequence—1 mm/min loading up to 1,000 N.
Bone Mineral Density Evaluation
All experimental specimens were imaged with clinical CT at 0.625 mm thickness slices (no spacing) 3 times: the first set of images were taken when the whole intact cervical spine was received from the tissue bank, the second just before the test (potted and instrumented), and the third after the completion of mechanical testing (still instrumented, Figure 2).
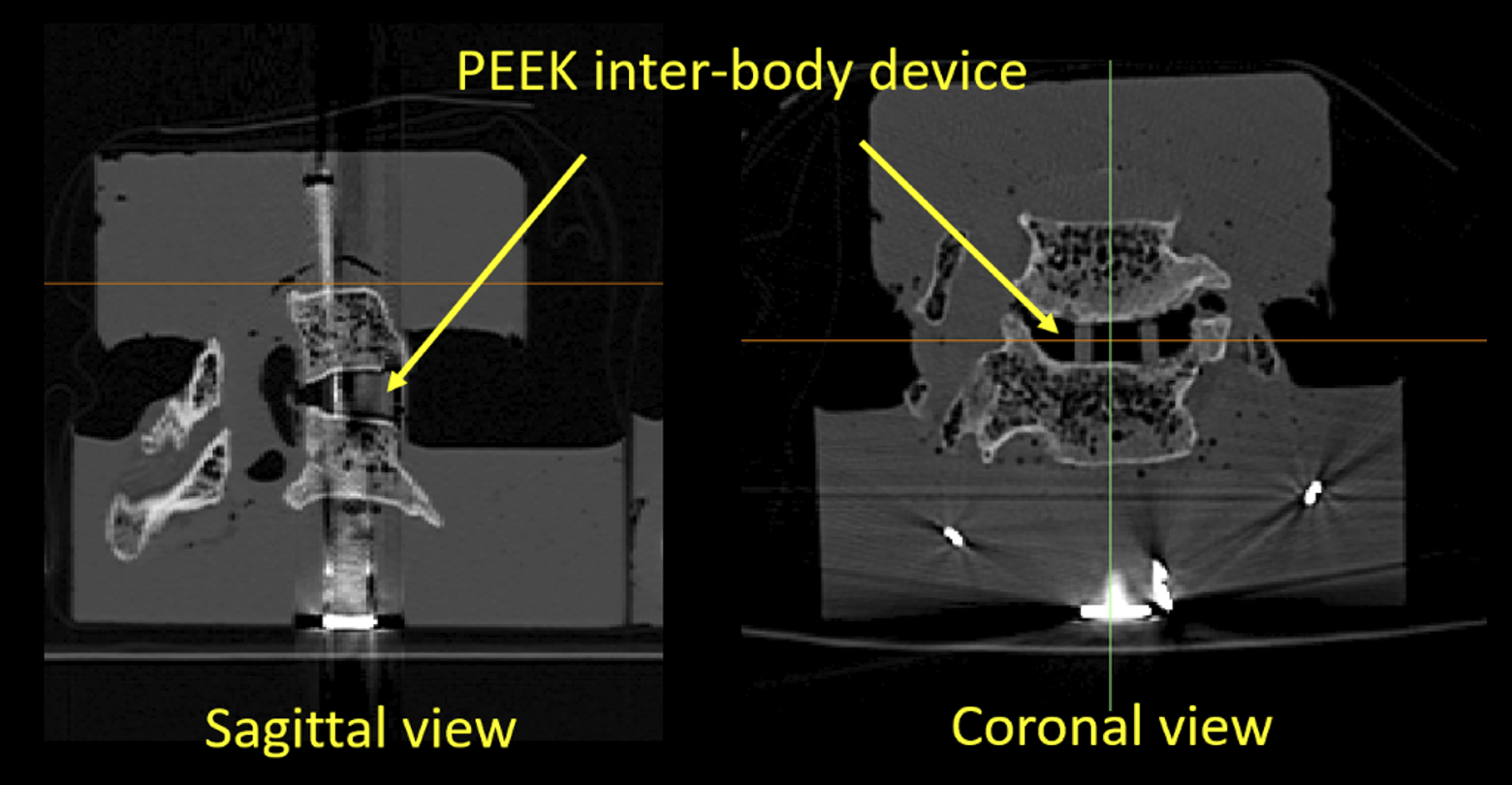
Post-test CT demonstrating the interbody device in place. The bright metal signature corresponds to hardware used to anchor the caudal vertebra when potting in acrylic cement.
