
Abstract
Study Design
Basic Science.
Objective
Poor subchondral bone mineral density (sBMD) has been linked with subsidence of cervical interbody devices or grafts, which are traditionally placed centrally on the endplates. Considering that sBMD reflects long-term stress distributions, we hypothesize that the cervical uncovertebral joints are denser than the central endplate region. This study sought to investigate density distributions using computed tomography osteoabsorptiometry (CT-OAM).
Methods
Twelve human cervical spines from C3–C7 (60 vertebrae, 120 endplates) were imaged with CT and segmented to create 3D reconstructions. The superior and inferior endplates were isolated, and the sBMD of the whole endplate, endplate center, and uncus was evaluated using CT-OAM. Density distributions were compared across the subaxial cervical spine.
Results
The uncinate region of the inferior and superior endplates was significantly denser than the central endplate across all vertebral levels (P < .01). When comparing sBMD of the whole inferior and superior endplates, the superior endplate was significantly denser than the inferior endplate (P < .0001). However, the inferior uncus was denser than the superior uncus (P = .035). When assessing sBMD by vertebral level, peak densities were observed at C4 and C5, while C7 was, on average, significantly less dense than all other vertebrae.
Conclusion
The subchondral bone of the cervical uncovertebral joints is significantly denser than the central endplates. While the superior endplate in its entirety is denser than the inferior endplate, the inverse was true for the uncovertebral joints. This study serves as a basis for future investigations of new implant designs and their implications on subsidence.
Keywords
Introduction
The use of interbody devices is common in cervical spine surgery to address mechanical or neurological derangements stemming from degenerative and other processes. 1 Through preservation of disc height and alignment, procedures such as anterior cervical discectomy and fusion (ACDF) and total disc arthroplasty (TDA) have demonstrated positive clinical outcomes. 2 However, such procedures are commonly complicated by interbody device subsidence, with rates ranging from 13.2% to 62.5%. 3 Although subsidence may be a step in the natural process of fusion and device bonding to host bone, several studies have demonstrated that significant subsidence of the device led to alteration in spinal alignment and increased risk of device migration and cyclical loosening.4-6 These complications could result in abnormal kinematics, segmental kyphosis, recurrent stenosis, or even catastrophic vertebral body fracture.6,7 Therefore, elucidation of the subsidence process and its associated risk factors is of increasing interest to preserve clinical outcomes.
Several risk factors for subsidence have been identified. Relative to the implant, the difference in elastic modulus between a stiff implant material and softer adjacent cortical bone has been cited as a factor. 4 Therefore, more elastic materials that mimic cortical bone (such as allograft or PEEK) may be preferred. 8 Other cited risk factors include the number of treatment levels, treatment at lower cervical levels (C5–C7), excessive endplate preparation, construct configuration, or non-adherence with postoperative brace wear.9,10 Osteoporotic bone has also been implicated with poor device performance. 11 Although global measurement of bone mineral density (BMD) has demonstrated relevance, the specific distribution of BMD throughout the endplate is limited. Muller-Gerbl et al 12 previously used computed tomography osteoabsorptiometry (CT-OAM) to demonstrate that density was highest in the posterior and lateral endplate regions and lowest in the anterior and central aspects. However, this analysis did not specifically analyze differences in certain regions of interest, such as the uncovertebral joint relative to the central endplate.
It is currently unknown whether variations in load distributions between the central endplate and uncinate region translate into differences in subchondral BMD (sBMD). The uncovertebral articulation is known to play a pivotal role in coordinated motion of the cervical spine, such as axial rotation with lateral flexion.13,14 Additionally, as the intervertebral disc loses height with normal aging, the uncus adapts to assume greater load from the vertebral column above. 13 Due to this inherent variability in function, we hypothesize that the sBMD of the uncus would therefore be greater than that of the central endplate. Understanding this density distribution has significant clinical relevance to performing successful cervical interbody surgery and even potentially to the development of new interbody device designs.
Therefore, the objective of this study is to use CT-OAM to map the sBMD of the superior and inferior endplates throughout the subaxial cervical spine. We hypothesize that due to long-term stress distribution on the uncovertebral joints, the uncinate processes will demonstrate greater sBMD when compared to the central endplate. Additionally, we hypothesize that the endplates of the mid-cervical levels will have greater sBMD than the lower levels, based on prior clinical findings of subsidence.
Materials and Methods
Specimens
This study was exempt from Institutional Review Board review owing to the use of deidentified human cadaveric specimens. A total of twelve fresh human cadaveric cervical spines were obtained from an approved tissue bank (ScienceCare, Phoenix, AZ). Six female and 6 male specimens were used, with an average age of 55.67 (range 27–89) and a mean BMI of 26.56 (range 17.5–40.2).
