
Abstract
Study Design:
Retrospective radiographic study.
Objective:
The aim of this study was to define the association between thoracic inlet measures in relation to anterior access to the cervicothoracic junction.
Methods:
Trauma CT scans in patients >16 years were analyzed. The projection angle (PA), defined as the angle subtended by a line along the superior endplate of the vertebral body and the line from the anterosuperior corner of the vertebral body to the manubrium, was measured at C7, T1 and T2; angles were positive if the projection was above the manubrium. Thoracic inlet angle (TIA), thoracic inlet distance (TID) and pelvic incidence (PI) were measured.
Results:
65 scans were assessed (33 males; mean age 47.7 years (s.d. 8.7)). The mean TIA 79.9° (s.d. 13.4°; range 52.6° – 112.2°), mean TID 66.1 mm (s.d. 6.6 mm) and mean PI was 50.5° (s.d. 10.2°). Mean values for the projection angles at C7, T1 and T2 were 24.2°, 7.6° and −8.3° respectively. PA were positive in 95% at C7, 73% at T1 and 30% at T2. PA at each level correlated significantly with age (mean r=−0.371; P = .015) and TIA (mean r=−0.916; P < .001) but neither TID nor PI. TIA correlated with age (r = 0.328; P = .008).
Conclusions:
The projection angles of the CTJ vertebrae are influenced by thoracic inlet angle and a lesser degree age. Understanding sagittal spinal parameters in the CTJ can aid in planning surgical strategy and approach.
Introduction
Anterior surgical approaches to the cervical spine are frequently utilized for a variety of pathology including degenerative, traumatic, infectious and oncologic etiologies.1,2 However, when an anterior approach to the cervicothoracic junction is required access may be more challenging as the medial clavicle and sternum may impede a direct approach – this may necessitate the use of an osteotomy.3-5
During surgical planning sagittal spinal parameters are often considered to guide appropriate reconstruction including maintenance or restoration of patient-specific alignment. In the cervical spine the Thoracic Inlet Angle (TIA) may be used. 6 Defined as the angle subtended by a line drawn perpendicular to the superior end plate of the T1 vertebral body and a line drawn through the midpoint of the T1 vertebral body superior endplate to the manubrium, the TIA can be used to estimate cervical spine alignment.7-9 The TIA is generally considered analogous to the Pelvic Incidence (PI) used for determining ideal lordosis in the lumbar spine. 9
The PI has recently been shown to correlate with the ‘projection angle’ of the sacral endplate with respect to the pelvis and predict ease of anterior access to the lumbosacral disc – in this case a PI over 73º suggests the trajectory of the sacral endplate is distal to the apex of the pubic symphysis. 10 It is intuitive therefore that a relationship may exist also between the TIA and access to the vertebrae at the base of the subaxial spine and across the cervicothoracic junction.
The aim of this study was to report on the correlation between sagittal thoracic inlet measures and anterior access to the cervicothoracic junction as indicated by the ‘projection angle’. The findings from this study may serve as an aide to surgeons when considering surgical strategy for pathology at the cervicothoracic junction.
Materials and Methods
Approval for this study was granted by the Health and Disability Ethics Committee (Ref: 20/STH/143). Patient consent was not required for this study.
Computed tomography (CT) scans performed for the purposes of major trauma assessment were obtained from the hospital radiology database. Scans were included from patients aged ≥16 years to eliminate the potential influence of skeletal immaturity. Scans were excluded if there was disease that prevented measurement of sagittal measures (e.g., fracture, tumor, trauma, spinal deformity such as spondylolisthesis or scoliosis, prior surgery), if there was an abnormal vertebral body count or if there was transitional anatomy present. All radiologic assessments were made using IntelliSpace PACS Enterprise (Koninklijke Philips N.V.) by a single fellowship-trained spine surgeon.
Patient details including age and sex were recorded. Thoracic inlet measures including the Thoracic Inlet Angle (TIA) and Thoracic Inlet Distance (TID) have been well-described in previous reports including assessment on advanced imaging modalities.6,7,9,11-14 Measurement of TIA and TID utilized the midsagittal CT image – clear visualization of the manubrium was essential to allow the thoracic inlet measures (Figure 1). Pelvic Incidence (PI) was measured, as has been previously described, by identifying the midpoint of both femoral heads to determine the bicoxofemoral axis, then measuring the angle subtended by a line from the bicoxofemoral axis to the center of the sacral endplate and a line perpendicular to the center of the sacral endplate (Figure 2).9,10 The Projection Angle (PA) was measured at C7, T1 and T2. The PA is defined as the angle subtended by a line along the superior endplate of the vertebral body and the line from the anterosuperior corner of the vertebral body to the manubrium. A positive angle, indicating potential access, is one with projection of the line along the endplate superior to the manubrium (Figure 3). A negative angle, indicating poor or impossible access, is one with projection inferior to the manubrium (Figure 4).
