
Abstract
Study Design:
Retrospective cohort.
Objective:
The objective of this study was to assess the effectiveness of the O-arm as an intraoperative imaging tool by comparing accuracy of pedicle screw placement to freehand technique.
Methods:
The study comprised a total of 1161 screws placed within the cervical (n = 187) thoracic (n = 657), or lumbar (n = 317) spinal level. A pedicle breach was determined by any measurable displacement of the screw outside of the pedicle cortex in any plane on postoperative images. Each pedicle screw was subsequently classified by its placement relative to the targeted pedicle. Statistical analysis was then performed to determine the frequency and type of pedicle screw mispositioning that occurred using the O-arm versus freehand technique.
Results:
A total of 155 cases (O-arm 84, freehand 71) involved the placement of 454 pedicle screws in the O-arm group and 707 pedicle screws in the freehand group. A pedicle breach occurred in 89 (12.6%) screws in the freehand group and 55 (12.1%) in the O-arm group (P = .811). Spinal level operated upon did not influence pedicle screw accuracy between groups (P > .05). Three screws required revision surgery between the 2 groups (O-arm 1, freehand 2, P > .05). The most frequent breach type was a lateral pedicle breach (O-arm 22/454, 4.8%; freehand 54/707, 7.6%), without a significant difference between groups (P > .05).
Conclusions:
The use of the O-arm coupled with navigation does not assure improved transpedicular screw placement accuracy when compared with the freehand technique.
Introduction
Stable fixation of spinal segments is integral to the success of a variety of spinal procedures. This can be achieved via methods such as transpedicular screw fixation, wires, hooks, interbodies, and so on, depending upon variables such as surgeon preference or procedure type. Transpedicular screw placement has been deemed biomechanically superior over other fixation devices 1 ; however, improper positioning of screws significantly increases the risk of adverse outcomes related to neural, vascular, or visceral injury. Current literature reports misposition rates ranging from 5% to 41% in the lumbar spine and 3% to 55% in the thoracic spine, 2 providing evidence for the need to enhance the accuracy of pedicle screw placement. That being said, several new medical technologies have been developed in an effort to minimize mispositioning rates and consequently improve patient outcomes.
The primary intraoperative imaging modality currently used for transpedicular screw fixation is C-arm fluoroscopy 3 ; however, it is important to note that some surgeons choose not to use imaging during screw placement. X-rays can provide a 2-dimensional (2D) view of screw placement using C-arm fluoroscopy within the operating room, but it is not until after the procedure is complete that the surgeon can obtain a 3D view of pedicle screws with a computed tomography (CT) scan. 4 This approach, defined in this study as “freehand technique,” refers to the placement of pedicle screws without intraoperative 3D visualization of the pedicle or navigation of screw placement. The O-arm Multidimensional Surgical Imaging System (Medtronic)—often coupled with the StealthStation Surgical Navigation System (Medtronic)—was developed to allow for 3D imaging within the operating suite with the intention of decreasing pedicle screw mispositioning and the frequency of correction surgeries. Current literature reveals inconsistencies in results regarding its effectiveness in enhancing pedicle screw accuracy when directly compared to freehand technique. Some studies have found that pedicle screws placed with the O-arm coupled with navigation are more accurate when compared to screw placement using freehand technique,5-8 while other studies have found no significant difference in accuracy between these 2 approaches.9-12 The authors of this study hypothesized that there would be no statistical difference in pedicle screw accuracy when directly comparing the O-arm to freehand technique.
Materials and Methods
After appropriate institutional review board approval, a cohort of patients who had spinal surgery over a 4-year period (June 2012 to May 2016) was retrospectively reviewed at a single institution. Inclusion criteria consisted of all patients who had pedicle screws placed using O-arm navigation or freehand technique in the inclusion period. Exclusion criteria included fixation without pedicle screws and use of navigation without the O-arm. This information was collected from hospital records and surgeon billing records of the 5 surgeons who performed spinal surgery at the study institution involved.