3D Segmentation
All specimens underwent CT imaging at a slice thickness of .625 mm. Axial, sagittal, and coronal raw imaging data was then exported in the DICOM format. These files were imported into the Mimics three-dimensional (3D) segmentation software (Materialise, Leuven, Belgium) for the creation of 3D models of the C3 to C7 vertebrae (60 cervical vertebrae total). Using a custom coordinate system-based program, the superior and inferior endplates of all vertebrae were isolated (120 cervical endplates total). Following whole endplate segmentation, the uncinate regions of the superior and inferior endplates were isolated from the remaining endplate center (Figure 1). 3D segmentation of (A) the entire C3 vertebra, whole superior endplate, uncinate processes, and endplate center (B) demonstrates these regions on the superior and inferior endplates.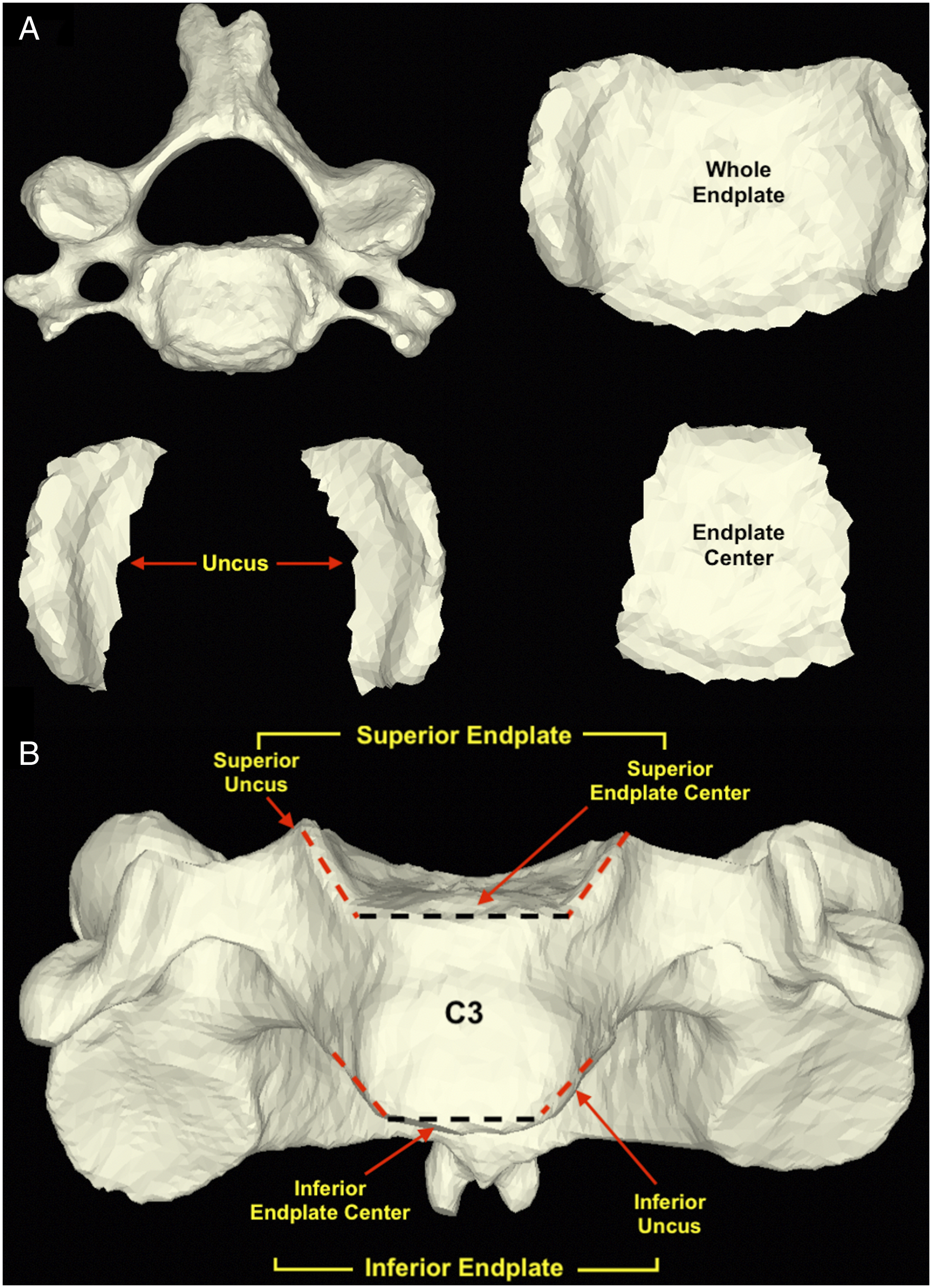
CT-OAM Analysis
Using CT-OAM, the sBMD was measured for the whole endplate, endplate center, and uncus of all 120 endplates (Figure 2). This was performed using a custom program which identified the topographical endplate surface via a coordinate system in the axial plane. Density measurements were collected from the endplate surface (depth of 0 mm) to a depth of 4 mm at .5 mm increments, for a total of 8 sBMD measurements. The maximum reading of sBMD was considered the region of interest (ROI) and was used for comparative analysis. Past work has demonstrated