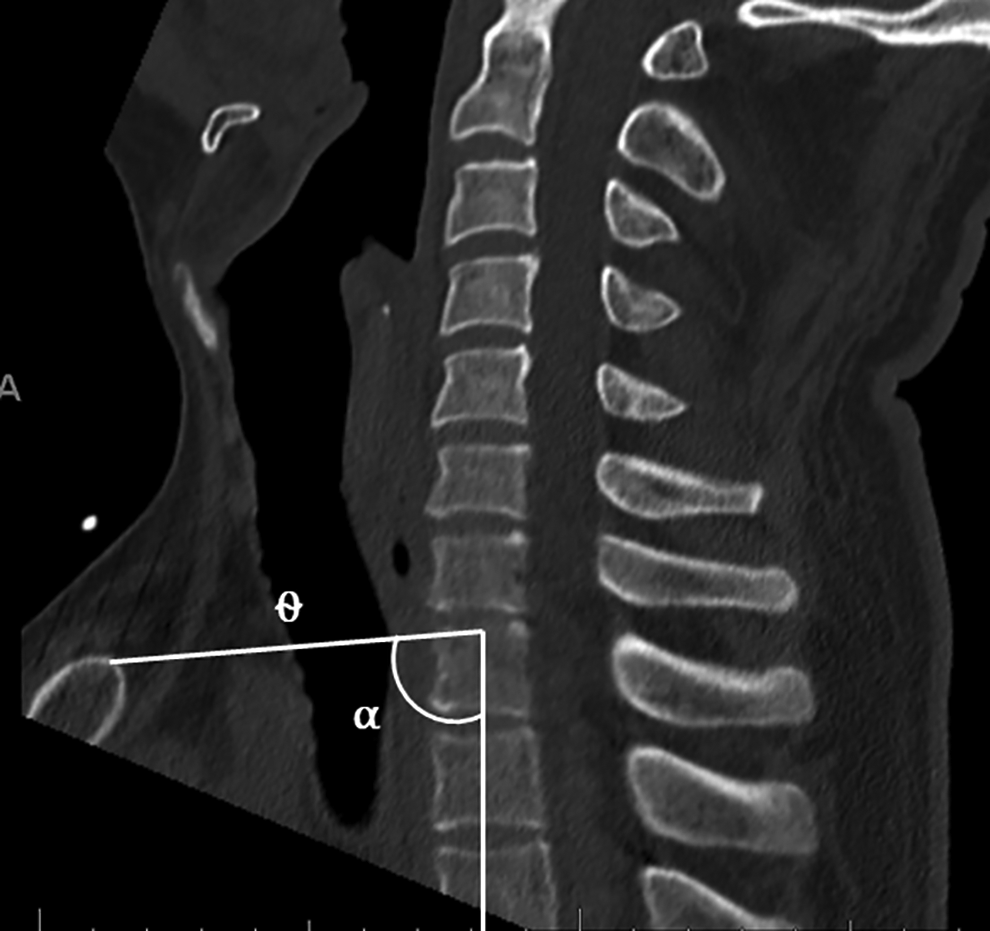
Thoracic Inlet Angle (TIA) is measured by the angle (α) subtended by a line from the midpoint of the superior endplate of T1 through the apex of the manubrium and a line drawn perpendicular through the center of the superior endplate of T1. The TID is the distance in millimeters from the midpoint of the superior endplate of T1 to the apex of the manubrium (θ).
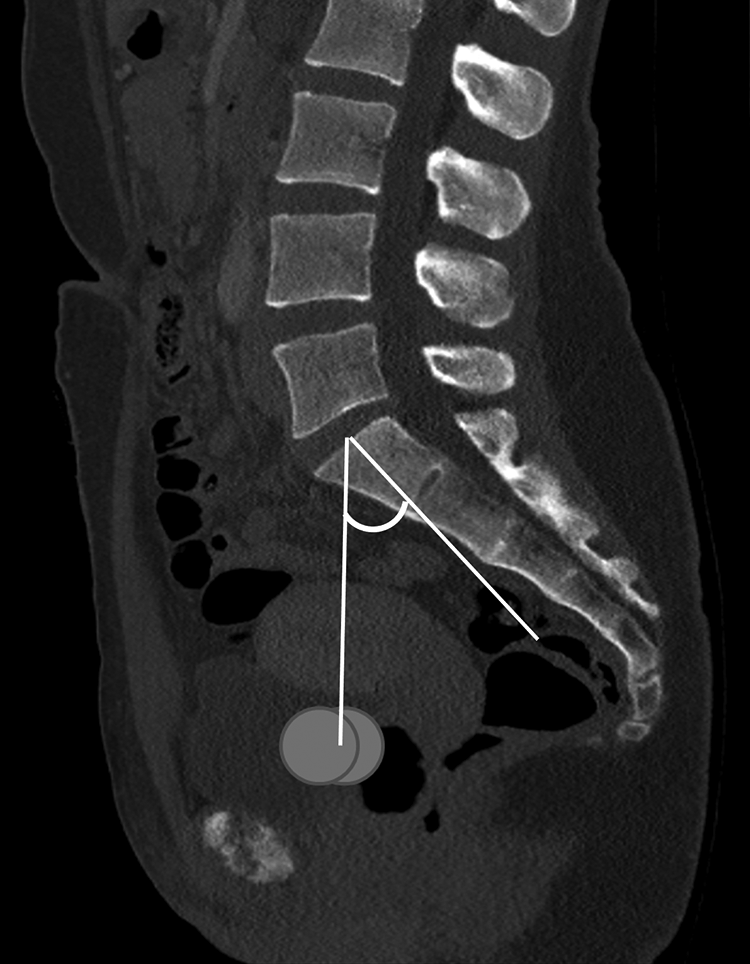
Pelvic Incidence (PI) is measured by identifying the center of the femoral heads on the relevant sagittal images (circles) then the midpoint between these identified on the midsagittal image to define the bicoxofemoral axis. PI is the angle then subtended by a line from the bicoxofemoral axis to the middle of the sacral endplate and a line drawn perpendicular through the center of the sacral endplate.

