
Abstract
Study Design:
Retrospective cohort study.
Objective:
To (1) define utilization trends for navigated instrumented posterior lumbar fusion (PLF), (2) compare reasons and rates of revision at 30-day, 60-day, 90-day, and 1-year follow-up, and (3) compare 90-day perioperative complications between navigated versus conventional instrumented PLF.
Methods:
Patients who underwent navigated or conventional instrumented PLF were identified from the Humana insurance database using the PearlDiver Patient Records between 2007-2017. Usage of navigation was characterized. Patient demographics and operative characteristics (number of levels fused, interbody usage) were compared between the 2 treatment groups. Propensity score matching was done and comparisons were made for revision rates at different follow-up periods (categorized by reasons) and other 90-day perioperative complications.
Results:
This study included 1,648 navigated and 23 429 conventional instrumented PLF. Navigated cases increased over the years studied to approximately 10% in 2017. Statistical analysis after propensity score matching revealed significantly lower rates of hardware-related revision at 90-day follow-up in the navigated cohort (0.49% versus 1.15%, P = .033). At 1-year follow-up, the navigated cohort continued to have significantly lower rates of hardware-related revision (1.70% versus 2.73%, P = .044) as well as all cause revision (2.67% versus 4.00%, P = .032). There were no statistical differences between the 2 cohorts in any of the 90-day perioperative complications studied, such as cellulitis and blood transfusion (P > .05 for all).
Conclusions:
These findings suggest that navigation is associated with reductions in hardware-related revisions after instrumented PLF. However, these results should be interpreted cautiously in the setting of potential confounding by other unmeasured variables.
Keywords
Introduction
The use of intraoperative navigation in spine surgery is increasing, and is now being utilized in approximately 10 percent of all procedures.1,2 Navigation offers improved three-dimensional conceptualization of anatomic structures and allows the surgeon to track placement of surgical instruments and implants in real-time, theoretically improving pedicle screw accuracy and sizing. 3 An additional advantage of navigation in spine surgery includes decreased radiation exposure for the surgical team by eliminating the need for intraoperative fluoroscopy.1,4-6 However, the use of navigation carries additional institutional costs to procure and maintain specialized equipment, requires additional technical expertise from the surgeon and operating room staff, and exposes the patient to additional radiation when compared to conventional procedures.7,8
Although navigation has been shown to improve accuracy of pedicle screw placement, 6 the impact of these improvements on clinical outcomes remains unclear. Although some studies have demonstrated no difference in overall perioperative complications between navigated and conventional lumbar fusion,1,9 others have demonstrated differences in specific medical complications such as rates of postoperative blood transfusion.1,9,10 Of particular interest is the effect of navigation on subsequent hardware-related revision after posterior lumbar fusion (PLF). While some studies have reported decreased rates of revision with use of navigated techniques,7,11 others have shown no difference. 9
Previous reports comparing revision rates between navigated and conventional PLF have largely been single institution studies,7,11 which may lack statistical power or fail to categorize reoperation into distinct causes such as hardware failure or malplacement, infection, or fracture. 9 Therefore, the aims of the current study were to 1) define contemporary utilization trends for navigated instrumented PLF; 2) compare reasons for and rates of revision at 30-day, 60-day, 90-day, and 1-year follow-up; and 3) compare 90-day perioperative complications between navigated versus conventional instrumented PLF.
Methods
Patient Population
A retrospective cohort analysis was performed using the Humana national insurance dataset within the PearlDiver database (PearlDiver Technologies Inc, Colorado Springs, CO), which contains records for over 50 million patients, from 2007-2017. The database contains hospital and physician billing records in the form of Current Procedural Technology (CPT) and International Classification of Diseases (ICD) 9th and 10th Edition codes. Procedures were identified using CPT codes while diagnoses were identified using ICD codes. Our institutional review board granted an exemption for studies using this dataset since all data is de-identified and anonymous. Patient consent was not obtained since all data is de-identified and anonymous. PearlDiver does not allow reporting of parameters with less than 11 patients and does not provide specific numerical values for parameters with less than 11 patients. This is done to preserve patient privacy.