that this ROI is most consistently at a depth of 1.5 mm–3.0 mm in the facet joints; therefore, a similar range was adopted for this study.15 Densitogram demonstrating the subchondral bone mineral density (sBMD) distribution of the superior and inferior cervical endplates as assessed by computed tomography osteoabsorptiometry (CT-OAM).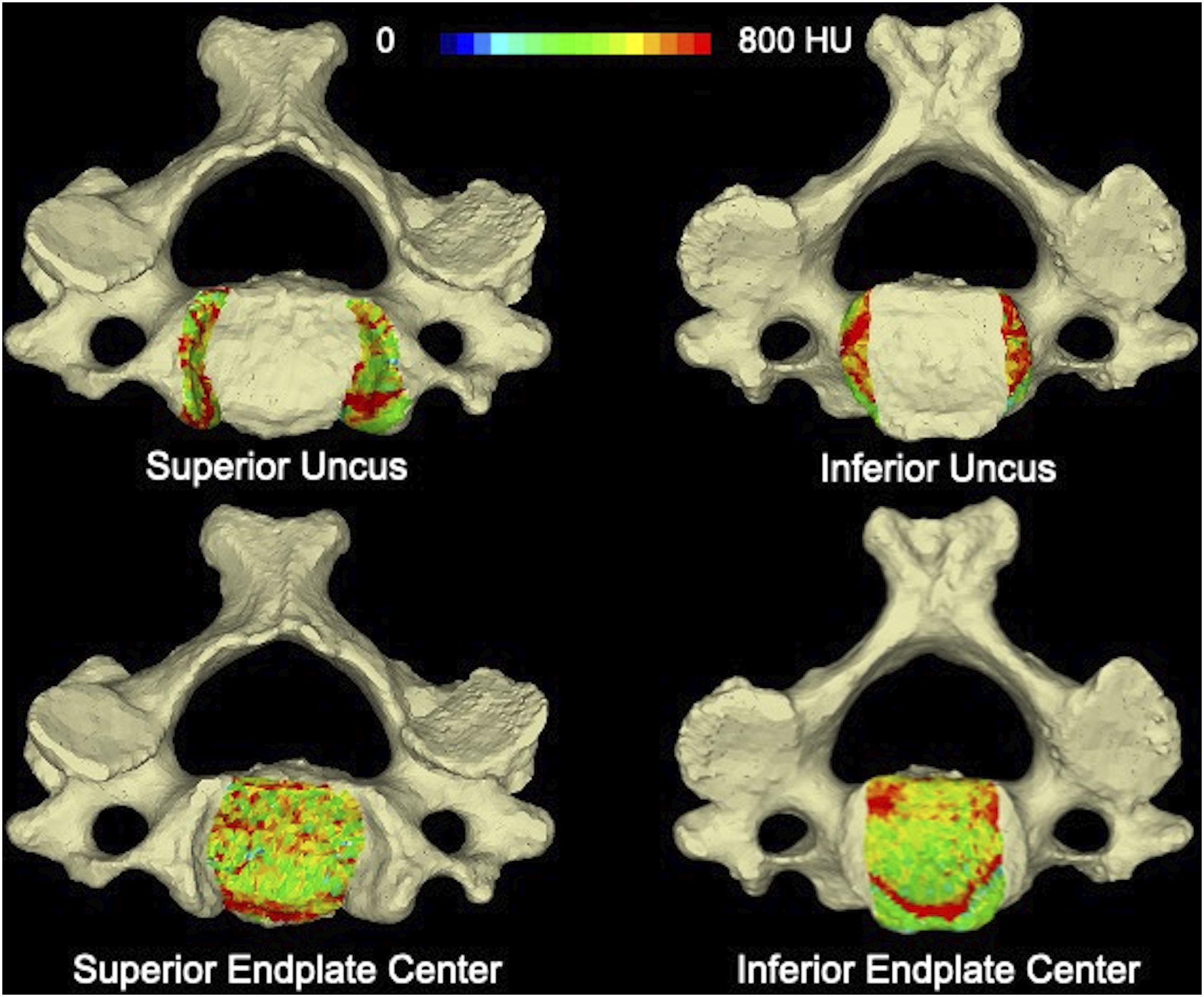
Statistical Analysis
All statistical methods were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY). sBMD data was determined to be normally distributed using the Shapiro–Wilk test; therefore, parametric testing was employed. The sBMD of the endplate regions (center vs uncus) and inferior vs superior endplates of the same vertebral body were compared using dependent t-test. Endplate sBMD was compared by cervical vertebral level via repeated-measures analysis of variance with post hoc dependent t-test and Bonferroni correction. This relationship was further explored via polynomial regression analysis with a quadratic model. Multivariate linear regression was used to evaluate the independent effect of sex and age on sBMD. The results are presented as means with corresponding standard deviations (SD). The threshold for statistical significance was set to P < .05.
Results
Endplate Center vs Uncus
