
Abstract
Objective:
Long-term administration of dienogest, which is known to have effect on bone mineral density, is frequently done in patients with endometriosis and adenomyosis, but a few studies focused on the bone mineral density changes after finishing the long-term therapy. This study aimed to reveal the factors that adversely affect lumbar bone mineral density.
Method:
Fifty-seven premenopausal women who visited our hospital were diagnosed as either endometriosis or adenomyosis, and they were treated by dienogest for more than 115 weeks (26.5 months). Based on a previous report, bone mineral density changes less than 2% was categorized as the osteopenic group (n = 30), and the others were assigned to the unchanged group (n = 27). Bone mineral density was measured at the lumbar spine using dual-energy X-ray absorptiometry. A representative ovarian reserve marker, endogenous estradiol levels, and follicle-stimulating hormone levels were measured over time and were compared between the osteopenic and unchanged groups.
Result:
Duration of dienogest intake was 59.5 months (osteopenic group) versus 57.5 months (unchanged group). These patients experienced ovarian surgeries in a similar frequency, but the ovarian reserve in osteopenic group was impaired as suggested by the decline of endogenous estradiol level during intake of dienogest compared to that of unchanged group (p = 0.0146). Endogenous follicle-stimulating hormone level between osteopenic group and unchanged group did not reach statistically significant difference, although the osteopenic group showed relatively higher level.
Conclusion:
This study might suggest that decreased ovarian reserve as judged by endogenous estradiol level is a factor that negatively affect bone mineral density, and measurement of endogenous estradiol level during intake of dienogest could have a predictive meaning of future decreased bone mineral density level.
Introduction
Dienogest is a fourth-generation progestin that is frequently used to treat endometriosis, 1 as The European Society of Human Reproduction and Embryology (ESHRE) guidelines issued in 2013 recommend using progestins in women with painful symptoms associated with endometriosis. 2 Although the guidelines recommend progestargens as one of the options for the treatment of abdominal pain, they also suggest that clinicians take different side-effect profiles of progestins into account when prescribing progestogens, as thrombosis and androgenic side effects might be irreversible. Dienogest possesses diverse physiological functions. For instance, it inhibits ovulation, estrogen production by inhibiting follicular growth and development, endometrial differentiation, endometrial cellular growth, and cytokine production. 3 Considering its mechanisms of action, dienogest is considered to be one of the most important therapeutic agents for patients with endometriosis. According to a long-term study in patients with endometriosis, menstruation resumed in 29.9 ± 11.8 days (mean value ± standard deviation) following administration of dienogest. Based on this result, continuous administration of dienogest is required to maintain its analgesic effect. However, dienogest administration has been associated with decreased bone mineral density (BMD), 4 and a recent report also suggested that the extent of decrease in BMD after 6 and 12 months was −2.2% and −2.7%, respectively. 5 It is also worth mentioning that the Japan Nurses’ Health Study, a clinical study targeting Japanese nurses, showed that the comorbidity of osteoporosis in women with endometriosis has an odds ratio of 1.89 (1.43–2.51), 6 suggesting that the BMD of patients taking dienogest should be accordingly monitored for the assessment of possible side effects, especially BMD.
In the past years, relatively few studies have assessed the detrimental effects of dienogest, while effects of long-term administration of dienogest should be appropriately evaluated. Reflecting the effect of mild ovarian suppression of dienogest, the serum estradiol concentration was significantly greater in the dienogest 2 mg/day arm, when compared to the placebo arm. 7 Thus, we aimed to investigate the association of estradiol levels in patients treated with dienogest for long periods of time. Therefore, in this study, patients undergoing prolonged treatment with dienogest for more than 115 weeks (26.5 months) were examined for lumbar BMD, and estradiol levels in these patients were also measured to investigate the relevance with BMD.