Patients who underwent PLF were identified using the following Current Procedural Terminology (CPT) codes: 22 612, 22 630, and 22 633. One-level instrumentation cases were identified using the CPT code 22 840 while 2-5 level instrumentation cases were identified using the CPT code 22 842. Interbody usage was identified with the CPT codes: 22 630 and 22 633. Computer-assisted navigation cases were categorized using the following CPT codes: 61 783, 20 985, 0054 T, 0055 T, 61 795, 20 986, 20 987. Cases involving simultaneous anterior or lateral approaches were excluded as were cases with diagnoses of trauma, fracture, infection, or neoplasia. From this subset, individuals were excluded if they did not have 1-year follow up or were less than 18 years of age.
Patient demographic and operative characteristics were collected, including age, gender, Charlson Comorbidity Index (CCI), obesity (body mass index (BMI) > 30), interbody usage, and number of levels fused. Selection of these patient demographic and operative characteristics as potential confounding variables was based upon prior published work on a similar topic. 1
Rate and Reason for Revision
The primary outcome of the current study was the rate of revision at 30-day, 60-day, 90-day, and 1-year follow-up. The occurrence of a revision was identified through the following CPT codes: 22 830, 22 849, 22 850, and 22 852. 12 Rate of revision was categorized based on ICD codes associated with the patient’s chart during time of revision (Online Appendix 1). The various reasons for revision identified included hardware issues, postlaminectomy syndrome, pseudoarthrosis, fracture, infection, or hematoma.
Other Perioperative Complications
Secondary outcomes include the incidence of various 90-day complications, which were selected based upon previous work. 13 These complications include arrhythmia with atrial fibrillation, urinary tract infection, anemia, arrhythmia without atrial fibrillation, heart failure, renal failure, cellulitis, pneumonia, myocardial infarction, respiratory complication, sepsis, deep vein thrombosis, stroke, blood transfusion, pulmonary embolism, death, and bleeding complication. These complications are listed in Table 1. All outcomes were identified with either CPT or ICD codes outlined previously. 13
Demographics of Patients Undergoing Navigated or Conventional Instrumented Posterior Lumbar Fusion.
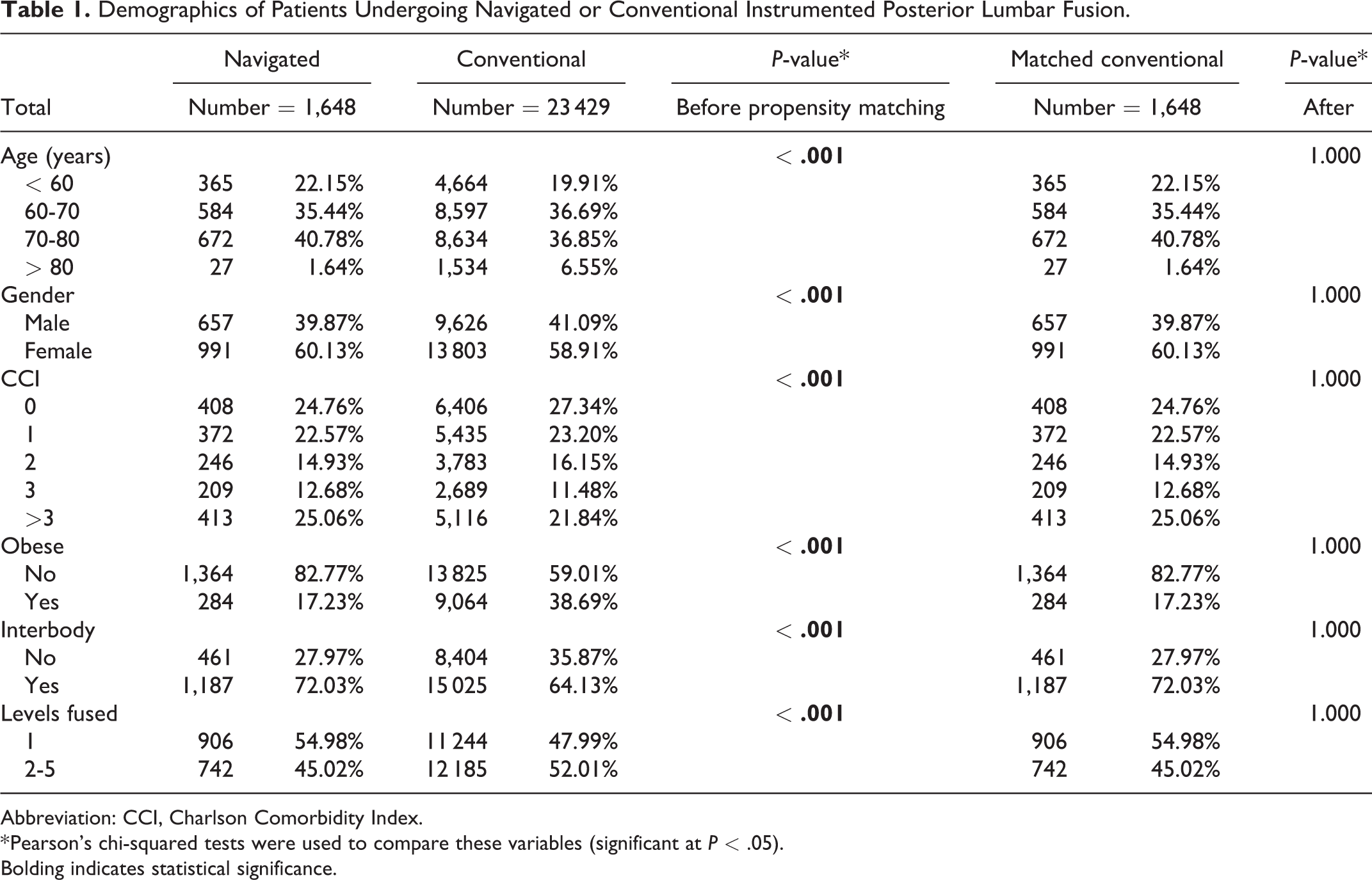
