
Abstract
Study design
Observational cohort study.
Objective
To assess the association of Modic changes and DEBC classification in patients with cervical degenerative disc disease.
Methods
The study includes 2 groups, neck pain patients presenting to the out-patient services (neck pain group) (n = 301) and polytrauma patients without cervical spine injury or a history of neck pain, who underwent whole spine MRI (control group) (n = 200). Degenerative changes in the MRI were classified according to the Modic changes (MC) and DEBC classification. Modifiers including End-Plate (EP) erosion and herniation (H+) presence were documented.
Results
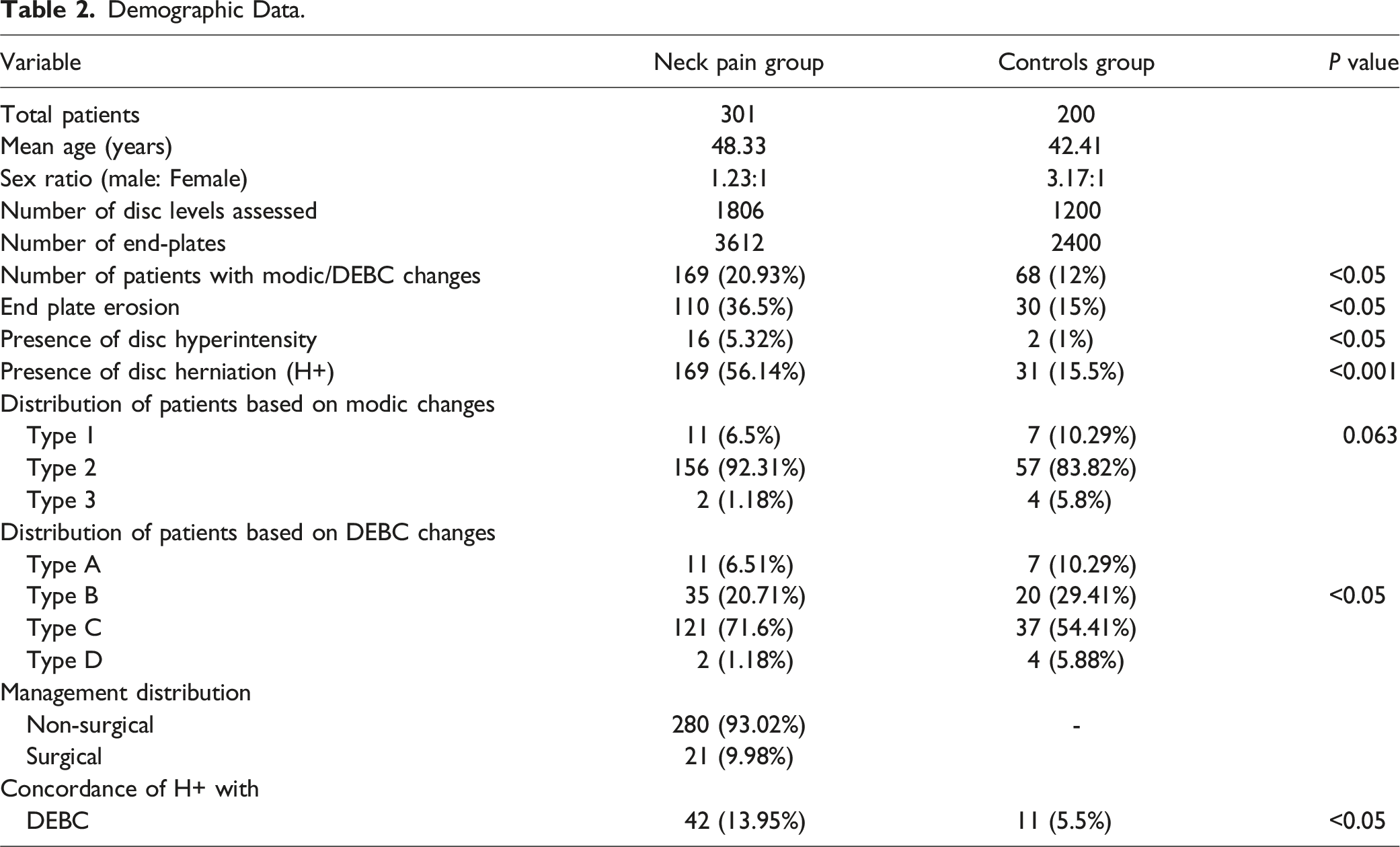
3612 EPs of 301 patients with neck pain and 2400 EPs of 200 controls were assessed. The incidence of MC and DEBC in the neck pain group was 20.93% and in the control group, it was 12%, (P < 0.05). In the neck pain group with DEBC changes, the distribution was Type A-6.51%; Type B-20.71%; Type C-71.6%; and Type D - 1.18%, while in the controls the distribution was Type A-10.29%, Type B-29.41%, Type C-54.41%, and Type D - 5.88%, The co-occurrence of H+ with DEBC in cases and controls was 13.95% vs 5.5% (P < 0.005). The odds ratio for the need for surgery was highest (OR: 6.8) when H+ and DEBC change co-occurred.