Method
Among the premenopausal patients who visited our hospital following the complaint of endometriosis or adenomyosis from January 2011 to December 2016, 57 patients taking dienogest for more than 115 weeks were retrospectively enrolled in this study. Informed consent was obtained from all participants (reference no. 0324). The following patients were excluded from the study: patients with a history of using gonadotropin-releasing hormone agonists, patients who had started taking dienogest but had a washout period that interrupted its administration and patients with endocrinological diseases that could affect bone metabolism, such as diabetes mellitus and chronic kidney disease, and patients smoking cigarettes. Of these 57 patients, a total of 12 had endometriotic cysts of ⩾2 cm in size detected by magnetic resonance imaging (MRI) or ultrasound, 32 had surgically confirmed ovarian endometriotic cysts, and 18 had uterine adenomyosis identified by MRI or ultrasound. Upon confirming the presence of these lesions, dienogest administration (2 mg/day) was initiated. BMD was measured at the lumbar spine using dual-energy X-ray absorptiometry (Discovery DXA System, Hologic, Inc., Marlborough, MA, USA). A previous report showed that the rates of change in lumbar spine BMD at weeks 24 and 52 before dienogest administration were −1.6% ± 2.4% and 1.7% ± 2.2% (mean value ± standard deviation), respectively. 4 They also reported that there was a statistically significant decrease in BMD, but a cumulative decrease was not observed upon long-term dienogest administration. 4 Based on these results and other reports, 5 the osteopenic event was defined as a final BMD measurement of less than −2% with respect to the initial BMD measurement in patients taking dienogest, and other patients were assigned to the unchanged group. The age, gravidity, parity, and period of dienogest administration in both groups were compared. Moreover, estradiol levels and follicle-stimulating hormone (FSH) levels during dienogest administration were measured every 6 months to 1 year in each participant. The median estradiol levels (chemiluminescence enzyme immunoassay (CLEIA) method) and median FSH levels (CLEIA method) were analyzed in each participant during the administration of dienogest.
Statistical analysis
The statistical analyses were performed using JMP Pro version 13 (SAS Institute Inc., Cary, NC, USA). The data were analyzed using Student’s t-test. A p-value < 0.05 was considered statistically significant.
Results
Table 1 shows demographic data of the 57 subjects. In the unchanged and osteopenic groups, the median ages at the start of dienogest administration were 42 and 40 years, respectively, and the age difference was statistically insignificant. The gravidity scores were 1 (range = 0–4) and 1 (range = 0–4) in the unchanged and osteopenic groups, respectively. The parity scores was 1 (range = 0–3) in both groups. The body mass index was 22.0 (range = 16.2–32.3) and 22.5 (range = 15.8–39.7) in the unchanged group and the osteopenic group, respectively. The periods of dienogest administration were 55 months (range = 33–94) and 62 months (range = 34–92) in the unchanged and the osteopenic groups, respectively. No significant difference was observed between the two groups.
Clinical data of participants. The clinical data of this study are shown. These data related to the bone mineral density showed no significant differences between the unchanged and osteopenic groups.
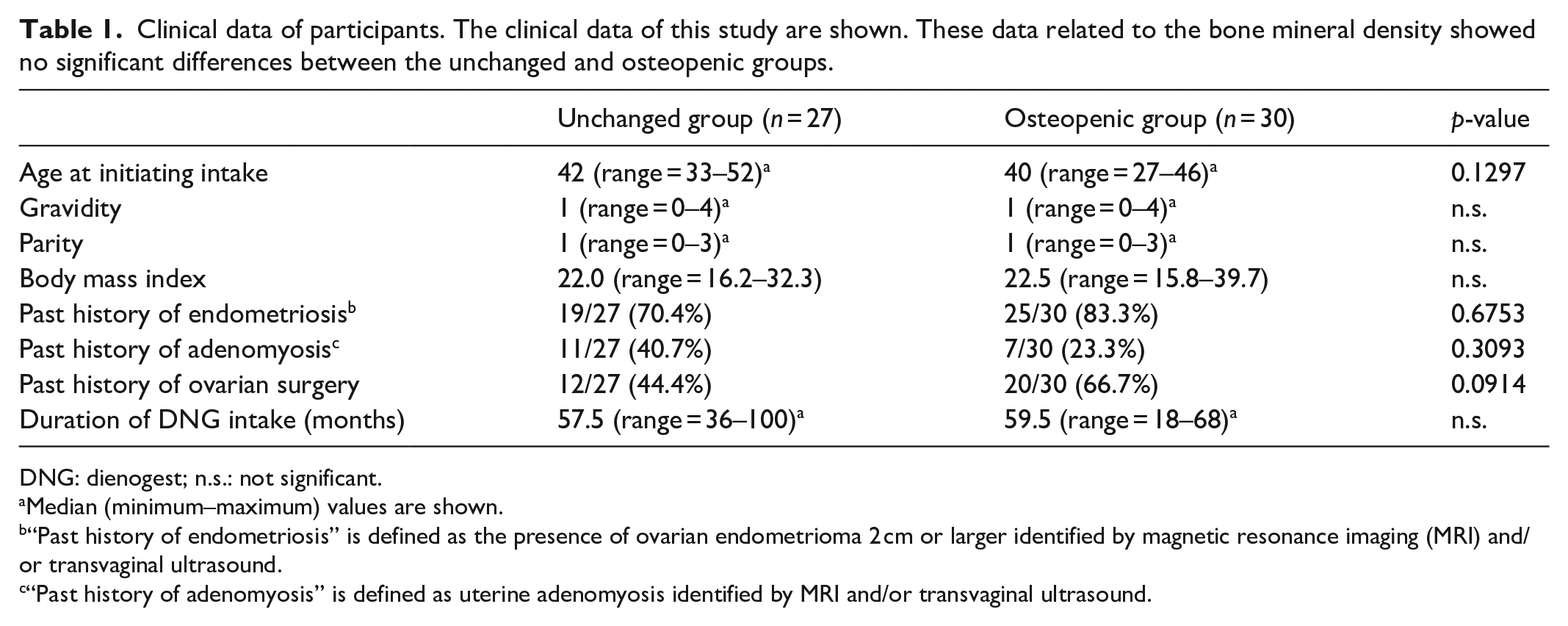
DNG: dienogest; n.s.: not significant.