Pedicle screw placement occurred in 84 of 263 patients that underwent an operative procedure involving the O-arm and in 71 of 345 patients using freehand technique by either an orthopedic surgeon or a neurosurgeon. Cases involved the cervical (O-arm 11.6%, freehand 12.9%), thoracic (O-arm 12.3%, freehand 32.3%), and lumbar (O-arm 42.5%, freehand 25.2%) spinal levels with some procedures spanning more than 1 level. There were 3 total orthopedic surgeons and 2 total neurosurgeons involved in this study. Two surgeons solely used freehand technique and 3 surgeons solely used the O-arm, therefore perceived case difficulty or spinal level did not influence the modality used. All surgeons using the O-arm were beyond the learning period required to effectively operate the device. Reasons for surgery were classified as trauma, tumor, degeneration, infection, or “other,” if it did not fit any other categorizations (Table 1). For patients with a tumor, a pedicle screw was inserted if the tumor disrupted spinal stability. Examples of “other” classification include scoliosis, kyphosis, and lumbar radiculopathy.
Summary of Patient-Specific Characteristics, Treatment Characteristics, and Screw Placement Accuracy.
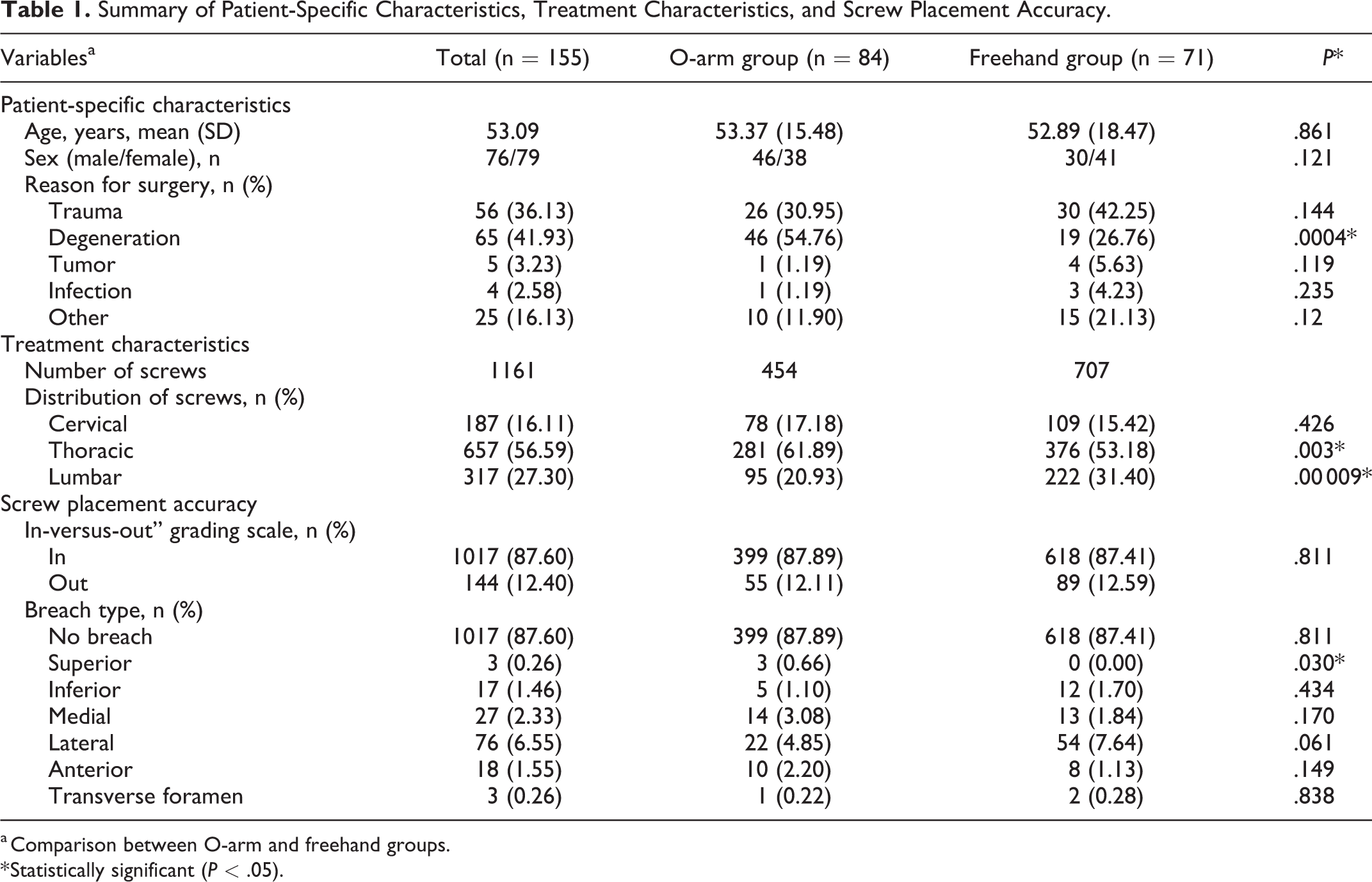
a Comparison between O-arm and freehand groups.