Conclusion
Our study highlights that patients with DEBC changes and disc herniation were more likely to experience neck pain and require surgical intervention, indicating the reliability and clinical significance of the DEBC classification in degenerative cervical spine patients.
Keywords
Introduction
Cervical disc degeneration is quite prevalent, with approximately 25% of individuals under the age of 40 showing signs of cervical degeneration. This percentage increases to over 60% in people over 40 years.1,2 Advanced degeneration may lead to degenerative disc disease with a wide clinical spectrum ranging from neck pain to myeloradiculopathy. 3 Symptoms are usually sufficiently alleviated with a conservative mode of management and surgeries are reserved for severe and progressive disease. 3
Various imaging phenotypes associated with degenerative disc disease observed on magnetic resonance imaging (MRI) such as Modic changes (MC) and endplate abnormalities have been identified.4-9 Modic changes involving vertebral end-plates were first described by Michael Modic in 1988 and have gained significant implications in degenerative diseases of the lumbosacral spine. 4 The clinical correlation of Modic changes in the cervical spine has been constantly debated over the last several years. Baker et al studied the effect of Modic changes and end-plate changes on outcomes following cervical spine surgery based on T1 and T2W images. 10 However, the Modic classification utilising only T1W and T2W sequences has some drawbacks as described by Rajasekaran et al, who introduced the Disc-Endplate-Bone Marrow Complex (DEBC) classification. This classification utilises STIR sequences in addition to the T1W and T2W series to identify edema masked by the fat-induced signal changes on T1W and T2W images. 11 The other concern with the Modic classification was the consideration of only the subchondral bone marrow changes while neglecting changes in disc and endplates, which is again controversial, as disc, end plate, and bone marrow complex form a single anatomical and functional interdependent unit. This has been proved by various studies in the past. 12 While Baker et al included the endplate changes in association with Modic changes, DEBC includes changes in the discs as well.10,11 The purpose of this study is to associate DEBC changes with the Modic changes in patients presenting with cervical degenerative disc disease and to understand the clinical implications of DEBC classification
Materials and Methods
This study was conducted at a tertiary-level referral centre after obtaining Institutional Review Board (IRB) approval (IRB No: 2022/5/08). Prospectively collected data from a single institution was analyzed retrospectively for degenerative changes in the cervical spine and correlated clinically. Consent was obtained from all patients included in the study. 301 consecutive patients who visited the spine outpatient department with complaints of neck pain for at least 3 weeks formed the study (neck pain) group. 200 consecutive patients who underwent whole spine MRI for isolated brain, thoracic, and lumbar spine injuries without neurological deficit formed the control group. The MRI was taken immediately after their presentation to the hospital but before surgery. Patient demographics, clinical presentation, and outcomes up to 2 years were recorded. Patients with trauma to the cervical spine, infection, spondyloarthropathies, deformity, or previous surgery were excluded. All radiological images were retrieved from the hospital’s Picture Archiving and Communication System (PACS).