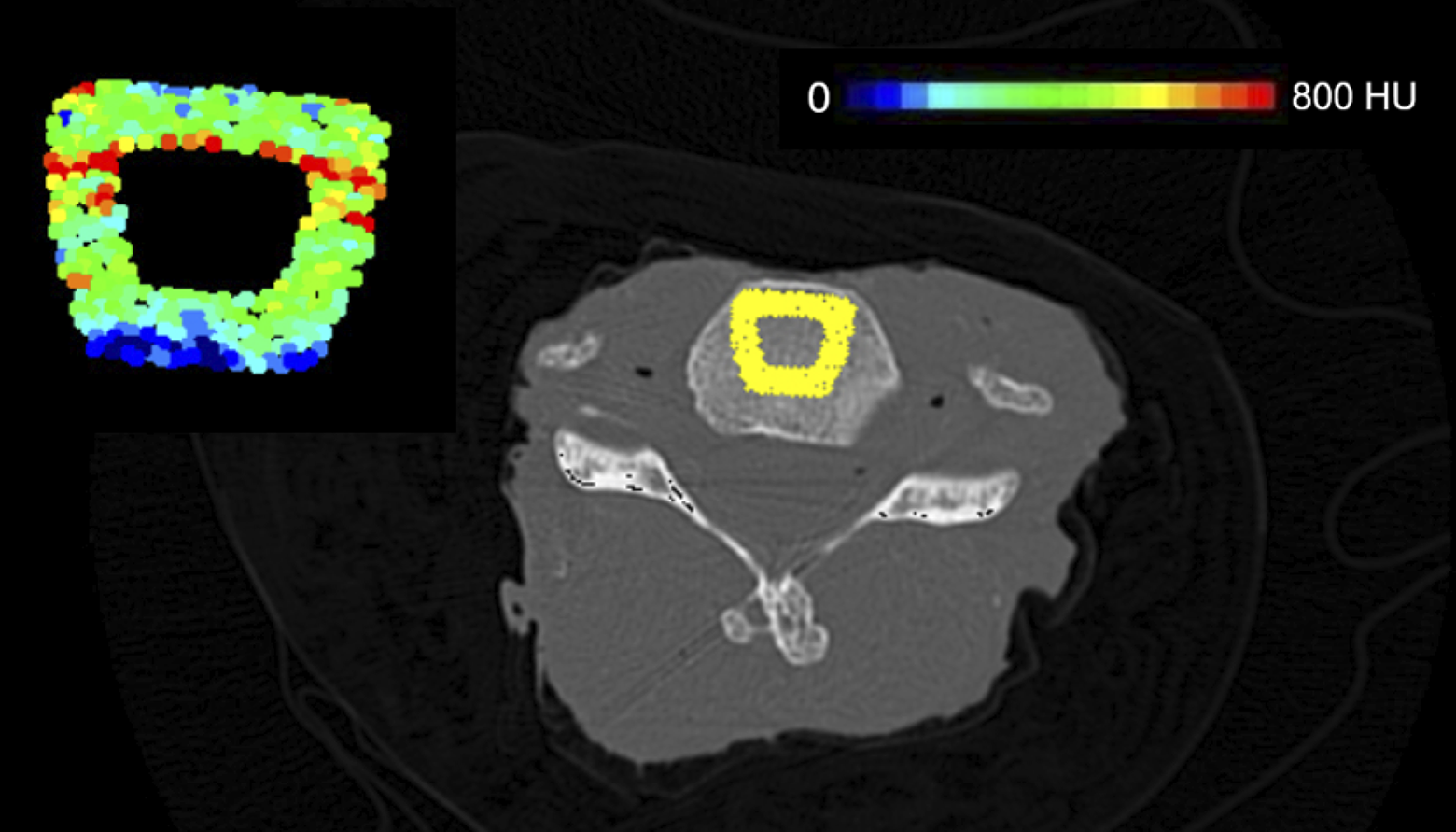
These images were used to assess the bone mineral density distributions using the CT-OAM method (Figure 3). 15 The CT data was also employed to create 3-dimensional models of the motion segments at the same intact, pre-test, and post-test conditions, which allowed for the evaluation of changes brought upon by the testing.
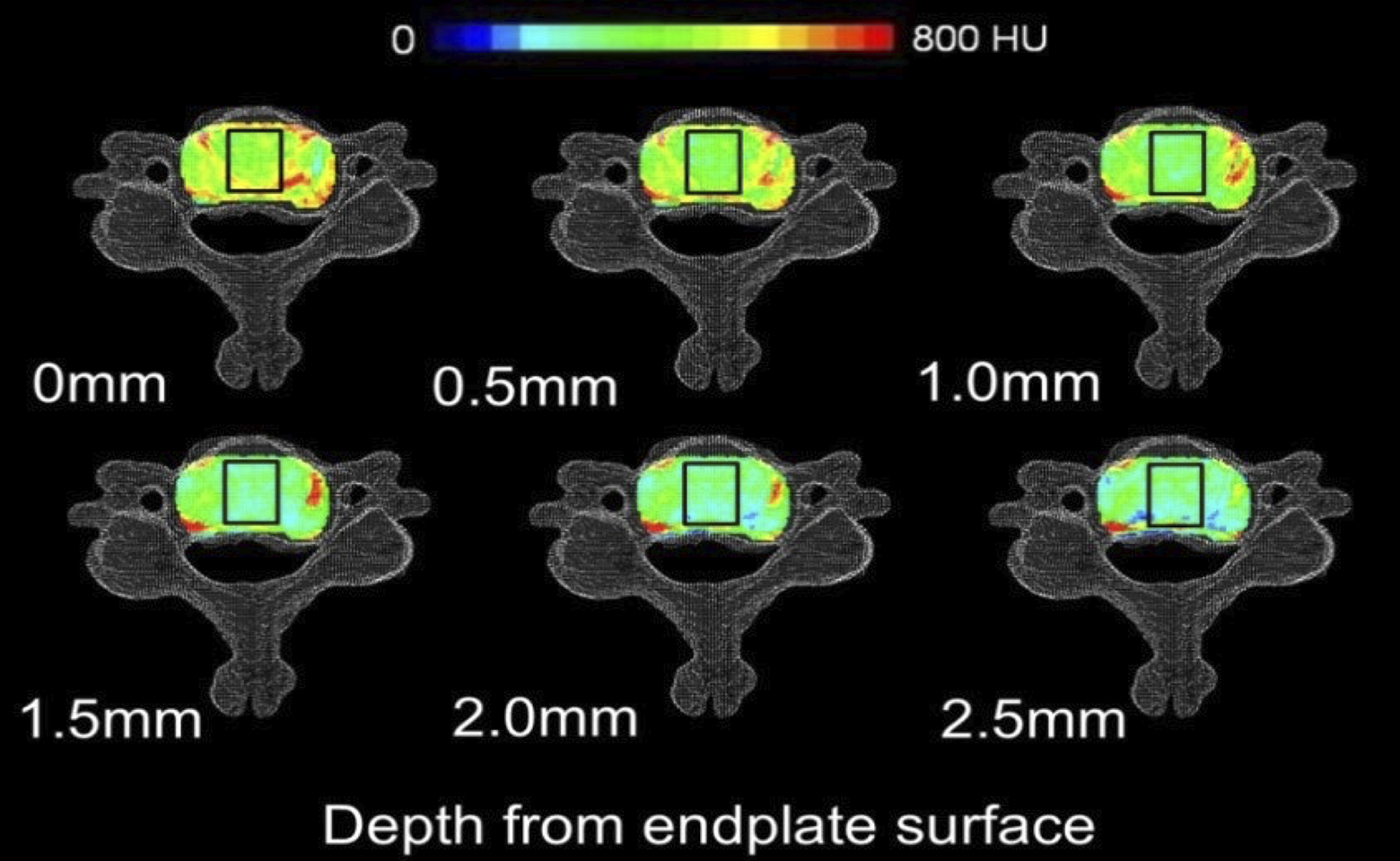
Distribution of HU at different depths within the cervical superior endplate. Black boxes indicate footprint of an implant projected to each layer.
