
Abstract
Study Design:
Retrospective study of the prospectively collected outcomes data.
Objective:
The indications for PPS placement during minimally invasive spine stabilization (MISt) procedures have increased in recent years. To the best of our knowledge, no studies have documented the outcomes of PPS insertion using the all-in-one PPS system. This study compared the conventional methods and the use of all-in-one percutaneous pedicle screw (PPS) system with respect to the speed and accuracy of PPS placement. We also determined the advantages associated with the use of the all-in-one PPS system.
Methods:
We evaluated 54 patients who underwent PPS insertion using the conventional method and the all-in-one PPS system during MISt procedures. We also assessed the number of implanted PPSs, the time taken to implant PPSs, and the accuracy of PPS placement based on postoperative computed tomography images.
Results:
A total of 254 PPSs were inserted (126 using the conventional method and 128 using the all-in-one PPS system). The PPS insertion time with the all-in-one PPS system (mean, 25.3 ± 9.1 s) was significantly shorter than that using the conventional method (mean, 63.1 ± 13.0 s; P < 0.01). With respect to the accuracy of PPS insertion, ≥ 2 mm pedicle breach was noted in one case each in both groups.
Conclusions:
PPS placement using the all-in-one PPS system is as safe as conventional methods and has the potential to save the surgical time of MISt procedures.
Keywords
Introduction
Several recent reports have demonstrated the effectiveness and safety of manually-inserted pedicle screws.1-8 Moreover, several studies have investigated the effectiveness of percutaneous pedicle screws (PPSs).9-12 PPSs have the advantage of minimal muscle dissection, and thus decreased blood loss and subsequent infection rates. This then translates to a shortened hospital stay and favorable patient outcomes.13-18 PPSs, widely used for minimally invasive spine surgery (MIS), are an indispensable tool to MIS surgeons. To improve the safety and efficiency of PPS insertion, a probe and guidewire were developed. 19 There have also been attempts to minimize radiation exposure and use of navigation systems during insertion of PPSs,20,21 as well as to shorten the operation time. These novel attempts include PPS insertion in the decubitus position and using a power tool.22,23
Recently, we commenced using the all-in-one PPS system (Viper Prime TM, DePuy Synthes Spine, Raynham, MA, USA) that has an integrated guide pin self-tapping screw to conduct minimally invasive spine stabilization (MISt). To the best of our knowledge, there are no published clinical reports pertaining to the effectiveness of PPS placement using the all-in-one PPS system.
We compared our conventional PPPs methods to the all-in-one PPS system with respect to the speed and accuracy of PPS placement and other advantages associated with the use of the all-in-one PPS system during minimally invasive thoracolumbar spine surgery.
Materials and Methods
Basic Patient Data
The protocol for this study was reviewed and approved by the ethics committee of our institution; Approval Number: 2 019 037; Approval Date: 2019.09.26. We obtained written informed consent or by opt from all participants. At our hospital, 54 patients (22 males and 32 females) underwent minimally invasive thoracolumbar fusion or fixation by a posterior approach between May 2018 and December 2019. The mean age of patients was 68.6 years (range, 29-86). Forty-nine patients had degenerative spinal disease, 2 had traumatic thoracolumbar fracture, and 3 had osteoporotic vertebral fracture.
Surgical Procedures
We randomly divided the cohort into 2 groups. Group C consisted of 27 patients who underwent PPS insertion using the conventional method (C method) and Group A consisted of 27 patients in whom the PPS was inserted using the all-in-one PPS system (A method). We used a biplane fluoroscopy system (Biplanar™ 500e, Swedish Medical Imaging Devices AB, TÄBY, Sweden) for PPS insertion during the surgery (Figure 1). All procedures were performed by the same surgeon.