A total of 60 inferior endplates were analyzed across the 12 specimens with a mean whole endplate sBMD of 526.92 ± 111.57 Hounsfield units (HU). The sBMD of the inferior uncus was significantly denser than the endplate center (690.60 ± 177.01 HU vs 514.77 ± 117.00 HU, P < .0001). The 60 superior endplates analyzed had an average whole endplate sBMD of 562.00 ± 133.45 HU. Similarly, the sBMD of the superior uncus was significance denser than the endplate center (658.88 ± 155.63 HU vs 528.52 ± 135.08 HU, P < .0001) (Figure 3). Subchondral bone mineral density in Hounsfield units (HU) in the regions of interest of the inferior and superior endplates. Asterisks denote statistical significance.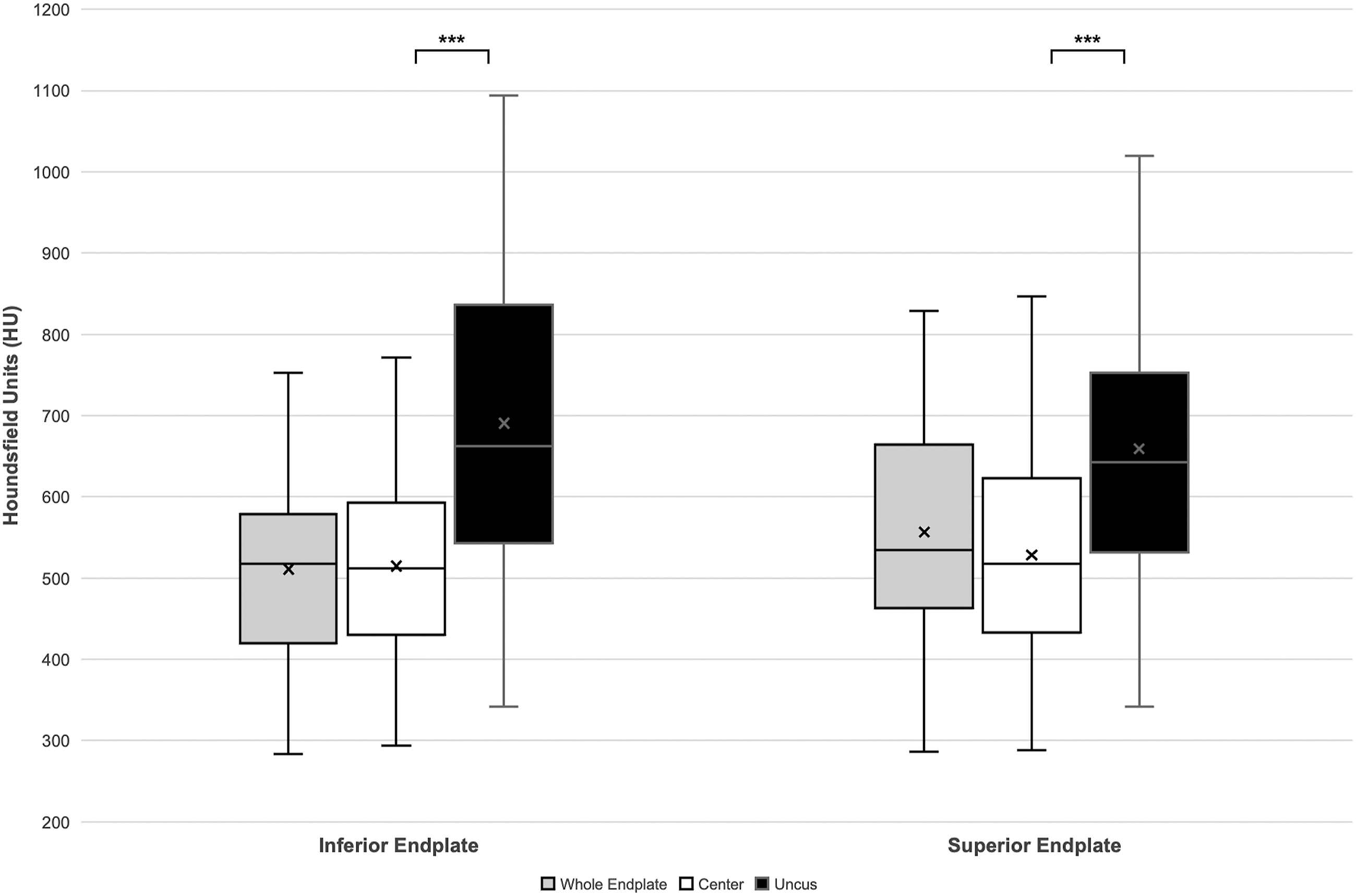
Sub-analysis evaluating sBMD by vertebral level demonstrated that the uncus of the vertebral body inferior endplates was significantly denser than the endplate centers at all levels. This included C3 (P = .0003), C4 (P < .0001), C5 (P = .001), C6 (P = .004), and C7 (P = .005). Similarly, the uncus of the vertebral body superior endplates was significantly denser than the endplate center at all levels, including C3 (P < .0001), C4 (P < .0001), C5 (P = .007), C6 (P = .004), and C7 (P < .0001) (Figure 4). sBMD in Hounsfield units (HU) by cervical vertebral level in the vertebral body (A) inferior endplate and (B) superior endplate. Asterisks denote statistical significance.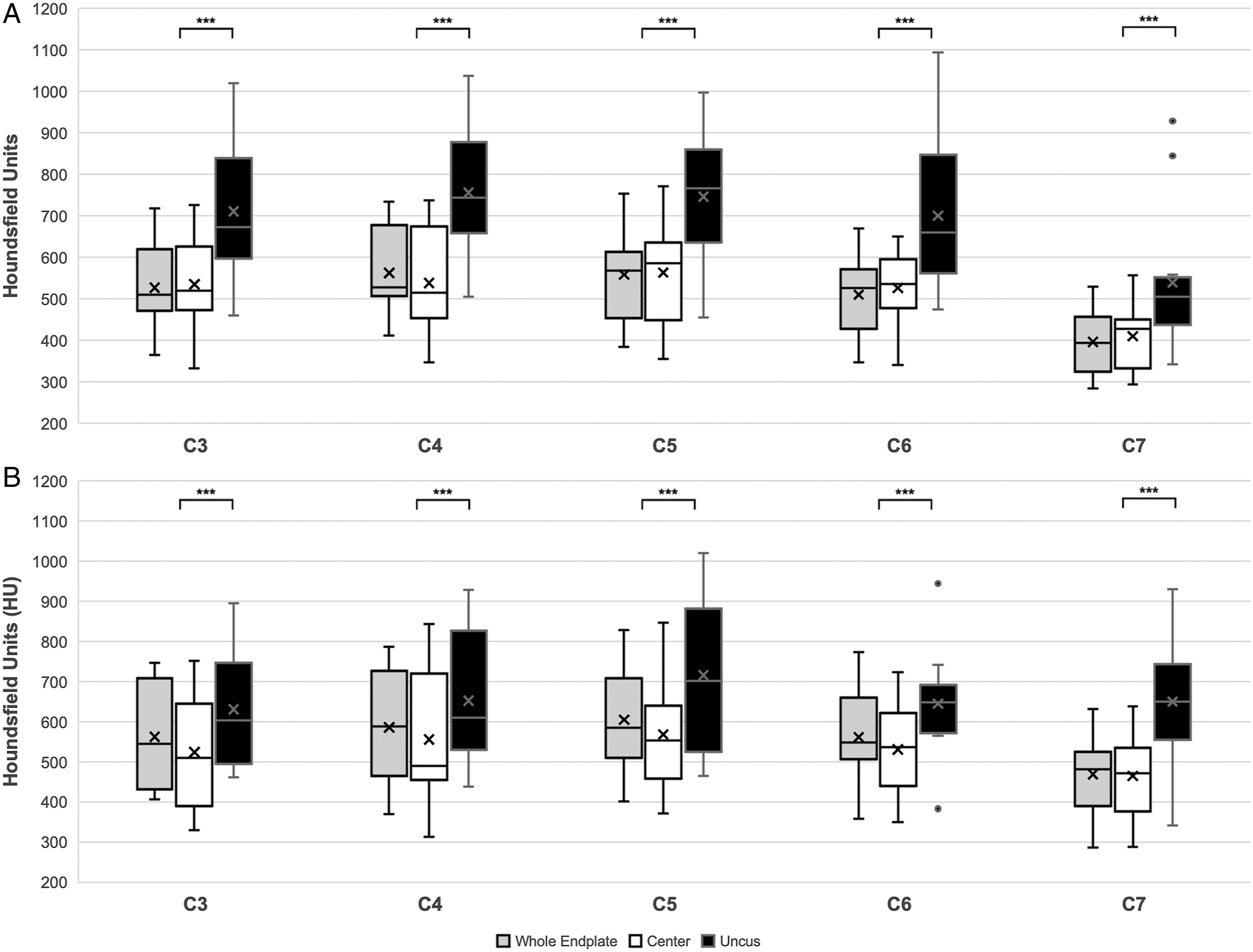
Inferior vs Superior Endplates
Comparison of Inferior and Superior Endplate Subchondral Bone Mineral Density in Hounsfield Units (HU) at all Levels and by Cervical Vertebral Level.