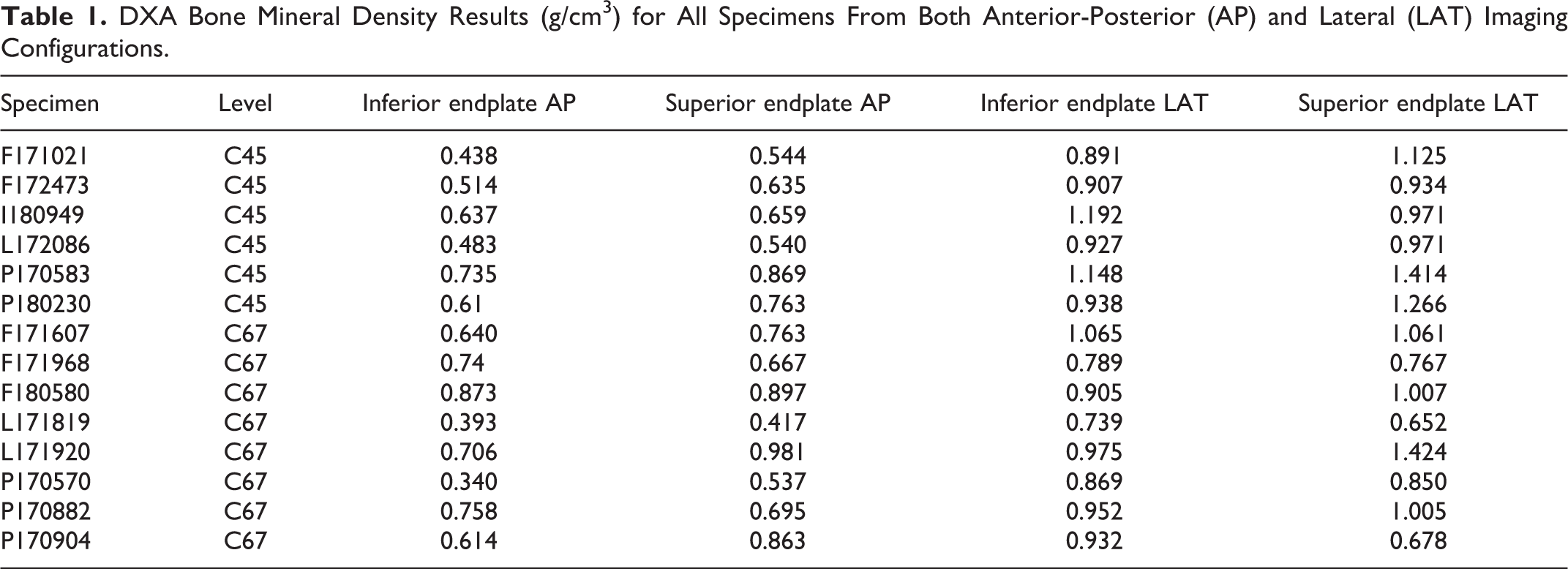
In order to establish a clinical benchmark for comparison purposes, the intact spines also underwent DXA analysis of bone mineral density (GE Lunar, Milwaukee, WI), even though the cervical spine is not a common site for DXA measurements clinically. Spines were analyzed both in Anterior-Posterior (AP) as well as lateral views using a forearm protocol (Table 1). This was done in order to assess the possible influence of posterior elements present in the image. After comparing both protocols, it was decided to use the lateral view to analyze bone mineral density of the spines in 3 regions of interest, given the lack of interference from the posterior elements. We assessed the cranial and caudal endplates on each vertebra, as well as a central band corresponding to the vertebral body. Bone density data was presented in g/cc.
DXA Bone Mineral Density Results (g/cm3) for All Specimens From Both Anterior-Posterior (AP) and Lateral (LAT) Imaging Configurations.
Results
Bone Density
The DXA tests produced statistically different values depending on the AP or the lateral protocol. On average, AP values were significantly lower than the results obtained from the lateral views, as demonstrated by a paired t-test. For the cranial endplates, the lateral views appeared to have higher bone density (mean AP 0.606 vs. 0.945 g/cc; P = 0.00000225), while caudal values also demonstrated a similar relationship (0.702 vs. 1.009 g/cc; P = 0.0000077). When comparing these findings to the CT OAM results for the dynamic test specimens, there was a positive correlation between both DXA measured values; however, comparing each of these to the CT OAM results yielded negative correlations. Table 2 shows the correlation, P-value and confidence intervals for these comparisons. Table 3 demonstrates the Hounsfield unit (HU) sBMD values obtained via CT-OAM at the region of interest along the footprint of the interbody cage.