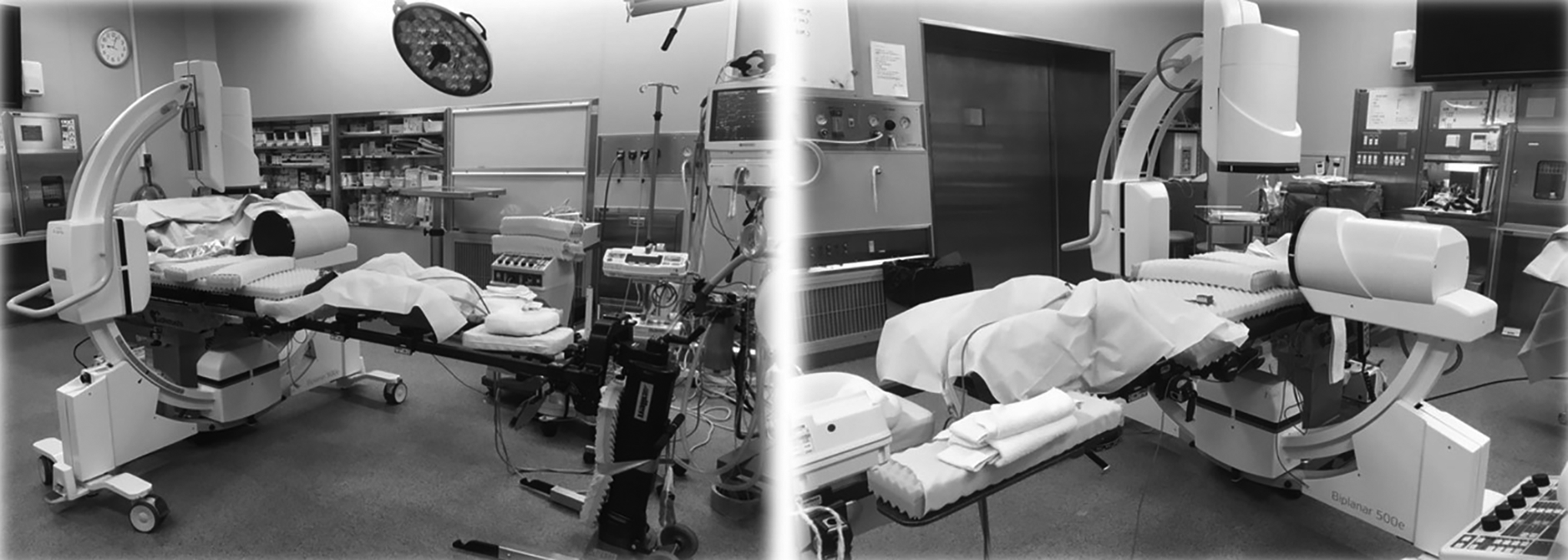
Photograph illustrating the biplane fluoroscopy system. The symmetrical G-shaped arm, comprising 2 independent perpendicular imaging systems, provides simultaneous anteroposterior and lateral views of the surgical site.
PPS placement with the conventional method (C method)
After making a 20-mm-long vertical or midline skin incision and opening the myofascia, finger navigation was used to identify the PPS placement points. These points were the lateral side of the facet joint, the intersection of the lateral side of the superior vertebral notch, and the base point of the transverse process and their shapes were evaluated. Subsequently, the probe was placed in contact with a point. If the tip of the probe was located on the lateral side of the pedicle on the fluoroscopic anteroposterior (AP) view, it was possible to insert the probe into the pedicle. Afterward, Jamshidi needles or customed cannulated probes were used to drill a screw hole that would be used for inserting the guidewire. 19 Subsequently, the screw would be inserted by means of the guidewire.
PPS placement with the all-in-one PPS system (A method)
We used the same entry point for screw insertion in each group. However, because the all-in-one PPS system has an integrated guide pin self-tapping screw (Figure 2), the steps mentioned above were not required. 24 The all-in-one PPS system also has a new screw tip design and a stylet that is fully controlled by the screwdriver. Thus, the surgeon can accurately aim for the pedicles and insert screws in one single instrument pass. (Figures 3 and 4). 24
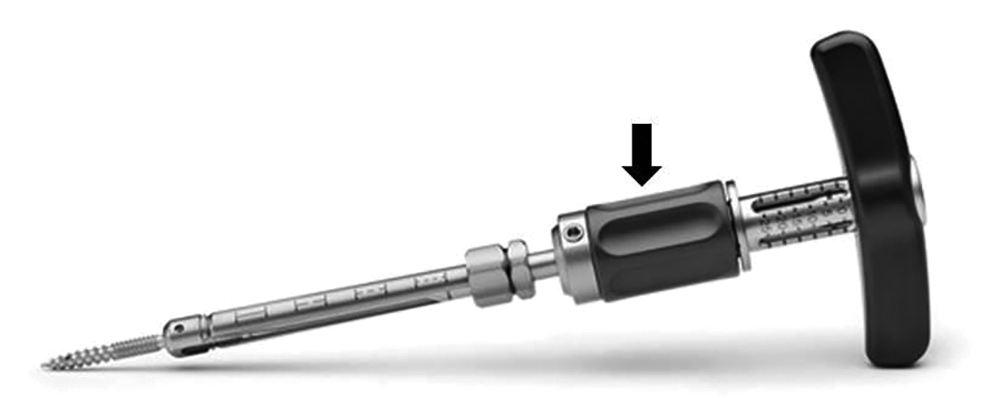
Illustration of an all-in-one PPS system. Featuring a new screw tip design and a stylet that is fully controlled by the screwdriver with the stylet control handle (allow) and the modular handle, surgeons can target pedicles and insert screws in one single instrument pass. Modified from VIPER PRIME TM System Surgical Technique.