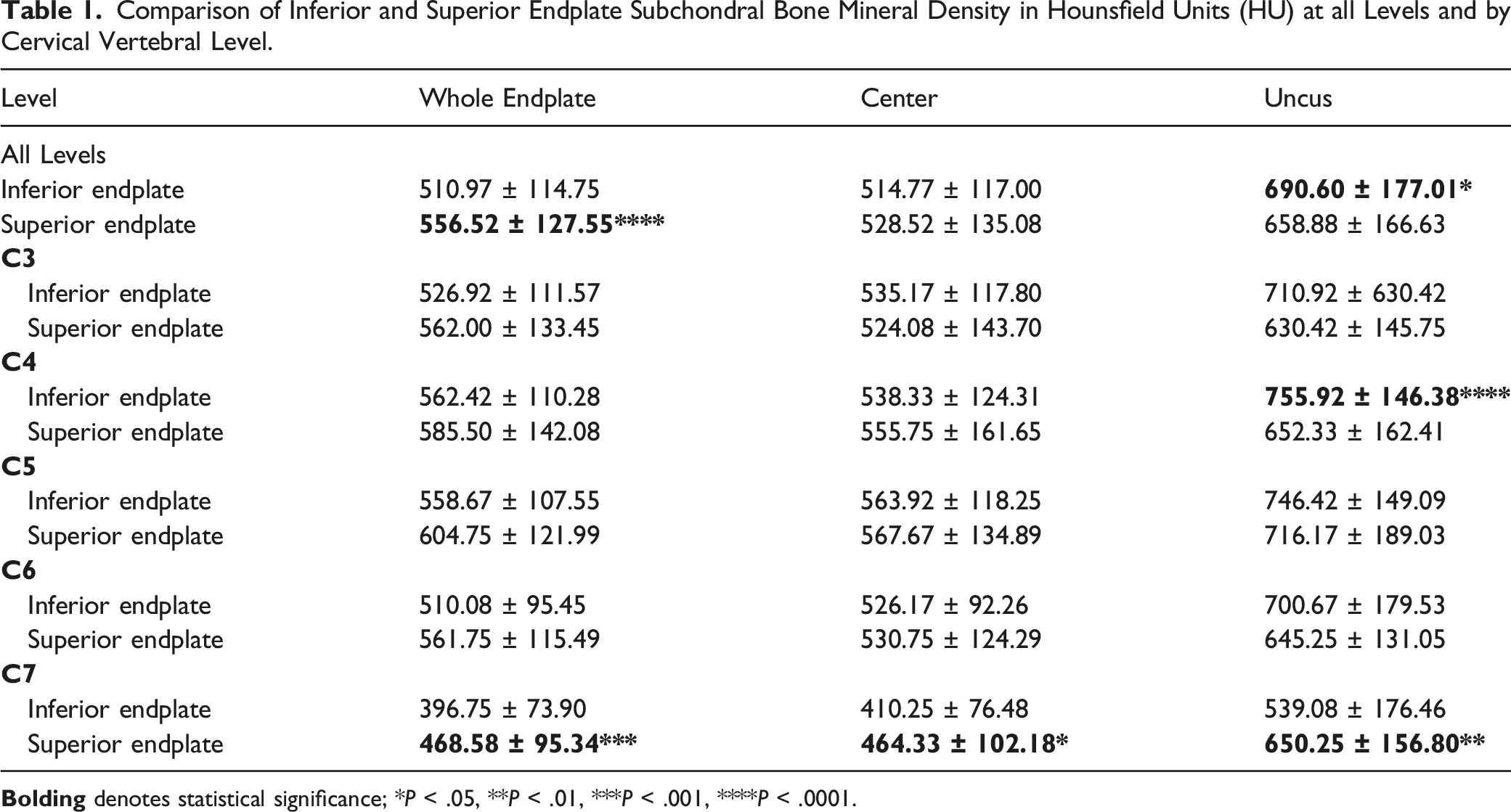
Further sub-analysis was performed by vertebral level. At C4, the inferior uncus was significantly denser than the superior uncus (755.92 ± 146.38 HU vs 652.33 ± 162.41 HU, P < .0001). At C7, the inferior whole endplate was significantly less dense than the superior whole endplate (396.75 ± 73.90 HU vs 468.58 ± 95.34 HU, P = .0002). Similar relationships were seen at the endplate center (410.25 ± 76.48 HU vs 464.33 ± 102.18 HU, P = .020) and uncus (539.08 ± 176.46 HU vs 650.25 ± 156.80 HU, P = .006). This latter finding is contradictory to the overall trend seen at all other levels, which demonstrated greater density at the inferior uncus relative to the superior uncus. Therefore, further analysis was performed excluding C7 (C3–C6 only), demonstrating significantly greater sBMD in the inferior uncus of C3–C6 than the superior uncus (728.48 ± 157.22 HU vs 661.04 ± 156.93 HU, P < .0001).
