
Abstract
Study Design
Retrospective cohort study.
Objectives
Investigate a composite score to evaluate the relationship between alignment proportionality and risk of distal junctional kyphosis (DJK).
Methods
84 patients with minimum 1 year follow-up were included (age = 61.1 ± 10.3 years, 64.3% women). The Cervical Score was constructed using offsets from age-adjusted normative values for sagittal vertical axis (SVA), T1 Slope (TS), and TS minus cervical lordosis (CL). Individual points were assigned based on offset with age-adjusted alignment targets and summed to generate the Cervical Score. Rates of mechanical failure (DJK revision or severe DJK [DJK> 20° and ΔDJK> 10°]) were assessed overall and based on Cervical Score. Logistical regressions assessed associations between early radiographic alignment and 1-year failure rate.
Results
Mechanical failure rate was 21.4% (N = 18), 10.7% requiring revision. By multivariate logistical regression: 3-month T1S (OR: .935), TS-CL (OR:0.882), and SVA (OR:1.015) were independent predictors of 1-year failure (all P < .05). Cervical Score ranged (−6 to 6), 37.8% of patients between −1 and 1, and 50.0% with 2 or higher. DJK patients had significantly higher Cervical Score (4.1 ± 1.3 vs .6 ± 2.2, P < .001). Patients with a score ≥3 were significantly more likely to develop a failure (71.4%) with OR of 38.55 (95%CI [7.73; 192.26]) and Nagelkerke r2 .524 (P < .001)
Conclusion
This study developed a composite alignment score predictive of mechanical failures in CD surgery. A score ≥3 at 3 months following surgery was associated with a marked increase in failure rate. The Cervical Score can be used to analyze sagittal alignment and help define realignment objectives to reduce mechanical failure.
Introduction
Adult cervical deformity (ACD), defined as the disruption of normal cervical alignment in the sagittal and/or coronal plane is a complex pathology.1,2 ACD is associated with significant disability, 3 and the relationship between cervical sagittal alignment and patient health-related quality of life outcomes has been well established in the literature. 4
While patients can have substantial benefit from surgical treatment and realignment surgery,5,6 the surgical correction of ACD remains complex, and has been associated with a high rate of post-operative complications and revisions.7,8 Mechanical failure, more specifically distal junctional kyphosis, has been of particular concern following corrective surgery for ACD, and remains a common cause of revision surgery.8,9
In the thoracolumbar deformity literature, mechanical failures and proximal junctional kyphosis have been extensively studied, with evolving prediction and prevention strategies.10,11 Post-operative alignment and its deviation from normative targets have been identified multiple times as major risk factors for proximal junction issues.12,13 In contrast to thoracolumbar deformity corrective procedures, which are more commonly vulnerable to proximal junctional issues, surgery for ACD is more susceptible to distal junctional kyphosis (DJK), the distal equivalent to PJK. Similar to PJK, several authors have demonstrated the importance of achieving appropriate sagittal alignment in DJK prevention.14,15
Inspired by recent publications in the thoracolumbar field, 12 this study aims to establish a composite score that evaluates post-operative alignment in ACD, and assess the relationship between post-operative alignment and mechanical failure.
Methods
Patient Sample
Study data was obtained from a multi-center prospective database of ACD patients undergoing surgery. Patients were enrolled at 1 of 13 institutions across the United States between 2012 and 2015. Institutional Review Board (IRB) approval at each of the 13 participating sites was obtained prior to conducting the study (IRB No. 2014-373). Informed consent was obtained from all participating patients. Inclusion criteria for the overall database were: age >18 years and presence of ACD, defined by the presence of at least one of the following: C2–C7 sagittal Cobb angle ≥10° (cervical kyphosis), C2–C7 coronal Cobb angle ≥10° (cervical scoliosis), C2–C7 sagittal vertical axis (C2–C7 SVA) ≥4 cm, and/or chin-brow vertical angle (CBVA) ≥25°. Exclusion criteria for the overall database include the presence of active infection or malignancy, an underlying neurologic pathology (e.g., Parkinson’s disease), or post-traumatic deformity. In addition to the above inclusion criteria, the present study only included patients who completed a minimum 1-year follow-up. Those with fusions extending to the pelvis were excluded from this study.