Abbreviation: CCI, Charlson Comorbidity Index.
* Pearson’s chi-squared tests were used to compare these variables (significant at P < .05).
Bolding indicates statistical significance.
Statistical Analysis
Unadjusted analysis
Data on patient demographics, comorbidities, and operative characteristics underwent univariate analysis using R software provided by PearlDiver. Univariate analysis was conducted using chi-squared testing. Statistical comparisons were conducted using the navigated group against the conventional control group. A P-value of < .05 was used as the cutoff for significance for univariate analysis.
Propensity score matching
For the second set of statistical analyzes, propensity score matching, utilizing the nearest neighbor algorithm, was utilized in order to control for potential confounding variables. 14 By creating a single score that is calculated based on covariate data, propensity scoring allows for patient mating from different treatment cohorts and accounts for potential nonrandom assignment of patients between the navigated and conventional instrumented PLF cases. 14 In the current study, each navigated case was matched with 1 conventional case with regard to age, gender, CCI, obesity, interbody usage, and levels fused. Propensity score matching is commonly used to create matched cohorts for comparison of orthopedic procedures.15-18 Propensity score matching was conducted using R software provided by PearlDiver.
After the navigated and conventional cohorts were matched with propensity scores, patient demographics, comorbidities, operative characteristics, revision rates by time of the aforementioned follow-up periods, and 90-day perioperative complications were compared between the navigated and matched conventional cohorts. Chi-squared tests were again used for categorical variables.
Results
Patient Population
A total of 25 077 patients who underwent navigated or conventional instrumented PLF were identified for analysis based on the inclusion/exclusion criteria. Of these cases, 1,648 (6.57%) were navigated procedures while 23 429 (93.43%) were conventional procedures (Table 2). The use of navigation tended to increase by year, and was ultimately utilized in nearly 10% of instrumented PLF performed by the later years of the study (Figure 1).
Matched Comparisons of Revision Rates Between Patients Who Underwent Navigated or Conventional Instrumented Posterior Lumbar Fusion.