Subchondral Bone Density by Level
The average sBMD values were compared among cervical vertebral levels. The inferior endplates of the C7 vertebrae had significantly lower sBMD (P < .05) when evaluating the whole endplate, endplate center, and the uncus relative to all other levels. This was true for the superior whole endplate of C7 (P < .05) compared to all other vertebrae, with the exception of C3. Other significant between-level differences were also seen, with highest sBMD recorded at C4 and C5, as demonstrated by Figure 5. Comparison of regional subchondral bone mineral density in Hounsfield units (HU) by cervical vertebral level. Asterisks with brackets denote statistically significant differences between levels.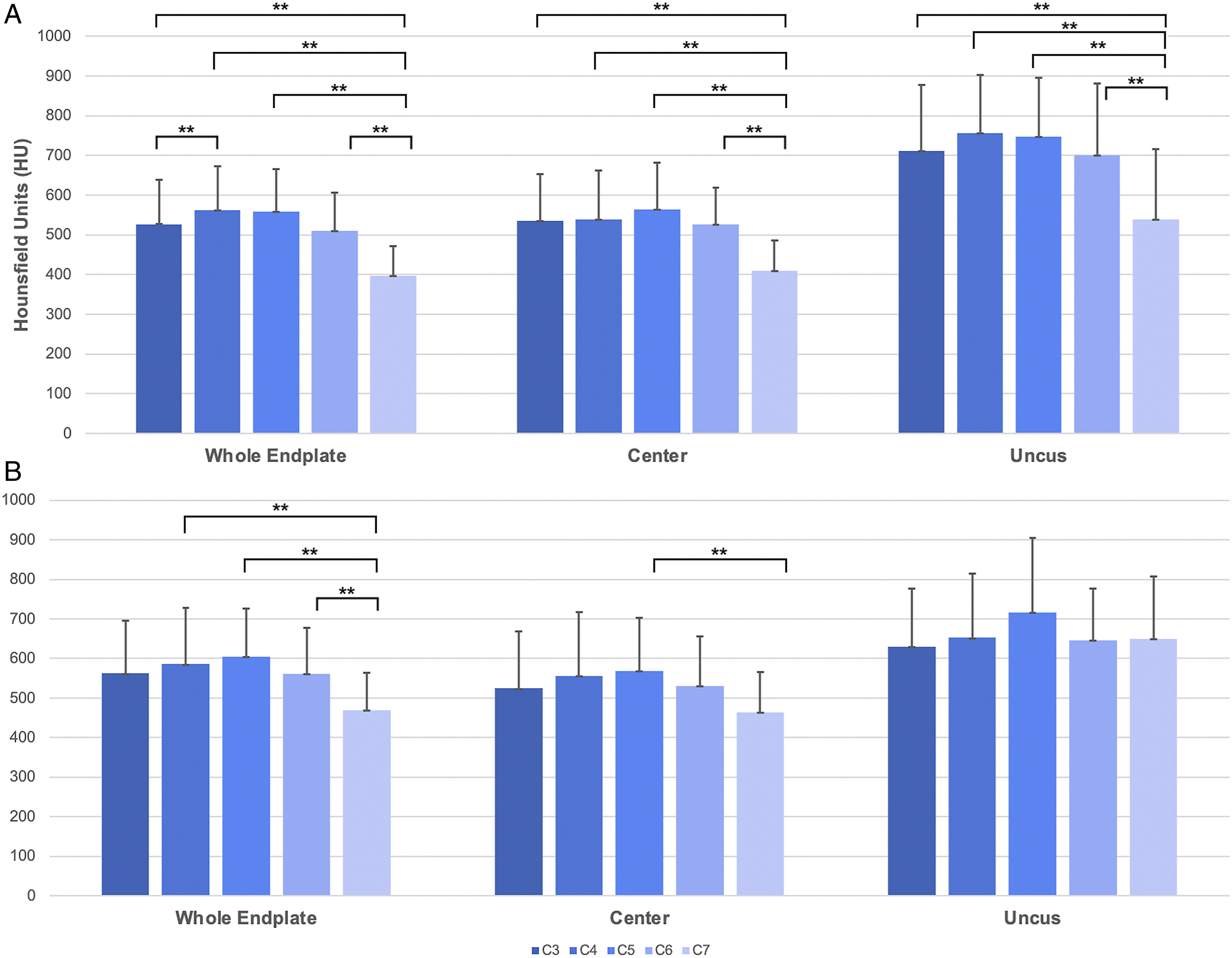
The relationship of cervical level and sBMD was further explored via regression analysis. A quadratic model was found to best represent the data due to the curvilinear distribution of data; therefore, polynomial regression analysis was used. Using this model to investigate the inferior endplate, significant curvilinear relationships were found for the whole endplate (R2 = .282, P = .003), endplate center (R2 = .201, P = .016), and uncus (R2 = .203, P = .021). When evaluating the superior endplate, a significant curvilinear relationship was found for the whole endplate (R2 = .136, P = .020), but not for the endplate center (R2 = .071, P = .095) or uncus (R2 = .024, P = .271). This means that