Data Collection
This was a prospective study in which baseline patient characteristic and demographic data were collected pre-operatively. Surgical data was collected at the time of the surgical intervention. Complications, including details pertaining to revision surgery, were recorded prospectively using standardized forms.
All patients had cervical and standing 36’’ postero-anterior (PA) and lateral spine radiographs at baseline and at 3-month, 6-month, and 1-year follow-up. Radiographic evaluations were performed at a central location using validated spine software. Parameters measured included classic spino-pelvic parameters, such as pelvic incidence (PI), pelvic tilt (PT), pelvic incidence minus lumbar lordosis (PI-LL), sagittal vertical axis (SVA), and T1-pelvic angle (TPA). We also measured cervical-specific parameters, including the C2–C7 coronal Cobb angle, cervical sagittal vertical axis (cSVA), T1 slope, C2 slope, and T1 slope minus cervical lordosis (TS-CL).
Post-operative alignment was measured on 3-month post-operative radiographs. For patients who underwent revision surgery prior to the 3 month follow-up timepoint, post-operative alignment was measured on pre-revision radiographs.
Mechanical failure was defined as having a revision for mechanical failure or having a radiographic DJK. Radiographic DJK was diagnosed radiographically, using the following criteria: DJK angle greater than 20° + ΔDJK angle greater than 10 compared with pre-operative baseline imaging. 16
Cervical Score Calculation
For each patient, the difference (offset) between the post-operative alignment achieved and the age-adjusted alignment target was calculated. The age-adjusted alignment targets were calculated, based on the literature using the following formulas:17-19