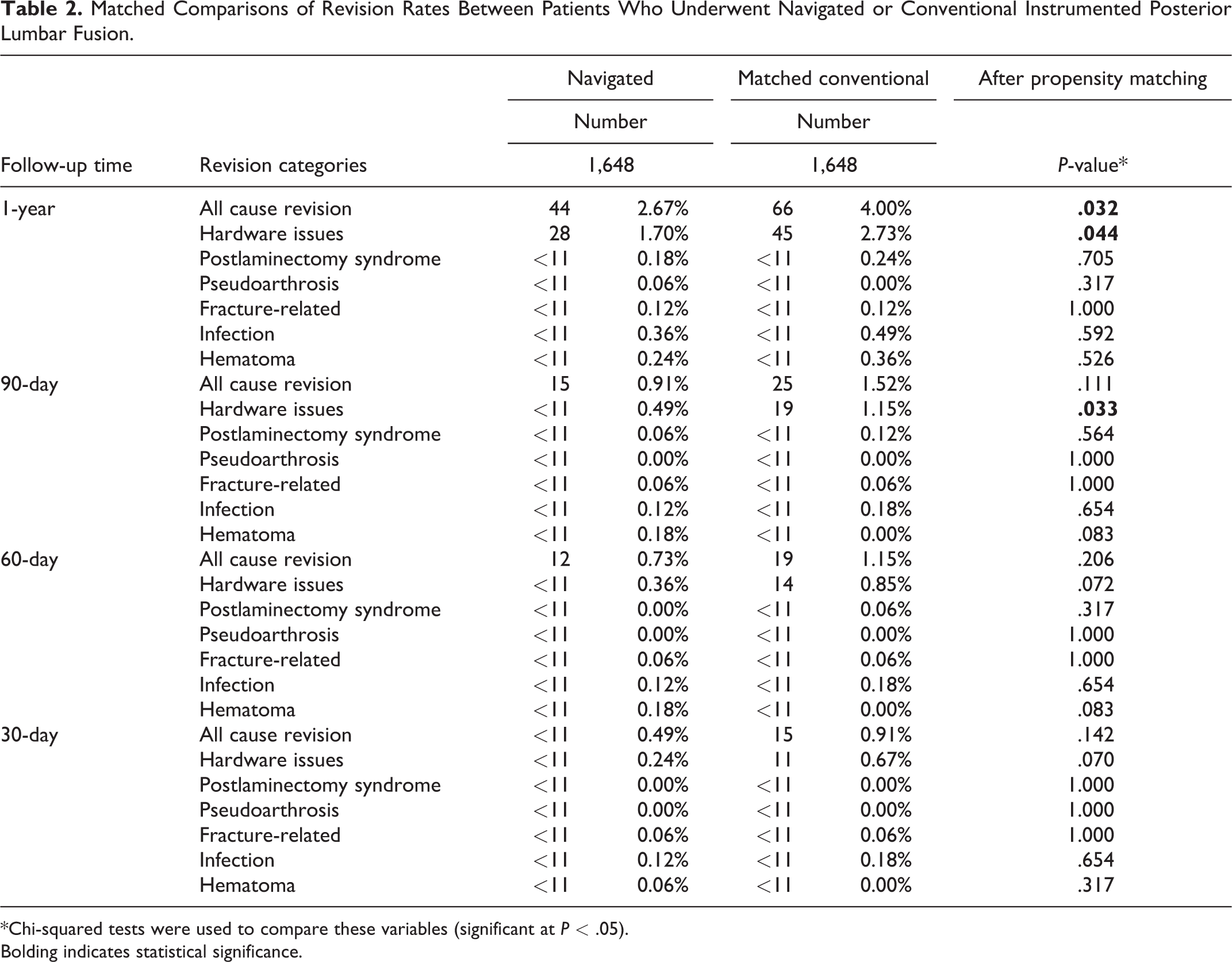
*Chi-squared tests were used to compare these variables (significant at P < .05).
Bolding indicates statistical significance.