Bone Mineral Density (BMD) Correlations.

* Denotes significance.
Computed Tomography Osteoabsorbptiometry (CT-OAM) Results in Hounsfield Units (HU) in a Region of Interest Underneath the Footprint of the Interbody Device.
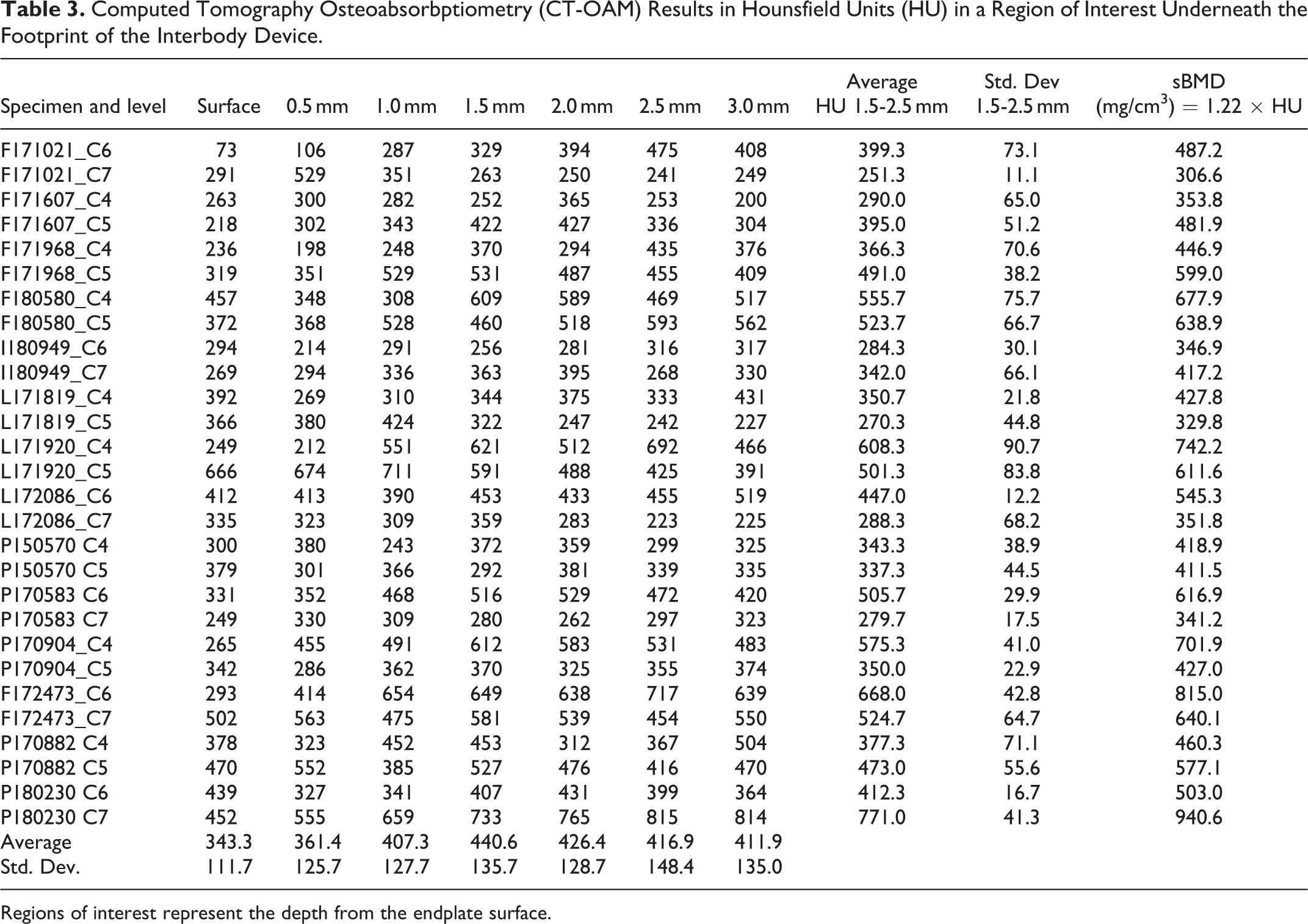
Regions of interest represent the depth from the endplate surface.
Static Tests
The static tests went up to 1 kN of loading, which was the upper limit of the load cell in the Instron testing frame system. The footprint of the cervical cage on the endplate is demonstrated by Figure 4. None of the samples experienced fracture up to this load. Figure 5 shows the results from the stiffness tests comparing the stiffness (Kstat) versus the DXA-sourced BMD values.
Representative illustration of the CT-OAM results in a region of interest directly underneath the footprint of the interbody device.