Each patient was then assigned a Cervical Score for mechanical failure, based on the offset between the post-operative alignment achieved and age-adjusted alignment targets on the T1S, TS-CL, and SVA. The details of the Cervical Score can be found in (Figure 1 Cervical Score calculation based on offset between alignment and age-adjusted targets.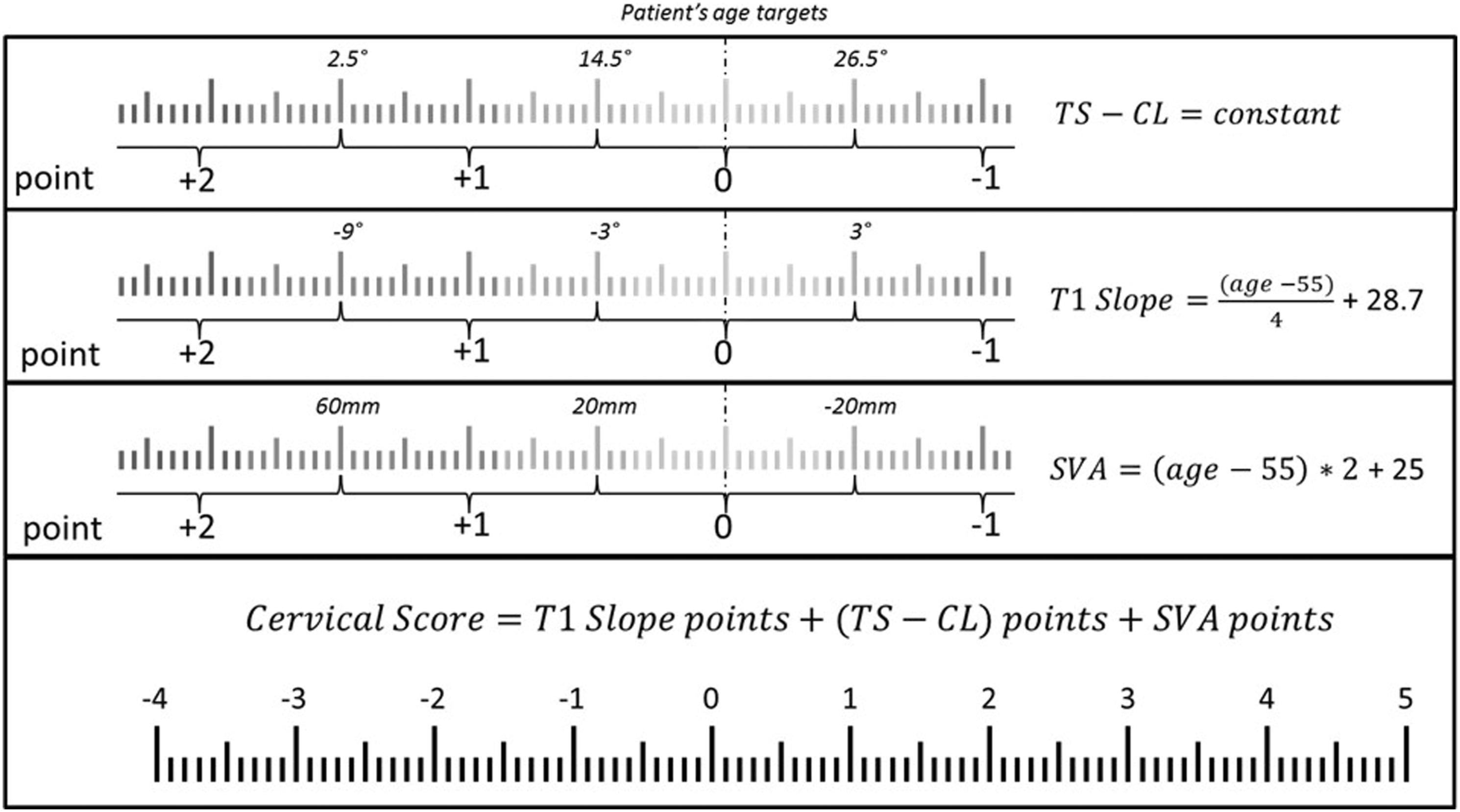
Data Analysis
Pre- to post-operative alignment was analyzed in the overall cohort using paired t-tests or Wilcoxon signed-rank tests as appropriate. Patients were divided into two groups: those who experienced mechanical failure, and those who did not. The two groups were compared regarding pre-operative alignment, post-operative alignment achieved, and the offset between post-operative alignment and age-adjusted thresholds using Mann–Whitney U test. We also analyzed the rate of mechanical failures by individual Cervical Score, and performed a cutoff analysis to assess the relative risk of failure by Cervical Score, using thresholds of 3 and 4 points. SPSS 20.0 (IBM Corp Released 2011. IBM SPSS Statistics for Windows, Armonk, NY: IBM Corp) was used for the analysis. Statistical analyses were two-sided, and P < .05 was considered statistically significant.
Results
Our database had a total of 145 patients with ACD who were eligible for 1-year follow-up; 84 patients met the specific inclusion criteria for this study. Our cohort had an average age of 61.1 years, and an average body mass index (BMI) of 28.3. A majority (64.3%) of our patients were women, and 34.5% of patients had a history of prior spine surgery. The median follow-up was 12 months.
Mechanical failure occurred in 21.4% of our cohort (n = 18), and of these patients with failure, 50% (n = 9) required revision surgery with a mean time between index surgery and revision of 145 days ±98.