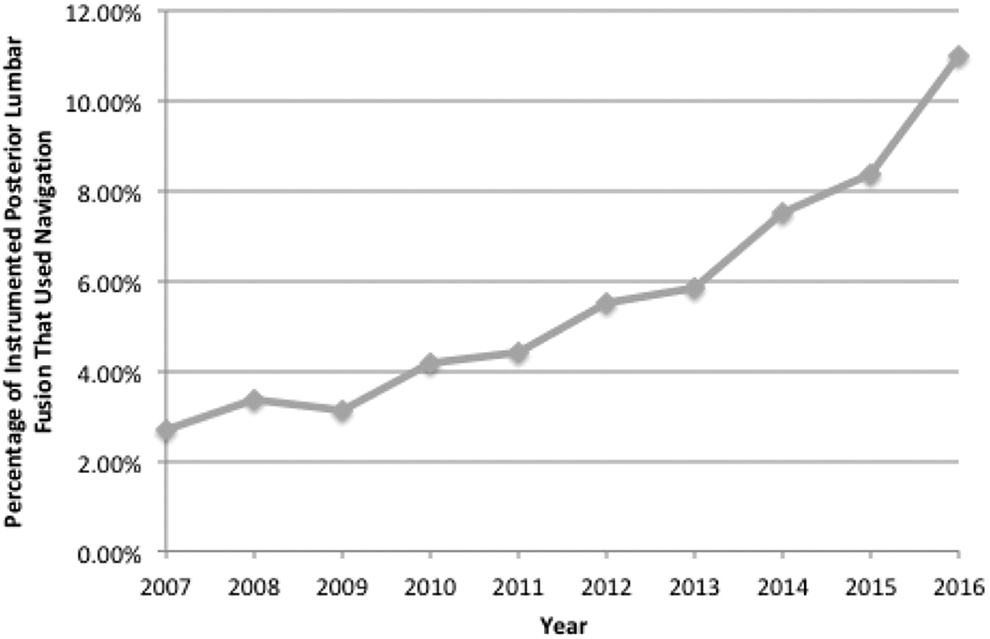
Graph showing the use of navigation for instrumented posterior lumbar fusions over the years studied.
Patients who underwent navigated PLF tended to be younger, female, had a lower BMI, and a greater proportion had CCI > 3 (P < .05). In terms of operative characteristics, use of an interbody graft and single-level fusions were more common in the navigated cohort (P < .05). Subsequent propensity score matching controlled for all significant differences in patient demographics, comorbidities, and operative characteristics between the 2 groups (P > .05 for all) (Table 2).
Rate and Reason for Revision
There were no statistical differences in revision rates at 30-day and 60-day follow-up between the matched navigated and conventional cohorts (P > .05). However, at 90-day follow-up, the navigated cohort had significantly lower rates of hardware-related revision compared to the conventional cohort (0.49% versus 1.15%, P = .033) (Table 3). This trend continued with the navigated cohort demonstrating lower rates of hardware-related revision (1.70% versus 2.73%, P = .044) as well as all cause revision (2.67% versus 4.00%, P = .032) by 1 year follow-up (Table 3). No other causes of revision were statistically different between the 2 treatment groups at any of the studied follow-up periods including infection (P > .05) (Table 3).
Matched Comparisons of Postoperative Adverse Event Rates Between Patients Who Underwent Navigated or Conventional Instrumented Posterior Lumbar Fusion.