A positive projection angle is demonstrated for C7 with the plane of the superior endplate projecting proximal to the manubrium.

A negative projection angle is depicted for T2 with the plane of the superior endplate projecting distal to the apex of the manubrium.
All scans, and therefore measures, were taken in the supine position - it has been shown that the change in thoracic inlet measures between standing and supine positions is negligible and so erect imaging has not been used to complement the CT measures.6,11,13 Further it is established that the manubrium is poorly visualized on plain radiography and therefore poorly reliable as a point of measure compared to CT.11,13-15
Statistical Analysis
All data was compiled with a Microsoft Excel spreadsheet. ExcelSTAT was used for statistical analysis. Mean, standard deviation and range are reported where applicable. Univariate analysis was performed with the Mann-Whitney U-test. Intraobserver reliability was assessed using Cronbach’s alpha. This was completed by performing a second random set of ten measurements in a blinded-fashion 6 weeks after the first. Pearson correlation analysis was used to explore association between the sagittal variables and projection angles. Linear regression analysis was used to analyze significant determinants.
Results
65 scans were analyzed (33 male). The mean age was 47.2 years (s.d. 18.7; range 16-88 years).
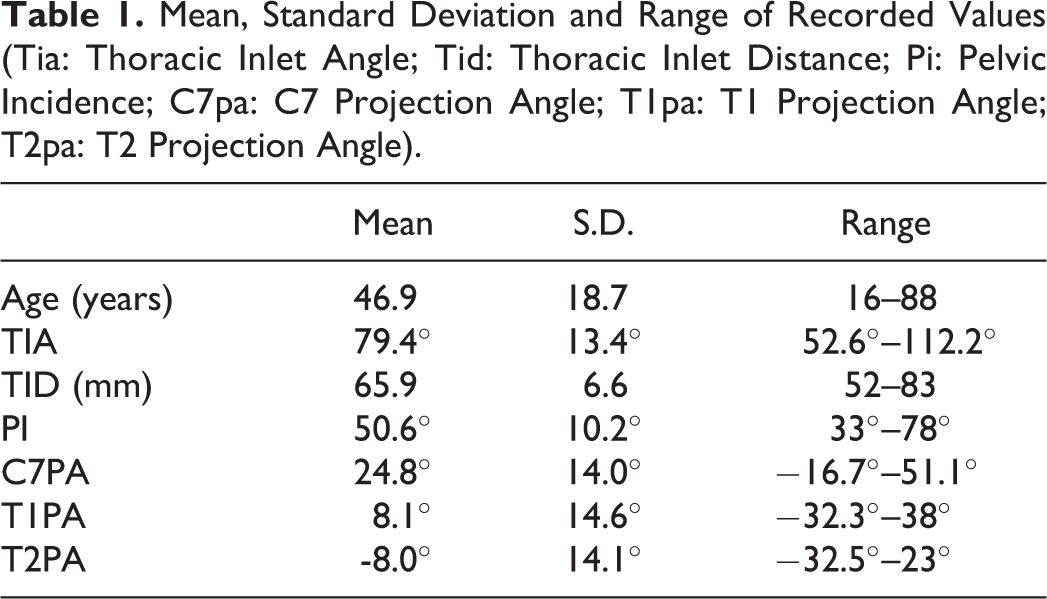
Mean values for the thoracic inlet dimensions, pelvic incidence and projection angles are shown in Table 1. There were no differences in variables between male and female subjects.
Mean, Standard Deviation and Range of Recorded Values (Tia: Thoracic Inlet Angle; Tid: Thoracic Inlet Distance; Pi: Pelvic Incidence; C7pa: C7 Projection Angle; T1pa: T1 Projection Angle; T2pa: T2 Projection Angle).
Cronbach’s alpha showed excellent reliability for all measures: TIA (0.958), TID (0.987), C7PA (0.971), T1PA (0.944) and T2PA (0.977).
Positive projection angles, that is projection above the manubrium, were present in 95% at C7, 73% at T1 and 30% at T2.