* Statistically significant (P < .05).
For the O-arm group, the StealthStation Surgical Navigation System (Medtronic) was used to cannulate pedicle screws based on 3D imaging obtained with an O-arm Multidimensional Surgical Imaging System (Medtronic). Patients were placed in a prone position on a radiolucent table. Access to the dorsal spinal segments was obtained using a midline approach and structures were exposed before imaging was performed. Pedicles were cannulated using a navigated pedicle finder. The pedicle was tapped under navigation and checked with a navigated ball-tipped probe before introducing the screw using a navigated screw inserter.
For the freehand group, anatomic landmarks and specific entry sites were used to guide pedicle screw insertion. Patients were placed in a prone position on a radiolucent table. As in the O-arm group, access to dorsal spinal segments was obtained using a midline approach. Anatomic landmarks were used to determine the entry point, after which a small hole was drilled into the pedicle. The pedicle was cannulated using a pedicle finder and the channel was checked with a non-navigated ball-tipped probe. Neuromonitoring was used in every surgical case within both groups. Pedicle screw stimulation was not consistently used because a number of procedures involved thoracic pedicle screws.
An independent review of all intraoperative and postoperative scans was performed by 4 authors (BDC, CMN, KAR, HMP); each scan was examined by a medical student, resident, and attending for quality control. Intraoperative and/or postoperative imaging was used for evaluation of pedicle breach depending on the approach; imaging consisted of plain film, CT scans, and magnetic resonance images when available. There was no standardized postoperative imaging protocol because of the retrospective design of this study. Postoperative CT scans were available to determine pedicle breach in each O-arm case, however due to the nature of freehand technique a CT scan was not always available for review. Placement of each screw was classified by location of pedicle breach; either superior breach, inferior breach, medial breach, lateral breach (Figure 1), anterior breach, transverse foramen breach, or no breach (Figure 2). A pedicle breach was defined using the “in-versus-out” grading scale, qualifying a breach as any measurable displacement of the screw outside of the pedicle cortex in any plane on postoperative images.
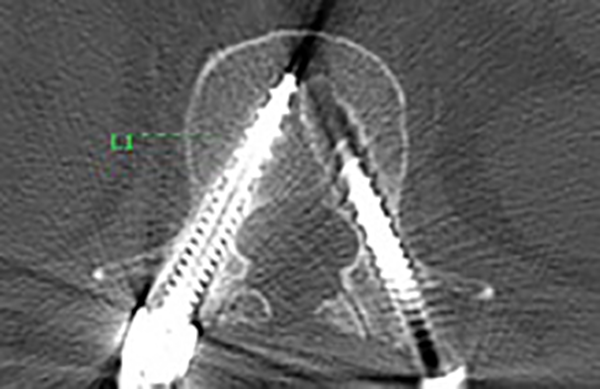
No breach of the pedicle.