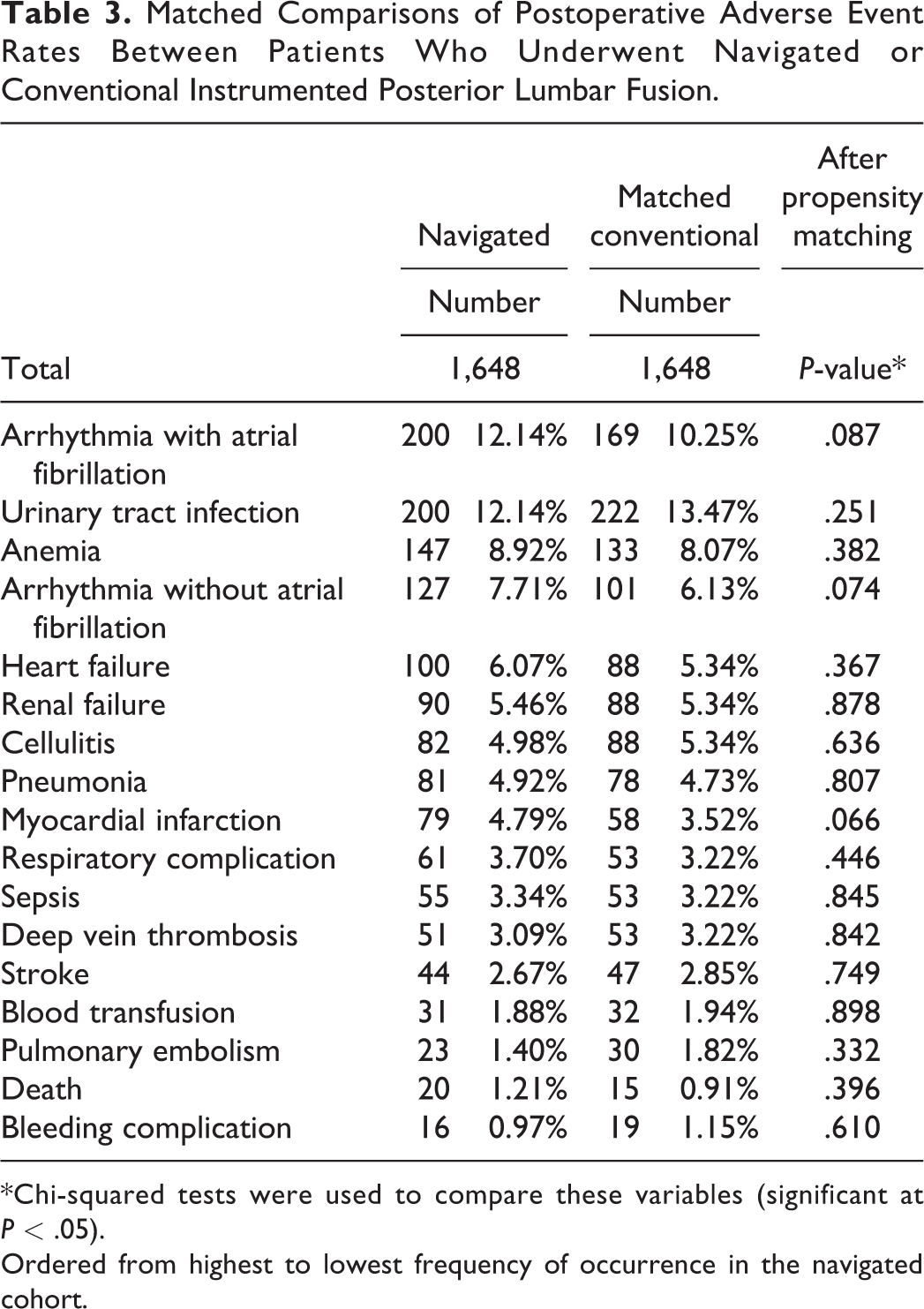
*Chi-squared tests were used to compare these variables (significant at P < .05).
Ordered from highest to lowest frequency of occurrence in the navigated cohort.
In terms of absolute number of hardware-related revisions, in the navigated group, number of hardware-related revisions at 90-day follow-up was <11 and at 1-year follow-up was 28. In the conventional group, number of hardware-related revisions at 90-day follow-up was 19 and at 1-year follow-up was 45. This highlights the importance of beyond 90-day follow-up data.
Other Perioperative Complications
After propensity score matching, there were no statistical differences between any of the studied 90-day complications including anemia, cellulitis, sepsis, deep vein thrombosis, or blood transfusion between the 2 treatment groups (P > .05 for all) (Table 1).
Discussion
Several previous studies have demonstrated that navigation results in significant improvement in accuracy of pedicle screw placement compared to conventional approaches. 6 However, data concerning whether this improved accuracy translates to differences in hardware-related reoperation following PLF is limited. While some studies have examined short-term complication and revision rates, they were limited by their small sample sizes or failed to address the specific indication for reoperation.7,9,11 The current study demonstrates that navigation is associated with significant reductions in the rates of hardware-related revisions after instrumented PLF at both 90-day and 1-year follow-up.