The cervical segments including C2-C3 disc to C7-T1 discs and adjacent EPs in the control and case groups were assessed for MC types using a 3T (Siemens, Germany), Magnetom Lumina platform using fast spin-echo. Degenerative changes in the same segments were also classified based on the ‘Disc-End Plate-Bone-Marrow Complex’ classification by a spine surgeon and radiologist (Figure 1) (Table 1). ‘Disc- End plate-Bone-Marrow Complex’ changes. The figure shows 4 different types of DEBC. Type A (A), (B), (C) shows T1W hypo, T2W hyper, and STIR hyperintense signal changes. Disc hyperintensity may or may not be present and the end plate is often indistinct with possible erosions. It represents an ongoing acute active inflammatory process. Type B (D), (E), (F) shows edema in STIR interspersed with either fat or sclerosis and represents a state of ‘Chronic persistent inflammation’. Disc hyperintensity may or may not be present and the endplate shows erosions. Type C (G), (H), (I) shows hyperintensity in both T1 and T2 and hypointensity in STIR. There is no hyperintensity in discs and end plate erosions are present. It represents a state of ‘Latency’ with no element of acute activity. Type D (J), (K), (L) shows hypointense signals on all 3 sequences. There is no hyperintensity in discs and end plate erosions are present. It represents inactivity. Radiological Basis for Classification of the DEBC Changes.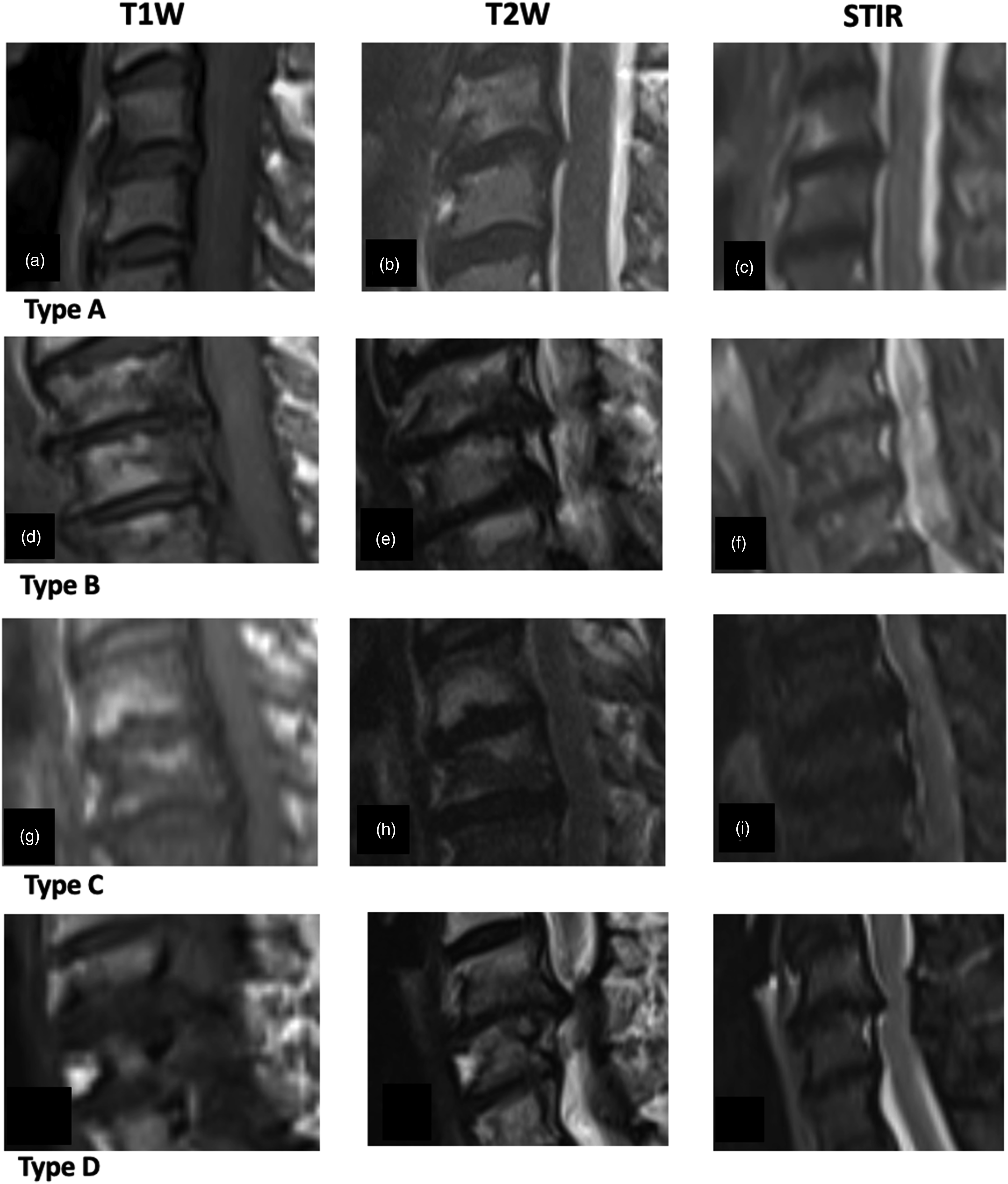

The study analysed the association between the Modic changes and DEBC classification in patients with cervical degenerative disc disease. Also, we evaluated the association of each of the components of the DEBC changes, including the disc, end plate, and sub-chondral bone marrow changes with the need for surgical intervention.
Significance was calculated by binomial test and Chi-square test with the effect size of 0.3-0.5. Prevalence and association of outcome were calculated by Altman’s - Odd ratio with the 95 % CI and the scoring of z statistics. Logistic expression was plotted for independent variables associated with each class of both Modic and DEBC against dependent variables surgery and non-surgery.
Results
Demographics
Demographic Data.
Assessment of MC
Distribution of Modic and DEBC Changes in Control and Neck Pain Group.