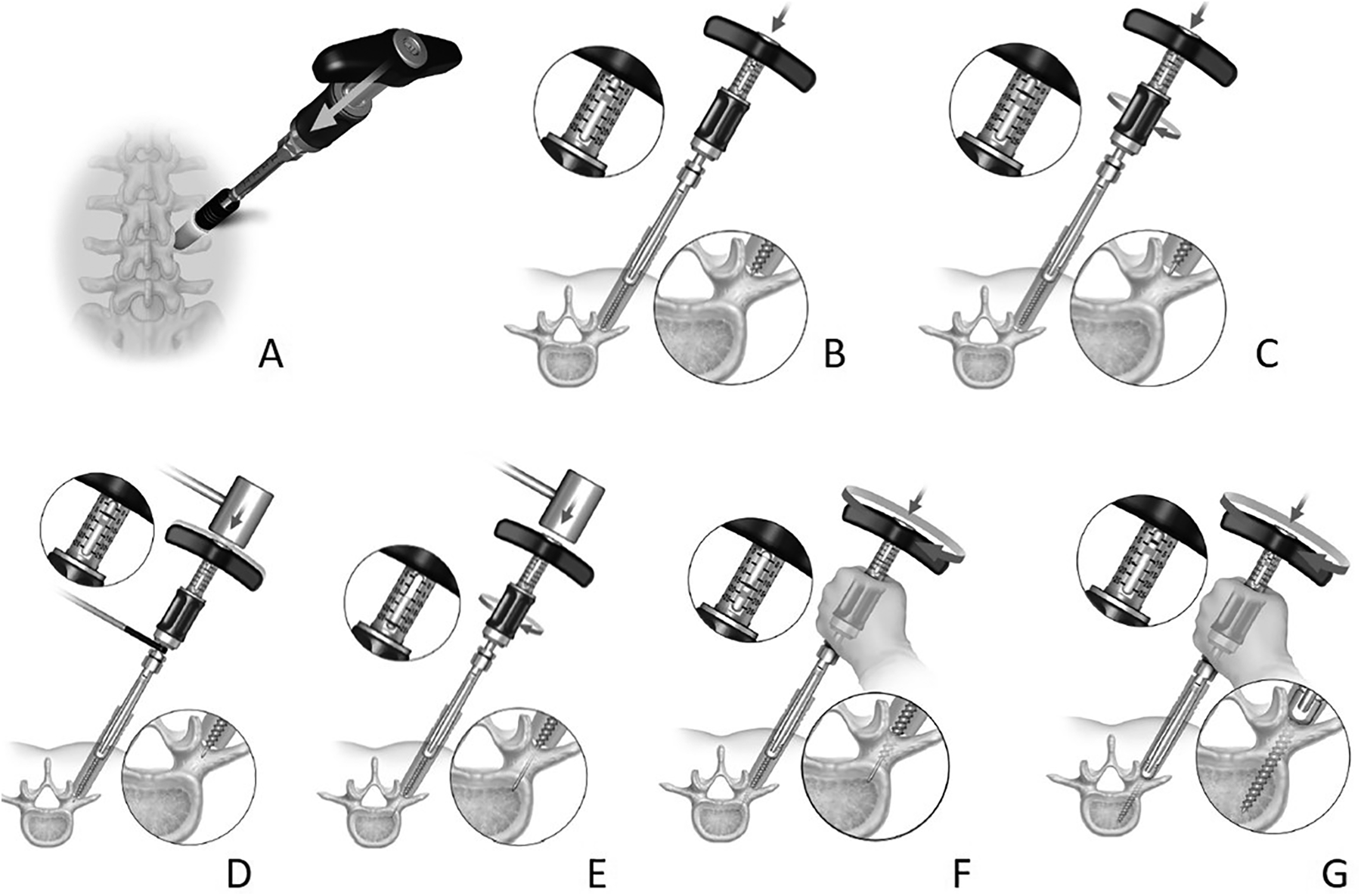
Schematic drawing illustrating of the screw insertion steps using with the All-in-one PPS system.