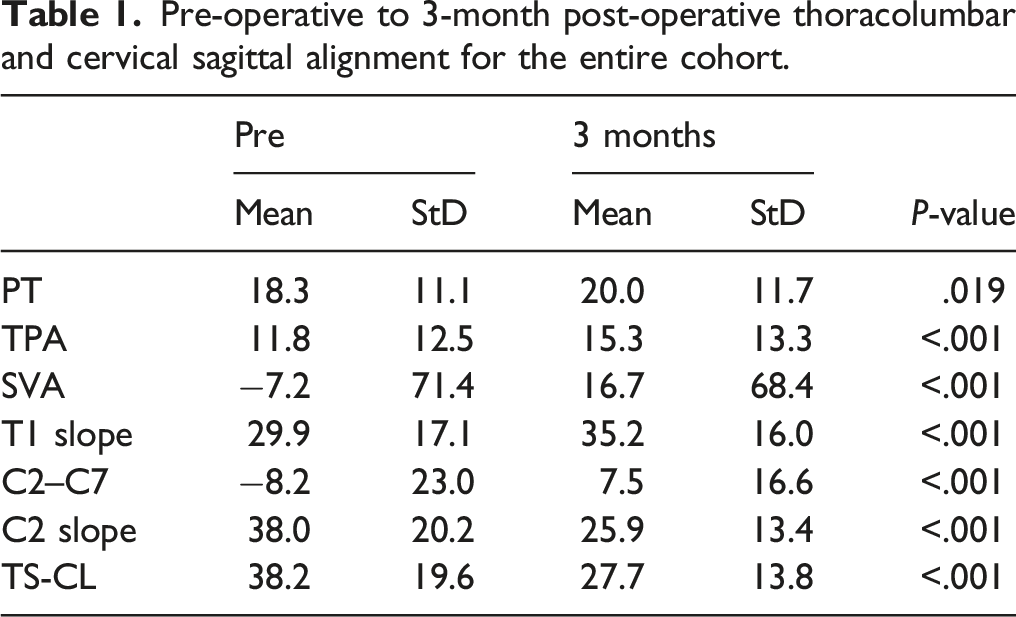
Pre-operative to 3-month post-operative thoracolumbar and cervical sagittal alignment for the entire cohort.
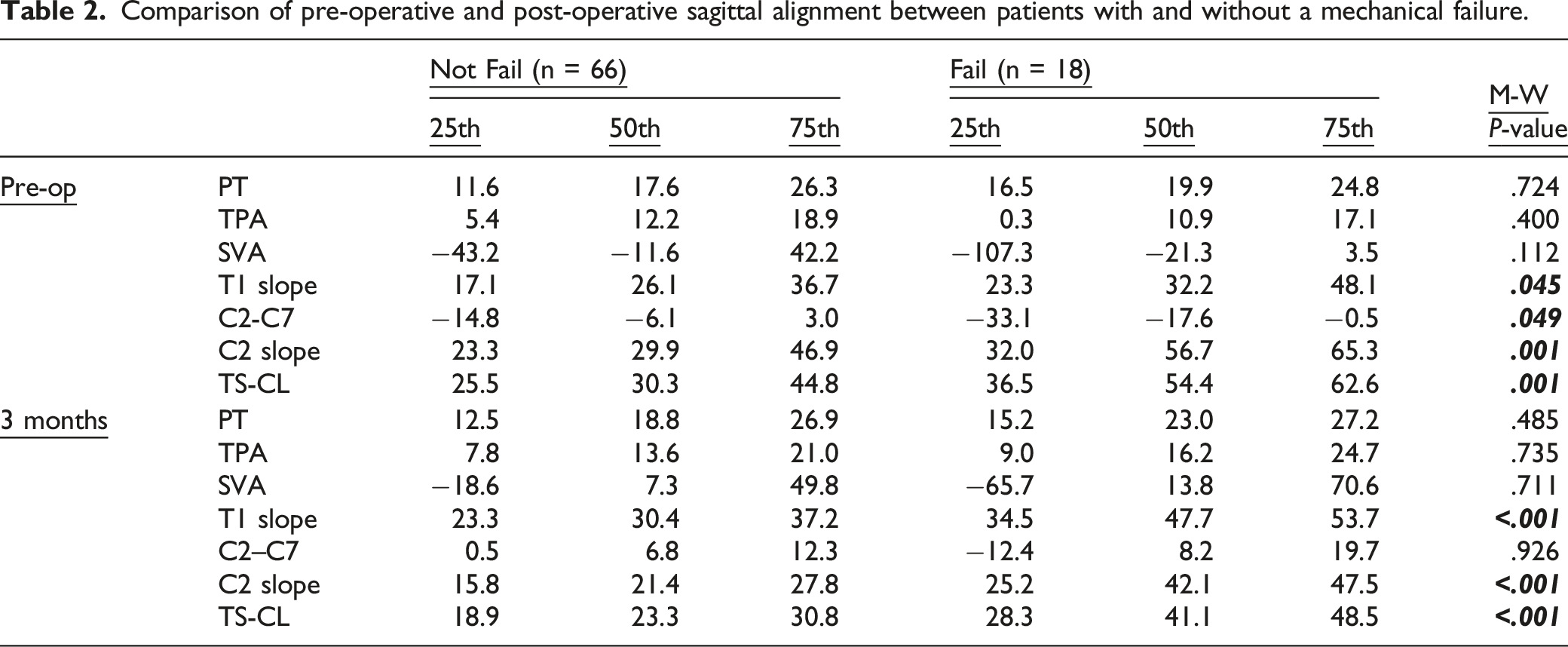
Comparison of pre-operative and post-operative sagittal