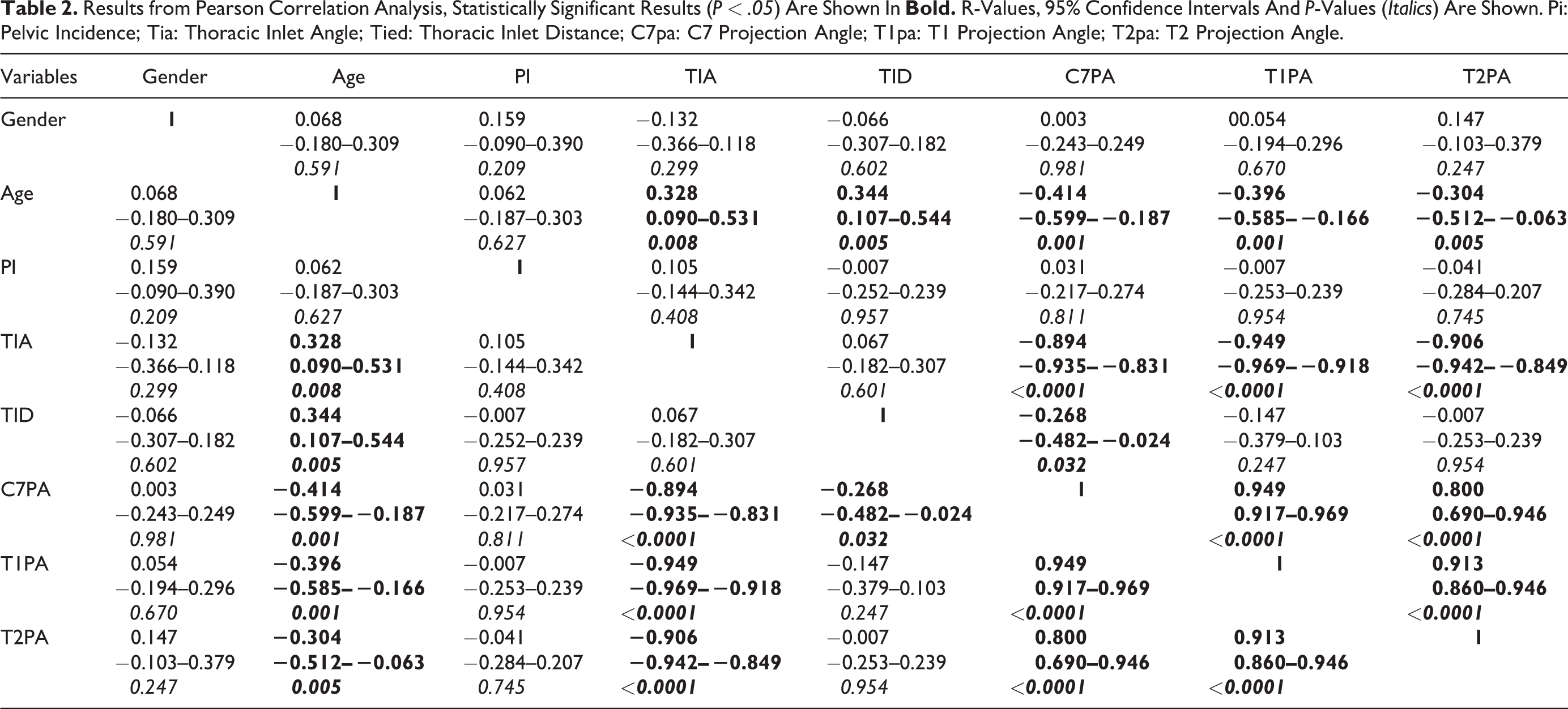
Results from the Pearson correlation analysis are shown in Table 2. Age correlated significantly with both thoracic inlet measures and all projection angles albeit only mildly so. The TIA however correlated strongly with all projection angles. The TID correlated mildly with only the C7PA. Scatterplots for PA against TIA are shown in Figures 6–8.
Results from Pearson Correlation Analysis, Statistically Significant Results (P < .05) Are Shown In
Linear regression was performed using both age and TIA providing the following models:



Discussion
Anterior access to the cervicothoracic junction may be needed to treat a range of pathology.1,2 Degenerative disease, trauma, infection or tumor resulting in loss of structural integrity of the anterior column may necessitate anterior access; compression of the spinal cord from anterior column pathology such as metastatic disease or extradural disease may be better managed via an anterior approach to adequately and safely decompress the spinal cord than via a posterior approach that can be technically challenging at the cervicothoracic junction.16-18 Analysis of individual anatomy and assessment of potential access is essential to reduce morbidity and achieve surgical goals.
The aim of this study was therefore to determine the relationship of sagittal thoracic inlet measures, principally the TIA, and anterior access to the cervicothoracic junction. Although age correlated with the projection angle of the vertebrae, this was only mild. The main determinant of anterior access was the TIA evidenced by a strong correlation with the projection angle in each instance. The projection angle of the superior endplate of the vertebrae correlated strongly with the TIA in a similar fashion to previous work demonstrating the projection angle of the lumbosacral disc in relation to the PI. 10 In the previous work it was evident that once the PI is over 70º then anterior access to the lumbosacral disc becomes difficult if not a suboptimal strategy.