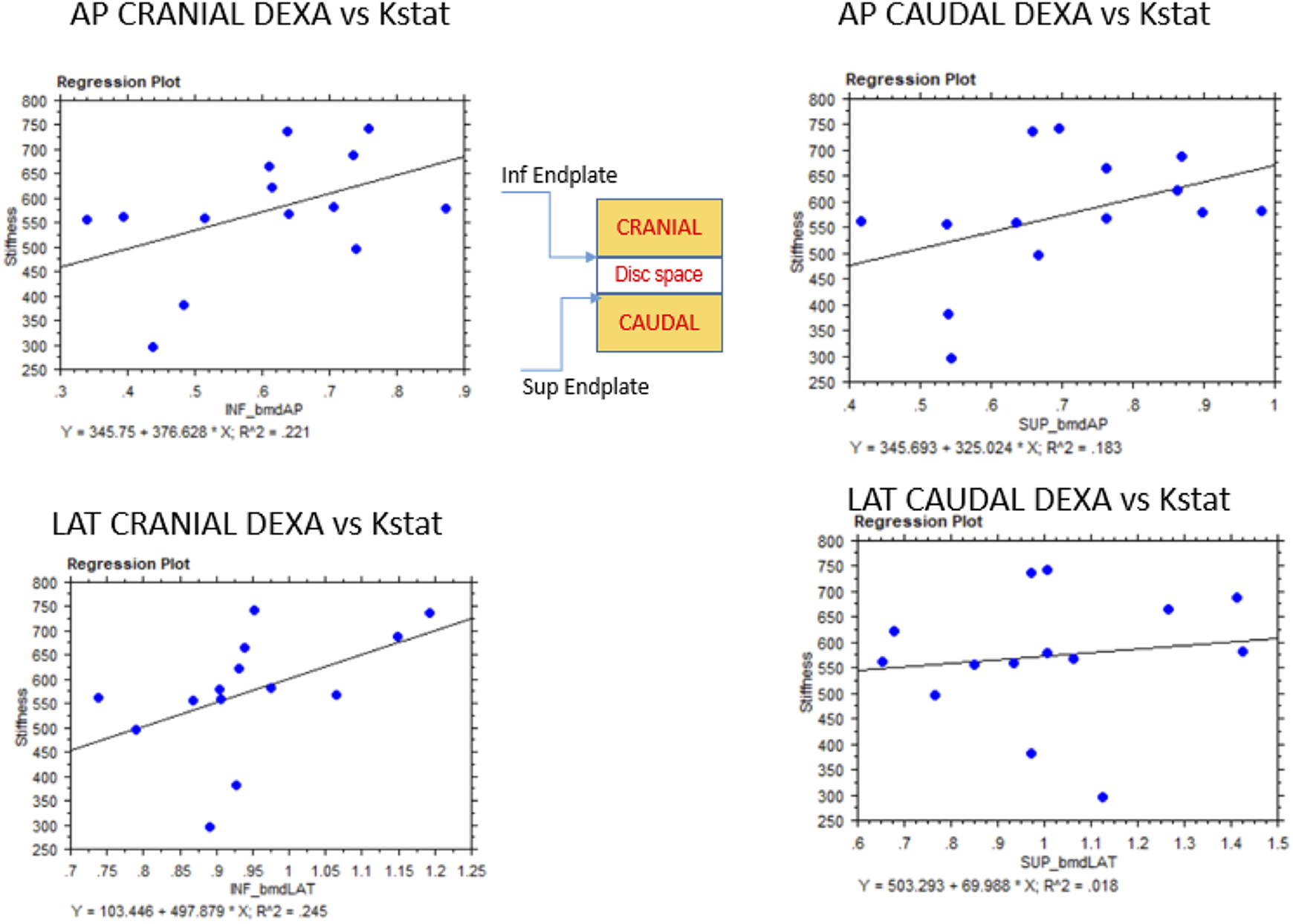
Experimental results for stiffness vs. DXA measured BMD. BMD is shown in the horizontal axis (g/cc) and the Stiffness is shown in the vertical axis in N/mm units.
Cyclic Tests
After the cyclic test was completed, the data was analyzed by looking at the displacement vs. load charts. This chart (as demonstrated in Figure 6) was comprised of 4 regions, each representing one of the 4 blocks of the test: 1) initial load to 50 N; 2) 5 cycles of compressive load at 0.5 Hz from 50 to 250 N; 3) 10000 cycles of compressive load at 2 Hz from 50 to 250 N; 4) the unloading portion back to 0 N. For the purposes of this analysis, the third block of data was employed to evaluate deformation at the cage-endplate interface.
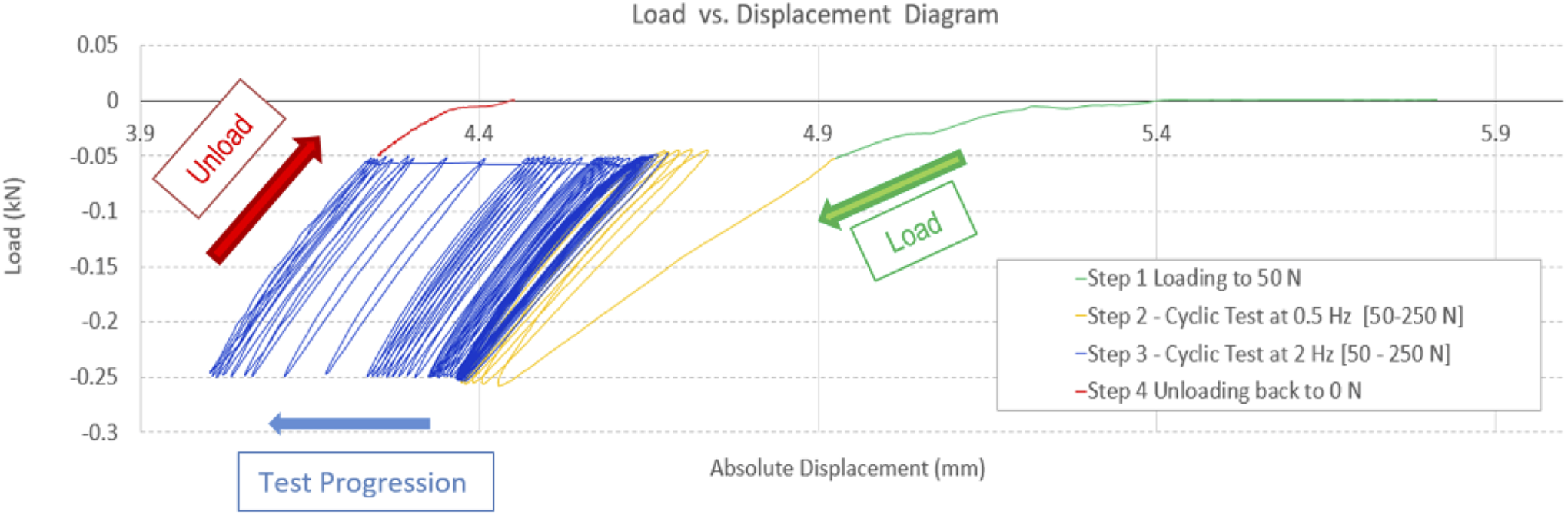
Representative regions of the load vs. displacement data from the cyclic tests.