alignment between patients with and without a mechanical failure.
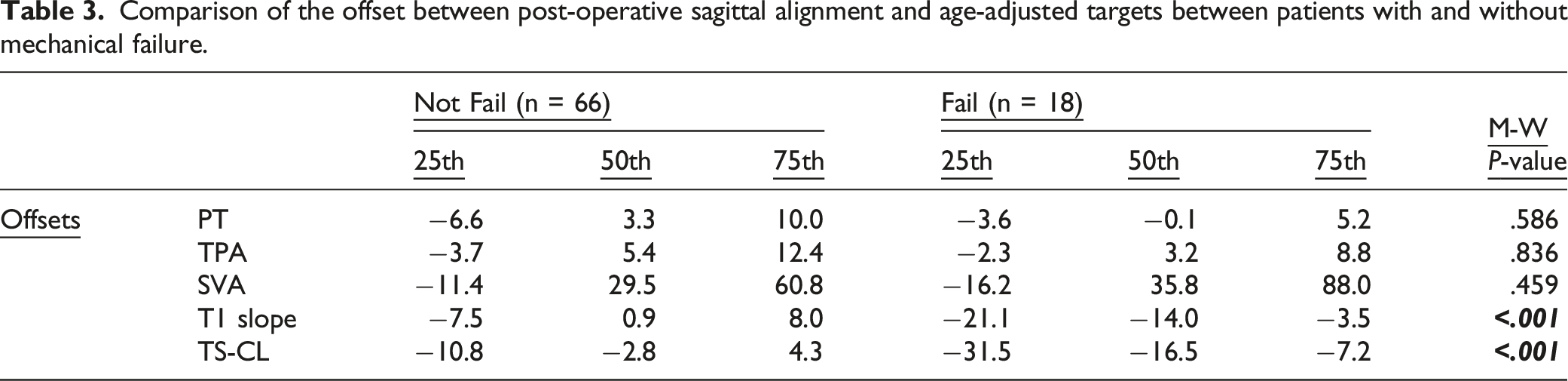
Comparison of the offset between post-operative sagittal alignment and age-adjusted targets between patients with and without mechanical failure.