In this current study it is notable that the projection angle from T2 was positive in almost one third of cases indicating potential access without osteotomy - the projection angle for C7 tended to become negative only once the TIA was above 105º while for T2 the PA only tended toward negative once the TIA was above 70º. As our understanding of the role of TIA in determining cervical alignment improves, its role in surgical planning, much like the PI in lumbar surgery, should be further elucidated. Noting that there is a likely threshold beyond which anterior access to the CTJ becomes difficult is a key component of sound surgical planning. However, it is worth noting that when accessing the disc space only, a narrow corridor could still be encountered and access to the posteroinferior corner of T1 would remain challenging. Some surgeons may consider the medial border of the clavicle as the limiting anatomic structure rather than the manubrium - this study was performed in a manner consistent with other reports that have considered the manubrium as the inferior limit of the surgical corridor.1,2,19
Complex spine surgery frequently involves advanced imaging modalities for planning and measurement of the projection angle and thoracic inlet parameters can aid in determining the best strategy for surgical access including consideration of osteotomy where needed. Incorporating the findings relating access to sagittal plane parameters into planning software may be an option. 20 Additionally, anticipating that anterior access to the CTJ may be difficult will allow the surgeon to ensure appropriate instruments, such as angled or articulted devices, are available.
Similar to this current study, Karikari et al. previously assessed the potential to access the disc space anteriorly across the cervicothoracic junction also using computed tomography. 1 The T1/2 level was most commonly the most caudad level accessible (46%) and the T2/3 to a lesser degree (20%). However, the relationship between access and sagittal plane parameters not explored. Mai et al. analyzed sagittal MRI imaging to determine the most caudad level accessible and noted that in 83% this was the T1/2 disc — approximately 10% more than in the current study. 15 Reasons for this difference may be related to imaging modality or body habitus but again sagittal plane parameters were not analyzed. Finally, analysis of supine MRI by Lakshamanan et al. utilized a line tangential to the manubrium to determine the most caudad level accessible via an anterior approach. 2 Although in nearly 70% of cases this line passed through T2 or T3, this assessment of imaging is more applicable when planning a corpectomy is required as the visualization is improved with removal of bone.
There was a weak correlation between age and the TIA. The inlet may change with age as the thoracic cavity dimensions change and therefore the ‘base’ upon which the cervical spine sits also changes. However, the influence of age on the projection angle was near negligible in the regression analysis. A more pronounced or protruded sternum, a factor of thoracic cavity morphometry, may additionally influence ease of access and this factor has not been assess in this current study. Extremes of PA are shown in Figure 5 where it is evident how the disc may be more easily accessed in the scan on the left compared to that shown on the right.
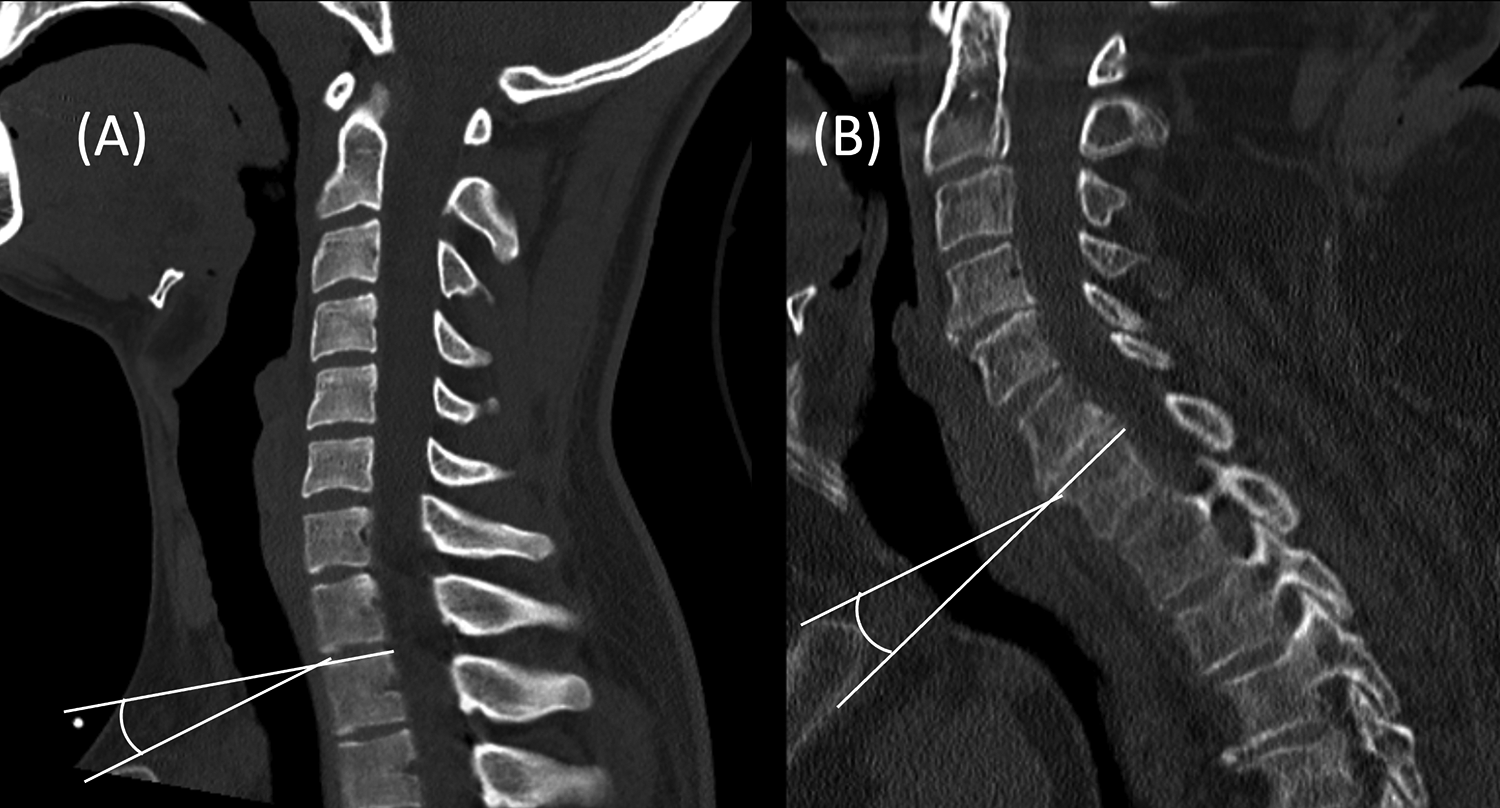
Comparison of strongly positive projection angle at C7 in a younger patient (A) against a strongly negative angle at C7 in an elderly patient (B).