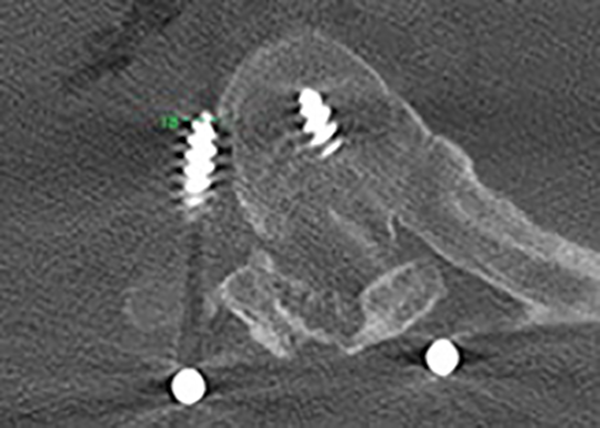
Lateral breach of the pedicle.
Data including patient-specific characteristics (age, gender, reason for surgery), treatment characteristics (number and distribution of screws), and pedicle screw accuracy (number and frequency of breaches) was collected and summarized (Table 1). Need for revision surgery was recorded and minimum follow-up was set at 1 month with final follow-up ranging from 1 month to 3.5 years. A total of 7 patients were lost to follow-up (O-arm 5, freehand 2, P > .05). There was no consistent reporting of postoperative symptoms therefore outcomes were primarily defined by the need for revision surgery.
Data was analyzed using chi-square tests for nominal data and t tests for interval-level data. Statistical significance was set at a P value of .05 and statistical analysis was performed using SPSS Version 24 (IBM Corp).
Results
A total of 155 consecutive patients (O-arm 84, freehand 71) who underwent cervical (n = 38), thoracic (n = 69), and lumbar (n = 105) instrumented procedures were retrospectively reviewed (Table 1). Among the 2 cohorts, 56 (36.1%) operations were performed for trauma, 5 (3.2%) for tumor, 65 (41.9%) for degeneration, 4 (2.6%) for infection, and 25 (16.1%) for “other.” Patient-specific characteristics (age and sex) showed no significant differences between the 2 groups (P > .05) (Table 1).
A total of 1161 screws were eligible for analysis (O-arm 454, freehand 707). These included 187 at the cervical level (O-arm 17.2%, freehand 15.4%), 657 at the thoracic level (O-arm 61.9%, freehand 53.2%), and 317 at the lumbar level (O-arm 20.9%, freehand 31.4%). Thoracic pedicle screws were more frequently placed in the O-arm group (O-arm 281/454, freehand 376/707, P = .003) and lumbar pedicle screws were more frequently placed in the freehand group (O-arm 95/454, freehand 222/707, P < .0001). The O-arm was more frequently used for degenerative pathology than freehand technique (O-arm 46/84, freehand 19/71, P < .001).
According to the “in-versus-out” grading scale, a pedicle breach occurred in 89/707 (12.6%) screws in the freehand group and 55/454 (12.1%) in the O-arm group (P = .811). The frequency of breach type among cohorts was recorded (Table 1). Spinal level operated upon did not influence pedicle screw accuracy between groups (P > .05). Despite an increased number of thoracic screws placed in the O-arm group, the overall accuracy at this level between groups was statistically insignificant (P > .05). The most frequent breach type was a lateral pedicle breach regardless of the spinal level in which the screw was placed (O-arm 22/454, 4.8%; freehand 54/707, 7.6%; P > .05). Only 1 of 454 screws in the O-arm group and 2 of 707 screws in the freehand group were symptomatic enough to warrant revision surgery (P = .838). The overall difference in the accuracy of screw placement between groups as defined using the “in-versus-out” grading scale was not found to be statistically significant (P = .811).