The distribution of the Cervical Score for the entire cohort is illustrated in (Figure 2 Distribution of the Cervical Score for the entire study cohort.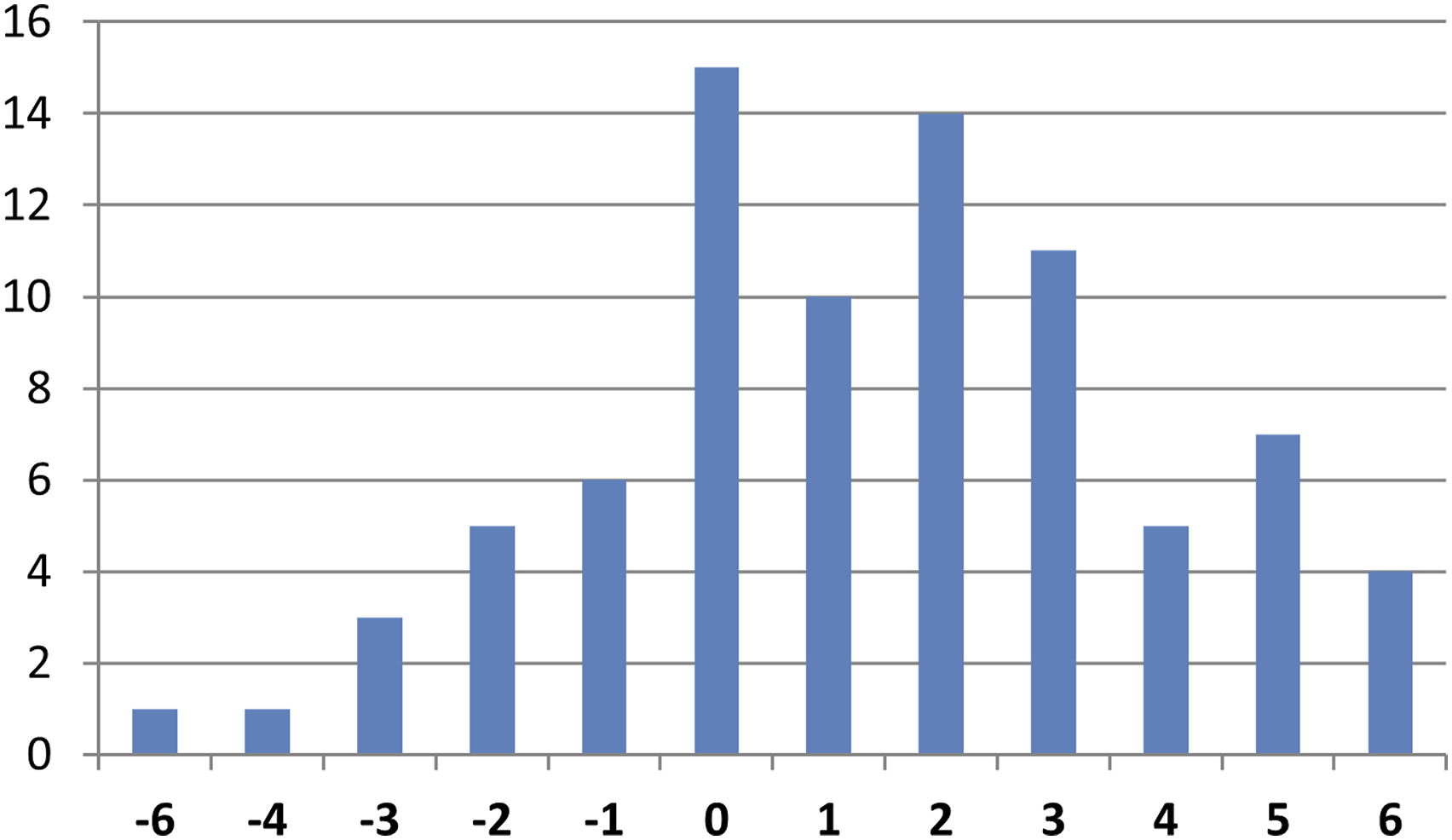
Proportion of mechanical failure for each individual Cervical Score.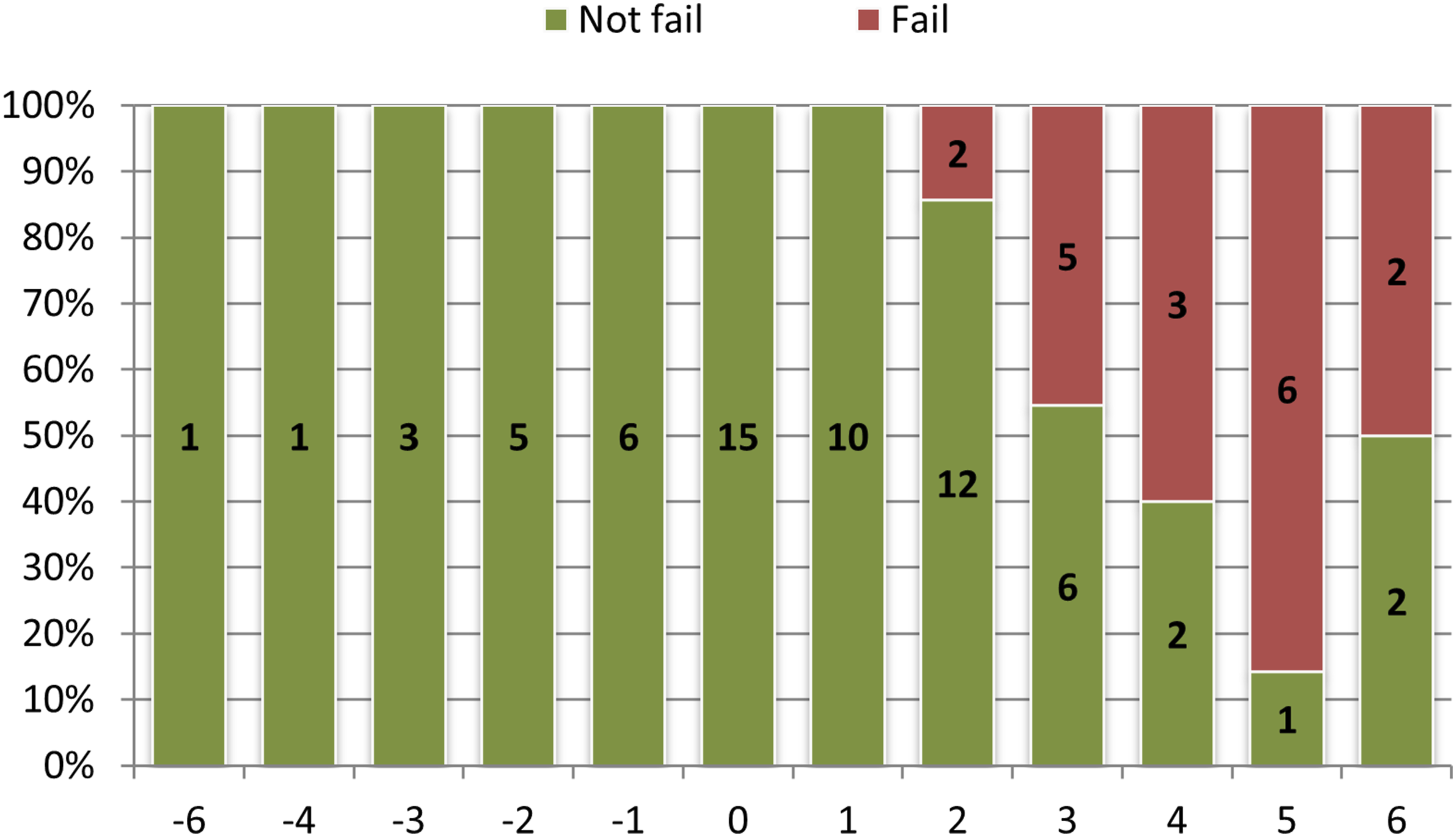
Discussion
This study focused on a cohort of ACD patients with minimum 1-year follow-up. Among our patient population, the rate of mechanical failure was 21.4%, out of which one-half underwent surgical revision. Pre-operative and post-operative cervical alignment were significantly different between patients who either did or did not develop a post-operative mechanical failure. A novel Cervical Score was developed that reflects the severity of post-operative sagittal malalignment relative to age-adjusted normative values. When applied to the 3-month post-operative imaging of ACD patients, the Cervical Score demonstrated a strong and significant association with subsequent development of mechanical failure. Patients with a Cervical Score of 3 or greater had a 35-fold greater risk of developing a mechanical issue within 1 year of surgery.