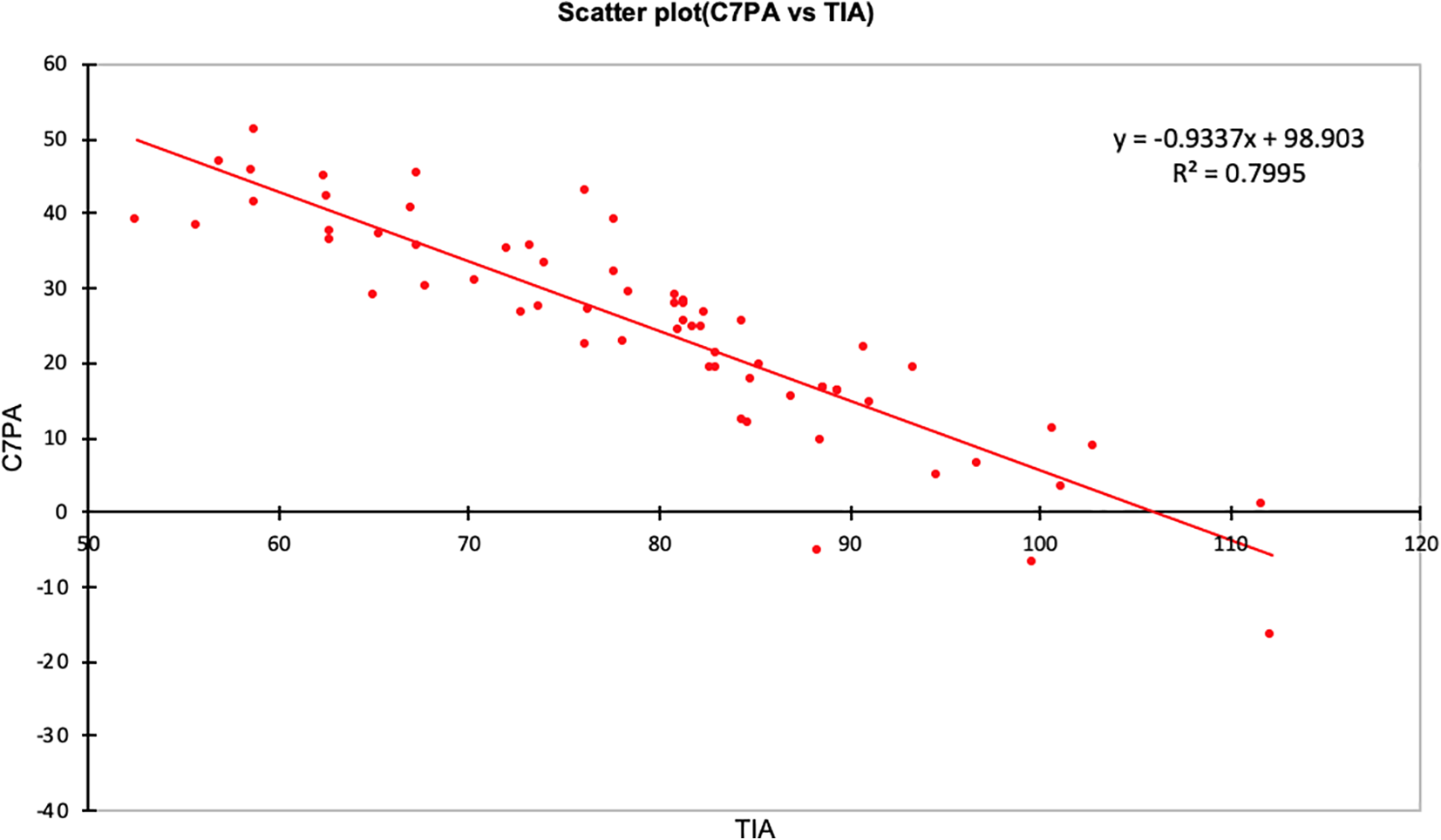
Scatterplot of C7PA (y) against TIA (x) with linear regression equation.