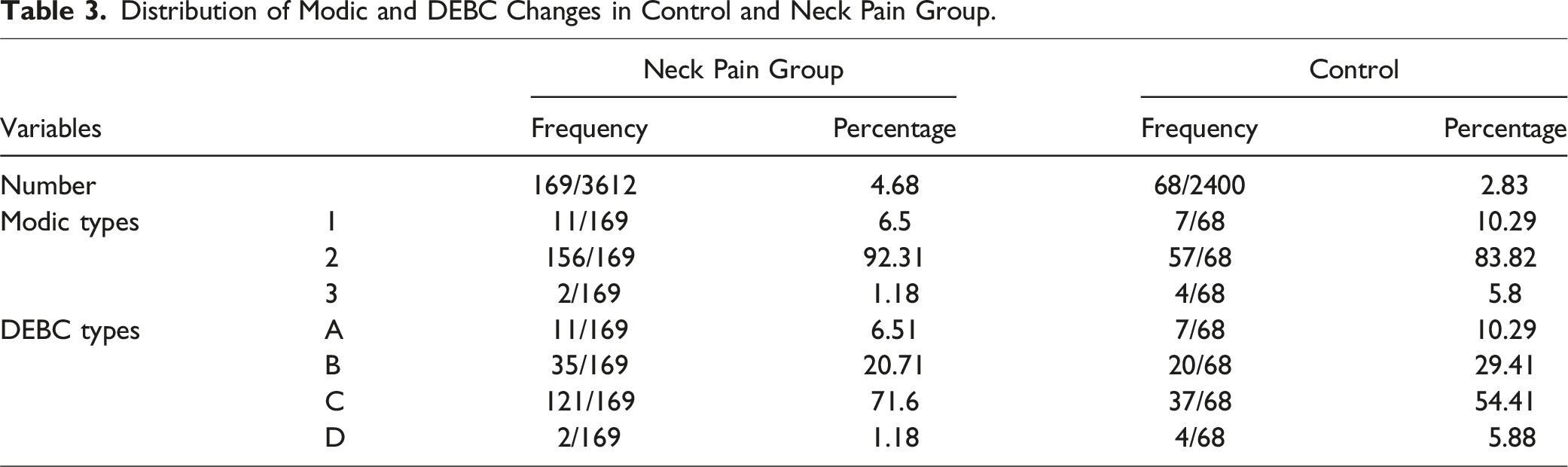
In the control group, the MC incidence was 12% (68/200) among which 10.29 % had Type 1 MC, 83.82% had Type 2 MC and 5.8% had Type 3 MC. Among the cervical levels, MC was predominantly noticed at C4-C5 and C5-C6 (37.5% each) in the controls (Tables 1 and 3).
Assessment of DEBC Changes
Among the neck pain group with DEBC changes, the distribution was Type A-6.51%; Type B-20.71%; Type C-71.6%; Type D - 1.18%, while in controls with DEBC changes, the distribution was Type A-10.29%, Type B-29.41%, Type C-54.41%, and Type D - 5.88%, (P < 0.05) (Table 3). The intra-observer and inter-observer variability correlation for classifying DEBC changes measured by Kappa was 0.81 except for the presence of disc hyperintensity (DH), which was 0.71.