sBMD increases at the vertebrae caudal to C3, peaking around C4 or C5 before progressively decreasing again at C6 and C7 (Figure 6). Significant curvilinear relationships of subchondral bone mineral density with cervical vertebral levels at the (A) inferior whole endplate, (B) inferior endplate center, (C) inferior uncus, and (D) superior whole endplate. Red lines represent the 95% confidence intervals of the curve (black line).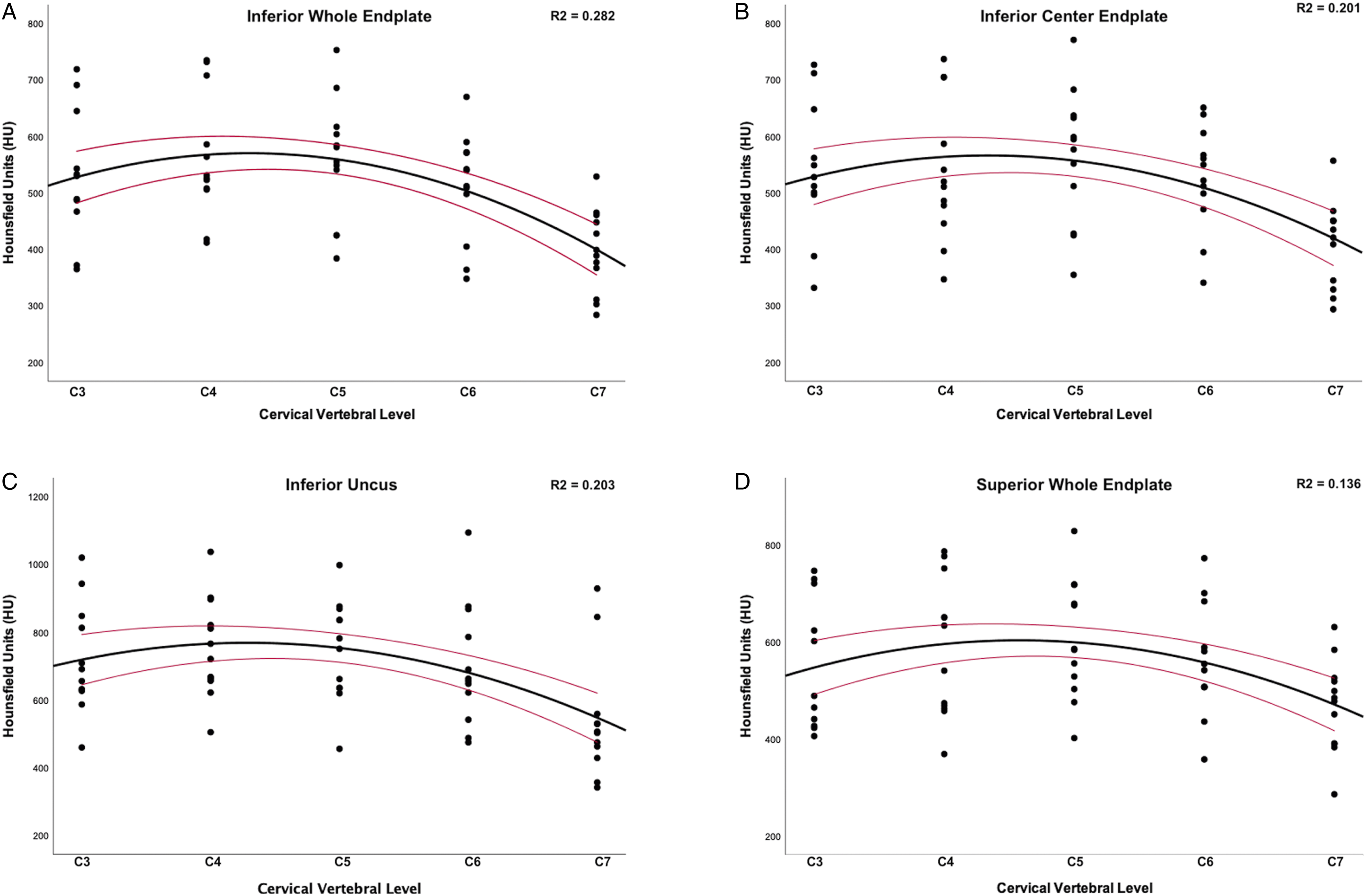
Effect of Age and Sex on Bone Density
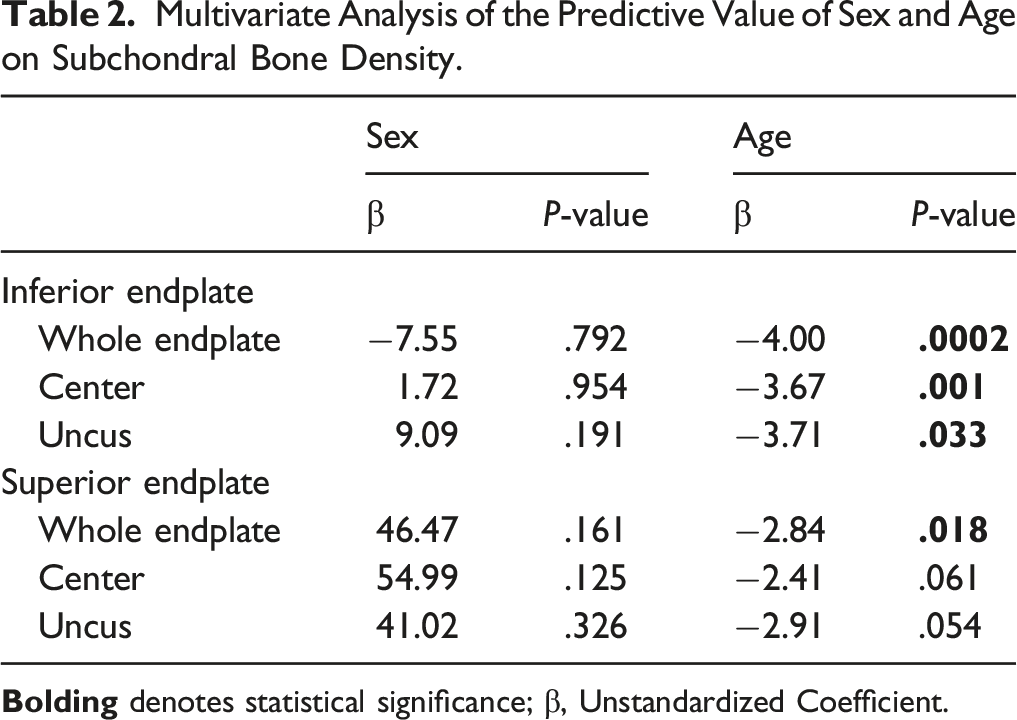
Multivariate Analysis of the Predictive Value of Sex and Age on Subchondral Bone Density.
Discussion
This study sought to investigate the regional sBMD of the cervical endplates, comparing CT-OAM density measurements of the central endplate and uncus of the inferior and superior endplates across the C3–C7 vertebrae. Notably, the uncus was found to be significantly denser than the central endplate region across inferior and superior endplates at all cervical levels. Additionally, the superior endplates were found to have significantly greater sBMD relative to the inferior endplates, although the inverse was true for the subchondral bone of the uncovertebral joints. When comparing density across cervical levels, sBMD was found to be distributed in a curvilinear fashion, with the highest density in mid-cervical spine and lowest density at C7. Age negatively affected sBMD, while sex had no independent effect.