Subsidence
The consistently observed “failure mode” was subsidence, which was obtained from the load vs. displacement diagram as shown in Figure 7. In an ideal elastic material, the load vs displacement curve would be a line with the same slope from cycle 1 to the n-th cycle of the test. However, in the case of viscoelastic materials such as the ones being tested in this circumstance, 2 phenomena are observed: a) hysteresis, where the line becomes a loop and b) the peak point progresses in time from the first cycle until the loading ends. These 2 features are readily discerned in a representative curve as shown in Figure 7.
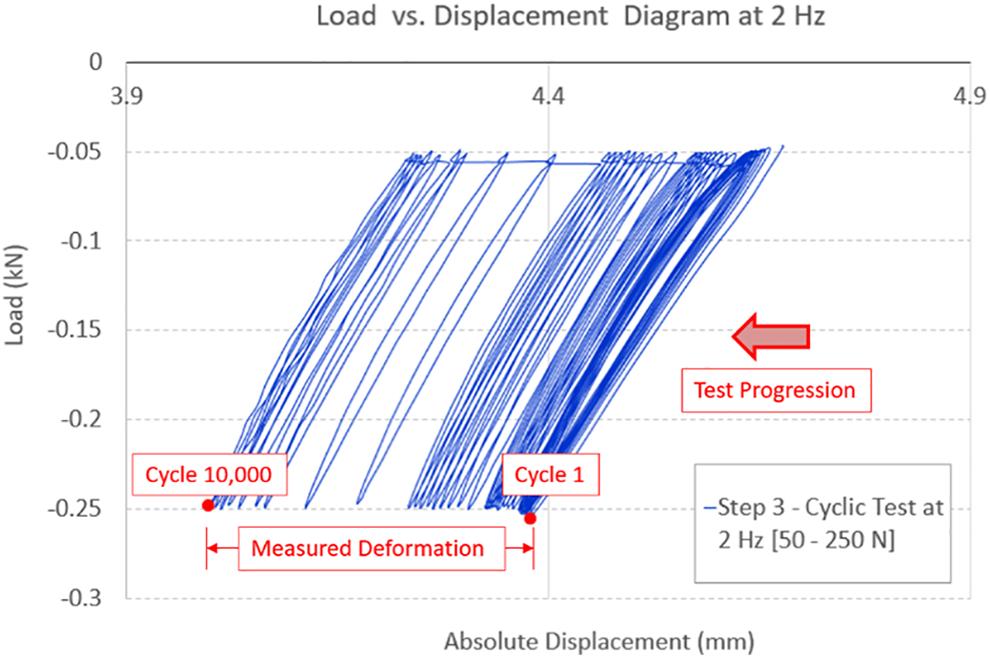
Graphical representation of the measured deformation reported as subsidence of the interbody device.
Table 4 shows the results of the deformation for each of the n = 14 specimens tested with cyclic loads. The mean ± SD (mm) results by level were 0.45 ± 0.36 and 0.40 ± 0.18, for C4-C5 and C-6-C7, respectively. There were no significant differences by level in this sample.
Experimental Subsidence Results by Level.
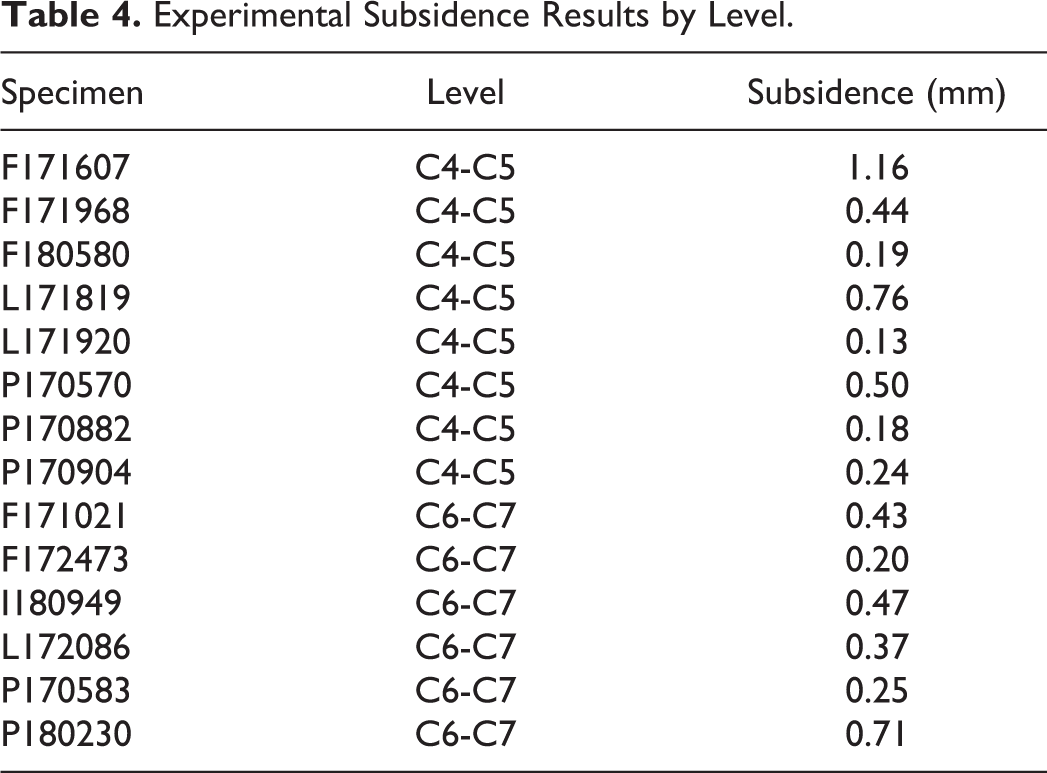
The experimental cyclic test produced the anticipated deformation results, in which a denser material experiences less deformation under the same load as one that is less dense. Figure 8 shows this relationship in a graphical manner with the deformation recorded at both 50 and 250 N loads, confirming the mechanical behavior with this load scenario. This is represented by the almost parallel slopes in both linear functions.