Median (minimum–maximum) values are shown.
“Past history of endometriosis” is defined as the presence of ovarian endometrioma 2 cm or larger identified by magnetic resonance imaging (MRI) and/or transvaginal ultrasound.
“Past history of adenomyosis” is defined as uterine adenomyosis identified by MRI and/or transvaginal ultrasound.
Figure 1 shows the rate of time course change in BMD. The initial evaluation of BMD (g/cm2) was set to 1, and the time-dependent percent change in BMD was evaluated. In the final observation period, the number of osteopenic patients was 27 and the number of unchanged patients was 30. Figure 2(a) shows estradiol levels in the two groups. In the osteopenic group, the median estradiol value was 47.3 pg/mL (range = 20 to 175.2 pg/mL). In the unchanged group, the median estradiol value was 74 pg/mL (range = 30.2–200 pg/mL). Estradiol levels measured over time were compared between the two groups because they fluctuated, and the unchanged group had a higher estradiol level than the osteopenic group, accounting for a significant difference (p = 0.0146). Figure 2(b) presents FSH levels. In the osteopenic group, the median FSH level was 22.7 mIU/mL (range = 8.4–44.5 mIU/mL). In the unchanged group, the median FSH level was 13.8 mIU/mL (range = 6.7–35.9 mIU/mL). FSH levels between the two groups were not statistically different, although the osteopenic group showed a relatively higher value.
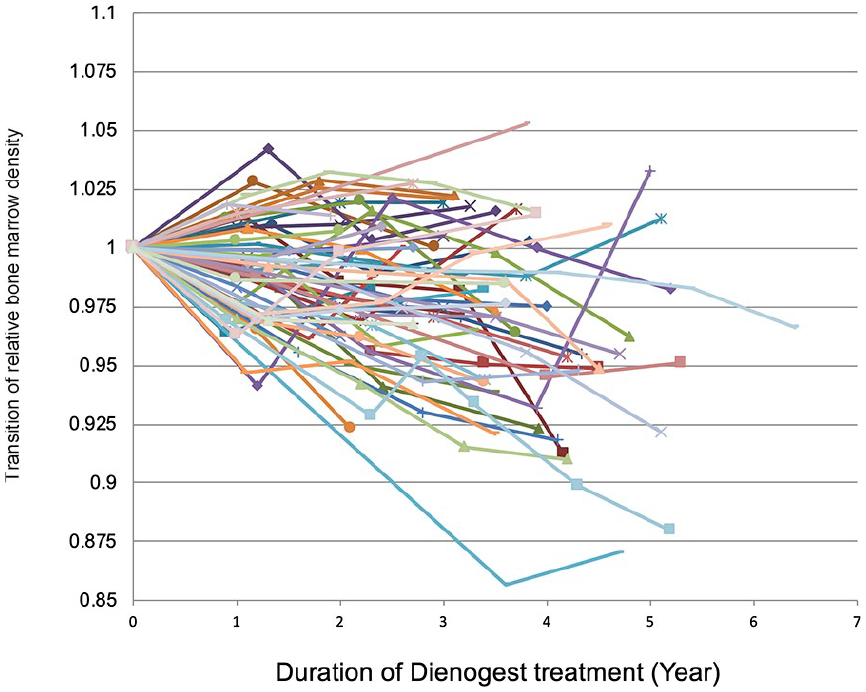
Time course change of bone mineral density. Rate of change in bone mineral density (BMD) is shown. The initial BMD (g/cm2) value judged by dual-energy X-ray absorptiometry was set to 1, and the change of each participant is shown.

Comparison of ovarian reserve marker between unchanged and osteopenic groups. (a) Estrogen levels in the osteopenic group and the unchanged group are shown. There was a significant difference between these groups. (b) Follicle-stimulating hormone levels in the osteopenic group and the unchanged group are shown.