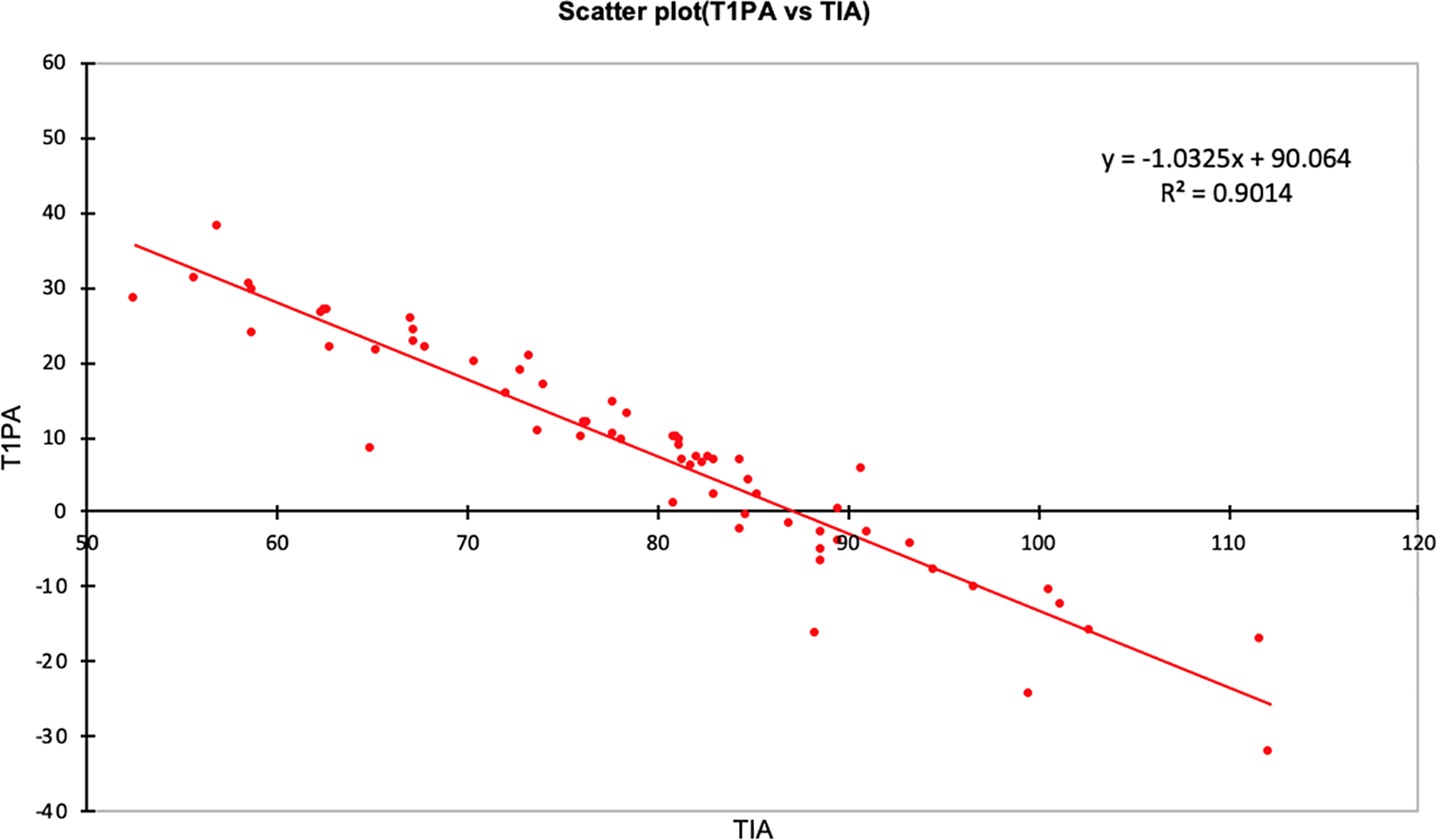
Scatterplot of T1PA (y) against TIA (x) with linear regression equation.