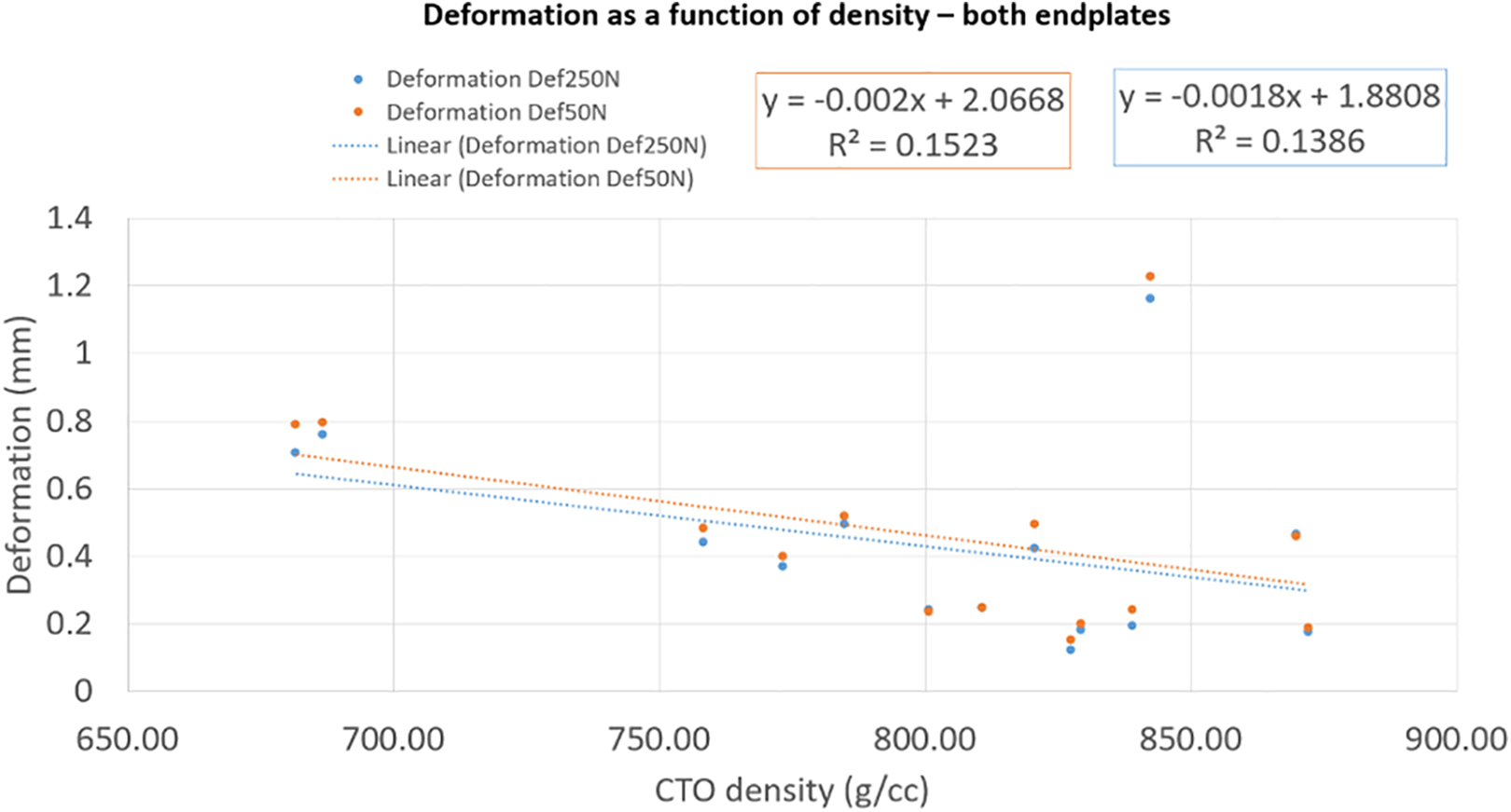
Deformation as a function of CTO-derived density measurements.
Discussion
This study sought to assess the clinical utility of 2 radiographic methods that are readily available to clinicians. CT-OAM was compared to the current clinical gold standard DXA by obtaining measurements of sBMD at the endplates of cadaveric cervical vertebral bodies. The cervical endplates were subsequently subjected to compression testing in order to evaluate how the results of CT-OAM readings translate to biomechanical strength. Although no direct correlations between results on DXA and CT-OAM were found, CT-OAM measurements of sBMD were able to accurately predict interbody cage subsidence.