Presence of Modifiers
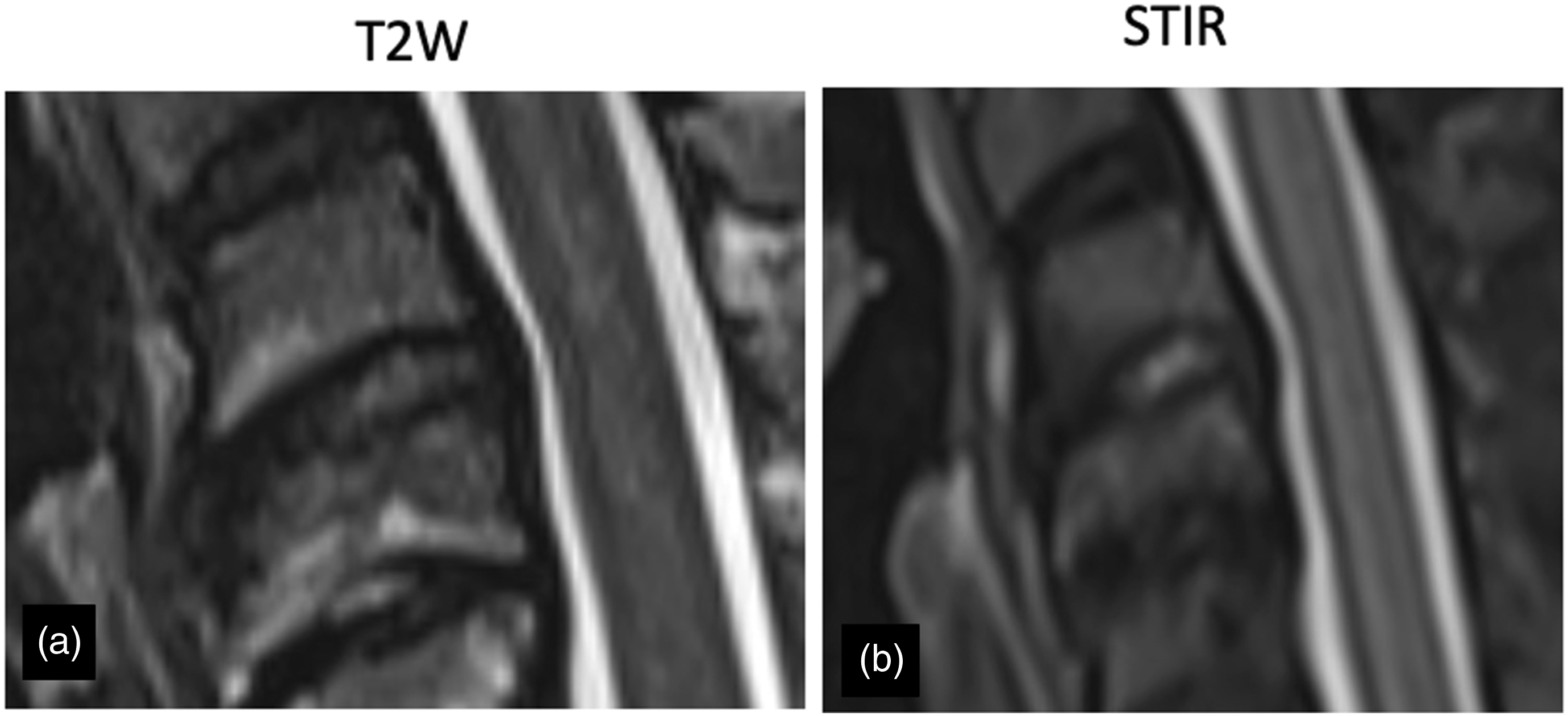
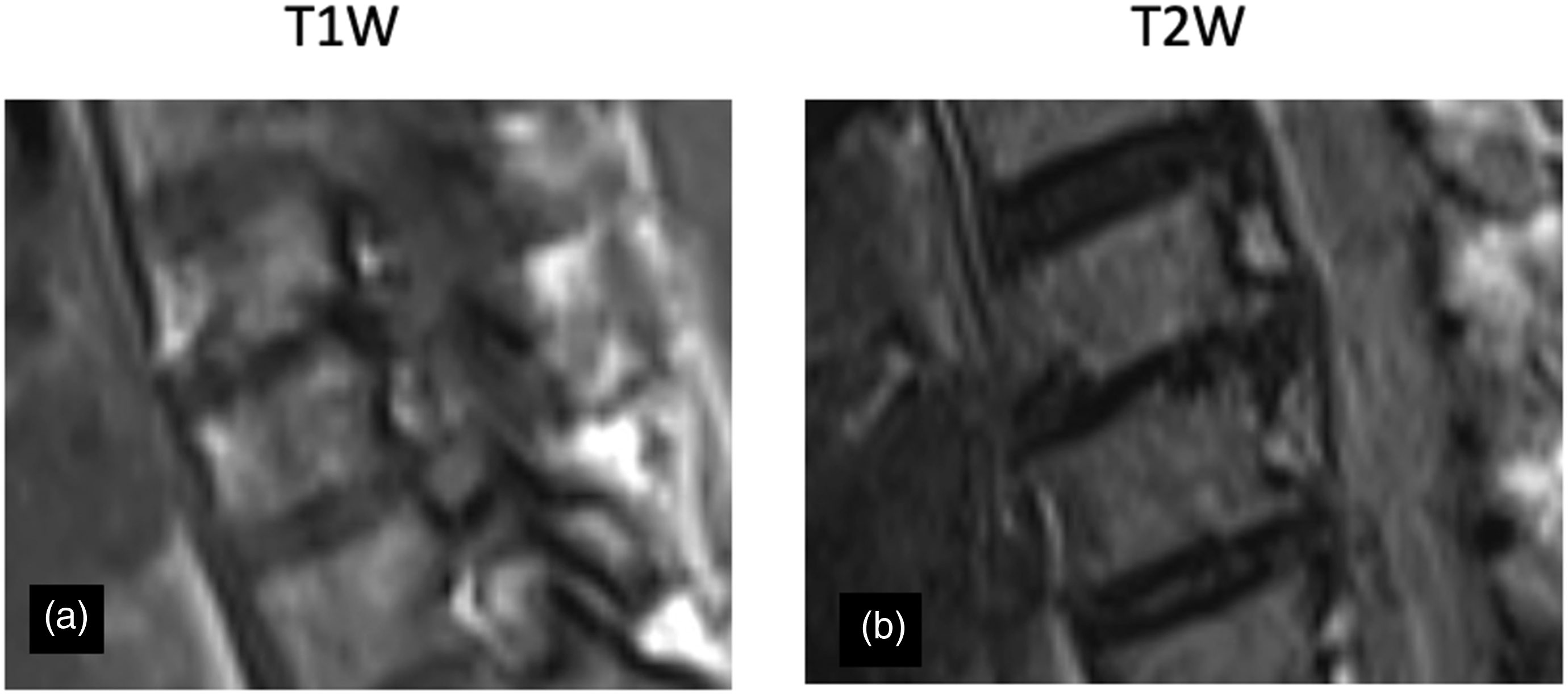
Among the 301 in the neck pain group disc herniation (H+) alone was present in 169 (56.14%), DEBC alone in 127 (42.2%), and both together in 42 (13.95%) (Figure 2). This is significantly different from the control group, where disc herniation (H+) alone was present in 31 (15.5 %), DEBC alone in 57 (28.5%) and both together in 11 (5.5%) (P < 0.05) (Table 2). Disc hyperintensity was found in 6/301 (5.32%) patients in the neck pain group and 2/200 (1%) patients in the control group (P < 0.05) (Figure 3). End-plate erosions (EPE) were found in 110/301 (36.5 %) of all neck pain patients and 30/200 (15%) controls and a variable extent in every patient with DEBC (Table 2) (Figure 4). Concordant Disc herniation with DEBC changes. (A), (B) T2W sagittal and axial image showing concordant disc herniation with DEBC changes. Disc hyperintensity. (A) T2W and (B) STIR image showing DEBC changes with disc hyperintensity. Endplate erosion: (A) T1W and (B) T2W images show endplate erosions in patients with DEBC changes.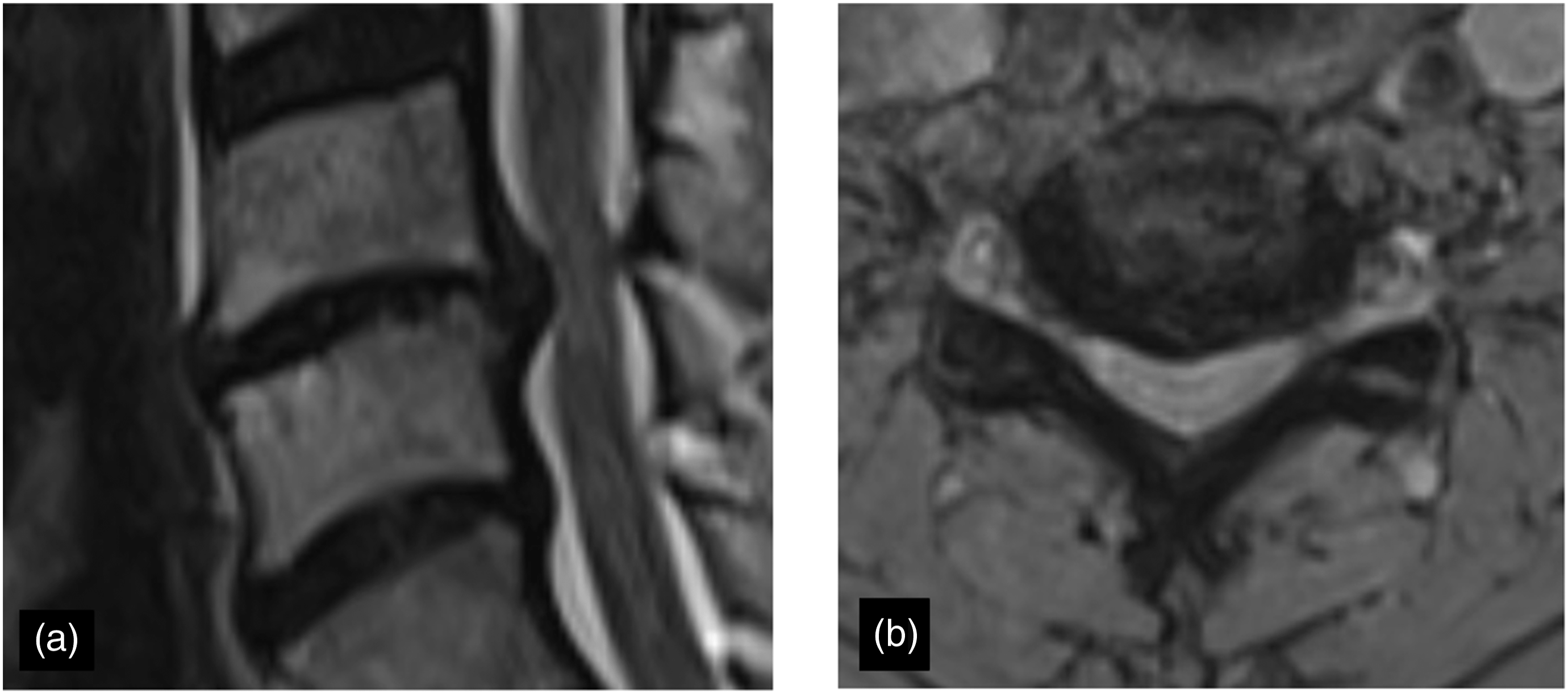
Reclassification Based on DEBC
Classic Modic description based on T1 and T2 alone had misclassified 35 EPs (20.71%) in the neck pain group and 20 EPs (29.41%) in the control group.