In terms of utilization, the current study showed that the incidence of navigated PLF is increasing annually and comprised approximately 10% of all instrumented PLFs by 2017, a number consistent with those reported by previous studies.1,2,9 Notably, however, the use of computer-assisted navigation is not adopted universally. In a worldwide cross-sectional survey, Hartl et al identified characteristics including neurosurgical training and having a high-volume practice as reasons that surgeons use navigation. Unfamiliarity with navigation or inadequate training, lack of access, and high associated costs were reasons why surgeons preferred freehand pedicle screw techniques. 2 Noting these differences in utilization between individual surgeons and institutions, large-scale databases studies may help to capture the differences in clinical outcomes between navigated and conventional PLF which may not be captured in a single-center study where 1 approach is utilized more commonly than the other. In addition, it is worth noting that in the current study, navigation tended to be utilized more in single-level cases with an interbody compared to conventional cases. This finding may be due to the fact that navigation is often utilized more in cases employing minimally invasive (MIS) techniques. For example, MIS transforaminal lumbar interbody fusions are increasingly being performed and often utilizes navigation. MIS approaches to spinal surgery have been increasingly popularized due to reduction of morbidity of surgery. 19 Navigation is a valuable adjunct in MIS spine surgery, as it allows for a larger area of visualization of bony and soft tissues through a smaller area of surgical dissection. 20
Looking specifically at revision rates, the current study demonstrated that computer-assisted navigation resulted in significantly lower rates of hardware-related revision at 90-day and 1-year following instrumented PLF, as well as a significantly lower rate of all-cause revision at 1-year postoperatively. This observation is concordant with findings from previous single-institution studies.7,11 In a single institution study of 1,208 patients undergoing thoracolumbar fusion, Xiao et al compared 2-year revision rates in patients undergoing fusion with O-arm-assisted navigation versus those undergoing fusions with either freehand techniques or fluoroscopic guidance. 11 Specifically, the authors noted that the navigated cohort had a significantly decreased likelihood of all cause reoperation, reoperation for hardware failure, and reoperation for screw misplacement compared to the freehand/fluoroscopic cohort. 11 Similarly, in a study of 502 patients from a single institution, Dea et al reported that the revision rate within 1 year was lower in the navigated group (0.8%) versus the conventional group (6%). 7 Further, the authors identified a significant decrease in revisions due to screw misplacement in the navigated cohort. 7 Of note, these studies were single institution studies from centers that routinely employ navigation. Thus, their results lacked overall generalizability and external validity.
However, contrary to the current study’s findings, Pendharkar et al used a large national database to conclude that there were no differences in 30-day and 90-day revision rates for navigated versus conventional lumbar fusion. 9 However, it is worth noting that the authors did not attempt to specify the indication for revision and lacked long-term follow-up. 9 In fact, the current study also initially found no differences in all-cause revision rates at 90-day follow-up between the 2 cohorts. However, after categorizing revision rates by cause, this study demonstrated significantly lower rates of hardware-related revision in the navigated cohort at the 90-day timepoint. This highlights the importance of parsing the overall revision rates into distinct categories in future studies. The categories include revisions for hardware issues, postlaminectomy syndrome, pseudoarthrosis, fracture, infection, and hematoma. Furthermore, the current study reported timepoints up to 1-year that again revealed lower rates of hardware-related revision as well as all-cause revisions in the navigated cohort.
It is worth noting that there are several preoperative, intraoperative, and postoperative factors beyond just the use of navigation that may have influenced postoperative revision rates. Although these factors were not analyzed in the current study, they include preoperative radiographic parameters, such as lordosis and pelvic measurements, as well as intraoperative characteristics, such as correction of lordosis and fusion enhancers. 21 In addition, postoperative factors such as early mobilization have also been shown to influence revision rates. Tempel et al demonstrated that high pelvic incidence and lumbar lordosis mismatch was strongly associated with the development of symptomatic adjacent level disease requiring revision after single-level transforaminal lumbar interbody fusion. 22 However, another previous study has shown that, on average, time from index posterior lumbar interbody fusion to revision for symptomatic adjacent segment disease was approximately 4.7 years. 23 Therefore, most revisions due to symptomatic adjacent segment disease may not be captured in this study. To our knowledge, there has not been a study that has attempted to directly determine any association between use of navigation and better achievement of pelvic incidence and lumbar lordosis matching. Further, in a study by Debono et al, the authors showed lower rates of 90-day revisions in patients who underwent PLF and had early postoperative mobilization, (3.7% vs 6.1%, P = .03). 24
The current study did not identify any differences in rates of hardware-related revision at 30 and 60-day follow-up. One potential reason could be that surgeons may choose to observe the patient for errant pedicle screw misplacement for an extended period of time prior to reoperation. This may be due to the fact that most breached pedicle screws are asymptomatic. Lonstein et al reported in their meta-analysis of 4790 pedicle screws a breach rate of 5.1%, with no more than 0.2% of them causing neurological symptoms. 25
Although the current study demonstrated statistically lower rates of hardware related revision at 90-day and 1-year follow-up in the navigated cohort, the absolute number of cases that required revision was still quite low. For example, at 1-year follow-up, only 44 out of 1,648 cases required revision in the navigated cohort while only 66 out of 1,648 cases required revision in the conventional cohort. Although the cost of revision is high, direct data comparing the savings for reduced revision versus costs of navigation setup/maintenance is lacking. Due to the low absolute number of cases requiring revision in either cohort, institutions may not have to adopt computer navigation solely for the purpose of reduced revision rates. However, for institutions that are already considering adopting this technology due to increasing use of MIS techniques or patient interest, reduced revision rates can certainly be included as another benefit of this new technology.