Discussion
Pedicle screw placement remains the standard of care for spinal fusions in the 21st century. New methods for enhancing pedicle screw accuracy are frequently being introduced because of its importance in preventing neural, vascular, and/or visceral injury to the patient. Assisted navigation with the O-arm is a technique used to enhance pedicle screw accuracy, and previous studies have shown that the O-arm improves accuracy when compared with conventional methods such as the freehand technique.5-8 However, inconsistencies in the literature make the effect of the O-arm on pedicle screw accuracy unclear.9-12 The results of this retrospective study support the authors’ hypothesis that O-arm navigation does not significantly increase pedicle screw accuracy when compared with freehand technique.
There are pertinent limitations to our study. In our retrospective analysis, a variety of surgeons at varying levels of experience and training were involved. Each surgeon either used solely freehand technique or solely O-arm navigation. This does not allow for a direct comparison of screw placement accuracy between modalities used by the same surgeon. However, the authors believe potential bias may have been introduced if surgeon choice of modality was influenced by the perceived difficulty of the case or spinal level involved, for example. Additional limitations of this study include its retrospective study design and statistically significant differences between the O-arm and freehand cohorts for patients with degenerative pathology as well as number of screws placed within the thoracic and lumbar spinal levels. It is important to note, however, that breach frequency was not affected by these differences between cohorts. Given the study limitations, surgeon choice of O-arm or freehand technique does not appear to alter rates of pedicle screw mispositioning. Urbanski et al 10 performed an analysis of 49 patients and 835 screws that found no difference in properly positioned screws between navigation and freehand groups in scoliosis surgery, with an observed increase in radiation exposure to patients in the navigation group. Kraus et al 11 analyzed 2003 screws within the thoracic or lumbar spinal regions to find no statistical difference in pedicle screw placement between 3D navigated and conventional freehand groups. These findings are congruent with our results. Notably, spinal level did not significantly influence pedicle screw accuracy between groups in our study. Few studies have directly compared the O-arm and freehand technique within the cervical levels, and several studies have shown O-arm navigation to be superior to conventional methods within the thoracic levels5-8 while ours does not. This warrants a further look into potential hidden variables that may influence the propensity for the O-arm to improve pedicle screw accuracy beyond conventional methods. Potential explanations for the discrepancies in the literature may include lack of standardization of outside modalities used to evaluate pedicle screw placement such as neuromonitoring or pedicle screw stimulation; or a lack of standardization among grading scales used to evaluate pedicle screw placement. 13 Controlling for surgeon preference may also skew results, as a surgeon who prefers freehand technique may perform equally as well as the surgeon who prefers the O-arm coupled with navigation, as previously mentioned. This conclusion supports those experienced freehand surgeons who may be reluctant to adopt O-arm navigation as they have proven to perform equally as well in our study.
Future studies that investigate additional variables that may contribute to pedicle screw accuracy would be useful to directly compare the O-arm to freehand technique. Other factors to consider may include the surgeon’s length of time in practice, level of O-arm training, procedure type/difficulty, 14 as well as factors such as deformity type and specific pathology. Better controlling for other factors may allow for better assessment regarding the effect of the O-arm on pedicle screw placement. A future study investigating the effect of O-arm training time on pedicle screw accuracy may be beneficial. It is possible that improved surgeon training with this technology would produce more reliable increases in pedicle screw accuracy that would otherwise not be seen when compared with conventional methods. 15 Our study also did not control for duration of experience with freehand technique when evaluating the possible benefit from the use of O-arm navigation, as prior studies have shown this can be a valuable tool for a training surgeon.4,16 Further consideration should also be given to assessment of radiation exposure and procedure time, as these have been shown to be significantly increased with O-arm navigation. 10 Future study of these factors may allow for a better understanding of how surgeons may benefit from the O-arm and how it can be used to improve surgeon pedicle screw accuracy and overall patient care.
Conclusions
In our retrospective review, there was no statistically significant difference in accuracy of pedicle screw placement with O-arm navigation versus freehand technique. Investigation into other factors that may influence the accuracy of O-arm and freehand technique for pedicle screw placement may be useful to better delineate how to use this technology to improve patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.