Our results show that patients who experienced mechanical failure had larger baseline deformities prior to surgical intervention. This observation has been previously noted 15 with reported thresholds of C2-C7 kyphosis greater than 12° and TS-CL greater than 36.4°. Patients presenting with the largest deformities were more likely to undergo larger corrections, increasing the risk of complications. 8 They also had greater amounts of residual deformity following surgery, when compared to their counterparts who did not experience a mechanical failure. This residual deformity can be the result of an incomplete correction, leading to increased mechanical loading at the distal junction due to gravity and a lever arm effect. 20 When combined with poor muscle quality, as previously documented in the literature, this increase in mechanical loading can lead to progressive failure. 21 This residual deformity can also be the early sign of a progressive failure. Monitoring early post-operative alignment, especially during the first several months following surgery, may allow for non-operative interventions, such as physical therapy or posture training, to help reduce the risks of needing revision surgery.
In contrast to previous reports that have assessed alignment and DJK, the present study proposes a novel Cervical Score to assess post-operative alignment. Compared to a singular radiographic parameter, this combined score allows assessment of the proportionality between parameters rather than focusing on a single aspect of alignment. 12 Parameters included in the Cervical Score have been previously associated with cervical deformity, 22 as well as with PJK 13 and health-related quality of life. 23 Other factors have been reported to be associated with junctional pathologies, including osteoporosis, age, and neurological comorbidities.15,24 While these other factors may be associated with an increased risk, surgeons have limited ability to directly affect these parameters. Thresholds used in the Cervical Score were tailored to patient age. This approach of using age-adjusted thresholds has been successfully applied to proximal junctional issues in the thoracolumbar literature. 13 The post-operative distribution of Cervical Scores revealed that most of the patients had a score between −1 and 2, and that very few patients were severely over-corrected or under-corrected (above 4 or below −4).
Our results suggest that the Cervical Score could be of use in predicting mechanical failures. In our study, a score of 3 and above was indicative of significantly higher odds of experiencing mechanical failure. Therefore, pre-operative planning should not only account for regional correction, but also the global alignment and the alignment induced by this correction. In the thoracolumbar literature, overcorrection has been linked to mechanical failure and PJK.25,26 Our results in ACD patients contrast with this finding in that undercorrection may actually play a significant role in the development of mechanical failure following cervical realignment. An increased forward sagittal alignment, combined with poor muscle and bone quality, could be dramatic due to the dynamic aspect of the cervical spine leading to more dynamic solicitation. 27 With the development of improved dynamic evaluations, 28 future studies investigating the effect of cervical fused alignment and the range of motion distal to the fusion could provide further insight.
This study is not without limitation. First and foremost, the relatively small sample size combined with a follow-up of 1-year may limit the generalization of this result. Validation of these findings based on larger sample size is warranted. Second, the large variability in terms of pre-operative deformity does not allow for more granular analysis of regional and focal alignment. Finally, the lack of dedicated patient-reported outcomes and neurological examinations limits the ability to characterize a potential association between the proposed Cervical Score and patient quality of life.
Conclusion
Mechanical failures following ACD surgery occurred in almost 1 out of 5 patients in this cohort, with 50% of them requiring a revision surgery before 1-year follow-up. Larger pre-operative malalignment combined with poor post-operative sagittal alignment were associated with mechanical failure. The proposed Cervical Score enabled quantification of the proportionality of sagittal alignment. A Cervical Score of 3 or above was associated with a marked increased risk of mechanical failure within the first year following surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes (current), Nuvasive (current), K2M (current), Innovasis (past), Biomet (past), and individual donations.