In clinical practice, preoperative assessment of a patient’s bone integrity via the evaluation of BMD and consideration of comorbid diagnoses which may have deleterious effects on bone health are critical for achieving successful outcomes. Studies have repeatedly shown that patients with osteoporotic bone are at increased risk for interbody cage subsidence, migration, screw loosening, and iatrogenic fracture after spinal fusion procedures, all of which may interfere with arthrodesis and palliation of symptoms.20-22 Although DXA is the mainstay for the evaluation of BMD and establishing a diagnosis of osteoporosis, it is limited to 2-D assessment. By measuring BMD from a single planar view, DXA only affords the clinician the ability to obtain a broad understanding of bone quality but is incapable of providing data on density distributions in specific regions of interest. On the other hand, CT-OAM is a 3-D technology that can provide information on isolated density distributions in regions and depths of interest, which for the purpose of this study included the subchondral cortical bone of cervical vertebral endplates.14,17
An initial comparison was conducted between DXA protocols by performing measurements in AP and lateral configurations using a forearm protocol in a GE Lunar unit. However, the AP measurement protocol was biased as a result of the inclusion of the posterior elements of the spinal column, leading to inaccurate measurements. The lateral approach conferred the advantage of excluding these structures in the measured region of interest, leading to values that may be considered more appropriate. Although the additional bony structures of the posterior spinal column were absent from the lateral DXA reading, the mean BMD observed on lateral views was greater than that seen on AP views (Table 1). These findings are consistent with existing literature which has demonstrated that lateral view DXA of the spine more consistently detects osteopenia due to a more accurate estimation of trabecular bone mass, even when readings from AP DXA appear to be normal. 23
The results of DXA and CT-OAM did not show significant correlations as shown in Table 2. However, this does not mean that one does not validate the other as there were key differences in the region of interest (ROI) studied in addition to procedural capacity to assess subchondral bone. The DXA measurement is an aggregate report of the defined ROI when the analysis is carried out. In this case, the whole endplate was used with the caveat of very low image resolution on the screen where the analysis was defined. On the contrary, the CT-OAM method can be as fine as the resolution assigned to the CT scan itself. In this case, the slices were 0.625 mm in thickness without spacing, providing very high-resolution images of the subchondral layer of cortical bone. The CT-OAM analysis was carried out in 0.5 mm intervals down to a depth of 3.0 mm beneath the endplate surface. Our previous work has indicated that the ROI is most consistently located at a depth of 1.5 to 3.0 mm at the facet joints. 16 Building off of these findings, it was decided to focus CT-OAM measurements on the same band of depth within the endplate.
Despite these disparities in the analysis methods, the mechanical loading scenarios were suitable to produce larger deformations via interbody cage subsidence in less dense regions of bony tissue, as would be expected in linear elasticity. Similarly, the results showed that the regions with higher sBMD values on CT-OAM experiences less subsidence of the interbody cage. It should be noted that past studies have demonstrated cervical level-dependent differences in density distributions, with highest densities in the mid-cervical spine and lowest at the caudal vertebrae, which may be attributed to greater biomechanical load in the mid-cervical spine. 24 This may have specific significance clinically as a past study evaluating subsidence of stand-alone PEEK interbody devices following ACDF demonstrated a higher risk of device subsidence at the C5-6 and C6-7 segments. 25 However, the present investigation was to correlate subsidence with sBMD measurements obtained via CT-OAM rather than to quantify the magnitude of subsidence based on cervical level, although this is an important area for future study.
The findings of this study corroborate the utility of CT-OAM, a technology which is readily available to providers in the clinical setting, for the evaluation of the integrity of the bony endplate in the cervical spine. While this imaging modality does expose the patient to higher levels of ionizing radiation than DXA, preoperative CTs are commonly obtained routinely, particularly for patients for whom there may be concern for poor bone quality. Therefore, the CT-OAM data can be derived from standard of care preoperative imaging, thus sparing the patient from an additional dedicated DXA scan and the associated radiation.
This study is not without limitation. Although the biomechanical testing configuration utilized to apply stress on the motion segment was able to consistently reproduce failure as interbody cage subsidence, testing was limited to a compressive axial load. This is different from the loading forces applied on the motion segment in a living cervical spine, which can also include bending and torsion forces in all planes. This means that although this study concluded on significant findings under model conditions, it was not able to factor in deviations from the model conditions that could potentially be observed in vivo. Moreover, it is important to note that although DXA is the standard and clinically available technique utilized for evaluating bone mineral density, it is not commonly used in the cervical spine. Additionally, in order to maximize testing per specimen, the C4-5 and C6-7 levels were used, although the C5-6 motion segment is the most commonly operated level. This was because our potting method required transection through the disc space since cutting mid-vertebra would result in insufficient specimen security during cyclic testing. These limitations must be considered when translating this study’s results to the clinical setting. Future clinical studies directed toward evaluating the correlation between CT-OAM, patient-reported outcomes, and interbody cage subsidence in the in vivo setting may represent a valuable area for future comparative analysis. Regardless of these limitations in the experimental model, this study’s findings expanded on current knowledge and provided evidence in support of the utility of CT-OAM for the qualitative assessment of bone at the cervical endplates.
Conclusion
This study achieved its stated aim of validating the use of CT-OAM as a method to analyze the bone mineral density of subchondral bone at the cervical endplates. While subsidence is a multi-factorial event and is still poorly understood with regard to the endplate tissue structure-function relationships, studies such as this are providing new information on currently available technology such as CT-OAM and are providing new tools for clinicians treating spinal conditions in need of augmentation and stabilization via interbody devices. The CT-OAM method is easily translated to the clinical setting, has been validated in many other joints, and does not impose added tests or costs on the patient.
Footnotes
Authors’ Note
Each author certifies that his or her institution waived approval for the reporting of this investigation and that all investigations were conducted in conformity with ethical principles of research. The Manuscript submitted does not contain information about medical device(s)/drug(s). This work was performed at Rush University Medical Center, Chicago, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study’s research activities were funded by a Cervical Spine Research Society (CSRS) Seed/Starter grant.