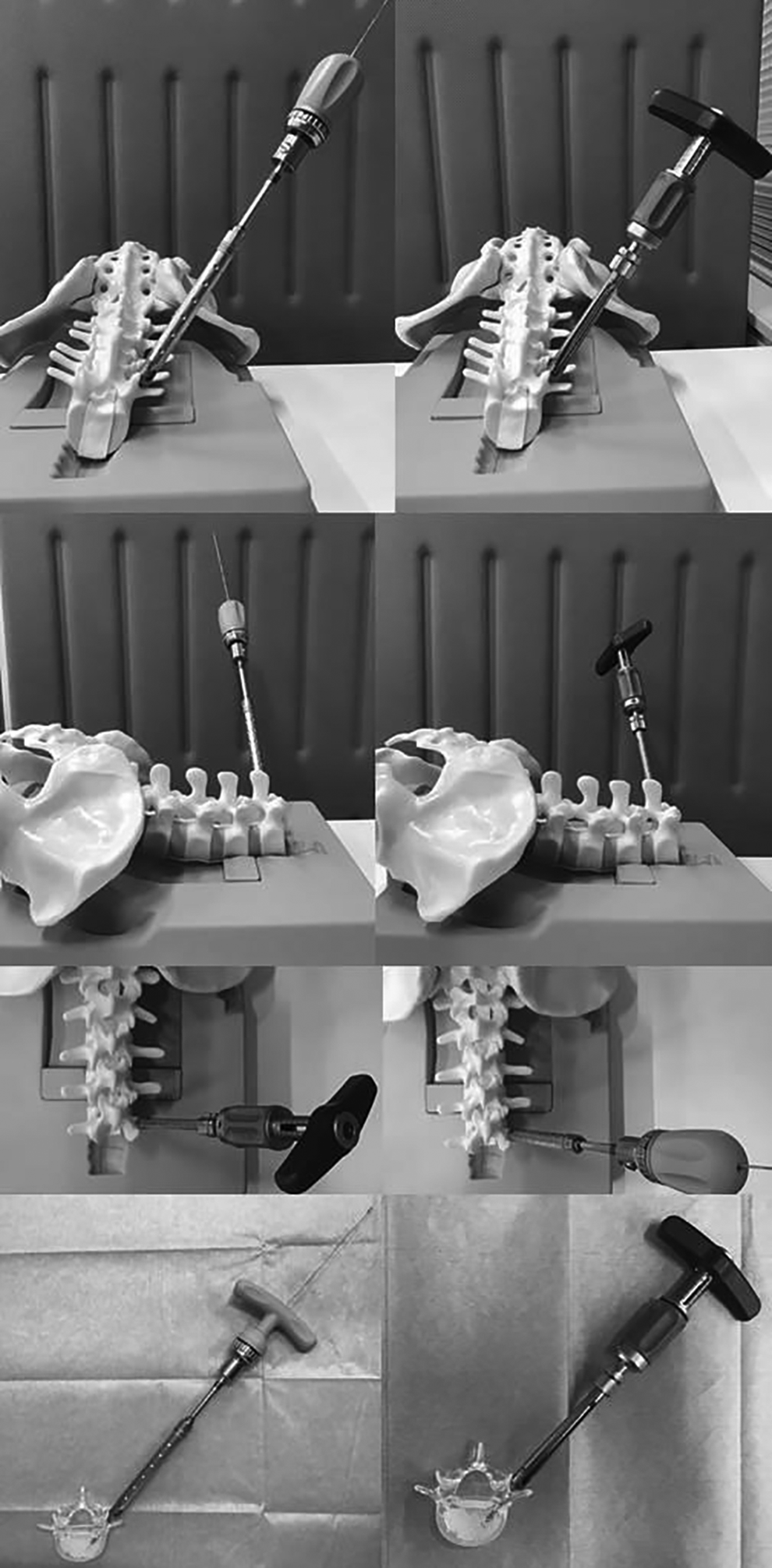
Photograph illustrating seen from various angles the use of the conventional PPS system shown on the left and the all-in-one PPS system shown on the right. Reduction in pedicle preparation and screw insertion job steps. In the all in one PPS system, we do not need guidewires for PPS insertion.