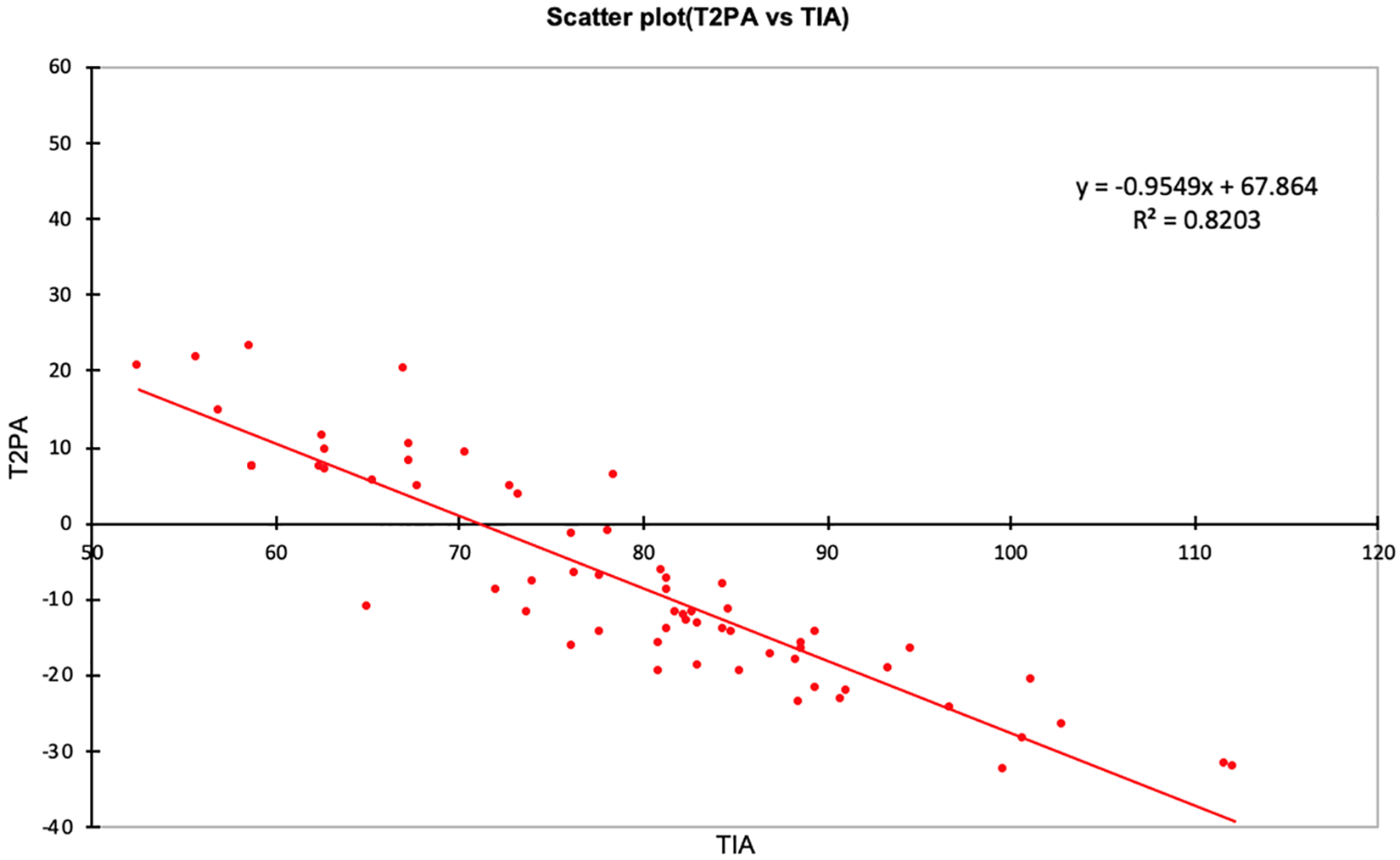
Scatterplot of T2PA (y) against TIA (x) with linear regression equation.
Limitations of this study include use of computed tomography alone in the supine position, although we note that the TIA does not appear to change between supine and standing postures. 11 However, any surgical procedure is likely to be performed in a position not dissimilar to that in which these scans were obtained with the cervical spine in extension to accentuate surgical access. There is also potential for spinal alignment, and therefore the thoracic inlet angle, to change with respiration although this is thought likely to be only mild without aggressive inspiration or expiration.21,22 To define the influence of patient positioning, flexing or extending the spine, application of traction - both through cervical tongs and taping or depressing the shoulders, and respiratory status on thoracic inlet parameters and the anterior access to the CTJ, intra-operative 3-dimensional imaging could be utilized. However, this would confer additional radiation exposure and raises ethical questions about unnecessary patient risk.
This study also only analyzes patients without overt disease of the spinal column accepting that CT is not the diagnostic tool of choice to define disc disease. Although normative data is often useful, application of the findings of this study to the deformed spine may not be immediately appropriate – one needs to consider that a deformed spine may be stiff, perhaps in the setting of post-traumatic deformity, or flexible, perhaps arising from acute pathologic fracture secondary to metastatic disease. The findings from this study may have more ready application to the latter but the degree of correction may only be evident when the patient is fully anesthetized and traction applied. Furthermore, while this study defines the osseous structures that may impede access to the cervicothoracic junction, the complex vascular and neurologic anatomy present in the thoracic inlet must also be studied in detail on advanced imaging and it may be the need for protection of these structures that dictates the need for manubrial or sternal osteotomy although various corridors have been described to facilitate safe passage past the major structures to gain access to the CTJ.23,24
In conclusion, a strong negative correlation between the Thoracic Inlet Angle and the Projection Angle of the cervicothoracic vertebrae was found and the influence of age on anterior access appears only minor. As the TIA approaches 105º, access to C7/T1 may become more challenging. During surgical planning attention to the sagittal thoracic inlet measures can help guide not only alignment goals but also access strategy when an anterior approach to the cervicothoracic junction is desired.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.