Discussion
Results of this study indicate that long-term administration of dienogest for more than 115 weeks is associated with a considerable individual variation in BMD levels. This study also found that estradiol levels during dienogest administration were lower in the osteopenic group than in the unchanged group. Furthermore, the division point of the BMD reduction rate was set to 2%.4,5 It has been reported that the lumbar vertebral BMD in Japanese women decreases to approximately 98% from the ages 44 to 49 years old and 90%–92% from the ages 50 to 54 years old, assuming that Japanese women aged 20–44 years have a lumbar vertebral BMD of 100%. 8 The 2% reduction rate over 5 years, which is a natural reduction rate in BMD from ages 45 to 49 years, is considered the division between the unchanged group and the osteopenic group. In line with this fact, considering that the median ages at the start of dienogest administration were 42 and 40 years in the unchanged and osteopenic groups, respectively, the natural reduction rate in the study groups should be lower. Hence, it is possible that this grouping does not exclude the effect of the natural reduction rate of BMD.
This study is not free from certain limitations. This study is a retrospective analysis and sample size calculation was not done. We believe that a more detailed analysis of age-dependent effects of oral dienogest intake should be evaluated. In addition, in this study, both patients with and without a history of ovarian surgery were included, which means that the state of the ovaries before the start of the oral administration of dienogest may have affected the estradiol levels. Although estradiol and FSH levels are regarded as possible ovarian reserve markers, 9 it is desirable to examine anti-Müllerian hormone (AMH) levels as it is a better marker for predicting future BMD decline. Recently, a meta-analysis showed that the presence of endometriotic ovarian cysts significantly lowers the AMH level, which is an ovarian reserve marker, compared to other cysts or cases without ovarian lesions. 10 This suggests that ovarian surgery or the presence of endometriosis in the ovaries increases the risk of diminished ovarian function. In this study, there was no significant difference in the frequency of ovarian surgery between the osteopenic group and the unchanged group (data not shown). However, to maintain BMD, it is important to determine the ovarian reserve before and after the ovarian surgery prior to dienogest administration.
This study suggests a new modification of the treatment of endometriosis. Namely, the addition of a small amount of estrogen could reduce the effectiveness of dienogest. We have shown that stromal cells obtained from ovarian endometriosis lesions respond to vitamin D administration and suppress the inflammatory response. 11 The use of vitamin D as an adjunctive after surgery for endometriotic ovarian cysts can be considered beneficial not only for preventing recurrence but also for maintaining healthy bone mass. However, this hypothesis requires further clinical studies.
Long-term use of dienogest suggested that dienogest administration dramatically improved the quality of life of women with endometriosis, which persisted for as long as 12–24 weeks. 3 Moreover, in that study, individual patients experienced positive effects of dienogest, such as pain reduction, and expressed their desire to continue with the treatment, resulting in a long-term use of dienogest for 115 weeks or longer. Ota et al. 12 reported that dienogest was postoperatively administered in 568 patients with endometriosis, and an evident decrease in BMD was observed in 4% of patients in the span of 5 years. This result is consistent with the results of this study, that is, that the long-term use of dienogest affected the BMD in both the osteopenic and unchanged groups. While the effect of dienogest on BMD should be evaluated, we also believe that dienogest is a drug that can be used for a long period of time, spanning over several years. When examining the effects of the long-term administration of dienogest on BMD, obtaining several measurements of estradiol levels is considered beneficial in preventing the decrease of BMD at an early stage in individual cases. In addition, we found that the FSH level cannot be used as a reference value as it varies significantly from individual to individual. This may reflect the fact that FSH levels fluctuate, especially during the menopausal transition period. 10
Conclusion
This study suggests that adding a small amount of estrogen according to the estradiol level of an individual patient may be beneficial for patients who require long-term use of dienogest. Furthermore, we believe that it is also beneficial to simultaneously take dienogest and other medicines/supplements, such as vitamin D, that potentially treat endometriosis and have a positive effect on bone metabolism. Finally, this analysis was not able to identify patients who are at risk of acquiring diseases as a result of decreased BMD. Hence, this problem requires further investigation.
Footnotes
Acknowledgements
The authors thank Editage for English language editing (TGOLK_1).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the University of Tokyo Hospital Institutional Review Board (approval no. 0324).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Science and Culture (grant no. 18k09248), the Japan Agency for Medical Research and Development (grant nos 17gk0110014h0002 and 18k0210018h0001), and the Ministry of Health, Labor and Welfare.
Informed consent
Written informed consent was obtained from all subjects before the study.