Assessment of Outcome
The following variables were assessed in this study: (1) the number of implanted PPSs, (2) the time required to implant a PPS, and (3) the accuracy of PPS placement as determined postoperatively based on computed tomography (CT) images using the grade classification described by Gertzbein and Robbins. 25 A CT scan was obtained to check the PPS placement within 4 days of surgery. PPS misplacement was defined as a breach of the pedicular wall, which was graded on a 2-mm steps’ as follows: grade A, no breach; grade B, breach <2 mm; grade C, breach 2-4 mm; grade D, breach 4-6 mm; grade E, screws that do not pass through the pedicle or that, at any given point in their intended intrapedicular course, breach the cortical layer of the pedicle in any direction by more than 6 mm). 25
In Group C, the screw insertion time was defined as the time from the installation of the probe at the insertion point to the completion of the insertion of the screw into the pedicle. In Group A, screw insertion time was defined as the time from the installation of the stylet tip, which served as the guide pin at the screw insertion point, to the completion of screw insertion into the pedicle. All the screw is planed preoperatively using a CT were assessed by measuring the diameter and length of all the screws using the ShadeQuest / View R image data integration system manufactured by the Yokogawa Electric Corporation.
Statistical Analyses
Statistical analyses were performed using the Excel Statistical Software Package (Ekuseru-Toukei 2012; Social Survey Research Information Co., Ltd., Tokyo, Japan). Between-group differences with respect to categorical variables were assessed using the Chi-squared test, while those with respect to continuous variables were assessed using the Mann-Whitney U test and Student’s t-test. P values < 0.05 were considered indicative of statistical significance.
Results
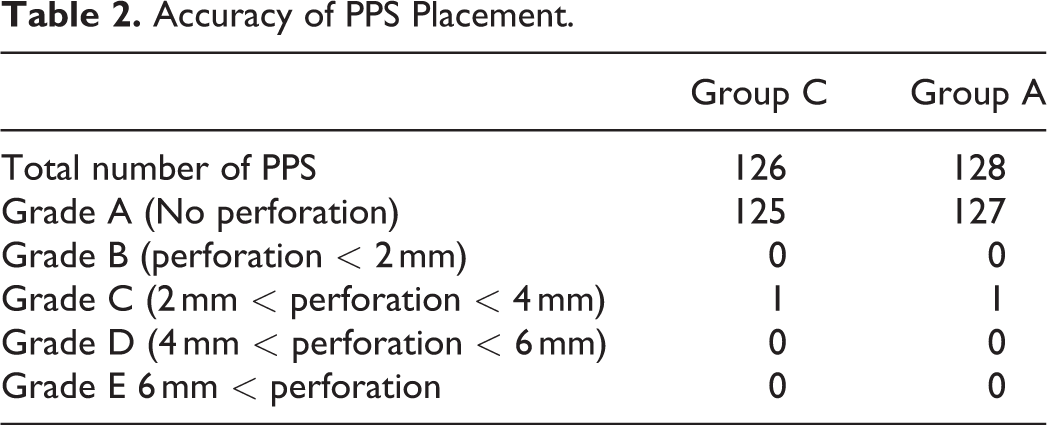
The demographic characteristics of patients are summarized in Table 1. There were no significant between-group differences with respect to patient characteristics. A total of 254 PPSs were inserted in 54 patients from T9 to S1 levels. Of the 254 PPSs, 126 were implanted using the C method, while 128 were implanted using the A method. The mean time taken to implant a PPS using the A method (25.3 ± 9.1 s) was significantly shorter than that using the C method (63.1 ± 13.0 s, P < 0.01) (Figure 5). The A method shortened the screw insertion time by approximately 0.4 times. Breaches of ≥ 2 mm (Gertzbein and Robbins grade C) were observed with one screw in Group C (0.79%) and one screw in Group A (0.78%). Thus, there were no significant between-group differences with respect to the accuracy of screw placement (Table 2). None of the patients developed postoperative complications.