Among the 35 EPs in the neck pain group, 33 EPs with Type 2 MC were reclassified into Type B DEBC due to the presence of edema in STIR images and 2 EPs with Type 2 MC were reclassified due to the presence of disc hyperintensity. Whereas the 20 EPs with Type 2 MC in the control group were reclassified into Type B DEBC due to the presence of edema in STIR images (Table 2).
Odds Ratio for Surgical Management
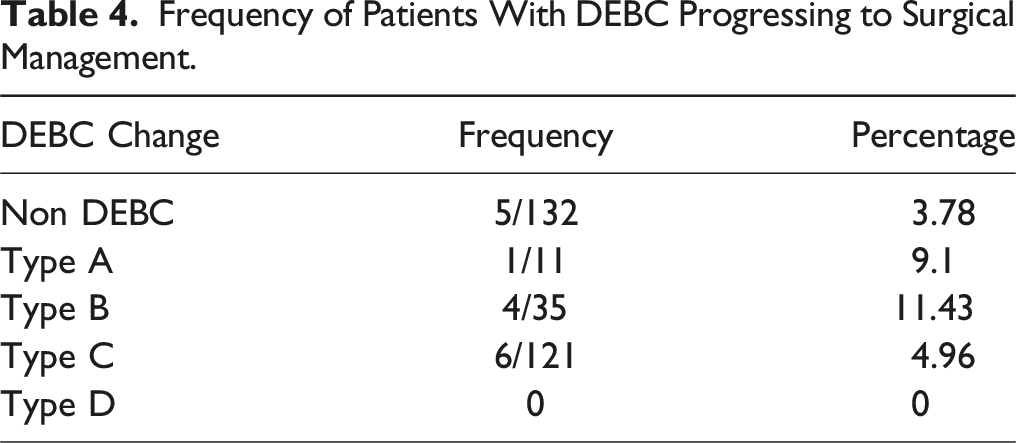
Frequency of Patients With DEBC Progressing to Surgical Management.
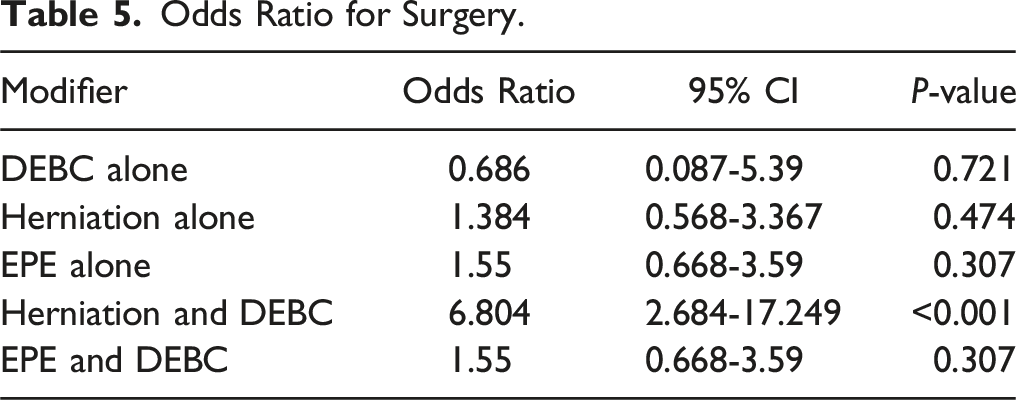
Odds Ratio for Surgery.