This study has several limitations which must be considered when interpreting its results. First, this study used cadaveric specimens to quantify sBMD, limiting the number that could be evaluated. Despite the limited number of specimens, a total of 60 vertebrae (120 endplates) were analyzed, and highly significant differences were found. Furthermore, the specimens used encompassed a wide age range (mean: 55.67 year, range: 27 to 89 year). However, this allowed for an accurate depiction of the broad demographic typically undergoing surgery to the anterior cervical spine. Finally, the manual segmentation process used to isolate the uncinate regions from the central endplate introduces the potential for human error. This can be attributed to inter-specimen and inter-level variability in uncinate height, width, and angle, all of which may have contributed to slight over- or underestimation of the uncinate surface area.
The traditional paradigm of anterior cervical surgery with an interbody device involves device placement centrally on the endplate. However, poor bone quality may contribute to interbody subsidence and associated morbidity.3,9,16,17 This study found that, on average, the uncinate regions of the inferior and superior endplates were approximately 34% and 25% denser than the central endplates, respectively. Further, these findings corroborate those of Muller-Gerbl et al 12 who used CT-OAM to demonstrate the topographic mineralization in endplates, finding regions of highest mineralization in the posterior and lateral aspects. Given that sBMD is known to reflect the long-term distribution of stress on bones and joints, these findings may potentially be explained by differences in load across the uncovertebral joint and intervertebral disc.18,19 The nucleus pulposus of the intervertebral disc has high proteoglycan and water content, in effect acting as a cushion by transmitting dynamic load outward to the spinal ligaments. 20 On the other hand, the uncovertebral joint plays a pivotal role in the stability of cervical motion segments in all planes of motion, while also contributing significantly to load bearing.13,21 This is especially important in the context of spondylosis, where thinning of the intervertebral disc results in a greater axial load on the uncus.22,23
Past studies have consistently found significant variation in sBMD by cervical vertebral level, with highest density in the C4 and C5 bodies and lower density at C7 relative to all other levels.17,24-27 The present analysis redemonstrated this relationship, also showing that this was true for both the central endplate and uncinate regions. This is specifically clinically relevant as a past study by Kao et al 9 investigating subsidence of stand-alone PEEK interbody devices demonstrated a higher risk when placed at the C5–C6 and C6–C7 segments. Anderst et al 25 conjectured that these density findings may potentially be attributed to greater in vivo load in the mid cervical spine, with resultant higher sBMD. Prescher 28 further postulated that the vertebrae at C3 through C5 may also experience greater load due to natural cervical lordosis. On the other hand, the C7 vertebra sits more vertically and is substantially larger than the cephalad vertebral bodies, potentially leading to a greater mismatch in volume and density. Additionally, several investigations of cervical kinematics have found that segmental motion is highest in the mid-cervical spine, paralleling the distribution of sBMD by level seen in this study.29,30
To the best of our knowledge, this is the first study to directly compare the sBMD of the inferior and superior cervical endplates of the same vertebral body. The results demonstrate that the subchondral bone of the whole endplate is denser at the superior relative to the inferior endplate. This finding is intuitive considering that interbody device subsidence is most commonly reported to affect the inferior endplate. 31 However, the opposite relationship was true at the uncinate region, where sBMD was greater at the inferior endplate. This could potentially be attributed to the anatomic relationship of the inferior uncus with the pedicles. Relative to the uncus of the superior endplate, the inferior uncinate region has greater continuity with the bone of the ipsilateral pedicle, which has been shown by Anderst et al 25 to be the anatomic region of the cervical spine with the highest sBMD. Interestingly, the uncinate region of the C7 inferior endplate was found to be significantly less dense than the C7 superior uncus. A possible explanation for this observation could be the transition toward thoracic vertebral anatomy, since the uncovertebral joints are typically exclusively found between the C3 through C7 vertebrae. 13 Therefore, the articulation of the inferior endplate of C7 with the flatter surface of the superior endplate of T1 may be characterized by a more even load distribution.
The findings of this investigation may have significant implications when translated into clinical practice. Traditional cervical interbody devices are placed centrally on the endplate. However, as the results of this analysis have demonstrated, these devices do not leverage the much denser bone in the posterolateral regions. More modern device designs could target these regions of higher sBMD by extending further laterally to place greater load at the uncovertebral joint. Theoretically, this could provide several advantages thus reducing the risk for subsidence. Bell et al 32 showed that a 25% difference in vertebral body BMD corresponds to a 50% difference in bone strength and integrity. Therefore, considering that the uncinate regions were 25%-34% denser than the central endplate, this could translate to a minimum 1.5 times increase in strength, hypothetically decreasing the risk for endplate failure. Furthermore, such designs would evenly distribute the load of cephalad structures in 2 regions, while also maximizing the surface area of contact with host bone. This could be especially beneficial at the inferior endplate, which has a lower overall sBMD relative to the superior endplate, but a denser uncinate region. This would also confer the advantage of a larger window for the placement of graft and biologics. Moreover, this load distribution may provide improved stability for stand-alone configuration devices, which have demonstrated a reportedly lower rate of arthrodesis and construct integrity following ACDF in the literature when compared to those augmented with an anterior static plate.33-36 This has largely been attributed to poorer initial fixation. Future comparative biomechanical studies should investigate the implications of these findings on regional contact pressures and endplate failure when loading the central endplate vs the uncinate regions. Such studies may help inform future directions for clinical investigation.
Conclusion
This study utilized CT-OAM to demonstrate that the sBMD of the cervical uncovertebral joint between C3 and C7 is significantly denser than the bone of the central endplate. When comparing sBMD between inferior and superior endplates, the superior endplate was denser in its entirety. However, the inverse was true for the bone in the uncinate region. Furthermore, endplate sBMD was greatest in the mid-cervical spine and lowest at C7, with advanced age negatively affecting bone quality. Future investigations are warranted to elucidate the biomechanical and clinical implications of these findings.
Each author certifies that his or her institution waived approval for the reporting of this investigation and that all investigations were conducted in conformity with ethical principles of research.
The article submitted does not contain information about medical device(s)/drug(s).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.