Patient Demographics.
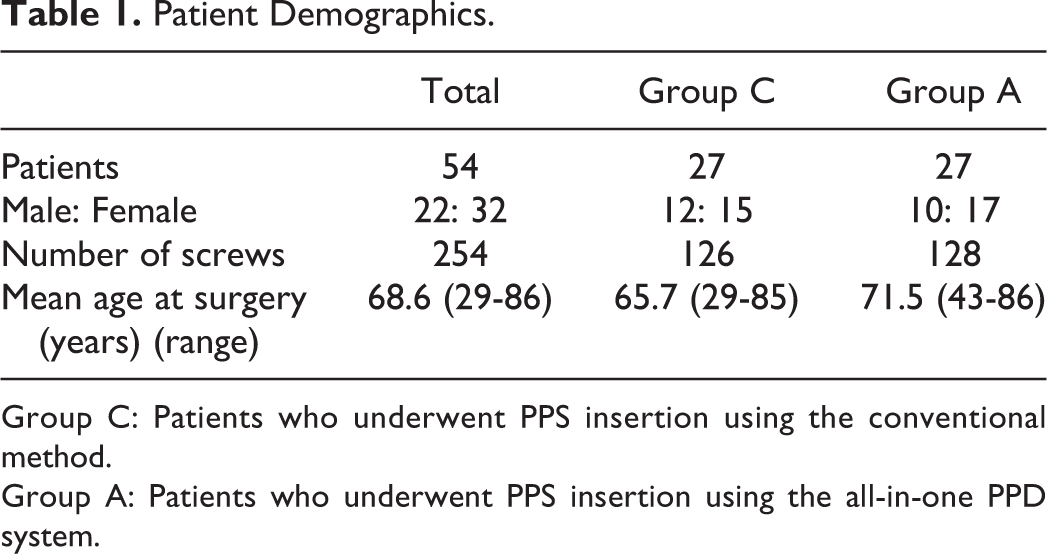
Group C: Patients who underwent PPS insertion using the conventional method.
Group A: Patients who underwent PPS insertion using the all-in-one PPD system.
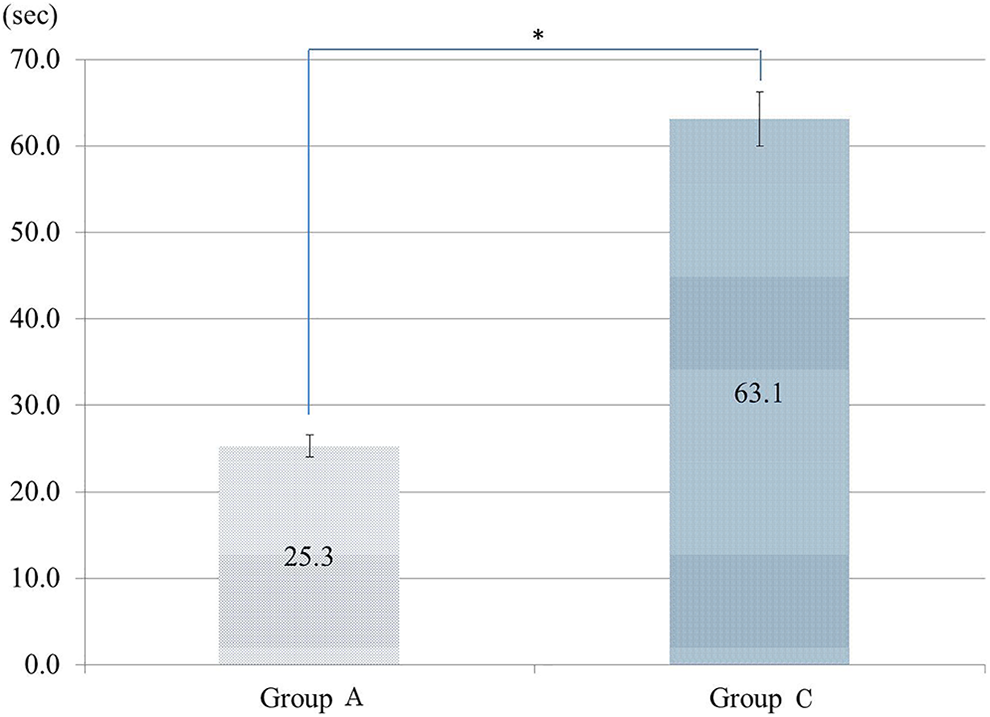
Time taken for percutaneous pedicle screw placement using the conventional methods and the all-in-one methods.