Additionally, the current study demonstrated no differences in 90-day medical complications between navigated and conventional procedures. A potential concern regarding use of navigation is a higher risk of wound infection due to the use of bulky equipment and increased staff movement within and through the operating room; however, no such associations were identified. Pendharkar et al similarly showed no differences in both 30-day and 90-day rates of medical complications between navigated and conventional cases. 9 However, some previous studies have reported a significantly lower rate of blood transfusion and overall medical complications in patients undergoing navigated procedures.1,10
The current study has several notable limitations in accordance with the use of a large database. The accuracy of databases depend on accurate and consistent coding practices across multiple sources, which is not a guarantee. 26 In addition, the population included in this database is not a random sample, and the present study’s conclusions may not be applicable to all patients undergoing PLF. However, the incidence of patients receiving navigated lumbar fusion is consistent with 2 separate large national databases and a cross-sectional survey, thus lending additional credence to the current study’s data and conclusions.1,2,9 In addition, while the present study explored revision rates as well as many specific 90-day medical complications, the database was unable to provide information on spine-specific parameters such as radiographic parameters, level of degeneration, degree of deformity, or instability. Since these spine-specific parameters were not recorded and not included in the matching process, there is the possibility that 1 cohort could have patients with more degeneration, kyphosis, or instability. Variables such as experience, volume, and training of surgeons are important to consider. Unfortunately, these variables are not included in PearlDiver and could not be analyzed. However, as this study utilizes a national sample, the effects of these variables may be averaged out and less influential. In addition, unfortunately, the PearlDiver database is unable to determine which procedures employed MIS techniques and this variable could not be controlled for. Further, unfortunately, the R software provided by PearlDiver does not allow calculation of the absolute standardized mean difference and demonstration of unbiased matching could not be performed. However, significant bias is not expected as nearest neighbor is a commonly used algorithm. In addition, the current study was only able to include up to 1-year follow-up data, as many patients in the database did not have 2-year follow-up. However, most revisions related to the index surgery should have been adequately captured within 1 year. In addition, since the number of hardware-related revisions at 90-day follow-up in the navigated cohort was <11, we are unable to use PearlDiver provided statistical software to perform paired T-tests to determine any significant increases in hardware-related revisions in the navigated cohort as a function of time. Finally, the PearlDiver database does not include granular details regarding which fusion enhancers were actually used in the procedure and these variables could not be controlled for. Despite these limitations, the present study’s large sample size and propensity score matched study design lend significant power to the conclusions.
The findings of the current study suggest that navigation is associated with reductions in the rates of hardware-related revisions after instrumented PLF. However, although propensity score matching was used, these results should be interpreted cautiously in the setting of potential confounding by other unmeasured variables, such as surgeon volume and specific navigation system. Further prospective trials are needed to establish any causality.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_21925682211019696 - Computer-Assisted Navigation Is Associated With Decreased Rates of Hardware-Related Revision After Instrumented Posterior Lumbar Fusion
Supplemental Material, sj-docx-1-gsj-10.1177_21925682211019696 for Computer-Assisted Navigation Is Associated With Decreased Rates of Hardware-Related Revision After Instrumented Posterior Lumbar Fusion by Patawut Bovonratwet, Alex Gu, Aaron Z. Chen, Andre M. Samuel, Avani S. Vaishnav, Evan D. Sheha, Catherine H. Gang and Sheeraz A. Qureshi in Global Spine Journal
Footnotes
Authors’ Note
Our institutional review board granted an exemption for studies using this dataset since all data is de-identified and anonymous. Patient consent was not obtained since all data is de-identified and anonymous.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.