Discussion
The incidence of MCs in the cervical vertebrae varies from 5% to 40% and is directly related to the frequency of neck pain and disc degeneration.13-15 Hayashi et al 16 demonstrated that individuals with MCs had a higher likelihood of experiencing severe disc degeneration (DD) at the same segment level with an odd ratio of 3.9 in comparison to those without MC. 16 In addition, Matsumoto et al. found that after 10 years of monitoring 497 patients who showed no symptoms, the occurrence of MC was directly linked to different factors indicating the advancement of DD. 14 Kang et al. conducted a study on patients presenting with neck pain and found a correlation between MC (Modic changes) with severe disc herniation and reduced disc height. Furthermore, the results of the study highlighted that individuals diagnosed with MC had a higher likelihood of undergoing ACDF compared to those who did not have MC. 17 Several mechanisms explain the relationship between DD and MCs. MCs lead to the degradation of the endplates, which in turn hampers the nourishment of the disc. This is believed to expedite the degeneration process of the disc.12,18
Modic changes have been extensively studied in the literature with their correlation to clinical symptoms and clinical outcomes, however, it has their limitations.19,20 Original Modic classification is based only on T1 and T2 sequences without STIR sequences due to which it is difficult to differentiate between fat and edema. Another major drawback is that it considers the disc, end-plate, and bone marrow as separate entities, while in reality, it is a single anatomical and functional interdependent unit.12,18,21 So, abnormality in any 1 can lead to abnormality in the other. Structural endplate abnormalities refer to specific defects in the endplate, which have been associated with the occurrence of low back pain and, in certain cases, precede disc degeneration. 18 There are limited studies that have investigated anomalies in the endplates of the cervical spine. Studies by Harada et al highlighted a comprehensive description of the endplate phenotype in patients with cervical spine pathology on MRI. They found that these phenotypes are clinically significant and are associated with pain, disability, degeneration, and adverse surgical outcomes such as adjacent segment degeneration or disease.22,23
The DEBC classification, originally described for the lumbo-sacral spine further addresses the concerns by analyzing STIR images and incorporating the disc and endplate changes into the classification. This study provides further insights into the risks of patients failing conservative management and requiring surgery. In our present study, we have analysed the association between Modic changes and DEBC classification and reported its clinical implications in patients with cervical disc degeneration. Previously the importance of endplate abnormalities in the cervical spine was introduced by Baker et al who introduced the Modic-Endplate Complex (MEC) in their study which considered the importance of structural endplate abnormalities in patients undergoing ACDF procedure. 21
In our study, the DEBC classification detected edema in 33 patients (21.1%) which was previously undetected and was considered to be pure fat according to the Modic classification. Two EPs (1.28%) were reclassified from type 2 MC into type B DEBC due to disc hyperintensity. The study had high inter and intra-observer reliability, reclassifying 22.4% of EPs (P < 0.05). A similar study by Vettiyil B et al, also indicating the importance of STIR sequences in Modic classification, found that 8% of patients who underwent lumbar spine MRI had end-plate changes only on STIR. 24
Literature concerning the impact of Modic changes on treatment outcomes has been previously studied and is a topic of debate. The study by Baker et al analyzed 628 patients of whom 84 patients had MC, 166 had EPC, and 187 had a combination of both changes. Their results showed that MC and EPC commonly manifest together and in patients who underwent ACDF for a degenerative pathology, the presence of a combination of these changes resulted in an overall poor postoperative outcome. 21 This was in stark contrast to the study by Li et al reported that post-operative outcomes were independent of the presence of Modic changes, however, none of them considered endplate abnormalities. 25
While all these studies focused on postoperative outcomes, none of the studies determined the effect of end-plate and MC on the requirement of surgical intervention in patients with cervical degenerative disc disease.21,25 Our study clearly shows that the highest odds for requiring surgery in the cervical spine was the concomitant presence of H+ and DEBC with an odds ratio of 6.8 while it reduces to 1.38 in the presence of herniation only. End-plate erosions, however, demonstrated a similar odds ratio (1.5) for requiring surgery in isolation as well as in combination with DEBC changes. In our study, disc hyperintensity was seen in 1% of controls and 5.32% of neck pain patients. Disc hyper intensity led to re-classification in 2 endplates, however, the study population was insufficient to attain significance.
There are a few limitations in our study. First, it is a retrospective study with relatively a smaller sample size. Moreover, being a single-centre study, it needs to be validated at different centres with a relatively larger sample size. Moreover, it is important to note that imaging characteristics can be observed at several levels within the cervical spine, and the choice of level to focus on is subjective. Furthermore, phenotypes that manifest in different areas of the cervical spine may or may not cause symptoms, which could explain the variations in preoperative neck pain and the need for surgical management.
Conclusion
The study shows that the DEBC classification is a reliable method of classification of degenerative disease in the cervical spine. It allows for a more comprehensive understanding of degenerative changes occurring in the disc-endplate-bone marrow complex as a whole. 29.41% of patients in the controls and 20.71% in the neck pain group were re-classified to a previously undescribed ‘chronic persistence’ (Type B DEBC) group which under favourable conditions can show manifestations. The study reflects that the need for surgery is of the highest probability when H+ and DEBC occur together, indicating that disc endplate bone marrow acts as a single anatomic and functional interdependent unit.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.