Accuracy of PPS Placement.
Discussion
A method of inserting PPS that does not need the use of a guidewire was recently reported by Spitz et al 12 and Kleck et al. 26 However, these methods are cumbersome and require the use of a navigation system. The all-in-one PPS system is a novel technique for PPS placement, which eliminates the need for guidewires, Jamshidi needles, and pedicle preparation instruments. The all-in-one PPS system features a new screw tip design and a stylet that is fully controlled by the screwdriver; it is the only system that allows the surgeon to target the pedicles and insert the screws with a single instrument pass.
In the conventional PPS insertion procedure, the first step is skin incision and dissection of fascia followed by finger navigation; the second step entails the insertion of a probe or Jamshidi needle; in the third step, the inner sleeve of the probe is pulled out followed by insertion of the guidewire; the fourth step entails pulling out the probe jacket and tap; and the final step involves tap removal and screw insertion. The all-in-one PPS system simplifies this process by omitting the abovementioned 5 steps. According to the preliminary report, the all-in-one PPS system reduces the screw insertion time by approximately 60%, which is comparable to that observed in our study. 27 In the same cadaver study report, 8 surgeons found that the all-in-one PPS system was 33% faster than the conventional methods.
Figure 6 shows the differences between the conventional and all-in-one PPS system. The all-in-one PPS system entails use of very few instruments. The stylet takes the place of both the probe and the guidewire. Use of the all-in-one PPS system resulted in fewer instrument passes between the surgeon and the nurse on the back table. We used a biplane fluoroscopy system for intraoperative guidance of PPS insertion. Nakahara et al documented favorable PPS placement using a conventional dual fluoroscopy-guided technique, irrespective of the surgeon’s experience. The classical modified method for PPS insertion guided by dual fluoroscopy entails a greater risk of radiation exposure; however, it increases the likelihood of accurate placement irrespective of the setting or surgical skill set. 28
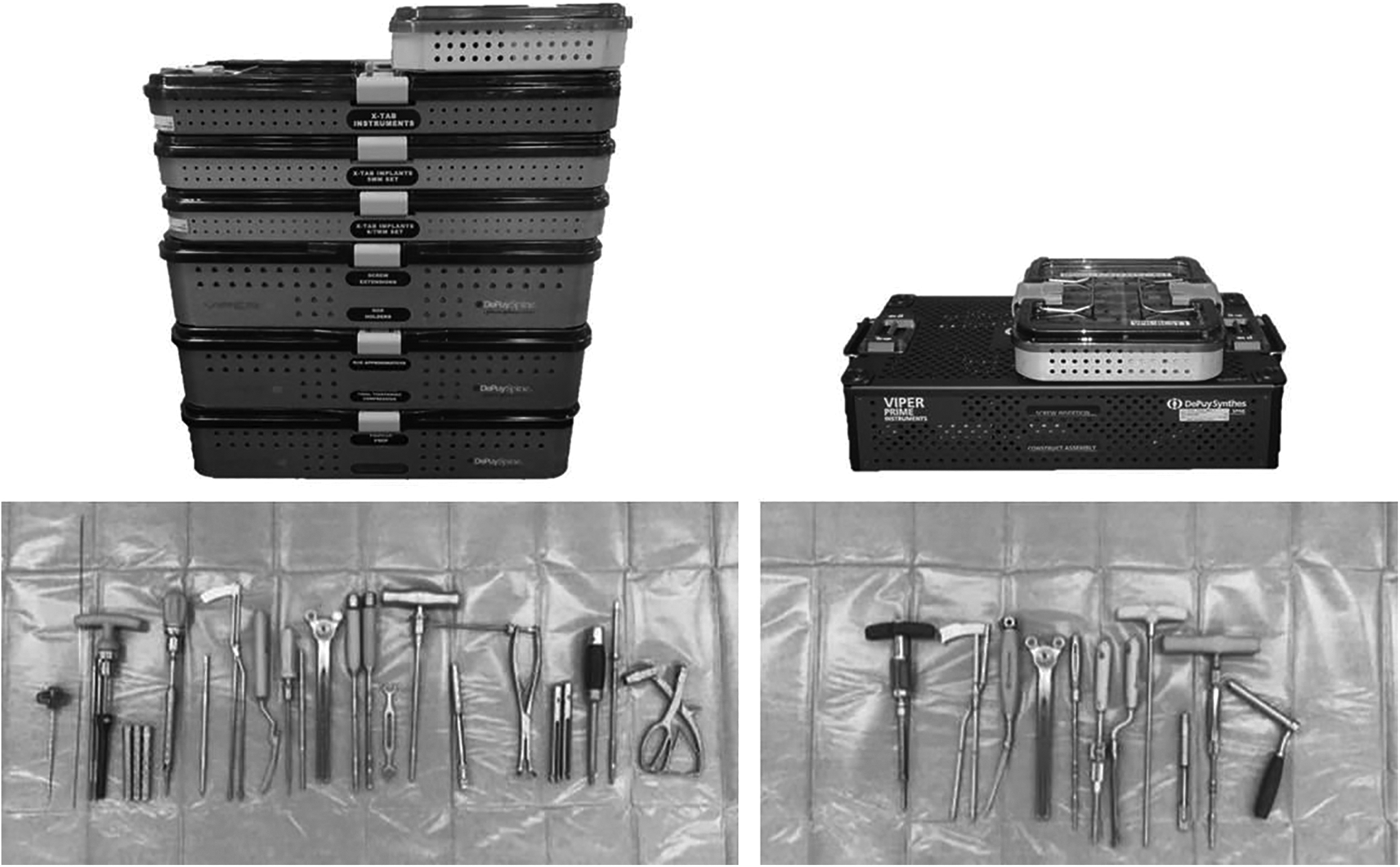
Surgical instrument set of the conventional PPS system shown on the left and the All-in-one PPS system shown on the right. More organized back table with fewer instruments required and fewer instrument passes between the surgeon and the back table.
Serious intraoperative complications associated with PPS placement include great vessel and bowel injuries due to the guidewire’s anterior migration and penetration through the anterior aspect of the vertebral body. 19 In the all-in-one PPS system, we do not need guidewires for PPS insertion. The screwdriver and stylet are integrated, so if we use them properly, the stylet will not break through the anterior aspect of the vertebral body while inserting the PPS.
Moreover, it is difficult to simultaneously insert screws at multiple levels as with the conventional method. It is difficult to insert the screw while visualizing the image on the left and right sides or on multiple vertebral bodies concurrently.
One reason is the high cost of the stylet (approximate cost, 200 USD). As long as the stylet is not damaged, we can insert the screw one by one and use only one stylet during the same surgery. Since the screw is inserted in a single step in the A method, it is difficult to correct the trajectory. The all-in-one PPS system should preferably be used by surgeons well versed with the conventional PPS.
This study had some limitations. We did not conduct a detailed evaluation of radiation exposure. The radiation exposure evaluation could be an advantage (or disadvantage) for the all-in-one PPS system. Also, the diameter and length of the screws varied for each patient in this study. However, the aim of the present analysis was to compare accuracy, which is a radiological assessment. While no difference was found in placement accuracy between 2 groups, our data do not allow us to conclude that the compared 2 groups are equivalent in terms of surgical outcome. Cases with osteosclerosis were not included in this series. In patients with bone sclerosis of spine, the stylet insertion takes more time, and screw insertion is somewhat difficult without a tap. Further research about radiation exposure and long term results is required.
By maintaining the screw placement accuracy and avoiding radiation exposure, the use of an all-in-one PPS system appears to be beneficial to patients, surgeons, and surgical staff. Therefore, this approach further contributes to the development of MISt procedures.
Conclusions
Compared to the conventional method, the all-in-one PPS system shortened the screw insertion time by approximately 0.4 times, with equivalent insertion accuracy. The all-in-one PPS system is a promising new tool for MIS.
Footnotes
Abbreviations
Authors’ Note
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request. The protocol for this study was reviewed and approved by the ethics committee of our institution named—“Funabashi orthopaedic hospital ethics committee”; Approval Number: 2 019 037; Approval Date: 2019.09.25. Written informed consent was obtained from participants. This study received an exemption by the institutional review board of our institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.